
Abstract
Introduction
Cervical cancer brachytherapy requires highly conformal dose delivery while minimizing radiation exposure to surrounding organs at risk. However, conventional tandem and ring applicators are limited by fixed geometry that may not optimally accommodate patient-specific anatomy. The purpose of this work was to evaluate the dosimetric performance of a novel tandem and ring applicator (RTA) featuring adjustable tandem translation relative to the ring, intended to improve organ-at-risk (OAR) sparing while preserving target coverage in high-dose-rate (HDR) brachytherapy for cervical cancer.
Methods and Materials
A novel RTA allowing linear tandem translation within the ring plane was developed to enable patient-specific alignment without altering ring position. Two cervical cancer patients treated with external beam radiotherapy (45Gy/25 fractions) followed by HDR brachytherapy (27.5Gy/5 fractions) were analyzed. Conventional and novel RTAs were sequentially applied to acquire CT-based datasets. Plans were optimized for adequate HR-CTV D90 coverage while minimizing D2cm3 doses to bladder, rectum, sigmoid, and bowel. EQD2 values (α/β = 3 for OARs; 10 for HR-CTV) were compared. Five retrospective cases were replanned using the novel RTA. Point A was redefined as 2cm superior along the tandem from the cervical os and 2cm lateral perpendicular to the tandem axis.
Results
For patient 1, the novel RTA reduced average daily D2cm3 by 0.54Gy (rectum), 0.78Gy (bladder), and 0.18Gy (sigmoid), with cumulative EQD2 reductions of 2.23Gy, 4.88Gy, and 1.05Gy, respectively. Patient 2 showed daily reductions of 0.52Gy (rectum) and 0.44Gy (bladder), with EQD2 decreases of 3.20Gy and 4.55Gy. HR-CTV EQD2 increased by 1.67Gy. Retrospective plans demonstrated consistent reductions in OAR doses.
Conclusion
The novel RTA demonstrated favorable dosimetric trends for OAR sparing while maintaining target coverage in cervical HDR brachytherapy. The revised Point A definition provides a preliminary framework for anatomically consistent dose reporting in flexible tandem configurations.
Introduction
Gynecological malignancies—particularly cervical and endometrial cancers—continue to represent a significant global health burden, accounting for considerable morbidity and mortality among women worldwide. 1 Cervical cancer, in particular, remains a leading cause of cancer-related death in low- and middle-income countries, underscoring the critical importance of accessible and effective treatment strategies. Radiotherapy plays a pivotal role in the curative management of cervical cancer, especially for patients with locally advanced diseases. High-dose-rate (HDR) brachytherapy is an essential element of this approach, delivering high doses of radiation directly to the tumor while limiting exposure to surrounding normal tissues. 2 The therapeutic success of HDR brachytherapy depends not only on advanced imaging and treatment planning but also on the mechanical precision and versatility of applicator systems used to position radioactive sources.
Applicator design is thus central to the dosimetric quality of intracavitary brachytherapy. The most widely adopted devices include the tandem and ring and tandem and ovoid systems, which enable placement of the intrauterine tandem for central tumor coverage and lateral vaginal components for peripheral dose distribution.3,4 These applicators have been validated in large clinical trials and integrated into international treatment guidelines, forming the standard of care across many institutions. 5 However, despite their clinical utility, traditional applicators face persistent limitations that can impair treatment quality, particularly in complex or anatomically variable cases.
One of the primary challenges is the wide interpatient anatomical variability, which can result in poor applicator fit and suboptimal positioning of the source channels relative to the high-risk clinical target volume (HR-CTV). 6 This can lead to underdosing of tumor tissue or excessive irradiation of organs at risk (OARs), such as the bladder, rectum, sigmoid colon, and bowel. Furthermore, standard applicator geometries lack flexibility in cases involving uterine retroversion, bulky parametrial involvement, or distortion due to prior surgery or tumor invasion. 7 Their rigid structure can also contribute to procedural difficulty, increase patient discomfort, and limit their use in certain clinical scenarios. 8 The need for highly conformal dose distributions in close proximity to critical structures makes these limitations especially consequential.
While advances in imaging, including CT and MRI-based treatment planning, have significantly enhanced applicator visualization and dose optimization, the physical limitations of applicator geometry remain a critical bottleneck in fully realizing the potential of image-guided adaptive brachytherapy (IGABT).9-11 IGABT allows for tailored dose distributions based on tumor regression and anatomical changes over time, but this approach still depends heavily on the mechanical adaptability and precision of the applicator system.
In response to these clinical and dosimetric challenges, we developed a novel tandem and ring applicator featuring adjustable linear translation of the tandem relative to the ring plane. Unlike standard fixed-geometry systems, this design allows for patient-specific adjustment of tandem placement without altering ring position, improving alignment with the uterine canal and supporting more precise source distribution. The applicator’s modular construction also facilitates better anatomical accommodation, potentially reducing insertion-related discomfort and enhancing treatment reproducibility. By enabling tailored tandem positioning, the system aims to enhance dose conformity, reduce OAR exposure, and improve overall treatment quality in diverse clinical presentations.
In addition, this design necessitated a redefinition of the conventional Point A, historically used as a reference for dose prescription in cervical brachytherapy. Because the tandem’s position is no longer fixed within the applicator, Point A was redefined in this study as 2 cm superior to the cervical os along the actual tandem axis and 2 cm lateral perpendicular to that axis. This anatomically driven definition was intended to provide a more geometrically consistent framework for dose prescription across variable tandem configurations.
This study presents the conceptual development, engineering implementation, and initial dosimetric evaluation of the proposed applicator. Through comparative planning with conventional tandem and ring systems, we assess the impact of this innovation on dose distribution to target volumes and OARs. The redefined Point A and modular tandem positioning together represent a preliminary step toward more personalized brachytherapy approaches, with potential implications for clinical practice, especially in anatomically challenging or previously undertreated patient populations.
Material and Methods
The Applicator Design
A novel tandem and ring applicator (RTA) was developed to address the geometric rigidity of conventional systems and improve anatomical adaptability in cervical cancer high-dose-rate (HDR) brachytherapy. In standard RTAs, the tandem is fixed centrally within the ring, limiting the ability to adjust to patient-specific anatomical variations. The novel RTA was engineered to allow longitudinal translation of the tandem relative to the ring, enabling three distinct positional configurations: centrally aligned, proximally displaced (toward the uterine orifice), and distally displaced (toward the vaginal introitus) (Figure 1). This mechanical flexibility allows improved source positioning to enhance dose conformity and reduce exposure to nearby OARs, including the bladder, rectum, sigmoid colon, and bowel. The (A) Variations in the pear-shaped dose distribution caused by tandem shifts—top view. (B) Physical displacement of the tandem relative to the ring, demonstrating increased flexibility in treatment planning. Figure 1B demonstrates the tandem translation mechanism and the adjustable tandem-ring interface permitting controlled longitudinal displacement of the tandem relative to the ring plane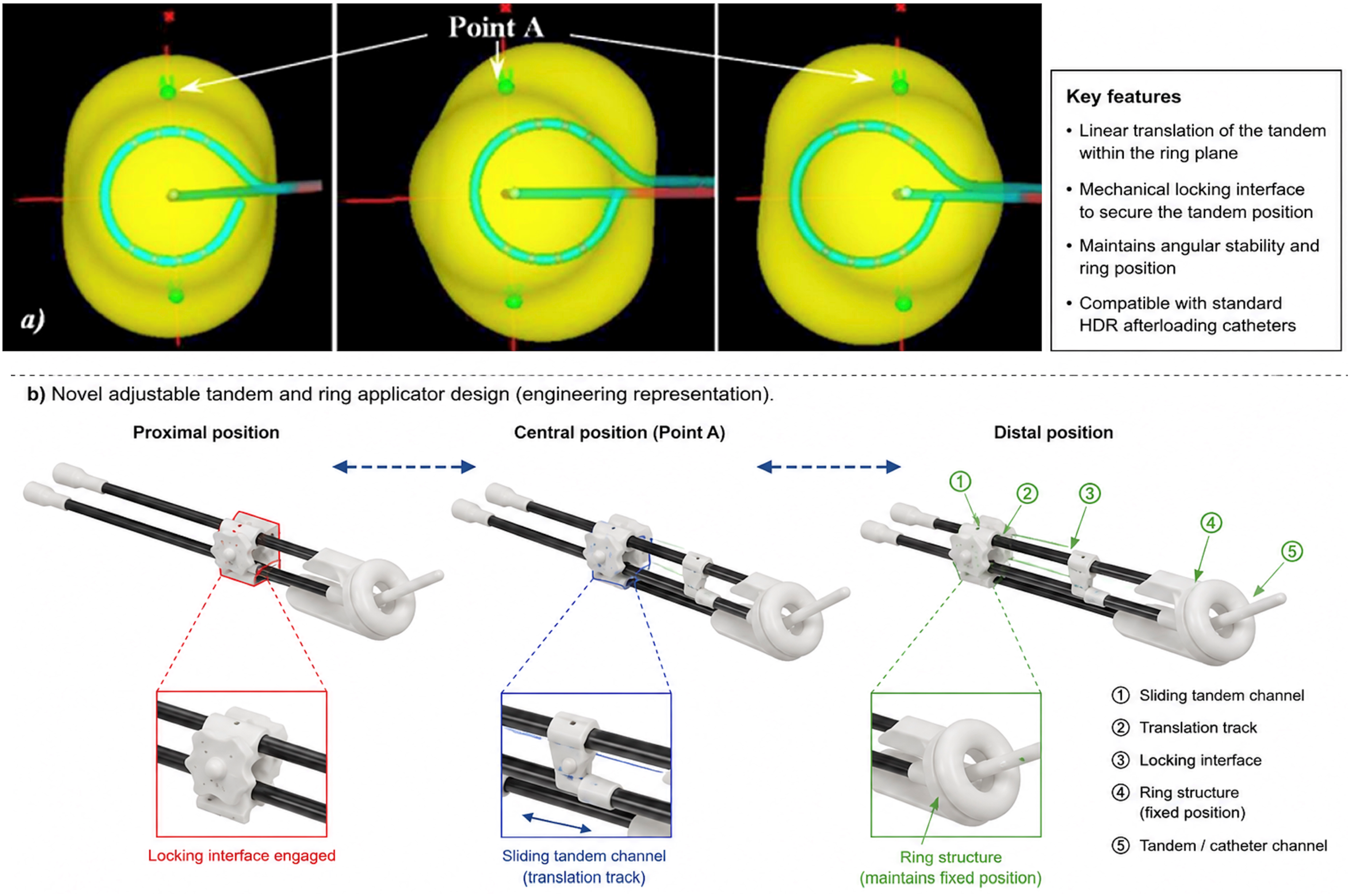
The prototype applicator was designed using a modular assembly consisting of a modified tandem channel integrated into a ring support structure permitting controlled longitudinal translation of the tandem relative to the ring plane. Tandem displacement was achieved through a guided sliding track mechanism allowing reproducible proximal or distal adjustment while maintaining angular stability during insertion and treatment delivery. Once the desired position was achieved, the tandem was secured using a mechanical locking interface designed to prevent unintended displacement during imaging and irradiation.
The current prototype permits approximately ±1.5 cm of longitudinal tandem translation relative to the central ring position. The applicator was constructed using biocompatible and sterilizable medical-grade materials compatible with HDR afterloading procedures and standard clinical sterilization workflows. The tandem channel dimensions were designed to maintain compatibility with commercially available HDR source guide tubes and remote afterloading systems.
To accommodate this geometric variability, a redefinition of Point A—the traditional dose prescription reference point—was implemented. In this study, Point A was redefined as the point located 2 cm superior along the actual tandem axis from the cervical os and 2 cm lateral perpendicular to that axis. This definition maintains anatomical consistency across all tandem positions and enables accurate dosimetric comparisons between plans, overcoming inconsistencies introduced by non-standard tandem trajectories.
Patient Selection and Treatment Protocol
Two patients diagnosed with locally advanced cervical carcinoma were prospectively enrolled under institutional review board approval. Each patient received external beam radiotherapy (EBRT) to the pelvis, totaling 45 Gy in 25 fractions using intensity-modulated radiation therapy (IMRT). This was followed by HDR intracavitary brachytherapy boost to a total dose of 27.5 Gy delivered in five fractions, consistent with GEC-ESTRO and ABS recommendations.
The study was conducted under an IRB-approved protocol, and the requirement for written informed consent was waived due to the retrospective nature of the study and minimal risk to participants. All procedures performed in this study were conducted in accordance with institutional ethical standards and the Declaration of Helsinki of 1975, as revised in 2024.
Applicator Insertion and Imaging
Applicator insertions were performed under general anesthesia by an experienced radiation oncologist. For each brachytherapy fraction, both the standard commercial RTA and the novel RTA were sequentially placed to acquire comparative imaging datasets. To minimize anatomical variability between sequential insertions, bladder filling protocols, patient positioning, anesthesia conditions, and vaginal packing approaches were maintained as consistently as possible during comparative imaging acquisition. Nevertheless, minor anatomical variations between insertions could not be completely eliminated. In the novel applicator, the ring was intentionally positioned distally toward the anterior vaginal wall to investigate the impact of tandem displacement on dose distribution.
Post-insertion CT imaging was performed using a multi-slice CT scanner (SOMATOM Definition AS, Siemens Healthcare) with 1 mm slice thickness. Standard imaging parameters (120 kVp, automatic mA modulation) were applied to ensure high spatial resolution and minimize imaging dose.
Contouring and Treatment Planning
HR-CTV, intermediate-risk CTV (IR-CTV), and relevant OARs (bladder, rectum, sigmoid colon, bowel) were contoured on each CT dataset by a single expert physician, following GEC-ESTRO recommendations to ensure consistency. Treatment planning was conducted using the Oncentra Brachy v4.5 planning system (Elekta AB, Stockholm, Sweden), utilizing TG-43U formalism for dose calculations.
Treatment plans were optimized using inverse planning simulated annealing (IPSA) algorithms, with the goal of achieving at least 90% coverage of the HR-CTV by the prescription dose (D90) while minimizing the D2cm3 for all OARs. Source dwell positions and times were adjusted individually for each plan. In Patients 1 and 2, the novel RTA was used in both the standard tandem position and a shifted position within the same treatment course, with the corresponding dose distributions shown in Figure 2. This figure demonstrates how translating the tandem relative to the ring plane in the RTA configuration can reduce bladder dose, as shown by the shift to a more distal position in the dose distribution. Dose distributions for a representative case, illustrating (A) the initial RTA configuration with the tandem centered within the ring, and (B) the adjusted configuration following translation of the tandem relative to the ring plane to reduce bladder dose. The arrow indicates the direction of the tandem shift to its more distal position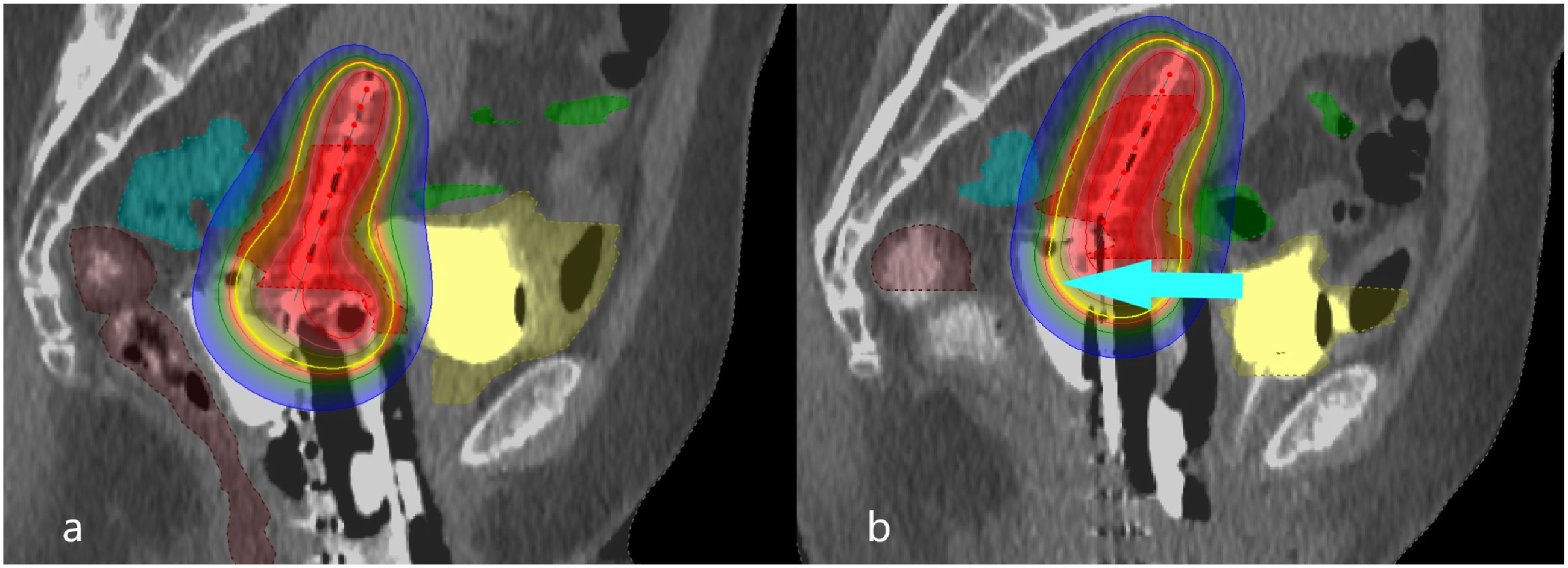
Treatment Plan Dataset
A total of ten clinical treatment plans were analyzed: five plans per patient. For patient one, two plans used the standard RTA and three used the novel applicator. For patient two, three plans utilized the standard RTA and two employed the novel design. To further explore the influence of applicator geometry on dose distribution, five additional retrospective plans were generated on existing CT datasets by varying tandem positioning within the novel applicator.
Dosimetric Analysis
The primary dosimetric endpoints were as follows: • HR-CTV D90: the minimum dose received by 90% of the HR-CTV, representing target coverage. • OAR D2cm3: the minimum dose received by the most irradiated 2 cm3 volume of the bladder, rectum, sigmoid colon, and bowel.
Cumulative biologically effective doses from EBRT and HDR brachytherapy were calculated using the linear-quadratic model, converting all doses to equivalent doses in 2 Gy fractions (EQD2). For this, an α/β of 10 was used for tumor tissue, and 3 for late-responding normal tissues.
Statistical Analysis
Descriptive statistics were calculated for all dosimetric parameters. Comparisons between treatment plans utilizing the standard versus novel applicator were performed using the Wilcoxon signed-rank test, appropriate for paired, non-parametric data with small sample size. Statistical significance was defined as p < 0.05. All statistical analyses were performed using IBM SPSS Statistics v29.0 (IBM Corp., Armonk, NY).
Given the exploratory nature of this pilot feasibility study and the limited sample size, statistical analyses were intended primarily to identify preliminary dosimetric trends rather than establish definitive inferential conclusions.
Results
The Dosimetric Comparison Between Standard and Novel RTA
A total of 15 HDR brachytherapy treatment plans were analyzed, including 10 clinical fractions from two patients and 5 retrospective plans. Dosimetric parameters for the clinical target volume (CTV) and OARs were compared between the standard RTA and the novel RTA with three tandem positions (central, proximal, distal).
Target Coverage (CTV D90)
Across all plans, the mean CTV D90 with the novel RTA was 85.3% ± 4.7% of the prescribed dose, compared to 84.9% ± 5.1% with the standard RTA (p = 0.42, Wilcoxon signed-rank test), indicating no statistically significant difference in tumor coverage. Notably, in Patient 2, a 1.67 Gy increase in cumulative EQD2 to the CTV was observed with the novel RTA, suggesting potential feasibility of future dose escalation strategies pending additional validation.
Organs at Risk (OARs)
• Rectum: The novel RTA significantly reduced the mean daily D2cm3 dose to the rectum by 0.53 Gy compared to the standard RTA (mean 1.46 Gy vs. 1.99 Gy, p = 0.008). This corresponded to a cumulative EQD2 rectal dose reduction of approximately 3.20 Gy over the course of treatment. • Bladder: The bladder demonstrated the most substantial dose sparing, with the novel RTA lowering mean daily D2cm3 doses by 0.61 Gy (1.30 Gy vs. 1.91 Gy, p = 0.005). This corresponded to a cumulative EQD2 decrease of up to 4.88 Gy, which may be clinically relevant based on established OAR dose-response relationships. • Sigmoid Colon: Sigmoid colon doses decreased by 0.43 Gy daily (mean 1.02 Gy vs. 1.45 Gy, p = 0.02) with the novel RTA, yielding a cumulative EQD2 reduction of 1.05 Gy. This dose reduction may be relevant given the sigmoid colon’s sensitivity to radiation exposure. • Bowel: A modest increase in mean daily D2cm3 bowel dose of 0.29 Gy (0.89 Gy vs. 0.60 Gy, p = 0.03) was observed with the novel RTA. While statistically significant, these doses remained well below tolerance thresholds, suggesting potentially limited clinical impact, Table 1.
Summary of Statistical Outcomes
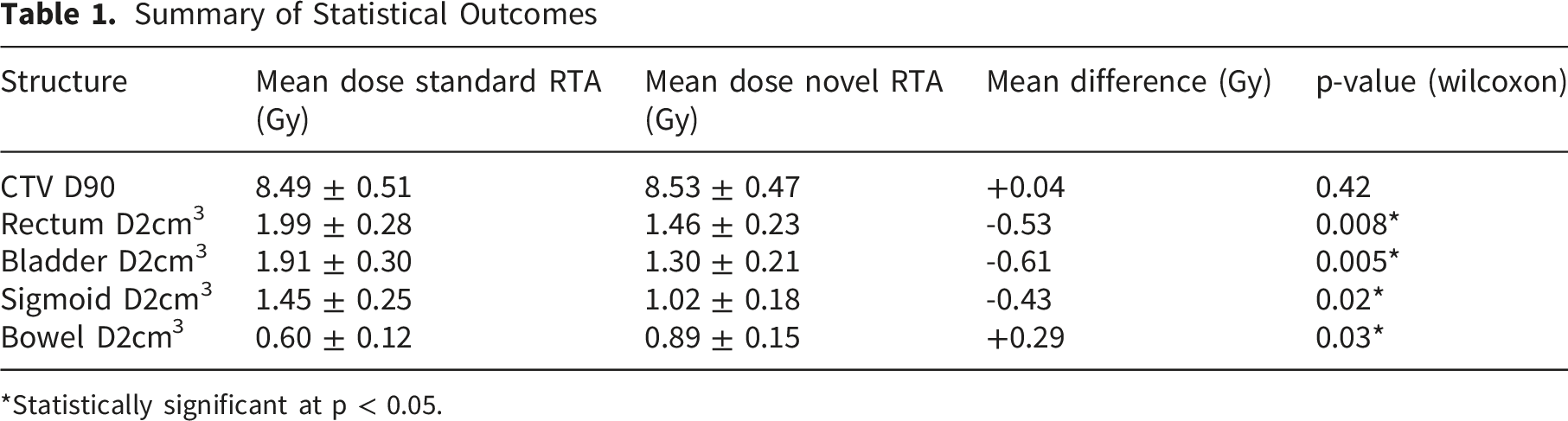
*Statistically significant at p < 0.05.
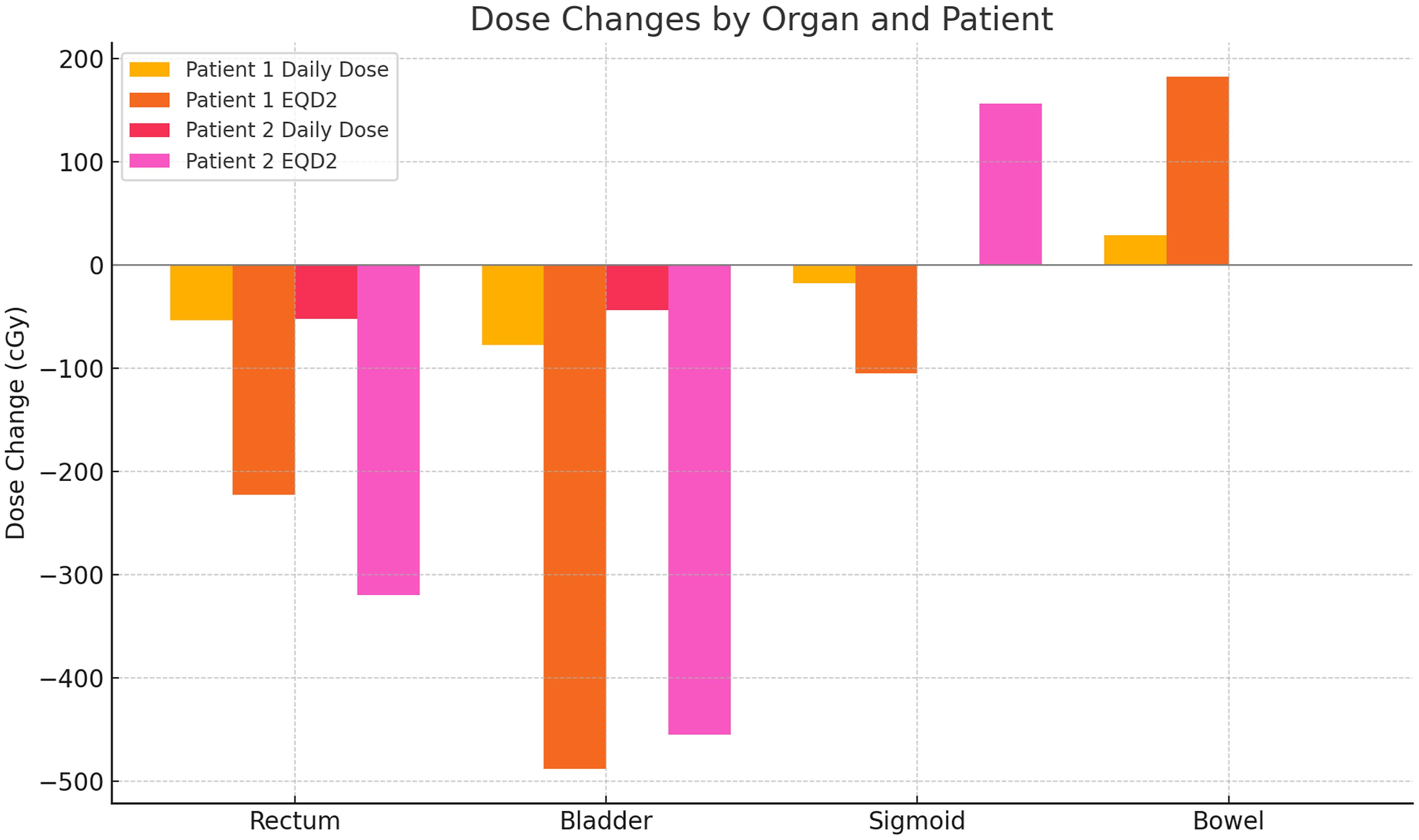
Changes in radiation dose for two patients across four organs—rectum, bladder, sigmoid, and bowel—comparing a novel RTA to standard planning
Retrospective Plans
Analysis of five retrospective treatment plans confirmed the trends observed in clinical fractions. The novel RTA showed mean daily dose reductions of 0.33 Gy for bladder (p = 0.04), 0.34 Gy for rectum (p = 0.06, borderline significance), and 0.67 Gy for sigmoid colon (p = 0.01), with no significant change in CTV coverage (p = 0.55).
Summary of Statistical Outcomes
Although several dosimetric parameters demonstrated statistically significant differences, these findings should be interpreted cautiously due to the exploratory nature of the study and the limited sample size. The observed trends primarily support the technical feasibility and potential dosimetric utility of the proposed applicator design and warrant validation in larger prospective patient cohorts. For the rectum, bladder, and sigmoid colon, p-values were less than 0.05, indicating measurable dosimetric differences between the standard and novel RTA configurations (Figure 4). However, given the exploratory nature of the study and the limited sample size, these findings should be interpreted cautiously and viewed primarily as preliminary observations supporting the technical feasibility and potential dosimetric utility of the proposed applicator design. No statistically significant difference in CTV coverage was observed between the two techniques (p = 0.42). Although the bowel dose increases also reached statistical significance (p = 0.03), the absolute dose values remained relatively low. Overall, the observed trends suggest that the novel RTA may provide favorable dosimetric characteristics for organ sparing while maintaining target coverage. p-values for daily dose changes across four organs for patient 1 and patient 2. The dotted line at p = 0.05 marks the statistical significance threshold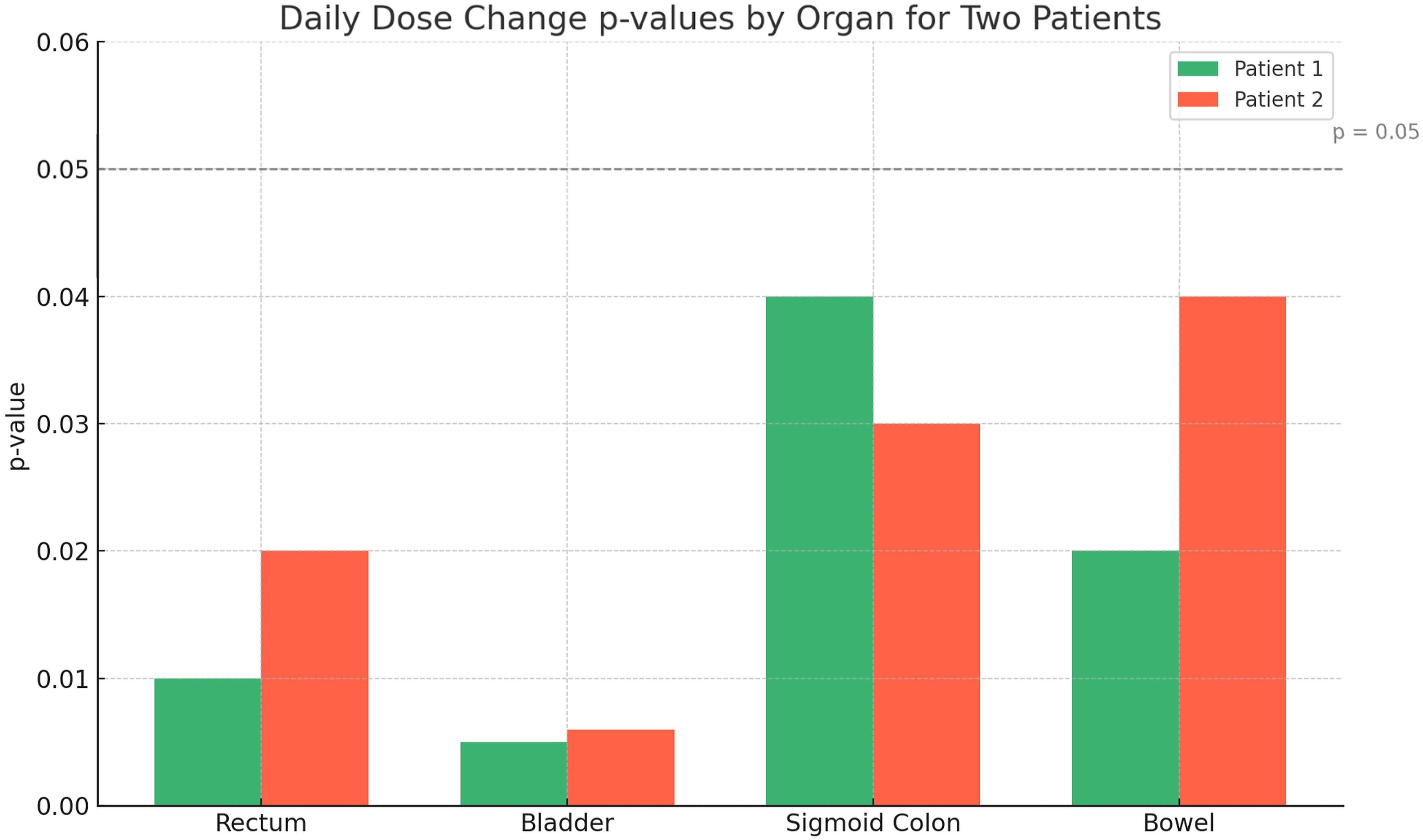
Dose Distribution Trends Across Organs and Patients
Patient 1 – Daily D2cm3 Dose Comparison (Gy) Between Standard and Novel RTA
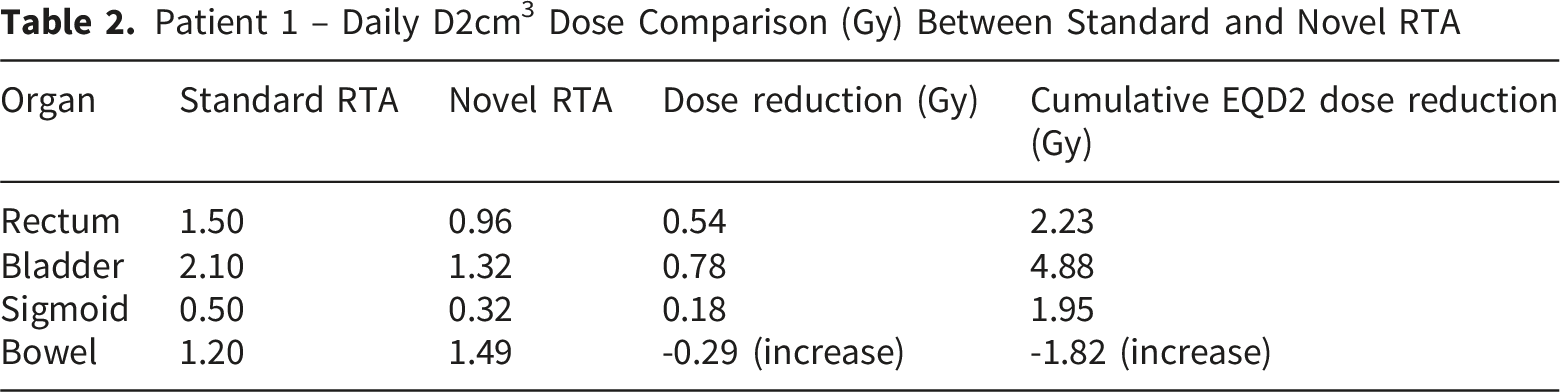
In the sigmoid colon, Patient 1 benefited from modest dose sparing, whereas Patient 2 saw an increase in cumulative EQD2 by 1.56 Gy, indicating some variability in dose distribution outcomes. Additionally, the bowel dose increased for Patient 1 by 0.29 Gy daily and 1.82 Gy cumulatively. These findings underscore the novel RTA’s ability to reduce radiation exposure to critical organs such as the bladder and rectum but also highlight a potential redistribution of dose burden to adjacent structures like the sigmoid colon and bowel in select cases. Such trade-offs may warrant individualized consideration during treatment planning to optimize therapeutic benefit while minimizing toxicity.
Point a Geometry and Dosimetric Integration in the Novel RTA Applicator
To support standardized dose prescription across all plans, Point A was redefined dynamically based on the actual tandem position within the novel RTA, which permits variable tandem placements (central, proximal, or distal). In each configuration, Point A was identified by measuring 2 cm superiorly along the tandem axis from the external cervical os (or applicator flange), followed by a 2 cm lateral offset perpendicular to the tandem axis. This local coordinate system preserved geometric consistency with the classic Manchester system while accommodating the novel applicator’s positional flexibility.
The redefined Point A coordinates were successfully generated in all 15 treatment plans and used as supplemental dosimetric landmarks for evaluation. Across all configurations, Point A remained within 3 mm of the paracervical triangle contour in 92% of plans, as confirmed on co-registered imaging. No significant deviation (>5 mm) was observed between Point A and the tumor volume edge in any case, supporting the geometric feasibility of the approach.
While cumulative EQD2 values at Point A varied slightly across tandem positions, the relative dose deviation between standard and novel RTA plans remained within ±4% in all cases, indicating that tandem flexibility did not compromise dose delivery to this surrogate target location. Furthermore, the spatial integrity of Point A was preserved across both patients and all retrospective plan variations, enabling consistent comparative analysis despite anatomical heterogeneity.
Discussion
This study presents a novel RTA that introduces positional adjustability of the tandem relative to the ring component—an innovation intended to improve geometric conformity to patient anatomy in high-dose-rate (HDR) brachytherapy for cervical cancer. The dosimetric analysis across multiple treatment fractions demonstrated trends toward reduced radiation exposure to OARs—notably the bladder, rectum, and sigmoid colon—without compromising CTV coverage. These findings suggest that the Novel RTA may provide favorable dosimetric characteristics that could potentially improve the therapeutic ratio pending further validation.
Clinical and Dosimetric Significance
Dose reduction to OARs is of paramount importance in gynecologic brachytherapy due to the dose-limiting toxicities associated with bladder (cystitis), rectal (proctitis), and sigmoid (sigmoiditis) radiation exposure. In our cohort, the Novel RTA achieved mean reductions of approximately 0.33–0.34 Gy per fraction to the bladder and rectum and up to 0.67 Gy per fraction to the sigmoid, which cumulatively correspond to equivalent dose in 2 Gy fractions (EQD2) reductions of nearly 5 Gy to the bladder, 2 Gy to the rectum, and 1 Gy to the sigmoid over five fractions. These dosimetric reductions may be clinically relevant based on established OAR dose-response relationships reported in prior literature.3,6,7
Importantly, these dose-sparing benefits were achieved without reducing CTV D90. In fact, in one case, total CTV EQD2 increased by 1.67 Gy, suggesting that the improved applicator geometry may potentially facilitate future dose escalation strategies, although this requires additional validation, with possible implications for local tumor control—a known predictor of long-term outcomes.2,10
Point A: Traditional Definition vs. Novel RTA Recontextualization
A key conceptual advancement in this study is the redefinition of Point A in the context of the novel RTA’s variable tandem position. Traditionally, Point A has been defined as 2 cm superior to the external cervical os and 2 cm lateral to the tandem, based on a fixed applicator geometry standardized by the Manchester system and ICRU Report 38. 12 This coordinate system presumes a rigid tandem centrally located in a fixed ring.
However, the Novel RTA allows proximal, central, or distal displacement of the tandem relative to the ring, disrupting the classical spatial assumptions. To preserve the anatomical relevance of Point A—representing the region where the uterine artery crosses the ureter—we propose a dynamic Point A definition:
The proposed Point A adaptation should presently be viewed as a preliminary conceptual and geometric framework requiring additional clinical validation before broader implementation. As applicator geometry evolves, rigid coordinate systems should also be adapted to reflect the treatment delivery. This approach aligns with the principles of image-guided adaptive brachytherapy (IGABT), where precision and personalization are crucial.4,7
Mechanistic Insights and Applicator Advantage
The observed dosimetric trends may in part be attributable to the enhanced anatomical conformity permitted by the novel RTA’s sliding tandem mechanism. By adjusting the tandem’s longitudinal position relative to the ring, clinicians can fine-tune the applicator configuration to better align with patient-specific pelvic anatomy and tumor geometry. This is particularly beneficial in patients with uterine or cervical deviations, irregular tumor shapes, or post-treatment anatomic changes.
Standard RTAs with fixed tandem-ring geometries often necessitate trade-offs between optimal target coverage and OAR sparing. 5 In contrast, the Novel RTA allows tailored source positioning that displaces high-dose regions away from sensitive structures while maintaining favorable dose conformity to the target. This approach echoes recent trends in brachytherapy towards customization, including hybrid intracavitary-interstitial techniques and adaptive planning, but with the added benefit of maintaining procedural simplicity.8,13
Clinical Significance of Dosimetric Improvements
In this study, reductions in D2cm3 doses to the rectum and bladder ranged from approximately 0.44 to 0.78 Gy per fraction, translating into cumulative EQD2 decreases exceeding 2.00 Gy for the rectum and nearly 5.00 Gy for the bladder in some patients. These findings may be clinically relevant and consistent with prior reports demonstrating that even modest reductions in OAR dose can reduce the incidence and severity of radiation-induced toxicities. For instance, in 14 it was showed that bladder D2cm3 values above 80–90 Gy EQD2 were associated with significantly higher rates of late cystitis, while rectal D2cm3 values exceeding 70–75 Gy EQD2 correlated with increased risk of proctitis. The observed dose reductions may potentially help maintain OAR doses below these key toxicity thresholds, particularly in patients requiring dose escalation or re-irradiation.
The ability to maintain equivalent or improved CTV D90 coverage while simultaneously reducing OAR exposure is an important observation, as adequate CTV dosing is strongly correlated with improved local control and survival outcomes in cervical cancer. Notably, in 15 it was reported that CTV D90 >85 Gy EQD2 is associated with superior local control. In our analysis, one patient experienced a CTV EQD2 increase of 1.67 Gy compared to the standard applicator plan, facilitated by more favorable source positioning made possible through the sliding tandem mechanism. These findings preliminarily suggest that the novel RTA may enable better OAR protection but may also support dose escalation protocols while preserving acceptable OAR dose parameters.
Compared to traditional tandem and ring or tandem and ovoid systems, the novel RTA provides a mechanically simpler alternative to more invasive interstitial or hybrid techniques. For example, while in16,17 was demonstrated that hybrid intracavitary–interstitial applicators offer superior conformality and target coverage in large or irregular tumors, these systems require more complex procedures, increased resource use, and specialized expertise. In contrast, the novel RTA achieves significant dosimetric improvements without the need for interstitial needles, offering an attractive balance between effectiveness and procedural efficiency.
Importantly, although slight increases in bowel and sigmoid colon D2cm3 were noted in some cases when using the novel RTA, these remained well below established tolerance limits and are comparable to dose variations reported in studies using advanced or hybrid applicator configurations. In our study, the highest observed sigmoid D2cm3 increase was under 1.2 Gy EQD2, and bowel doses remained within accepted parameters. These findings underscore the importance of individualized OAR evaluation but support the novel RTA’s overall favorable risk–benefit profile.
Moreover, compared to dose modulation through tandem angle variation, 7 which can influence the spatial distribution of dose but lacks direct control over tandem-to-ring spacing, the novel RTA’s longitudinal adjustability provides more granular control over isodose shaping. This may result in more consistent dose reductions across fractions and greater reproducibility across patients with varying uterine orientations or tumor topographies.
Limitations
Despite promising preliminary dosimetric findings, this study has several important limitations. First, the sample size was limited, restricting statistical power and limiting generalizability of the findings. Consequently, statistical analyses should be interpreted cautiously and viewed primarily as exploratory observations intended to guide future prospective investigation rather than definitive evidence of clinical superiority. Second, this was a retrospective dosimetric analysis, and clinical outcomes such as local control, toxicity rates, and patient-reported quality of life were not assessed. Third, all plans were generated on CT imaging, which, while widely available, may underrepresent soft-tissue boundaries compared to MRI. Future studies should incorporate MRI-based planning to further optimize delineation of the CTV and OARs—particularly the sigmoid and bowel. 6 Because both applicator configurations were sequentially evaluated within the same procedural setting, some degree of anatomical variation related to bladder filling, rectal position, tissue deformation, or vaginal packing may have influenced dosimetric comparisons despite attempts to standardize procedural conditions.
Additionally, while bowel dose increased slightly in some patients due to shifts in dose distribution from tandem repositioning, all values remained within acceptable thresholds. Nonetheless, this finding underscores the importance of comprehensive OAR evaluation during treatment planning to prevent unintended dose escalation to non-target tissues.
Future Directions
Further validation of the novel RTA should occur through prospective clinical trials evaluating not only dosimetric endpoints but also clinical outcomes, including acute and late toxicity profiles, tumor control rates, and patient-reported outcomes. The integration of MRI-guided adaptive brachytherapy could further enhance the precision of tandem positioning and dose delivery. Moreover, real-time or semi-continuous tandem adjustability, as well as automated planning algorithms that optimize source dwell positions based on tandem placement, represent logical next steps in applicator development.
Finally, future work should focus on patient selection criteria—identifying anatomical or tumor characteristics that predict maximum benefit from novel RTA use. This would support a more targeted implementation strategy and guide training for radiation oncologists and dosimetrists adopting the system.
Conclusions
The novel RTA featuring a sliding tandem mechanism represents a promising preliminary technical development in intracavitary brachytherapy for cervical cancer by enabling precise, patient-specific adjustment of the tandem position relative to the ring. This design approach may provide enhanced anatomical adaptability through discrete proximal or distal tandem displacement within the ring plane, allowing optimized source geometry tailored to individual uterine and vaginal anatomy.
Dosimetrically, this flexibility was associated with reductions in radiation dose to critical organs at risk —particularly the bladder and rectum—while maintaining or improving coverage of the clinical target volume. The device’s capacity to modify the spatial relationship between tandem and ring redefines the traditional Point A coordinates in a geometrically adaptive manner, potentially facilitating more adaptable dose conformity and improved spatial dose modulation.
The observed cumulative EQD2 dose reductions to OARs, suggest a potential for reducing radiation exposure to organs at risk, although clinical outcome validation remains necessary. Additionally, this adaptable applicator design offers a streamlined, less invasive alternative to combined intracavitary-interstitial approaches, with potential workflow and procedural advantages without compromising dosimetric outcomes.
Although these preliminary dosimetric findings are encouraging, further validation through prospective clinical trials and integration with advanced image-guided and adaptive planning techniques is warranted to confirm clinical benefits.
Ethics Statement
This work was conducted under an Institutional Review Board (IRB)-approved protocol at at Dana-Farber Cancer Institute/Brigham and Women’s Hospital (Protocol 19-089; Title: “Retrospective Study of Radiation Therapy Treatment Plans to Improve Treatment Techniques”; approved December 13, 2024). The requirement for written informed consent was waived by the IRB due to the retrospective nature of the study and minimal risk to participants. All procedures performed in this study were conducted in accordance with institutional ethical standards and international ethical guidelines, including the Declaration of Helsinki of 1975, as revised in 2024.
Footnotes
Acknowledgments
This work has been partially funded by Taiclet Technology Awards 2020.
Ethical Considerations
This work was conducted under an Institutional Review Board (IRB)-approved protocol at Dana-Farber Cancer Institute/Brigham and Women’s Hospital (Protocol 19-089; Title: “Retrospective Study of Radiation Therapy Treatment Plans to Improve Treatment Techniques”; approved December 13, 2024). The requirement for written informed consent was waived by the IRB due to the retrospective nature of the study and minimal risk to participants. All procedures performed in this study were conducted in accordance with institutional ethical standards and international ethical guidelines, including the Declaration of Helsinki of 1975, as revised in 2024.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been partially funded by Taiclet Technology Awards 2020.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.