
Abstract
Despite comprising the largest segment of the sexual minority population and experiencing unique stressors and health disparities, bi+ dementia caregivers remain underrepresented in health and caregiving research. This secondary analysis of cross-sectional survey data from LGBTQ+ dementia caregivers (bi+, n = 125; gay[g]/lesbian[l], n = 161) examined whether associations between minority and caregiving stressors and global health differed by caregiver group. Bi+ caregivers reported significantly higher minority stress and lower family quality of life but better health than g/l caregivers. Moderation analyses revealed: higher perceived stress predicted worse health for bi+ but better health for g/l; higher family quality of life predicted better health for both groups, with a stronger effect among bi+ caregivers; and more lifetime discrimination predicted worse health for both groups, with a stronger effect among bi+ caregivers. Results underscore the need for inclusive, affirming research and interventions addressing bi+ caregiver stress experiences.
Keywords
Background
More than 11 million adults in the U.S. provide unpaid care to family members, friends, and other people living with Alzheimer’s disease and other dementias (ADRD). 1 ADRD caregivers are particularly susceptible to physical, social, emotional, and financial challenges, more so than caregivers of older individuals living with other chronic conditions, given the extensive assistance they tend to provide. 2 Beyond the nature of tasks being provided during care, caregiving experiences can vary depending on additional factors such as caregiving duration and the social position of the caregiver (e.g., race/ethnicity, sexual orientation, gender identity), factors that ultimately influence the caregiver’s health and well-being.1,3
LGBTQ+ is an umbrella term used to describe people who self-identify as lesbian, gay, bisexual, transgender, queer, nonbinary, intersex, and/or who express behaviors and attractions that do not align with heterosexual or conventional gender norms. 4 Recent population-based data estimates suggest that 1 in 5 LGBTQ+ adults are caregivers to a family member or friend with a disability or health problem. Over half of these caregivers are providing personal care (e.g., medical/nursing tasks) and approximately 20% are providing care to someone living with ADRD. 5 Research about LGBTQ+ ADRD caregivers is limited; however, LGBTQ+ ADRD caregivers have reported fewer financial and social resources and caregiver supports than non-LGBTQ+ ADRD caregivers and may be caring for someone who does not accept their LGBTQ+ identity, which can increase the psychological impact of caregiving. 6 In fact, findings from a study with a convenience sample of only LGBTQ+ ADRD caregivers found the majority of the sample reported elevated depressive symptoms and below average health. 3 Bi+ populations, those with non-monosexual identities (e.g., bisexual, pansexual, queer), are the largest sexually minoritized group in the U.S, and research suggests they face significant health disparities compared with both monosexual minority (i.e., gay, lesbian) and heterosexual individuals.7-9
Research suggests that disparities in health and well-being among bi+ individuals may be understood within an expanded Minority Stress and Resilience Framework. 10 Within the Minority Stress Framework, 11 health disparities among sexual minority populations arise from chronic exposure to stigma, discrimination, and social marginalization, as well as the expectation of these stressful experiences. Feinstein and Dyar 10 further expanded the Minority Stress Framework to theorize the phenomenon of bisexual-specific stressors, such as monosexism, identity invalidation, and erasure within both monosexual minority and heterosexual communities, factors that can lead to social isolation, invisibility, internalized stigma and consequently, poorer health outcomes. For some, the ability to “pass” as heterosexual may temporarily buffer exposure to external stigma, but it can also reinforce invisibility, erode identity affirmation, and reduce opportunities for social support. While such challenges can threaten the health of bi+ individuals,12-15 protective factors such as identity integration, affirming social networks, and community connectedness can mitigate these stressors by fostering resilience and psychological well-being.11,16,17 Identity integration promotes self-acceptance and reduces internalized stigma, buffering the emotional strain associated with identity concealment or invalidation.11,17 Affirming social networks provide validation and emotional support, directly counteracting experiences of rejection and isolation, while community connectedness enhances belonging and access to collective coping resources.18,19
The combination of minority stress and the demands of ADRD caregiving likely influence the health and well-being of bi+ caregivers. The unique stressors that many bi+ individuals experience (e.g., monosexism, isolation), can intersect with ADRD caregiving challenges (e.g., burnout, limited respite), amplifying vulnerability to caregiver burden and poor mental health.20,21 Bi+ caregivers may have reduced access to bi+- affirming caregiver support groups both within and outside of the LGBTQ+ community or experience invisibility within mainstream aging and ADRD networks. 22 Without affirming spaces to share their experiences, bi+ caregivers may internalize stigma or conceal their identity, further intensifying poor mental health outcomes. Conversely, when bi+ identities are affirmed and they are included within both LGBTQIA+ and caregiving communities, minority stress can be buffered, creating opportunities for resilience, coping capacity, psychological well-being, and caregiving engagement.10,19
Despite comprising the largest segment of the sexual minority population and experiencing unique stressors and health disparities, bi+ ADRD caregivers remain underrepresented in health and caregiving research and have been described as the invisible majority. 9 Furthermore, ADRD caregivers have been characterized as invisible second patients 23 due to the substantial physical, emotional, and social demands of ADRD caregiving. Taken together, these dual forms of invisibility suggest that we can appropriately consider bi+ ADRD caregivers as a twice hidden population. Given that existing research suggests that both ADRD caregiving challenges and minority stress can influence health, the current study examined associations between minority stress and stress on global health to determine if these associations differed among bi+ and gay/lesbian (g/l; monosexual) ADRD caregivers. We hypothesized that both minority and caregiving stress would be negatively associated with global health and that the impact would be greater for bi+ caregivers than g/l caregivers.
Methods
Data
This study is a secondary analysis of cross-sectional survey data from the Family Quality of Life Among LGBT Care partners of Persons with Dementia study, which examined the characteristics and caregiving experiences of LGBTQ+ ADRD caregivers. 3 Respondents were recruited through research registries, social media platforms, newsletters, and online forums that reach LGBTQ+ populations and individuals living with or caring for someone with ADRD. The methods and procedures for the original study are described in detail elsewhere. 3 Respondents were eligible if they self-identified as LGBTQ+ and provided unpaid assistance or attendance to the needs of an individual with ADRD for an average of at least 8 hours per week. Self-reported ADRD caregiver status was confirmed using the Ascertain Dementia 8-item Informant Questionnaire, a commonly used proxy report of ADRD diagnosis used in the National Health and Aging Trends Study. 24 Study recruitment posts included a link to a landing page explaining the purpose of the study including the eligibility screening criteria and an electronic indication of consent (i.e., consent implied by completing the survey). Upon eligibility, respondents accessed a one-time, self-administered online survey through a HIPAA-secured survey platform. Respondents received a $25 electronic Amazon gift card upon completion of the survey. Data were collected from October 2019 to February 2020, and a total of 286 surveys were completed without missing data. Study materials were only available in English. The University of Tennessee-Knoxville Institutional Review Board reviewed and approved the original study design and procedures.
Measures
Study Group
The study group variable was dichotomously coded to represent caregiver sexual orientation (i.e., bi + vs g/l) based on the survey’s sexual identity question (response options: gay, lesbian, bisexual, or specify if not listed; responses specifying another identity were recoded as queer/another sexual orientation and included in the bi+ group). The original study did not assess sexual behavior or sexual attraction. Although the study group variable was coded dichotomously for regression analyses, our analytic focus was on whether the association between minority and caregiving stressors and global health differed between bi+ and g/l caregivers, as assessed through interaction terms and post-estimation marginal effects. While one category necessarily serves as the statistical reference group, results are interpreted as differences in slopes between groups rather than as a unidirectional comparison. We therefore use the term study group to describe this variable to reflect the comparative, rather than hierarchical, nature of the analysis.
Sociodemographics
Sociodemographic measures included age, gender identity, race, ethnicity, income, employment status, and marital or partner status. Age was captured in years. Gender identity was operationalized by using data obtained from two survey items. Respondents were asked to select which best represented how they currently think of their gender (man, woman, not listed/other). Next, respondents were asked, “Do you consider yourself to be transgender?” (yes/no). Respondents who indicated they were not transgender and selected woman for their gender identity were classified as cisgender women, and those who indicated they were not transgender and selected man for their gender identity were classified as cisgender men. Respondents who indicated they were transgender and selected man for their gender identity were classified as transgender men, and those who indicated they were transgender and selected woman for their gender identity were classified as transgender women. Two respondents indicated they were transgender and selected “not listed/other” for their current gender, and they were categorized as transgender, identity not listed.
For race, respondents who selected any of the non-White (i.e., African American/Black, Native American/Alaska Native, Asian, Pacific Islander/Native Hawaiian, other) racial identity categories provided were categorized as a member of a minoritized racial group (yes/no) in the current analysis. To assess ethnicity, respondents were asked whether they considered themselves to be of Hispanic/Latino/a/e/x) American origin, such as Puerto Rican, Mexican, Cuban, or other Spanish background (yes/no). Respondents were asked to report their income from categories in increments of $10,000 ranging from $1000 to $70,000 or more. The current study operationalized income with a dichotomous annual income variable ($49k or less; $50k or more). To capture employment status, respondents indicated whether they were employed at a job for pay, full time; employed at a job for pay, part time; a homemaker, not currently working for pay; not currently employed, retired; or not currently employed or not retired. The current study measured employment status with a dichotomous variable of currently employed at a job for pay part or full time (yes/no). Partner status categories included never married, married/partnered, widowed, separated, and divorced, which was recoded dichotomously as currently married/partnered (yes/no).
Minority Stress
We measured minority stress with five indicators including lifetime discrimination, lifetime victimization, daily discrimination, microaggressions, and perceived stress.25,26 Lifetime victimization was measured with nine questions asking respondents to report the number of times (never to three or more times) during their lives they had been victimized due to their LGBTQ+ identity. Total scores ranged from 9 to 36; higher scores indicated more frequent lifetime victimization (Internal consistency: α = .86). Day-to-day (measured with six questions) and lifetime (measured with five questions) discrimination asked respondents to rate their experiences with daily and lifetime discrimination related to being LGBTQ+, with response categories ranging from never to three or more times. Total scores ranged from 6 to 24 for day-to-day discrimination (α = .86) and 5 to 20 for lifetime discrimination (α = .79), with higher scores representing more frequent discrimination. Eight questions were used to assess experiences with microaggressions related to being LGBTQ+, with response options ranging from never to three or more times. Total scores ranged from 8 to 32, with higher scores representing more frequent microaggressions (α = .87). Perceived stress was ascertained with the 10-item Perceived Stress Scale27,28 that asked respondents to rate how often they thought or felt a certain way (as described by the item stem) during the previous month. For example, respondents were asked how often they were upset because of something happening unexpectedly or how often they felt difficulties were piling up and could not be overcome. Total scores range from 14 to 40, with a score ≤13 indicative of low stress, 14 to 26 representative of moderate stress, and ≥27 indicative of high stress (α = .79). The Cronbach’s alpha coefficients reported above were estimated using data collected from the study’s sample. 3
Caregiver Stress
Caregiver stress was conceptualized in relation to both the caregiving relationship type and family quality of life. 29 Specifically, among LGBTQ+ caregivers, caring for a spouse or partner, as opposed to a friend, is associated with higher levels of stress, 30 and lower family quality of life is associated with higher caregiver stress.20,31,32 Shiu et al, (2016) found that caregivers providing care to friends had fewer caregiving demands than those caring for a parter or spouse. This difference likely reflects greater role obligation, co-residence, and caregiving intensity among spouse/partner caregivers, who are more often the primary or sole provider of care. Greater caregiving demands are associated with increased subjective caregiving stress, which has been linked to poorer health outcomes. 33 Respondents were asked to report their relationship to the person with ADRD (i.e., spouse/partner, daughter/son, other relative/friend), which was then recoded as spouse/partner = 1 and all others = 0. Respondents were asked to complete the Family Quality of Life in Dementia Scale (FQOLDS), 29 a 41-item scale designed to capture the quality of life across four domains (i.e., caregiver support, disease-related support/medical care, family interactions, and well-being) among families caring for someone with ADRD as informed by its members. Total scores range from 41 to 205, with higher scores indicative of higher levels of family quality of life. In the present sample, the Cronbach’s α for the FQOLDS was 0.96.
Global Health
Caregiver’s global health was assessed using the PROMIS Global Health Scale, 34 a 10-item scale that asked respondents to rate their health across five domains including fatigue, physical function, emotional distress, pain, and social health, as well as general health perceptions. Raw scores range from 16 to 68, with a score ≥29 representing average or better global health (Cronbach’s α in the present sample was 0.86).
Data Analysis
Descriptive statistics were used to detail sample characteristics, minority stressors, caregiving stressors, and global health. We used chi-squared tests for categorical variables and ANOVA for continuous variables to assess between group (bi+ caregivers vs g/l caregivers) differences in sociodemographic characteristics, minority and caregiving stressors, and global health. To assess associations between minority and caregiving stress on global health, hierarchical linear regression analyses were conducted. Variance inflation factors (VIFs) were reviewed to assess for collinearity among our outcomes, covariates, minority stressors, and caregiving stressors. The only variables with a VIF score equal to or greater than five were daily discrimination (VIF = 6.47), lifetime discrimination (VIF = 5.24), and microaggressions (VIF = 6.12). Due to the exploratory nature of this study, we elected to model each stressor separately to examine its association with global health and if the magnitude of this association differed among the study groups. Stressors were included in the models as a continuous variable, an approach used by the parent study. 3 Study group and one minority or caregiver stressor were entered in model 1 (unadjusted model). Then age, gender identity, member of a minoritized racial group, Hispanic/Latino/a/x identity, and income were added in model 2 (adjusted model).
Marital/partnership status was not included as a covariate because it would have been conflated with the caregiving relationship variable (i.e., caring for a spouse or partner). In addition, at the bivariate level, there were no significant differences in the prevalence of being married or partnered across study groups. Similarly, retirement status was not examined independently, as employment status was operationalized dichotomously (currently employed for pay, full- or part-time = yes/no), and income was included as a control to account for socioeconomic differences while avoiding multicollinearity with employment-related variables.
In model 3, an interaction term, study group*stressor, was added to determine if study group (bi+ and g/l) moderated the association between the minority and/or caregiver stressor and global health. Post-estimate margins were performed and predicted probabilities were plotted to better interpret how the association between a minority or caregiving stressor and global health differed among the study groups. Separate hierarchical linear regression models were fit for each minority and caregiving stressor. Analyses were performed using Stata/SE 16.1. The level of significance for statistical tests, including interaction terms, was set at P < 0.05.
Results
Sample Characteristics
Sociodemographic Characteristics for Bi+ and Gay/Lesbian Caregivers, N = 286

Note. n (%) provided for categorical variables; mean, standard deviation (SD), and range provided for continuous variables.
aP values are based on the F-statistic for continuous variables and the chi-square test statistic for binary and categorical variables.
bGender identity and transgender identity: Participants who indicated they were transgender and selected man for their gender identity were classified as transgender men, and those who indicated they were transgender and selected woman for their gender identity were classified as transgender women.
cAmong those who endorsed being transgender, we provide a breakdown of how participants classified their gender identity.
dRace and minoritized racial group: Participants who indicated their race was not White were categorized as being from a minoritized racial group.
eEmployed: Participants who indicated they were employed at a job, full or part time, were categorized as employed.
Minority Stress, Caregiving Stress, and Global Health for Bi+ and Gay/Lesbian Caregivers

Note. Higher minority stress, family quality of life, or global health scores represent greater stress, better family quality of life, or better overall health, respectively.
Correlation Matrix of Global Health, Minority Stress, and Caregiving Stress Variables

Note. *P < .05; **P < .01.
Hierarchical Regression Models
Results From Hierarchical Regression Analyses With Minorirty and Caregiving Stressors Predicting Global Health Among Bi+ and Gay/Lesbian Caregivers (N = 286)

Note. Models adjusted for age, gender, belonging to a minoritized racial group, Hispanic/Latino/a/e/x identity, and income.
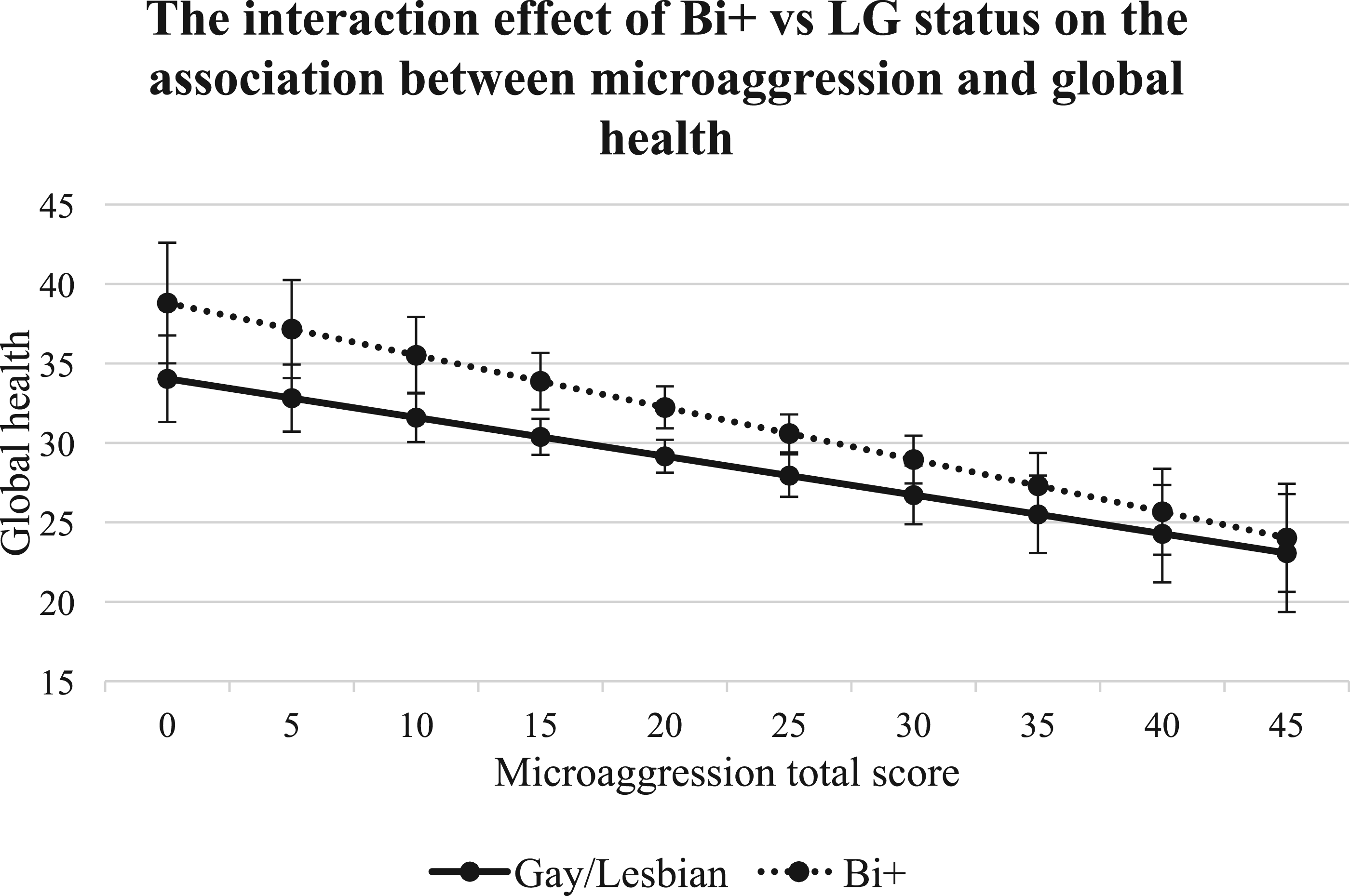
Study group (bi+ vs g/l) moderated the associations between global health and two indicators of minority stress (lifetime discrimination and perceived stress) as well as one indicator of caregiving stress, family quality of life. The overall lifetime discrimination model was significant (P < 0.0001) and explained 31.9% of the variance in the global health score. As illustrated in Figure 1, higher lifetime discrimination scores predicted worse global health for g/l and bi+ caregivers; the magnitude of this association was greater among bi+ caregivers. Regarding perceived stress, the overall model was significant (P < 0.0001) and accounted for 29.6% of the variation in global health. An inverse relationship among the study groups was revealed as shown in Figure 2. Higher perceived stress scores predicted worse global health for bi+ caregivers but better global health for g/l caregivers. The family quality of life model was significant (P < 0.0001) and explained 33.4% of the variance in the global health score. Higher family quality of life scores predicted better global health for both groups (Figure 3); the magnitude of the association was stronger among bi+ caregivers. There was no evidence of effect modification for study group in the models in terms of lifetime victimization, daily discrimination, microaggressions, and caring for a spouse/partner. Although not statistically significant, post-estimate margin plots (Figures 4–7) revealed trends towards significance, with a differential pattern in slopes across study groups. The interaction effect of Bi+ vs LG status on the association between lifetime discrimination and global health The interaction effect of Bi+ vs LG status on the association between perceived stress and global health The interaction effect of Bi+ vs LG status on the association between family quality of life and global health The interaction effect of Bi+ vs LG status on the association between lifetime victimization and global health The interaction effect of Bi+ vs LG status on the association between day-to-day discrimination and global health The interaction effect of Bi+ vs LG status on the association between microaggression and global health The interaction effect of Bi+ vs LG status on the association between caring for spouse/partner and global health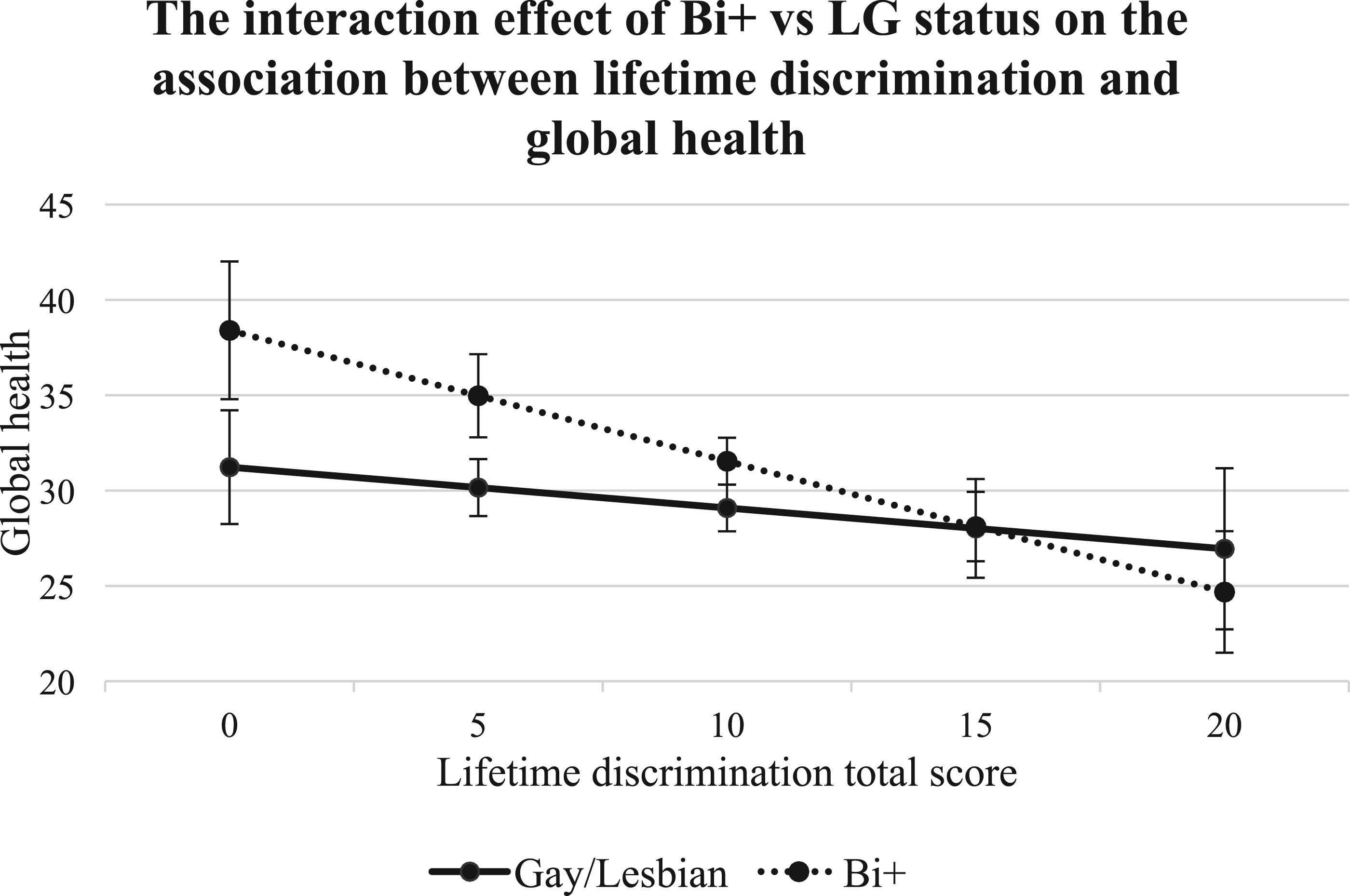





Discussion
This study contributes to the growing body of literature highlighting the heterogeneity of LGBTQ+ caregivers by demonstrating meaningful differences between bi+ and g/l ADRD caregivers across sociodemographic characteristics, minority and caregiving stressors, and global health. These findings reinforce the importance of examining differences in caregiving and health outcomes at the level of specific sexual minority subgroups rather than treating LGBTQ+ caregivers as a monolithic group. Notably, this study addresses a significant gap in the literature by centering bi+ ADRD caregivers, who are underrepresented in health research. Our results indicate that for bi+ caregivers, their experiences of stress, caregiving, and health differ in important ways from those of g/l caregivers, underscoring the need for more thoughtful approaches to caregiving supports, services, and future research that address the specific needs of each sexual minority subgroup.
Caring for a spouse or partner was the most common relationship type among both groups, though this was more frequent among g/l caregivers (61.5%) than bi+ caregivers (35.2%). This difference may be partially explained by limitations in the measure used to assess the caregiver–care recipient relationship, particularly regarding how spousal or partner categories were defined. The measure may not have fully captured relationship configurations more commonly reported among bi+ individuals, such as those identifying as pansexual or omnisexual.
In contrast to expectations, caring for a spouse or partner was positively associated with global health in adjusted models. This finding may reflect the well-established protective effects of a close and supportive marriage and partnership on health, including greater emotional support, social integration, and access to shared resources, rather than caregiving stress alone. Because marital or partnership status was not included as a separate covariate, and the original study did not assess relationship quality, it is possible that the spouse/partner caregiving variable captures both caregiving role and relational context. Future studies should distinguish caregiving relationship type from marital or partnership status and assess relationship quality to better disentangle caregiving burden from the health-promoting effects of supportive intimate partnerships.
Additionally, the gender of the caregiver’s partner was not collected and was not considered in the validated measures utilized. As such, it is plausible that bi+ caregivers who were married or partnered may have experienced differential levels of minority stress depending on whether others perceived their relationship as heteronormative or as indicative of LGBTQ+ identity. 35
LGBTQ+ individuals are recognized as a health-disparate population, with a substantial body of research indicating these disparities are often driven by minority stress, including experiences of discrimination related to their LGBTQ+ identities.7-9,11,12 In line with this evidence, the present study found that lifetime discrimination, lifetime victimization, daily discrimination, and microaggressions were negatively associated with global health among both bi+ and g/l ADRD caregivers. Notably, higher lifetime discrimination scores predicted poorer global health for both groups, with the magnitude of this association being stronger for bi+ caregivers compared with g/l caregivers. These findings underscore the existence of health disparities within the bi+ caregiver population and highlight the presence of bi+-specific minority stress, at least in terms of lifetime discrimination, on global health. These results are consistent with minority stress theory, 11 which posits that chronic exposure to discrimination and stigma accumulates over the life course, negatively affecting mental and physical health. This cumulative stress may be particularly pronounced among bi+ caregivers, who have been shown to lack the buffering effects of LGBTQ+ community support that can mitigate minority stress and promote well-being among g/l caregivers. 36
An expanded minority stress framework 10 provides a useful framework for understanding the unique stressors experienced by bi+ individuals due to anti-bisexual stigma, which differ from those experienced by their monosexual counterparts. Bi+ caregivers in our sample experienced more minority stress than g/l caregivers, including higher levels of victimization. Higher levels of victimization among bisexual people compared with lesbian and gay individuals have been found in previous research. 15 These elevated levels of minority stress may reflect the compounded negative attitudes bi+ individuals receive from heterosexual people because of their nonconformity to heteronormative standards, as well as from lesbian and gay people because of their nonconformity to monosexual standards. 35 Binegativity and hostility stemming from pervasive stereotypes that bisexuality is unstable, illegitimate, or inherently promiscuous can significantly undermine the ability of bisexual individuals to access safe and supportive communities. These stigmatizing beliefs not only contribute to social exclusion but also have deeply personal consequences. For example, stereotypes surrounding bi+ promiscuity and the perceived illegitimacy of bisexual identities can adversely affect romantic opportunities. Empirical research has shown that such negative attitudes often manifest in reluctance among heterosexual, gay, and lesbian individuals to engage in romantic relationships with bisexual partners. 10 Additionally, bi+ identities are questioned or invalidated when individuals are in monogamous relationships due to the erroneous assumption that bisexuality requires simultaneous involvement with partners of multiple genders to be legitimate. 37 Importantly, community belonging and being in romantic relationships have shown to be protective factors of health that can even mitigate the harms of minority stress.9,36,38,39
The degree to which an individual is perceived by others as belonging to an LGBTQ+ group may influence the experience of minority and caregiving stress. Research has demonstrated that perceived LGBTQ+ status can increase exposure to minority stressors. Bisexual individuals are more likely to experience stress related to disclosing and/or concealing their sexual identities than their g/l peers to avoid bi-negativity, limiting potential positive opportunities for connection with LGBTQ+ communities and reducing access to protective social support networks.10,16,19 Furthermore, among bi+ individuals in romantic partnerships, perceptions of their LGBTQ+ identity are often shaped by the gender of their partner, especially within monogamous relationships. For example, bisexual women partnered with other women are frequently assumed to be lesbians, even when they explicitly disclose a bisexual identity. Such misperceptions are associated with sexual identity questioning and uncertainty, where individuals begin to doubt whether the label ‘bisexual’ accurately reflects their sexual identity. 35 Moreover, there is evidence that bisexual women with male partners report more frequent experiences of bi-negativity compared with those with female partners, and this increased bi-negativity is linked to heightened levels of depression and alcohol use problems.35,40 Qualitative studies further indicate that bisexual identity erasure and feelings of invisibility in monogamous relationships are experienced as stressful and are associated with adverse mental health outcomes. 41
Bi+ caregivers in this study also had significantly lower family quality life scores. It is reasonable that the bi+ caregivers in our sample, who are experiencing more minority stress while also caring for someone with ADRD, may also be struggling with the quality of their family life and caregiving may be adding strain to their family. Income is another potential contributing factor, as many of the questions on the FQOLDS are influenced by income and other research has found a positive association between income and higher family quality of life scores among gay men. 42 However, it is imperative to note that the FQOLDS was not developed to capture the unique experiences of family life for LGBTQ+ caregivers. The FQOLDS does not account for LGBTQ+ individuals caring for a parent who is not accepting or affirming of their identity. This is a critical omission, as LGBTQ+ individuals who care for a parent report experiencing three times more emotional strain than their non-LGBTQ+ counterparts. 22 Additionally, the FQOLDS assumes the LGBTQ+ caregiver is caring for their family member living with ADRD. This may be problematic as research shows that LGBTQ+ caregiving often occurs between friends not just among family 38 and the bi+ caregivers in our study were less likely to be caring for their spouse or partner. The LGBTQ+ population is known for having non-traditional family structures due to experiencing stigma and discrimination from their birth family members, such as family rejection. As a result, LGBTQ+ people often create what is known as a chosen family, or a group of individuals who are not members of their birth family, who provide love and support, and this aspect of family is not addressed by the FQOLDS. Our understanding of LGBTQ+ caregivers family experiences with ADRD would benefit from further research that captures the lived experiences of LGBTQ+ caregivers with more accuracy, including bi+ caregivers whose family structures might look quite different than heterosexual and g/l caregivers.
For both bi+ and g/l caregivers, higher family quality of life scores predicted better global health, although the magnitude of this association was stronger for bi+ caregivers compared with g/l caregivers. It could be that family quality of life among bi+ caregivers may transcend the other challenges in their lives, which might include experiences of minority stress, bringing the most meaning to their lives and, ultimately, have a positive impact on their global health. Nevertheless, the lack of consideration of the lived experiences of LGBTQ+ ADRD caregivers in the FQOLDS previously mentioned likely discounts our opportunity to more accurately understand the influence of family quality of life in the caregiving experiences and health of bi+ and gay/lesbian ADRD caregivers.
Bi+ caregivers in this study reported higher global health scores than g/l caregivers. Research consistently demonstrates that bi+ people experience significant mental health disparities compared with their monosexual g/l and heterosexual counterparts,9,12-15 but less is known about the physical health disparities between these groups. While some research notes a higher risk of cardiovascular disease 43 and obesity 44 among bisexual and lesbian women compared with heterosexual women, physical health differences among sexual minority subgroups are understudied. Our finding of bi+ caregivers reporting better health than g/l caregivers differs from what was found in a study 21 that examined health-related quality of life among lesbian and bisexual women, which found a higher likelihood of poor general health among bisexual women than lesbians. Additionally, the higher global health scores observed among bi+ caregivers may, in part, be attributed to the proportion of individuals in this group caring for a spouse or partner, compared with g/l caregivers, as previous studies suggest that spousal and partner caregivers often experience poorer physical and mental health outcomes than non-spouses/partners. 21
Unexpectedly, we found that perceived stress was positively associated with global health and this association differed between bi+ and g/l caregivers. Higher perceived stress scores predicted worse global health for bi+ caregivers, yet higher perceived stress scores predicted better global health for g/l caregivers. While we did not examine social connection in the current study, one possible explanation for this finding could be related to differences in social connection between the two groups. For example, g/l caregivers in our sample who report high levels of stress may turn to LGBTQ+ community-serving organizations for support and social engagement. Programs offered by LGBTQ+ community-serving organizations are often tailored to g/l individuals, with limited offerings specifically designed for bi+ community members. 45 These types of supportive services and connection with other LGBTQ+ community members are protective and can help mitigate the negative effects of stress on health. 35 It is possible that the bi+ caregivers in our sample who are experiencing high levels of stress may have less access to LGBTQ+ community connections and, therefore, may not be reaping the potential protective reward of such engagement, a disparity suggested in previous studies.35,36,39
There are important research and practice implications that should be considered based on our findings. At the time of writing, research funding for LGBTQ+ health in the U.S. is under threat, posing a significant barrier to advancing knowledge about bi+ individuals, including those providing care to persons living with ADRD. 46 Researchers must continue to identify ways to conduct research, which includes data collection efforts that incorporate inclusive measures that are able to capture the diverse experiences of all LGBTQ+ subgroups at a time when public health infrastructure supporting such efforts is being abrogated. Continuing LGBTQ+ health research efforts is critical for informing best practices and developing evidence-based policies aimed at eliminating LGBTQ+ health disparities. Additional research is critically needed to develop new measures and adapt existing ones to accurately reflect the lived experiences of LGBTQ+ caregivers. Furthermore, it is imperative that practitioners working with bi+ populations, including those who are ADRD caregivers, are educated on the unique ways in which minority stress influences caregiving experiences and health. By fostering a safe and affirming environment, providers can more effectively support bi+ clients and patients. Moreover, providers should play an active role in advocating for inclusive practices and policies across the broader health care system and within community-based programming, including LGBTQ+ centers. It may be beneficial for LGBTQ+ community health centers to routinely assess the existence and effectiveness of their bi+-inclusive policies and programming, adjusting as needed to ensure bi+ individuals are included, supported, and represented.
Limitations
Given that we used a secondary analysis of existing data, our analysis was subject to certain limitations related to the data collected and measures used by the original study. As such, we were unable to assess the influence of LGBTQ+ community connection or the gender of the caregiver’s partner or spouse on the associations tested. Furthermore, the cross-sectional nature of the data limited our ability to examine how minority and caregiving stressors may change over time; therefore, we were unable to assess causality. Our sample of ADRD caregivers was restricted to individuals with internet access and the ability to navigate the online survey platform, which may preclude generalizability. Study materials were only available in English and therefore the results reflect the experiences of English-speaking caregivers only and may not be representative of non-English-speaking populations. Finally, our classification of bi+ participants was restricted to the only survey item that assessed sexual orientation, as there were no survey items that queried sexual attraction or behavior. Future research should employ multidimensional measures of sexual orientation (ie, identity, attraction, and behavior) to more comprehensively capture research participants who may not self-identify as one of the sexual orientation identities we used to conceptualize the bi+ caregivers study group. Despite these limitations, this study makes an important contribution to the literature by highlighting limitations in existing caregiving measures, many of which likely fall short in capturing the lived experiences of gay, lesbian, and bi+ ADRD caregivers and especially are lacking in attention to nuanced subgroup differences in measurement.
Conclusion
This study sheds much-needed light on bi+ ADRD caregivers, a population often overlooked in caregiving and LGBTQ+ health research, highlighting their distinct experiences with minority stress, caregiving, and health. These findings underscore the importance of disaggregating sexual minority groups in caregiving and health research. Study results emphasize the need for inclusive and affirming interventions that address the specific challenges bi+ caregivers face and are specifically tailored to the needs of bi+ ADRD caregivers so they can remain in their caregiving roles while also maintaining their own health and well-being. Although LGBTQ+ health research is at risk, research must hold steady, while also being thoughtful of using appropriate measurement that reflects the lived experiences of bi+ ADRD caregivers, a twice hidden population.
Footnotes
Ethical Considerations
The University of Tennessee-Knoxville Institutional Review Board reviewed and approved the original study design and procedures.
Consent to Participate
Study participants provided electronic indication of consent (i.e., consent implied by completing the survey).
Author Contributions
Krystal R. Kittle conceptualized and designed the study, led the development of the analytic plan, interpreted the data, and drafted the initial and final versions of the manuscript. She coordinated co-author input, integrated revisions, and takes full responsibility for the integrity and accuracy of the data analysis and reporting. As co-first author, Ethan C. Cicero, also helped conceptualize and design the study and made substantial contributions to data analysis and and led the creation and formatting of all tables. Dr Cicero also participated in the interpretation of findings and made valuable editorial contributions throughout the writing process. Joel G. Anderson shared these private data with Krystal R. Kittle for the purpose of secondary data analysis for this publication. Dr Anderson utilized his knowledge and expertise with participating in interpreting the results and making valuable editorial contributions throughout the writing process. Jason D. Flatt contributed to the interpretation of study findings and provided substantive editorial input that strengthened the clarity and coherence of the final manuscript. Jordan Pelkmans advised on data analysis and reporting as well as the interpretation of findings.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging [R03AG058528; R01AG083177; K23AG084851], Alzheimer’s Association [AARF-22-927069 and 23AARGD-NTF-1028973]. The statements in this article are solely the responsibility of the author and do not necessarily represent the views of the Alzheimer’s Association or the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.