
Abstract
The focus of this article is to discuss the application of cognitive-behavioral therapy and interpersonal therapy with a 65-year-old woman experiencing depressive symptoms and complicated grief associated with a brain injury and an acquired disability. Findings indicate the intervention, which consisted of 20 sessions, produced significant clinical improvement in depressive symptoms as measured by the Geriatric Depression Scale as calculated by the Reliable Change Index. Cognitive-behavioral techniques, such as cognitive restructuring and behavioral activation, were modified according to the client’s cognitive functioning and physical abilities. Interpersonal therapy techniques were used to examine current relationships and grief related to the acquired brain injury.
Keywords
1 Theoretical and Research Basis for Treatment
Geriatric depression is a well-documented phenomenon, which falls under the category of Mood Disorders in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000; Laidlaw, 2001). However, depression is not a process of normal aging (Zarit & Zarit, 2007). Laidlaw and McAlpine (2008) argued that older adults have unique experiences, including death anxiety, bereavement, and role-loss due to retirement or disability, which increase the likelihood of depressive symptoms. According to Segal, Qualls, and Smyer (2011), physical illness and institutionalization are additional risk factors for depression. Furthermore, cognitive impairment and dementia are often comorbid with depression in older adults (Steffens & Potter, 2008).
According to the DSM-IV-TR (APA, 2000), to meet criteria for a major depressive episode (MDD), an individual must experience at least five out of nine symptoms nearly every day for at least 2 weeks. Approximately 5 million older adults living in the United States meet criteria for a depressive disorder (Moss & Scogin, 2008). The number of older adults diagnosed with depression has steadily increased as the population continues to age. Between 1992 and 1998, the percentage of Medicare enrollees who were formally diagnosed with major depression increased from 2.8% to 5.8% (Crystal, Sambamoorthi, Walkup, & Akincigil, 2003). Recent studies of Medicare enrollees suggested as many as 25% of older adults have one or more symptoms of major depression (McCall, Parks, Smith, Pope, & Griggs, 2002; Waldo, 2004). Women are twice as likely as men to be diagnosed with depression in late adulthood (Garber & Flynn, 2001, as cited in Fisher, Cucciare, DroBel, & Yury, 2006; Nolen-Hoeksema, 2001). It has been hypothesized that the prevalence rates of depression between men and women differ due to biological factors such as genetics and hormones, as well as psychological and social factors, including gender roles, help-seeking behavior, vulnerability to victimization, and coping styles (Nolen-Hoeksema, 2001; Parker & Brotchie, 2010; Piccinelli & Wilkinson, 2000).
Cognitive-behavioral therapy (CBT) is an evidence-based therapy for geriatric depression based on the criteria developed by Division 12 of the American Psychological Association (Fisher et al., 2006; Laidlaw, Thompson, & Gallagher-Thompson, 2004; Scogin, Welsh, Hanson, Stump, & Coates, 2005). Laidlaw and McAlpine (2008) stated that CBT is a useful treatment for geriatric depression because it is present-focused and involves changing thoughts and behaviors that are currently maintaining or exacerbating the depressive symptoms. Satre, Knight, and David (2006) conducted a thorough literature review describing the efficacy of CBT for geriatric depression and concluded CBT is beneficial in resolving psychological issues related to disability and insomnia. Meta-analyses of interventions for older adults support CBT as an evidence-based treatment for depression (Pinquart, Duberstein, & Lyness, 2007; Pinquart & Sorensen, 2002). In addition, CBT has been demonstrated to be as effective as medication in treating geriatric depression with the added benefit of lasting effects after treatment has ended (Hollon et al., 2005).
The cognitive component of CBT is based on the premise that negative thoughts and cognitive errors can create a set of beliefs that can lead to symptoms of depression (Beck, Rush, Shaw, & Emery, 1979). Therefore, cognitive therapy can be useful in challenging maladaptive thought patterns to alleviate depressive symptoms. Behavioral activation (BA) is an integral part of CBT for depression and focuses on changing behaviors that maintain escape and avoidance and exacerbate symptoms (Dimidjian, Martell, Addis, & Herman-Dunn, 2008). BA is an effective treatment for geriatric depression (Yon & Scogin, 2008) that involves modifying behaviors to increase opportunities for the individual to receive positive reinforcement (Hopko, Lejuez, Ruggiero, & Eifert, 2003; Moss & Scogin, 2008).
Similar to CBT, interpersonal psychotherapy (IPT) is a brief, present-focused, and evidence-based treatment for late-life depression and grief (Weissman & Markowitz, 1994, as cited in Bleiberg & Markowitz, 2008). According to Karel and Hinrichsen (2000), IPT is “well-suited” and requires “little adaptation for older adults” (p. 715). A recent meta-analysis supports IPT as an effective treatment for depression (Cuijpers et al., 2011). In another study, 74% of older adults who received outpatient IPT significantly reduced their depressive symptoms (Hinrichsen & Clougherty, 2006). It is important to note that a major limitation of efficacy research for IPT with older adults is the inclusion of participants on antidepressant medication in all of the studies (Arean & Cook, 2002).
Unlike CBT, which focuses on behaviors and thoughts, IPT focuses on personal relationships, which may affect the client’s distressing symptoms. From an IPT perspective, depressive symptoms are associated with a relationship or an event (Bleiberg & Markowitz, 2008; Hinrichsen, 2008). This is especially important for clients experiencing grief and loss. Hinrichsen and Clougherty (2006) stated that IPT is a useful intervention in helping clients work through feelings associated with bereavement by focusing on the creation of new relationships.
Rumination is described as “engaging in a passive focus on one’s symptoms of distress and on the possible causes and consequences of these symptoms” (Nolen-Hoeksema & Jackson, 2001, p. 37). There is a positive correlation between depressive rumination and depression (Kirkegaard Thomsen, 2006; Nolen-Hoeksema, Wisco, & Lyubomirsky, 2008). Rumination about loss is an avoidant and maladaptive coping strategy that can maintain and exacerbate grief (Stroebe et al., 2007). Nolen-Hoeksema et al. (2008) posited that “rumination maintains and exacerbates depression by enhancing negative thinking, impairing problem solving, interfering with instrumental behavior, and eroding social support” (p. 401). Therefore, CBT and IPT may be effective in treating depressive rumination (Nolen-Hoeksema et al., 2008).
Depression is common among individuals who have experienced brain injuries (Bessell, Watkins, & Williams, 2008; Fleminger, Oliver, Williams, & Evans, 2003) and strokes (Whyte & Mulsant, 2002). Individuals with traumatic brain injuries may experience rumination in the form of thinking about preinjury functioning and feelings of guilt or blame surrounding the injury (Bessell et al., 2008). Ruddle, Coetzer, and Vaughan (2005) claimed that models of grief for death-related bereavement are applicable to individuals experiencing disability due to a brain injury.
Prolonged grief and bereavement may lead to depression and impairment in functioning (Stroebe et al., 2007). The proposed diagnosis of complicated grief for the DSM-V requires the individual to have experienced at least four of the following eight symptoms at least several times a day for at least 6 months: trouble accepting the loss, feeling uneasy about moving forward, feeling life is currently meaningless without the deceased, feeling agitated since the loss, excessive bitterness related to the death, inability to trust others, detaching from friends and family after the loss, and feeling as if the future life will not be meaningful without the deceased (Prigerson et al., 1996, as cited in Zhang, El-Jawahri, & Prigerson, 2006). It is important to note complicated grief is different from bereavement and is more strongly associated with suicidal ideation (Szanto et al., 2006). Stroebe et al. (2007) argued ruminating on the loss of a loved one is associated with denial and the suppression of negative thoughts and feelings rather than coping.
Evidence-based guidelines indicate cognitive therapy is effective in treating aspects of complicated grief such as trouble accepting the loss and reframing thoughts of hopelessness (Regehr & Sussman, 2004; Zhang et al., 2006). BA is another effective strategy for treating complicated grief (Boelen, 2006). Shear and Frank (2006) stated CBT and IPT are effective for treating complicated grief; however, they did not specifically address older adults.
In summary, CBT and IPT have been shown to be effective treatments for geriatric depression, rumination, and complicated grief. In addition, both approaches are an appropriate treatment for individuals with cognitive impairment. In the literature, several authors discussed the theoretical rationale of combining CBT and IPT to treat children and adolescents with depression (Spence & Reinecke, 2003) and adults with somatoform disorders (Stuart, Noyes, Starcevic, & Barsky, 2008). Other authors have argued that CBT and IPT should be integrated for culturally competent therapy with Latino adults (Perez & Phil, 1999). Presently, there are no published studies on this topic involving older adults. This case study combines the two theoretical approaches to treat complicated grief and depression in an older female client.
2 Case Introduction
At the initial assessment, Ms. White (pseudonym) was a 65-year-old single, college educated, heterosexual, Caucasian female who resided in a long-term care facility in an urban area in the Northwest. Approximately 5 years prior to presenting for treatment, Ms. White had a large, 7 cm, benign meningioma near the right temporal region of her brain and a series of subsequent strokes during a surgical procedure to remove the tumor. As a result of complications from the surgery, Ms. White experienced hemiplegia on the left side of her body, cognitive impairment, and speech disturbances. Ms. White was unemployed due to disability and her main source of income was supplemental security insurance.
3 Presenting Complaints
Ms. White was referred to outpatient individual therapy by a social worker at the long-term care facility where she resided since her stroke. The social worker noted that 6 months prior to intake, Ms. White became increasingly more tearful. Ms. White spoke of her second ex-husband every time staff or residents were nearby, which led to social alienation. Ms. White reported a tendency to overeat when feeling sad and felt criticized by staff and residents for gaining weight. Ms. White stated she wanted to reunite with her second ex-husband but was unsure of the reason he had not responded to her multiple phone calls or letters over the past 5 years. She believed his parents might be responsible for keeping them apart. The nursing home staff reported Ms. White’s second ex-husband filed a restraining order in an attempt to reduce the number of unwanted phone calls.
Ms. White stated her goal was to move to a lower level of care and to have more independence; however, due to her noncompliance with physical therapy and tendency to overeat when she felt sad, her weight had increased along with her level of disability. Ms. White required two nurses to transfer her from her bed to her wheelchair and therefore did not qualify for a lower level of care.
4 History
Ms. White grew up in the Western region of the United States. She was the youngest of three sisters; however, she had not been in contact with them for several years due to their frustration with her desire to be with her second ex-husband. She had a good relationship with her parents and siblings throughout childhood and adulthood. Ms. White reported that her father died approximately 3 years ago. She had weekly phone contact with her mother who lived 2 hr away.
Ms. White had been married twice and divorced twice. Her first marriage lasted 20 years and she had two adult children with her first husband. Her children did not live in the area but were in frequent phone contact and would occasionally visit her on her birthday. Her second marriage lasted 12 years and ended 5 years ago, approximately 3 months before her brain surgery. Ms. White reported she was also in frequent telephone contact with her first ex-husband, but had no relationship with her second ex-husband.
Ms. White received her master’s degree in biology and taught courses at the community college level prior to her surgery and stroke. Nursing home records indicated Ms. White was diagnosed with diabetes, obesity, and a history of transient ischemic attacks. Ms. White was on multiple medications to control her diabetes as well as blood thinners to reduce the risk of another cerebrovascular accident. Ms. White had been on a low-dose SSRI antidepressant for several years for depression.
Ms. White reported her depressive symptoms have existed since the time of her surgery and stroke; however, this was the first time she had sought counseling for any mental health condition. She denied any previous episodes of depression or sadness prior to her surgery. She had support from friends and family when she was initially in the hospital; however, this slowly “faded” approximately 1 year post stroke. Ms. White denied previous or current drug or alcohol use. During the initial interview, Ms. White denied current or past legal issues; however, the nursing home records and staff reported a restraining order was on file to prevent Ms. White from contacting her second ex-husband due to harassing phone calls.
5 Assessment
Diagnosis
Ms. White met criteria for MDD as evidenced by Ms. White’s self-report of depressed mood, suicidal ideation, decision-making difficulties, anhedonia, and hopelessness (APA, 2000). Ms. White appeared to have poor judgment and limited insight as demonstrated by unrealistic and obsessive expectations, lack of understanding of the purpose or meaning of the restraining order, and inability to abstract possible reasons why her second ex-husband had not contacted her in 5 years. During the intake interview, she endorsed suicidal ideation and feelings of hopelessness. Although Ms. White may have initially experienced bereavement over the loss of the relationship with her ex-husband or difficulty adjusting to her acquired disability, she reported her symptoms were becoming more distressing and had persisted for several years.
A formal assessment of Axis II was not conducted. Ms. White had several medical conditions, including obesity, diabetes, and a history of strokes. Ms. White experienced impairment in several areas of her life, including with her primary support system and her social environment. At intake, Ms. White’s Global Assessment of Functioning (GAF) score was between 31 and 40, as evidenced by impairment in reality testing and impairment in several areas, including work, judgment, thinking, and mood. It was not clear whether Ms. White’s cognitive impairment was a result of stroke, atrophy of brain tissue due to the size of the meningioma tumor, or removal of brain tissue during the surgical procedure.
Based on the anticipated DSM-V criteria, the diagnosis of complicated grief may be a future consideration for Ms. White (Prigerson et al., 1996, as cited in Zhang et al., 2006). At intake, Ms. White experienced significant impairment in her daily functioning for the past 5 years as a result of her multiple losses. She stated life was not worth living if she could not be with her second ex-husband and expressed great frustration with the idea that she was unable to hear his voice or contact him. During the intake assessment, she stated she did not want to move on because she believed he would return to her one day.
Assessment Tools
Ms. White was a client at the local community mental health agency where the clinician was working as a master’s level practicum student under the supervision of a licensed clinical social worker. The assessment was conducted using a semistructured interview form supplied by the agency, and Ms. White was diagnosed using the criteria outlined in the DSM-IV-TR (APA, 2000). No formal assessment tools or structured questionnaires were used during the assessment.
Geriatric Depression Scale
The Geriatric Depression Scale (GDS) is a screening tool designed to identify depressive symptoms in older adults, which consists of 30 self-report items that require a yes/no dichotomous response. A major strength of the GDS is the ease with which counselors can administer and score the test as one point is given for each response that indicates positive symptoms of depression. The cutoff scores for the GDS are as follows: normal = 0 to 9, mild depressive symptoms = 10 to 19, and severe depressive symptoms = 20 to 30 (Yesavage et al., 1983).
The GDS has been validated in older adults with mild cognitive impairment (Debruyne et al., 2009). The GDS has demonstrated internal consistency (α = .94) and test–retest reliability (r = .85; Yesavage et al., 1983). Therefore, the GDS was an ideal screening tool to monitor depressive symptoms throughout the course of treatment.
Saint Louis University Mental Status Examination
The Saint Louis University Mental Status Examination (SLUMS) is a brief cognitive screening questionnaire that assesses orientation, memory, attention, and executive function. In a recent pilot study, the SLUMS was more sensitive than other brief cognitive tests in the identification of mild neurocognitive impairment (Tariq, Tumosa, Chibnall, Perry, & Morley, 2006).
6 Case Conceptualization
Ms. White’s depressive symptoms appeared after her brain surgery approximately 5 years ago. After her life-altering surgery and stroke, Ms. White experienced prolonged grief and negative thoughts about herself and her future without her second ex-husband, which led to feelings of sadness and emptiness. As a result of the stroke, she exhibited cognitive impairment, which may contribute to her depressive thoughts and feelings. From a CBT perspective, Ms. White’s depressive rumination about life with her second ex-husband prior to the surgery served as a means of avoiding negative thoughts and emotions. Her frequent phone calls to her second ex-husband also served as avoidance of painful emotions, as she would attempt to call him when she became overwhelmed with loneliness and sadness.
The long-term effects of these thoughts and behaviors further contributed to her grief and depression. In social settings, Ms. White talked about her ex-husband without regard to the topic of conversation, which resulted in peers avoiding her or insulting her. This added to her depressive thoughts and increased her isolative behaviors.
Ms. White’s avoidant behavior prevented her from participating in activities she used to enjoy, thereby, decreasing her access to positive reinforcement. The counselor worked with Ms. White to identify avoidant behaviors such as emotional eating, ruminative thoughts about reuniting with her ex-husband, and disengaging from activities. Admission to the long-term care facility provided Ms. White with a necessary level of care, but it also restricted her access to familiar environmental reinforcement. For example, she repeatedly asked the nursing home staff to drive her to nearby restaurants and craft stores, as these were places she routinely went before her stroke. Ms. White acknowledged that listening to sad songs caused her to experience feelings of sadness and loneliness, which led to prolonged crying episodes. Ms. White had some insight to her behaviors and reportedly coped with her negative emotions by overeating or attempting to contact her ex-husband by phone. These behaviors were maintained by instant gratification and temporary relief from the negative emotions experienced by Ms. White.
IPT focuses on role transitions, grief, and interpersonal deficits (Hinrichsen, 2008). Prior to her stroke, Ms. White had generally secure attachments and few interpersonal problems. She experienced several role transitions after her surgery, including the transition into a nursing home and adjusting to an acquired disability. From an interpersonal therapy perspective, Ms. White had not been able to process her grief adequately and had not established new relationships due to interpersonal deficits. The most salient interpersonal deficits for Ms. White included the preoccupation over the loss of the relationship. She acknowledged the only time she reached out to other people was to solicit help to contact him. Therefore, the goals of the therapy were to facilitate the mourning process, teach social skills, and encourage Ms. White to establish new relationships that were reciprocal in nature and based on common interests.
7 Course of Treatment and Assessment of Progress
Course of Treatment
Treatment consisted of twenty 50-min individual sessions. The first seven individual therapy sessions were conducted at the nursing facility where Ms. White resided. As Ms. White began to report fewer symptoms of depression, the location of the sessions changed to the mental health clinic. Traveling outside of the facility served as a behavioral intervention by increasing access to rewards in the form of interactions with different individuals and providing independence and autonomy outside of the facility (Dimidjian et al., 2008).
Ms. White’s counselor was a student intern from a local master’s-level counseling psychology program with training in CBT. The counselor received weekly supervision by a licensed clinical social worker specializing in geriatric mental health. Treatment consisted of individual techniques from a cognitive therapy model for depression outlined by Young, Rygh, Weinberger, and Beck (2008) and BA model for depression as outlined by Dimidjian et al. (2008). Therapy was modified to incorporate IPT interventions, as described by Bleiberg and Markowitz (2008) as well as Hinrichsen and Clougherty (2006), to address aspects of complicated grief and depression. A summary of the components of CBT and IPT used in this case study is presented in Table 1.
Components of CBT and IPT Used in Treatment of Geriatric Depression With Complicated Grief
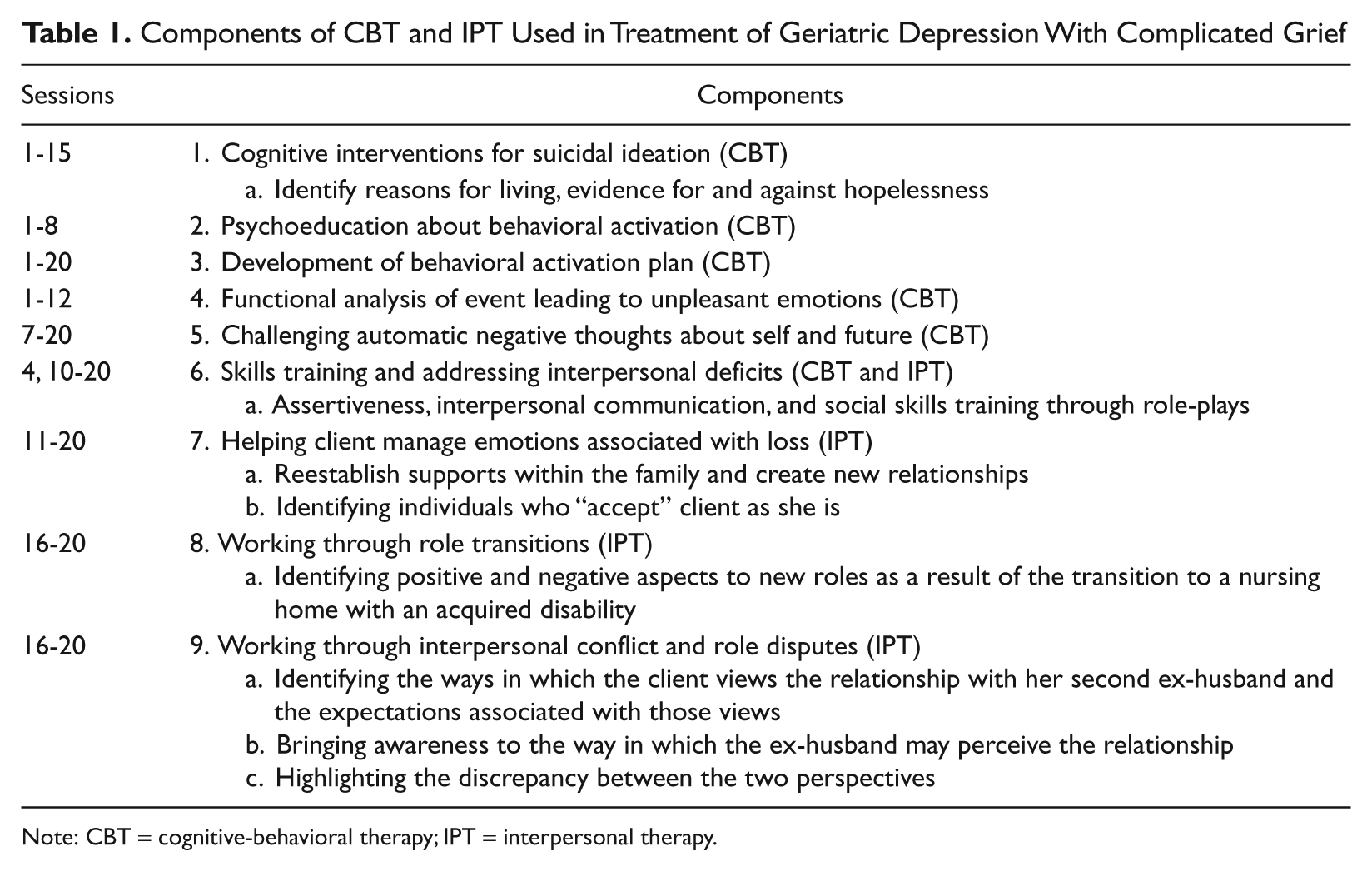
Note: CBT = cognitive-behavioral therapy; IPT = interpersonal therapy.
The main treatment goals associated with administering CBT included reduction in the severity and frequency of depressive thoughts and avoidant behaviors. Once Ms. White’s depressive symptoms improved, IPT was used to address issues of complicated grief associated with multiple losses in her life (i.e., loss of relationship, and loss of physical and cognitive functioning). Ms. White attended a weekly process group for older adults with depression cofacilitated by her counselor.
Sessions 1 to 4
The first four sessions with Ms. White involved rapport building and education on BA and sleep hygiene. The counselor assisted Ms. White in identifying sources of support and creating a safety plan she could enact when her suicidal thoughts increased in intensity or frequency. She did not endorse intent or a plan for completing suicide at the time.
During the fourth session, she stated she had been repeatedly criticized regarding her weight by nursing home staff. The counselor validated her feelings of sadness and frustration for being criticized and highlighted the relationship between Ms. White’s goal of moving to a lower level of care and the ways in which her behaviors (i.e., overeating, lack of compliance with physical therapy, and occupational therapy) could be barriers to reaching her goals. Ms. White and the therapist then engaged in a role-play to practice skills to talk to staff members when they expressed criticism.
Sessions 5 to 8
Ms. White continued to endorse suicidal ideation at least once per week during the second month of treatment. She reported her plan would be to hide her medication and take all of it at once because it was the only lethal method she could access. With a signed release of information, the counselor spoke with nursing home staff and her social worker, and a safety plan was enacted. Through the use of cognitive therapy techniques, Ms. White was able to identify reasons to live, which included her children and the incompatibility of suicide with her religious beliefs.
In Session 6, Ms. White reported crying most of the day while listening to sad songs on the radio. However, she reported she had started attending church several times a week and she was using her creativity to write a brief article on growing small plants in nursing homes. She reported multiple attempts to contact her second ex-husband by phone during this time, which resulted in disappointment because he disconnected the call when he heard her voice. Ms. White continued to demonstrate limited insight as evidenced by her inability to understand any reasons why he would hang up on her.
During the seventh session, the counselor began to examine many of Ms. White’s thoughts associated with her depression and grief. Ms. White often stated, “I am a burden to my family.” The counselor used cognitive restructuring and other CBT techniques to refute this thought (i.e., “Is there any evidence this is true?” and “If they have not directly said this, is it possible they do not feel that you are a burden?”). Ms. White responded positively to this intervention by noting she might be projecting her feelings onto her family members.
The eighth session was conducted at the community mental health clinic. The discussion focused on the client’s multiple losses and main stages of grief. Ms. White reported she was still in “shock” over the discovery of the tumor stating, “All of the sudden I lost my health, my job, my car, and my man.” She stated, “I often wonder what I have to live for.” When asked what she would tell someone in a similar situation, Ms. White replied, “It takes time and involves really painful feelings, but it will be okay.” Ms. White stated she was beginning to feel less depressed and could find several positive aspects of her life.
Sessions 9 to 12
The following month of treatment was difficult for Ms. White as it was December and she had been listening to “sad Christmas music.” Around the time of the ninth session, she was taken to the emergency room of a local hospital by ambulance because she was unresponsive in her wheelchair at the facility where she resided. The hospital records indicated she lost consciousness due to extremely high blood sugar levels. She had eaten several jelly doughnuts at church and did not tell the staff members at the facility because she felt they would criticize her. She stated, “I cannot bear to live without him and I can’t have him and now I can’t have food.” At this time, she endorsed suicidal ideation but did not specify a plan or intent citing her religion as a protective factor against self-harm.
Ms. White acknowledged using food, which was abundant during the holiday season, to cope with feelings of sadness and loneliness. The counselor worked with Ms. White to identify individuals she could call or talk to if she was feeling sad instead of turning to food for comfort. During the 10th session, Ms. White exhibited a remarkable change in affect. She was not tearful in session and she reported that she had not been crying as frequently. She stated she was calling one of her sisters when she needed someone to talk to or she would leave her room and move around the facility in her wheelchair or talk with other residents at the facility. At this time, she returned to the hospital for evaluation for confusion and altered consciousness due to ischemic strokes.
In session, Ms. White began to reexamine her interpersonal relationships and to develop assertiveness skills through role-play. Ms. White began to draw boundaries with her roommate by telling her roommate to turn the radio off when the music began to affect her mood. Ms. White also told family members she felt depressed and ways they could be supportive.
Sessions 13 to 16
The focus of the next four sessions involved finding adaptive ways of coping with sadness and challenging maladaptive thoughts regarding her second ex-husband. In the 13th session, Ms. White reported she had successfully located an individual at church who would call her ex-husband to offer him a job in the construction industry. The counselor and Ms. White reviewed motivations for asking another person to call her ex-husband. Ms. White initially stated she wanted to help him find a job, then after some discussion, she acknowledged she was not sure whether he needed a job or was still in the construction industry. Eventually, Ms. White stated she wanted him to move to the same location so he could “rescue” her from her situation.
During the 15th session, Ms. White stated she was still thinking about her ex-husband for several hours each day and hoping he would send her a valentine. The counselor and Ms. White worked collaboratively to generate ideas for staying busy and celebrating the Valentine’s Day holiday in a more productive way than ruminating (e.g., by giving cards to family and friends).
The final intervention in this treatment phase consisted of helping Ms. White identify evidence for and against her beliefs about her current and future relationship with her second ex-husband. Ms. White stated she believed he may still be interested in her but she could not be sure due to the fact he had not contacted her in 5 years. The counselor worked with Ms. White to challenge some of those ideas through questions such as “How much time would need to pass before the distinction could be made between ‘still interested’ and ‘perhaps he has moved in a different direction in his life’?” Ms. White replied, “I don’t know, I haven’t thought about that before.” This led to a discussion about drawing boundaries and establishing a realistic time frame in which Ms. White stated she would “know it is time to move forward.”
Sessions 17 to 20
The focus of the final four sessions shifted to Ms. White’s prolonged grief over her multiple losses. She expressed interest in learning how to “move forward.” Ms. White stated she was feeling less depressed and had not cried for several weeks. The counselor prompted Ms. White to identify aspects that have helped her cope with the losses up to this point and people in her life who accept her for who she is at the moment. Ms. White stated she “finally” recognized her second ex-husband was not willing to accept her in her current condition, which she acknowledged was “painful, but necessary to heal.” During the final sessions, Ms. White stated she was meeting new friends at church and her life was “heading in a positive direction.”
Assessment of Progress
Ms. White’s scores on the outcome measures at pretreatment and posttreatment are presented in Table 2. At pretreatment, her score on the GDS was 28, indicating severe depressive symptoms and at posttreatment her score was 10, indicating mild depressive symptoms (see Table 2).
Scores on the Geriatric Depression Scale at Pretreatment, Posttreatment, and 3-Month Follow-Up
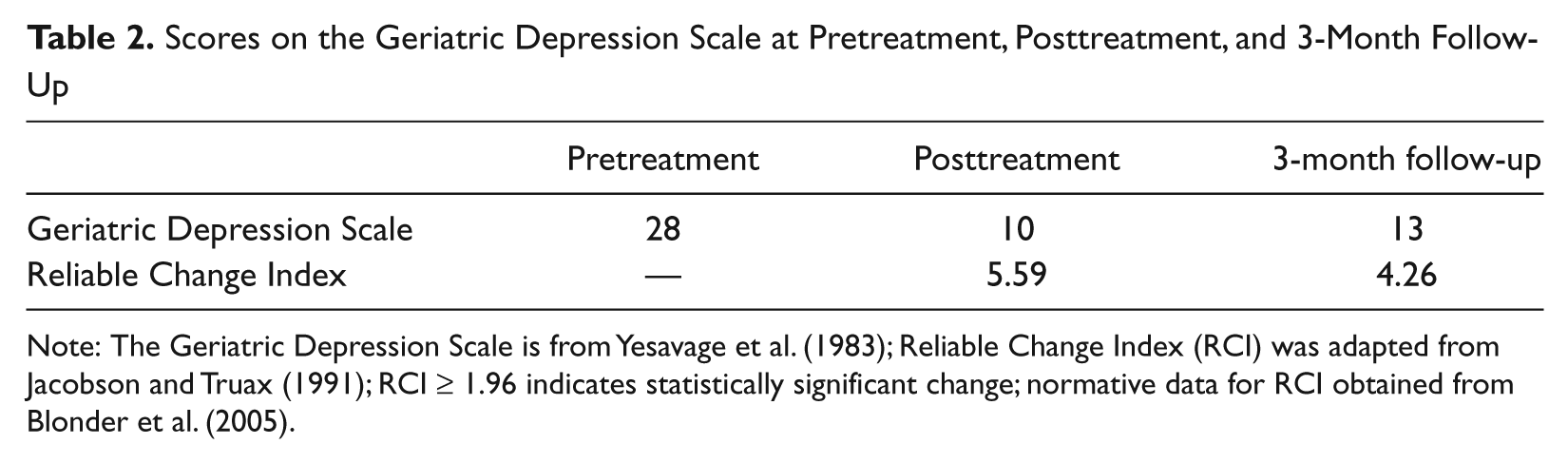
Note: The Geriatric Depression Scale is from Yesavage et al. (1983); Reliable Change Index (RCI) was adapted from Jacobson and Truax (1991); RCI ≥ 1.96 indicates statistically significant change; normative data for RCI obtained from Blonder et al. (2005).
The Reliable Change Index (RCI) is a statistic used to determine whether the difference between pretreatment and posttreatment scores is clinically significant (Jacobson & Truax, 1991). In this case, normative GDS data were obtained from a study with individuals 2 years post stroke with an average age of 61.5 (SD = 11.96) and an average of 13.52 (SD = 2.69) years of education (Blonder et al., 2005). Ms. White’s change in GDS scores between pretreatment and posttreatment were statistically significant (RCI = 5.59). For further information on calculating RCI, review Jacobson and Truax (1991).
The SLUMS was administered on three different occasions to screen for cognitive impairment, and Ms. White scored within the “mild-neurocognitive impairment” range each time. Consistently, Ms. White showed difficulty with executive functioning, numerical calculation, and orientation to the current year.
Ms. White appeared less tearful over the course of treatment and became increasingly involved at the facility by attending activities and resident council meetings. She wrote an article for the facility newsletter and stated it was helpful in reducing her depressive symptoms because it “helped people.” At the time of termination, Ms. White reported fewer interpersonal conflicts with her roommate and a better relationship with her children. Ms. White stated she learned to cope with her feelings of loss and sadness over her acquired disability as well as grief associated with the loss of relationship. She stated she would always care for her second ex-husband but no longer hoped to reunite with him.
8 Complicating Factors
The first seven therapy sessions were conducted in Ms. White’s room at the long-term care facility when her roommate was not present. Challenges associated with conducting therapy in long-term care settings include privacy and interruptions from staff. However, conducting therapy in the client’s natural environment can provide valuable information about behavior in context and interpersonal functioning. A recent case study conducted with an older female with depression demonstrated the importance of being flexible to the needs of older adults in terms of the location where therapy is conducted (Maxfield & Segal, 2008).
Authors of another case study highlight difficulties with treating a depressed individual with ongoing medical issues in a long-term care setting (Meeks, Teri, Van Haitsma, & Looney, 2006). Ms. White had several health-related problems during the course of treatment. Around the time of the ninth session, Ms. White was found unresponsive at church and taken to the hospital with extremely high blood sugar. The following week, Ms. White’s social worker noticed a change in her mental status. According to Ms. White, she was taken to the hospital for several MRI and CAT scans earlier in the week because she was losing consciousness. The laboratory and radiology reports from this time period were inconclusive, but her physician believed she was experiencing transient ischemic strokes. Individuals who have experienced an intercranial or brain tumor are at a greater risk for ischemic strokes, which can complicate treatment for depression (Kreisl, Toothaker, Karimi, & DeAngelis, 2008).
The degree to which Ms. White’s brain injury complicated treatment remains unclear. As Grief and Myran (2006) highlighted, there is little research on how individuals with cognitive impairment experience grief. Temporal lobe damage is associated with difficulties with speech, persistent talking, impaired organization of verbal material, difficulty consolidating memories, and impaired processing of information (Kolb & Whishaw, 2008). Although Ms. White exhibited cognitive impairment, she was able to make significant changes in her behaviors, thought patterns, and interpersonal relationships.
9 Access and Barriers to Care
One of the most challenging managed care concerns involved the use of medical transportation to bring Ms. White to the clinic for treatment. For every session, it was necessary to obtain an authorization for medical necessity from Medicaid and to coordinate with Ms. White’s facility to ensure she would be ready when medical transportation arrived.
10 Follow-Up
Ms. White continued to attend weekly group therapy after the termination of individual therapy. After 3 months, one 50-min session was scheduled as a follow-up. She stated she was dating a man who resided at her facility. She denied suicidal ideation and stated she had “a lot to live for.” At the follow-up appointment, her GDS score was 13, which falls in the moderately depressed range. The change in GDS scores between pretreatment and 3-month follow-up were statistically significant (RCI = 4.26; see Table 2).
11 Treatment Implications of the Case
This case illustrates the integration of CBT and IPT to treat depression associated with complicated grief in an older adult with an acquired brain injury. The rationale for the therapeutic intervention was based on evidence that suggests CBT and IPT are effective treatments for depression and grief and are appropriate for older adults with cognitive impairment (Bleiberg & Markowitz, 2008; Dimidjian et al., 2008; Karel & Hinrichsen, 2000; Regehr & Sussman, 2004; Scogin et al., 2005; Young et al., 2008). The interventions were originally developed as components of manualized treatments but, in this case, were employed independently. As this case study highlights, a CBT and IPT package may be an effective treatment for some older adults; however, further research is needed. A previous case study was also successful in combining aspects of CBT and ACT to treat chronic pain in an older adult (Lunde & Nordhus, 2009). These studies provide some evidence that a combination of treatments may be appropriate for treating complex geriatric cases.
In this case, the therapist, client, and staff worked well as a collaborative team, which was important for creating a comprehensive safety plan for Ms. White. With Ms. White’s permission, the therapist and social worker spoke by phone 1 to 2 times per month about her progress in therapy and health status. A recent study by Hyer, Yeager, Hilton, and Sacks (2009) revealed that a combination of group, individual, and staff support for individuals in long-term care is effective in treating depression. Ms. White received individual therapy, group therapy, support from the social worker, and antidepressant medication. Further research is necessary to determine how the working relationship between the staff, therapist, and client affect the treatment.
Segal et al. (2011) raised an important issue regarding the autonomy of clients in long-term care and their ability to decline participation in behavioral intervention techniques. The staff and residents identified Ms. White’s behaviors as problematic; however, the client also endorsed a significant level of distress and suicidal ideation with the cognitive capacity to consent to treatment. It is important for clinicians to consider these issues when working in long-term care.
12 Recommendations to Clinicians and Students
This present case highlights the need to assess for complicated grief associated with acquired disability in older adults presenting with cognitive impairment and depression. In this case, CBT and IPT interventions were effective in producing a clinically significant change in depressive symptoms and resolving issues related to complicated grief.
Footnotes
Acknowledgements
The author would like to thank Laura Heller, LCSW.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.