
Abstract
This is a single-case study of a middle-aged woman with specific phobia and panic symptoms associated with airplanes. Treatment was brief and supportive in nature, using hypnosis for both exposure purposes and as a self-regulatory tool for anxiety management. The patient’s identified target symptom (readiness to fly) was tracked using daily subjective, self-report measures over the 12-session treatment. Simulation modeling analysis for time-series was used to evaluate the level change across baseline, treatment, and follow-up phases. The patient’s self-assessed readiness to fly increased significantly over the course of treatment, and she successfully engaged in a “practice flight” toward the end of her treatment. However, this patient required a drastic shift in treatment modality, after which progress was made. Theoretical rationale for this shift and ultimate success is discussed.
1 Theoretical and Research Basis for Treatment
Specific phobia is defined as a persistent and excessive fear that is triggered by a specific object or situation (e.g., flying). Exposure to the feared object or situation typically provokes an immediate panic response (often including panic attacks), and the individual realizes the excessive nature of their fear. Typically, the feared stimulus is avoided or experienced with marked anxiety. This disorder impairs an individual’s ability to function in his or her daily routine, occupational functioning, or relationships (Diagnostic and Statistical Manual of Mental Disorders [4th ed., text rev.; DSM-IV-TR; American Psychiatric Association {APA}, 2000]). The fear of flying is not a diagnostic category on its own but falls into the situational type, including fears that are triggered by a specific situation (APA, 2000). Fear of flying is one of the most common forms of specific phobia and can include elements of agoraphobia and claustrophobia (Cummings, 1989).
Avoidance in Specific Phobia
Davis and Myers (2002) define anxiety as the fear conditioning and avoidance of stimuli that remind the patient of his or her first panic episode. In fact, avoidance is a standard feature of patients with any type of specific phobia, including that of airplanes (Cummings, 1989). Although patients suffering with specific phobias do tend to avoid the anxiety-provoking stimulus (i.e., an airplane), Goldstein and Chambless (1978) found that phobic patients are not actually afraid of the avoided stimulus, but instead they fear the panic attacks they might have when in those situations. This “fear of fear” theory touches on the agoraphobic element of specific phobias, as patients do not simply avoid a feared stimulus, but they avoid the possibility to experience panic.
Treatment Approaches for Anxiety Disorders and Specific Phobia
Exposure and desensitization
Since the 1960s, systematic desensitization, exposure, and relaxation training have been popular therapeutic techniques with psychiatric patients, particularly those struggling with anxiety disorders (Wolpe, 1961, 1963; Wolpe, Brady, Serber, Agras, & Liberman, 1973; Wolpe & Flood, 1970; Wolpe & Reyna, 1976). Research has continued to support the use of cognitive-behavioral techniques in the treatment of such disorders, as these interventions are currently considered the treatment of choice for anxiety disorders (Barlow, 2002; Block, Kelly, & Carpenter, 2006; Chambless & Hollon, 1998; Dugas et al., 2010; Dugas & Koerner, 2005; Lebrecque, Marchand, Dugas, & Letarte, 2007). Specifically, Davis and Myers (2002) suggest that any successful treatment of anxiety can be thought of as extinction learning, where the patient learns to feel safe in the presence of anxiety-provoking triggers. To achieve this, some researchers have written about the additional benefit of doing work in the actual place or situation that induces anxiety for the patient (Alpers, 2010; Choy, Fyer, & Lipsitz, 2007; Cornelio, Levine, & Wolpe, 1980; Levine & Wolpe, 1980; Ross, 1989; Wolitzky-Taylor, Horowitz, Powers, & Telch, 2008). This in vivo desensitization has obvious advantages; however, as Wilson (1989) astutely notes, patients sometimes strenuously resist physically reentering a feared situation. In such cases, avoidance techniques become a primary “pseudosolution,” and patients learn to rely solely on their ability to avoid.
Wilson also reports the possibility for strained affectations to arise with severely phobic patients. Such themes may include the need to hide one’s anxiety from others, the belief that one must feel no anxiety whatsoever, and the belief that keeping tight control over one’s anxious feelings will prevent those feelings from “running wild” (1989). For Ms. K, these “rules” were organized around issues of power and control. Patients who hold some or all of these rigid beliefs will often resist traditional cognitive-behavioral techniques in the following ways: forgetting, noncompliance, canceled appointments, and attrition (1989). Busch, Milrod, Singer, and Aronson (2011) echo these early findings, asserting that there is a notable percentage of anxious patients who simply do not tolerate the structured techniques used in cognitive-behavioral therapy (CBT) and therefore do not remain in treatment long enough to see results. Kraft (2011) also describes potential patterns of resistance to treatment for phobic disorders, including symptom substitution, increasing psychosomatic manifestations, refusal to actively participate in treatment, intellectualization, and somatization. The issue then becomes this: if traditional cognitive-behavioral techniques are considered the “treatment of choice” for anxiety disorders, yet highly phobic and rigidly avoidant patients tend to resist such techniques, how do we help them get better?
Imaginal exposure and hypnosis
Wilson (1989) posits that imaginal covert exposure has the ability to skirt some of the direct risks of resistance described previously. This treatment approach guides the patient to imagine various experiences, allowing them to gain control over the physical and psychological responses to the feared stimuli. Similarly, Lynn and Kirsch (2006) note that imaginal desensitization is a good starting point for overcoming severe avoidance in anxiety disorders. However, in contrast to the imaginal exposure suggested in the 1980s, Lynn and Kirsch (2006) incorporate hypnosis into the imaginal procedure to enhance the experience of exposure and mastery. Kraft (2011) also discusses the utility of hypnotic techniques to counteract resistance in highly phobic patients, reducing negative transference and giving the patient effective coping strategies for use in the outside world. In fact, a study conducted by Kosslyn, Thompson, Costantini-Ferrando, Alpert, and Spiegel (2000) examined the differences in neurological processes of participants assigned to engage in either hypnosis or mental imagery. Participants were given identical suggestions, but only those assigned to the hypnosis group used hypnotic induction prior to receiving the suggestions. Results of this neuroimaging study showed that when asked to perceive color, only the hypnosis group exhibited activated color areas of the left and right brain hemispheres when shown actual color or a gray-scale stimulus. This work done by Kossyln et al. (2000) suggests that the use of hypnosis in imaginal techniques may enhance the experience of sensory perception.
Sadock and Sadock (2007) describe hypnosis as being useful alone or with other forms of psychotherapy to manage symptoms associated with anxiety. Bryant (2008) also suggests hypnotic strategies with anxious patients, noting that hypnosis can be used to help the patient relax (through muscle relaxation and calming imagery) and also to support imaginal exposure techniques. Baker and Nash (2008) describe in detail how hypnosis may be used in brief, supportive, symptom-focused psychotherapies for the treatment of problems such as pain, smoking cessation, irritable bowel syndrome, anxiety disorders, and skin disorders. They note that normal to neurotic-level patients without severe complicating psychiatric disorders benefit the most from this type of treatment. The specific strategies suggested by Baker and Nash (2008) include the use of hypnosis to strengthen a patient’s existing defenses and to reinforce natural coping strategies by use of gratifying imagery, managing negative affect as it arises, and enhancing a sense of mastery over one’s symptoms.
A key factor in the use of hypnosis for the treatment of anxiety disorders is the introduction and mastery of self-hypnosis (Fromm et al., 1981; Fromm & Kahn, 1990; Lynn & Kirsch, 2006; Sadock & Sadock, 2007). Bryant (2008) describes self-hypnosis as a portable anxiety management tool. Similarly, Nash (2008) identifies self-hypnosis as a technique for self-soothing and symptom containment that can be transferred from the therapy office to everyday life.
Treatment Outcome Research for Hypnosis and Specific Phobia
Recent studies have shown support for the use of hypnosis in the treatment of anxiety disorders (Boutin & Tosi, 1983; Flammer & Bongartz, 2003; Hammond, 2010; Llobet, 2009; Stanton, 1992). However, much of the current literature on hypnosis focuses on physical and emotional components of medical conditions (e.g., Askay, Patterson, Jensen, & Sharar, 2007; Carmody et al., 2008; Elkins, Jensen, & Patterson, 2007; Hammond, 2007; Jensen et al., 2009; Nash & Tasso, 2010; Schnur et al., 2009; Schnur, Kafer, Marcus, & Montgomery, 2008; Spierings & Spierings, 2007) and traumatic experiences (e.g., Ibbotson & Williamson, 2010; Lynn & Cardeña, 2007; Poon, 2007, 2009; Spiegel, 2010). Very little treatment outcome research has been published since the 1990s examining the effectiveness of hypnosis in the treatment of phobias.
Kirsch et al. (1995) conducted a meta-analysis of 18 studies examining CBT alone and CBT with hypnosis in the treatment of a variety of psychological and somatic disorders, including pain, insomnia, anxiety, obesity, hypertension, phobia and ulcers. The findings showed that CBT plus hypnosis led to better outcomes and more gains than CBT alone. Because this meta-analysis included multiple presenting issues, few specific inferences can be made regarding a particular diagnosis. However, the results of this study revealed that the addition of hypnosis to CBT greatly enhanced treatment outcome by approximately 70%. In addition, of the presenting issues examined in this study, phobia was represented and showed marked improvement as a result of the combined CBT and hypnosis treatment approach. Similarly, Schoenberger, Kirsch, Gearan, Montgomery, and Pastyrnak (1997) also found CBT plus hypnosis to be successful in treating social phobia.
O’Neill, Barnier, and McConkey (1999) compared self-hypnosis to progressive muscle relaxation with anxious patients in a randomized study. Both groups displayed significant improvement on anxiety measures; however, the self-hypnosis group experienced greater cognitive changes and perceptions of treatment efficacy. Specifically, those subjects in the self-hypnosis group reported higher expectations for future success, as they showed a greater belief in their ability to manage anxiety. Results from this study lend support for the use of self-hypnosis in treatments focused on relaxation and alleviation of anxiety symptoms.
In addition, there is a vast literature of single-case studies supporting the use of hypnosis in the treatment of anxiety disorders and specific phobias (Byron, 2002; Hill & Bannon-Ryder, 2005; D. Kraft & Kraft, 2010; T. Kraft & Kraft, 2004; Mellinger, 1992; Nolan, 2008; Rogers, 2008).
Single-Case Studies and Time-Series Design
Although most research on the process and outcome of psychotherapy are large-scale randomized controlled studies (RCTs), researchers have argued that the way in which treatments are evaluated could benefit from the insight that can be gleaned from case-based research conducted in typical clinical settings (Peterson, 2004; Westen & Bradley, 2005). The body of literature on psychotherapy process and outcome research has recognized the utility of patient-rated symptom monitoring in single-case (N = 1) designs (Borckardt & Nash, 2008; Borckardt et al., 2008; Nash, Borckardt, Abbas, & Gray, 2011). One notable advantage of time-series design is that it simultaneously addresses effectiveness and process: (a) Does the patient get better? and (b) How does change unfold over time? (Borckardt et al., 2008; Nash et al., 2011). A continuous or daily measures time-series design allows researchers to examine phase effects and individual patterns of symptom change. Another advantage to this design is that it highlights target symptoms for each patient, reflecting meaningful, real-world changes. Collecting continuous daily measures provides more robust data, allowing for a level of detail not otherwise available in the predominant large-N designs.
2 Case Introduction
Ms. K was a 50-year-old divorced Caucasian woman, a science teacher at a school for advanced students. She had two adult daughters living out of state. At the time of treatment, Ms. K was in a long-term dating relationship with her boyfriend; however, she lived alone per her preference for autonomy. She was referred for psychotherapy to treat her long-standing fear of flying on airplanes. Her general practitioner had previously prescribed Ms. K a low dose of anxiolytic medication, which she insisted on carrying in her purse at all times, despite the fact that she preferred to address her anxiety without medication management. Ms. K was intelligent and extraordinarily competent. She was typically able to use her natural defenses in socially acceptable and productive ways. However, with her daughters now living out of state, Ms. K presented to treatment motivated to move beyond her anxiety about airplanes so that she could make a visit.
3 Presenting Complaints
Ms. K reported symptoms that were consistent with a diagnosis of specific phobia with panic features. She experienced overwhelming anxiety on airplanes, at airports, and sometimes on other modes of public transportation. Physically, her anxiety would manifest with shortness of breath, accelerated heart rate, bodily warmth and sweating, nausea, and muscular tension. Due to her fear of these panic-inducing situations, she had mastered the art of avoidance—not having flown in 12 years, and doing anything in her power to avoid enclosed spaces or public transportation that might somehow remind her of flying on an airplane. Despite the fact that she had anxiolytic medication available to her if needed, Ms. K’s fears were so severe at the beginning of her treatment that, even with the option to take medication, she could not bring herself to face her airplane phobia. Although her sophisticated avoidance techniques had kept her from experiencing regular periods of panic and anxiety, they had also begun to interfere with her ability to live her life freely and joyfully. Ms. K was unable to travel, which was something she had previously loved to do. In addition, she found herself constantly busy making sure her surroundings were comfortable and within her control. She was using many of her resources simply maintaining a constantly avoidant stance toward her own anxiety, and at the time of presentation to treatment, she was beginning to feel exhausted and chronically “stressed out.”
4 History
Ms. K grew up in a traditionally conservative, lower middle class family, which she described as on “old southern family.” She reports a close relationship with her parents and considers her sister a primary source of social support.
Ms. K reported that her airplane phobia and panic symptoms began on one specific airplane ride in Alaska when she was 30 years old. This particular evening flight experienced mechanical difficulties, and Ms. K vividly remembers the power cutting out and the aircraft intensely rocking and shaking. With no working lights or air conditioning, Ms. K recalls the incident as being very dark and hot, and she remembers feeling trapped and out of control—two themes that continued to play out during Ms. K’s treatment. It was during this event that she experienced her first full-blown panic attack—racing heart, nausea, shortness of breath, profuse sweating, and a feeling of pure terror. The aircraft eventually landed safely, but Ms. K’s experience would go on to affect her for the next 20 years.
Ms. K described feeling “shaken up” after the instance in Alaska but noted that she was still able to fly on airplanes as long as she was able to carefully construct a comfortable situation for herself—sitting on the aisle and having a close friend nearby to distract her from her fears. However, despite diligent efforts to control her anxiety, Ms. K experienced another full-blown panic attack 8 years later on an airplane. It was at this point that Ms. K stopped flying altogether. After this flight and her decision to avoid airplanes, Ms. K reported that her panic response generalized to all other situations in which she felt trapped and out of control.
5 Assessment
The patient completed an intake interview, in which she described her presenting complaints as listed above. At this meeting, she also identified one symptom that she would track on a daily basis—readiness to fly. This variable was posed to Ms. K in the form of a question that she would answer each day using a 9-point Likert-type scale. The question was specifically worded as follows: “You have to get on an airplane today. How ready do you feel?” Ms. K chose to use low numbers on the Likert-type scale as markers of symptom relief (very ready to fly) and high numbers on the Likert-type scale as markers of problematic symptoms (not at all ready to fly). Previous case studies have used a similar assessment procedure, in which the patient assessed his or her own experience of one or more target symptoms (e.g., Frankel & Macfie, 2010). Ms. K’s pretreatment baseline lasted 14 days, during which time she completed daily symptom tracking. At baseline, her mean symptom severity rating was 7.79 (SD = 0.43), indicating marked distress prior to treatment.
Personality Measures
The Minnesota Multiphasic Personality Inventory 2 (MMPI-2; Butcher, Dahlstrom, Graham, Tellegen, & Kaemmer, 1989) and Symptom Checklist-90-Revised (SCL-90-R; Derogatis, 1992) were administered at intake. On the MMPI-2, Ms. K reported no elevations within the clinical range; however, her highest clinical scales were Mf (Masculinity-femininity scale; T = 62) and Ma (Hypomania; T = 59). In addition, elevated supplementary scales include Do (Dominance; T = 70) and GM (Masculine gender-roles; T = 69) with a low score on GF (Feminine gender-roles; T = 38). Generally, this response pattern indicates a dominant, active, goal-oriented, driven, and stereotypically masculine personality. On the SCL-90-R, Ms. K’s results show elevated ANX (Anxiety; T = 63) when compared with a normative, nonpatient population.
Hypnotizability
Because this treatment would use hypnosis, Ms. K was assessed for her level of hypnotizability using the Stanford Hypnotic Susceptibility Scale, Form C (Weitzehnoffer & Hilgard, 1962), referred to more frequently as the Stanford-C or SHSS:C. On this measure, Ms. K scored a 5, which is considered moderately hypnotizable and sufficient for the use of hypnosis in treatment (Woody & Barnier, 2008).
6 Case Conceptualization
Ms. K was conceptualized as a highly defended, yet intelligent and socially competent woman struggling with a specific phobia of airplanes and associated panic features. Typically, her anxiety would manifest in terms of task completion, productiveness, and organization strategies. However, when Ms. K was faced with her feared situation, her anxiety manifested in physiological and emotional panic symptoms. Her persistent and long-standing avoidance of the feared stimuli only perpetuated her intense anxiety symptoms when avoidance ceased to be possible. Fearing her next panic attack as well as any situations that threatened her tight grip on control, Ms. K was generally quite anxious and high strung. Although her presenting symptoms were circumscribed, her character structure would play an important role in the treatment of such specified complaints. Her initial assessment pointed to traits of dominance, goal-orientedness, and stereotypical masculinity in addition to her self-reported struggles with anxiety. Ms. K described herself as organized, self-sufficient, fast paced, and productive. She enjoyed her independence and autonomy, and she prided herself on her ability to maintain control over various situations. Her character structure could best be described as obsessive, as she primarily and rigidly used intellectualization, rationalization, avoidance, and denial techniques to defend against her emotional life. Her fears were paralyzing, and the prospect of addressing them in treatment was equally terrifying for her. Given her ongoing attempts to grasp a sense of control, it became clear that Ms. K possessed a limited capacity to play—to be without defensive functioning and self-control in service of surprise and creativity (Winnicott, 1971). According to Winnicott (1971), no progress can be made in therapy prior to fostering a sense of playfulness in the patient. As it turned out, this lesson would come to be quite important in the treatment of Ms. K.
7 Course of Treatment and Assessment of Progress
Overview
Ms. K’s treatment lasted a total of 12 sessions—2 sessions of intake and assessment and 10 treatment sessions. The first 5 treatment sessions were weekly and then, as will be discussed in further detail, Ms. K missed a number of appointments, creating significant gaps of time between sessions. However, during this time, she continued keeping track of her identified symptom: readiness to fly.
Therapy was designed to address her phobia and panic features in a supportive way by use of hypnosis. Per the initial treatment plan, an exposure hierarchy would guide the sessions, systematically pairing Ms. K’s panic-provoking scenes with pleasantly relaxing imagery until she no longer felt anxious. Self-hypnosis would also be included in this course of treatment, as it has been written about extensively as a key piece of any hypnosis (Bryant, 2008; Fromm et al., 1981; Fromm & Kahn, 1990; Nash, 2008). The goals of self-hypnosis in Ms. K’s case were twofold: (a) self-hypnosis would provide Ms. K with a portable tool so that she could easily revisit her pleasant and relaxing imagery whenever she needed to do so, and (b) given Ms. K’s specific issues around power, control, and autonomy, self-hypnosis may be an even more effective vehicle for healing than heterohypnosis (Nash, 2008).
The Clinical Intervention
Ms. K’s treatment began as a structured exposure hierarchy intervention using hypnosis for its imaginative, experiential properties toward this goal. However, the first three sessions of the exposure protocol were wrought with struggle. Ms. K would routinely attempt to take control of the sessions by rearranging furniture, removing her shoes, directing the therapist’s physical positioning and critiquing word choices she found unhelpful during the induction. In these sessions, she was once again focused on carefully controlling a potentially scary environment, similar to the way she would ritualistically alter her environment on airplanes following her first panic attack. Despite these attempts, Ms. K was able to relax completely and fully participate in the suggested imagery. However, she was completely unable to experience any of the unpleasant suggestions or scenes. Although Ms. K was quite adequately hypnotizable, her defenses were so deeply ingrained that even while hypnotized, she was unable to relinquish control and experience some of her anxiety. She would frequently comment, “I know it’s not real, so I don’t feel anxious.” With this rigidly in place, an exposure hierarchy intervention would not be effective. If Ms. K could not allow herself to feel anxious in session, she would also not be able to experience that anxiety as transient and under her control.
After weeks of failed attempts to move Ms. K up her hierarchy and toward her own anxiety, it became clear that the initial treatment plan would need to change. Ms. K had begun displaying some of the common dogmatic themes and defenses that Wilson (1989) and Kraft (2011) write about in phobic patients, such as resisting the experience of anxiety, forgetting, and canceling scheduled appointments. Forcing the rigid structure of the protocol upon Ms. K only seemed to intensify her own tendency to become inflexible, careful, and controlled. Sessions had come to feel like hour-long power struggles, rather than cooperative moves toward symptom relief. Ms. K was comfortable only when she was in complete control, and over time it became clear that the new course of treatment would do best to work with her defenses rather than directly against them. This meant there would be no more structured protocol or exposure hierarchy. Instead, treatment needed to allow Ms. K to lead the way so she could focus on healing rather than competing for control of the appointments. Practicing and mastering self-hypnosis for relaxation would become the focus of our work in session, with the idea that Ms. K could learn and apply these techniques on her own terms, as she saw fit in her daily life outside of the therapy room.
Immediately after the discussed shift in treatment approach, Ms. K reported that she was considering purchasing a ticket for a short, local, round-trip plane ride to test out her new skills in self-hypnosis. She discussed this idea with some degree of ambivalence—not agreeing to commit to purchasing the ticket and not agreeing to fly without the anxiolytic medication that was prescribed by her general practitioner prior to beginning psychotherapy. However, this self-generated and creative treatment strategy was impressive movement toward recovery. Most importantly, this idea came from within Ms. K rather than from without (i.e., from her therapist), and she was in charge of it. Two weeks later, during the eighth session, Ms. K reported that she did purchase the “practice” plane ticket, and that she would be flying a local 1-hour, round-trip plane route alone. She spoke with pride about her decision and asserted that although she still felt slightly nervous about flying, she no longer held the paralyzing fears that she once had. Ms. K described this shift “as though a light switch has flipped”— that she felt suddenly more ready to test her abilities and manage her anxiety in real-life settings. Following her practice flight, Ms. K sent the following note:
“Wow, I did it! When I got to the airport, I felt a bit of anxiety, but I told myself that I had the [anti-anxiety medication] if I needed it. I sat down and did the self-hypnosis and felt so much better. About one hour before takeoff, I got nervous so I took .50 mg of [anti-anxiety medication]—I felt completely normal and didn’t even have one problem thought! I had forgotten how much I enjoy flying! On the return trip (after a 4 hr, 45 min layover) I decided not to take anything at all, and got on the plane. I used my self-hypnosis instead—it was AWESOME! I feel like a huge weight has been lifted. Thank you so much for all of your help. I now feel totally comfortable about the trip to Portland. In fact, I want to fly anywhere I can!”
At the termination session, Ms. K reported feeling excited and confident in her ability to fly due to the progress she had made in therapy. Despite the difficulties at the outset of treatment, Ms. K experienced and joyfully described meaningful real-life changes.
Assessment of Progress
Level change analysis
Time-series level change analyses were conducted using simulation modeling analysis (SMA; Borckardt, 2006) for time-series, which is a relatively new bootstrapping approach to assess the shorter data streams typically encountered in intervention research (Borckardt et al., 2008). SMA also accounts for the autocorrelation, or nonindependence of sequential observations, in the data stream. An effect size (Pearson’s r) is then calculated, along with the actual probability of obtaining that effect, given the length of the data stream and its level of autocorrelation. Level-change or phase-effect analysis compares the mean scores of the two data streams. Significant effect sizes for level change indicate significant improvement in the severity of the reported variable.
To test Ms. K’s data for symptom improvement, pretreatment baseline data (Phase A) was compared with the data collected during her treatment phase (Phase B). Descriptive statistics are reported in Table 1. To analyze the change in symptom severity from Phase A to Phase B, level change analyses were conducted in SMA. This analysis yielded a significant effect (r = −0.73, p > 0.001), indicating significant symptom improvement from Phase A to Phase B. Figure 1 illustrates this change graphically.
Descriptive Statistics for Readiness to Fly Across Phases
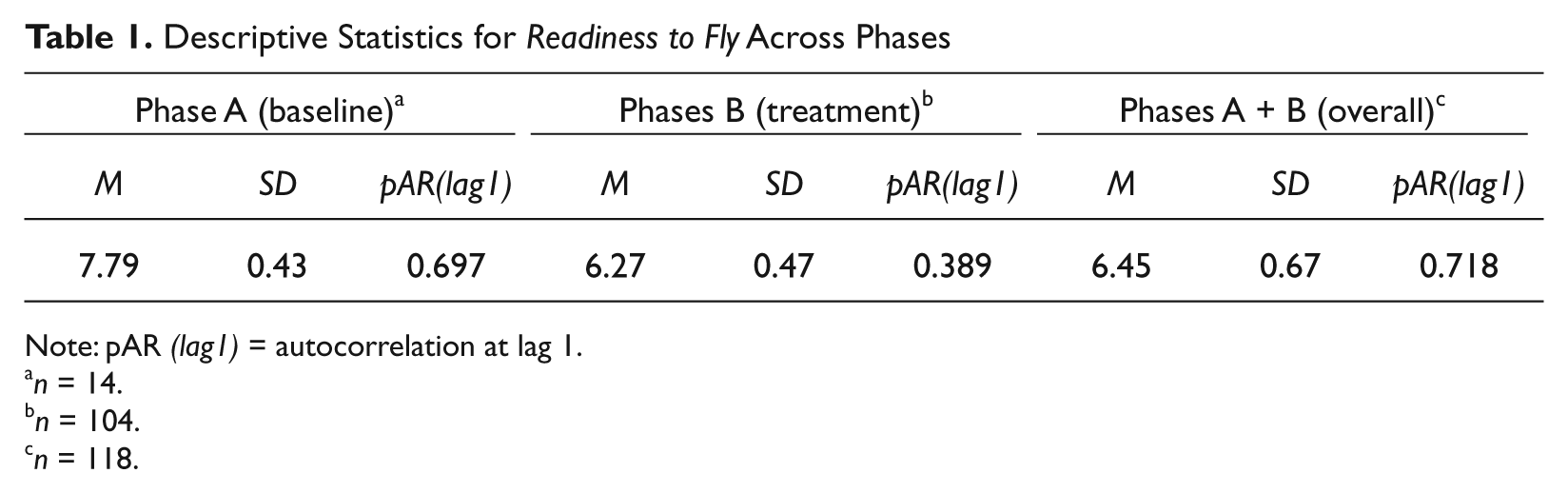
Note: pAR (lag1) = autocorrelation at lag 1.
n = 14.
n = 104.
n = 118.
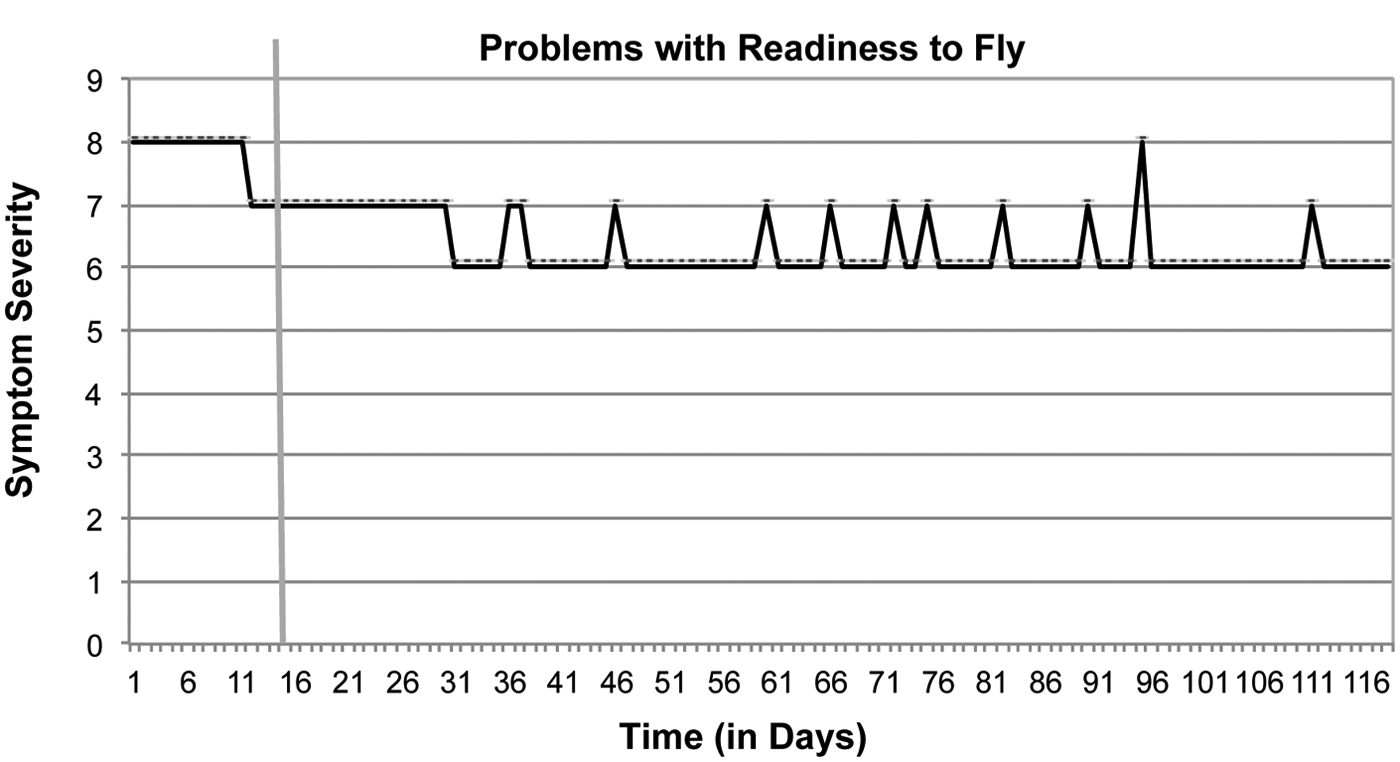
Daily ratings of readiness to fly during baseline and treatment phases
8 Complicating Factors
At Session 9, Ms. K declared she would no longer keep track of her symptom change, asserting, “I keep rating the same numbers over and over so I just stopped doing it.” Despite encouragement, Ms. K did not continue her self-assessed symptom tracking again until posttreatment follow-up. This meant that her daily records were not completed to incorporate Sssions 7 to 10. However, the data collected during her treatment totals 12 weeks, which is sufficient for reliable analysis (Borckardt, 2006). The data reported above reflect changes made in Ms. K’s symptomology from pretreatment baseline through Session 6. To examine Ms. K’s overall progress, she was given posttreatment follow-up measures to complete after termination.
9 Access and Barriers to Care
There were no issues with access or barriers to care in this case.
10 Follow-Up (How and How Long)
Despite the fact that Ms. K ceased recording her self-assessed symptom progress midtreatment, she reported marked improvement in her variable of interest. Given these noted changes, follow-up data were requested at the final session. Ms. K agreed to follow-up measures and completed 14 days of posttreatment follow-up assessment immediately after termination. She returned follow-up data along with a quick, hand-written note. It said, “Thank you again. I’m off to Portland next week and I feel totally ready!”
The mean severity rating of her follow-up data was 1.43 (SD = 0.49), indicating very little symptom severity and an increase in her readiness to fly. Phase effect or level change analyses were then conducted on Ms. K’s overall symptom change, including follow-up (Phase C). To analyze the change in symptom severity overall, Phase A (baseline) was compared with Phase C (follow-up). This analysis yielded a significant effect (R = −.99, p < .001), indicating significant symptom improvement from baseline to posttreatment follow-up. When comparing Phase B with Phase C, this analysis also yielded a significant effect (R = −.95, p < 0.001), indicating significant symptom improvement from Phase B to Phase C. This result illustrates the continued gains Ms. K experienced in treatment during the few weeks when she was not formally recording her symptom severity. Finally, the combination of Phase A and Phase B was compared with Phase C to examine the difference in symptom severity pre- and posttermination. This analysis yielded a significant effect (R = −.92, p < 0.001), indicating significant symptom improvement posttreatment versus pretermination. Overall, phase-effect analyses show that Ms. K experienced significant symptom relief over the course of treatment. Table 2 displays results of phase effect analyses over the entire course of treatment. Figure 2 illustrates Ms. K’s symptom remission through follow-up graphically.
Phases-Effect Results Across All Examined Phase Comparisons
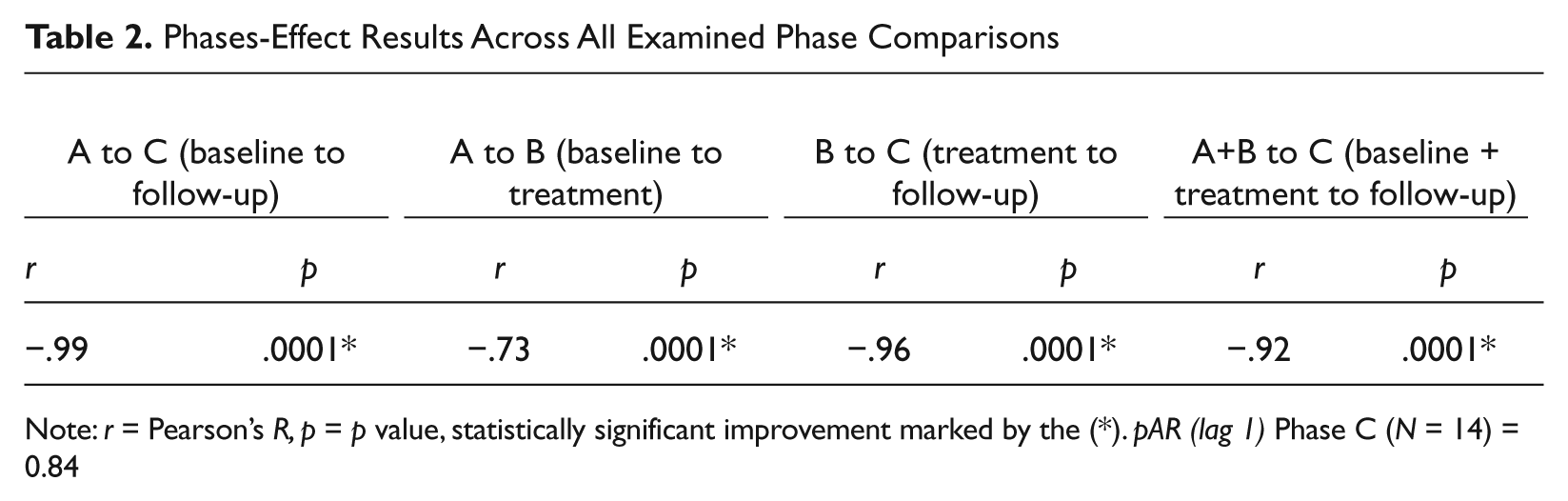
Note: r = Pearson’s R, p = p value, statistically significant improvement marked by the (*). pAR (lag 1) Phase C (N = 14) = 0.84

Daily ratings of problems with readiness to fly during baseline, treatment, and follow-up phases
11 Treatment Implications of the Case
Over the 12 sessions of psychotherapy, Ms. K’s self-assessed anxiety about flying on airplanes decreased, as her self-reported variable “readiness to fly” showed significant improvement from baseline through treatment and follow-up. Although her experience of phobic symptoms eventually improved, Ms. K’s rigid character structure posed a particular challenge for the initial treatment plan and protocol. Although her symptoms of fear and anxiety were quite well defined and circumscribed, a systematic, exposure-based treatment was wrought with complications given Ms. K’s personality and defensive structure. Her noted “inability” to feel anxious in session drastically reduced the potential for exposure to and mastery of her anxiety. As Busch and colleagues (2011) discuss, a patient’s character structure plays an important role in how they respond to a given treatment strategy. No single-treatment strategy can work for every patient with a given disorder (2011), and throughout the course of her treatment, it became clear that Ms. K was not tolerating the structured exposure techniques.
Drawing again on D. W. Winnicott’s early psychoanalytic theory, it seemed that Ms. K presented to treatment with a limited ability to play, and initially, the therapy did not foster the growth of playfulness. That is, until the focus of treatment shifted from a rigid insistence on a structured protocol to an environment which put Ms. K in the driver’s seat. Her defenses noticeably eased up with the creation of a transitional space that allowed for her spontaneous generation of meaningful material, and the authors posit that this shift was responsible for her eventual progress. As Winnicott astutely notes, “Where playing is not possible then the work done by the therapist is directed toward bringing the patient from a state of not being able to play into a state of being able to play” (1971, p. 38). Once therapy became a playful, creative, and generative space, Ms. K came up with important ideas all her own, without prompting, pushing, or insisting by the therapist. Moreover, she was in control.
Self-hypnosis was an important component of Ms. K’s treatment. It served as a portable anxiety management tool that she was able to use in and outside of the therapy sessions. This technique was particularly helpful in this case, given Ms. K’s desire for control and autonomy. Having mastered this skill, despite not having addressed specific features of her anxiety directly in sessions, Ms. K reported the ability to self-soothe in the face of fearful stimuli as they arose in her daily life. Although she did take a very small dose of her anxiolytic medication prior to the first leg of her practice flight, Ms. K reported success managing subsequent experiences of anxiety with self-hypnosis. Prior to treatment, even with anxiolytic medication available to her, Ms. K’s fears kept her from addressing her airplane phobia altogether. However, meaningful gains can be seen by (a) the fact that Ms. K voluntarily put herself in a “test” situation, (b) the fact that she got herself to the airport to follow though, and (c) the fact that on her return flight, she used only her self-hypnosis to replace anxiolytic medication. By the end of treatment, she was able to travel and fly without undue anxiety—an activity she had been actively avoiding for years.
This treatment was short term and supportive in nature, designed specifically to address symptoms of anxiety and specific phobia. However, despite the fact that her deeply ingrained patterns of power and control were not explored in this type of treatment, these themes could not be ignored. It was essential to understand how Ms. K’s character structure would play into her ability to engage in the type of treatment that was initially suggested, and learning to go with her defenses rather than against them proved to be a necessary component of treatment.
Limitations
It is important to highlight the limitations of the current study. First, Ms. K was prescribed anxiolytic medication prior to beginning psychotherapy. She did not regularly use this pharmacological intervention, but she decided to use a small amount on the first leg of her practice flight at the end of treatment. Although she did report additional success by use of self-hypnosis (and was able to use only self-hypnosis on the return flight), it is difficult to know exactly what level of an impact the pharmacotherapy ultimately had on Ms. K’s success in flying. Second, as is described in some detail, the therapeutic approach in this case shifted midtreatment. Although this may be explained and understood from a theoretical standpoint, the shift in intervention poses complications in understanding the course and outcome of this particular case. Finally, Ms. K did not complete empirically validated measures of symptom severity throughout treatment but rather reported on her own assessment of progress. She did complete an MMPI-2 and SCL-90-R at intake, but those measures were not repeated posttreatment. For this reason, the authors are careful to note that the reported improvement in airplane phobia reflects the subjective experience of the patient as reported on a self-generated and self-assessed measure.
12 Recommendations to Clinicians and Students
This single-subject research allowed for a rich exploration of a psychotherapy case treating airplane phobia using a supportive psychotherapy with adjunctive hypnosis. Although the discussed limitations of the present study may complicate our understanding of the treatment results, the authors were able to capture and examine the subjectively experienced pattern of symptom change over time, with a level of detail not typically afforded in large-N designs. Time-series design offers certain advantages over other research designs, as it allows for the detailed analysis of symptom change over time. In addition, such research lends itself to the empirical evaluation of clinical casework, bridging the gap between laboratory science and clinical practice. Use of self-report daily tracking measures on a case-by-case basis can broadly contribute to the overall efficacy in psychotherapy treatment in a cost-effective way.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.