
Abstract
Mindfulness-based therapy (MBT) has shown promise in reducing depression and psychological distress among individuals presenting with various medical and psychiatric problems. This case study examined the implementation of MBT with an undergraduate student with recurrent major depression and generalized anxiety disorder. A novel four-session MBT protocol was utilized and the patient demonstrated significant decreases in depressive and anxiety symptoms and an overall increase in quality of life at the posttreatment assessment. Treatment gains were maintained at the 1-month follow-up assessment. Consistent with previous treatment outcome studies examining the efficacy of comprehensive MBT interventions, results indicate that an abbreviated MBT protocol may be effective in treating depression and anxiety in younger adults.
Keywords
1 Theoretical and Research Basis for Treatment
Consistent with community samples, depression presents in approximately 15% to 20% of college students, with increased prevalence over the past two decades (American College Health Association, 2011, 2012; Benton, Robertson, Tseng, Newton, & Benton, 2003; Gallagher, 2007; Voelker, 2003). Given that three fourths of diagnosable mental health problems have an onset by young adulthood (Kessler et al., 2005), depression among college students is a serious and complex issue associated with several negative consequences. For example, depressed college students are more likely to smoke, abuse prescription medications, have a history of marijuana and alcohol abuse, and engage in high-risk behaviors such as unprotected sexual intercourse (The National Center on Addiction and Substance Abuse at Columbia University, 2007; Weitzman, 2004). Depression in college students also is associated with poorer academic performance, self-harm, suicidal ideation, and impairment in life functioning, with over 30% of college students reporting depression symptoms that negatively impact their ability to function (American College Health Association, 2012; Eisenberg, Gollust, Golberstein, & Hefner, 2007). Given the increased incidence of depression in college students, university counseling centers may have difficulty meeting the mental health needs of students, as longer term psychotherapy is often impractical in these settings and waitlists are common (Benton et al., 2003; Gallagher, 2007, 2012). Accordingly, there is a pressing need to develop shorter term treatments that effectively reduce depression in college students. Despite the need for efficacious treatments, there is currently little empirical support for psychological interventions for depressed college students in university settings (Gawrysiak, Nicholas, & Hopko, 2009; Lee, 2005). However, a few studies have demonstrated support for cognitive-behavioral therapy, supportive therapy, and brief behavioral activation in alleviating depression in college students (Armento, McNulty, & Hopko, 2012; Gawrysiak et al., 2009; Pace & Dixon, 1993; Reagin, 1982). Because depression is a common and debilitating condition among college students, further research on parsimonious and efficacious treatment options is essential.
One promising psychotherapy approach for depression is mindfulness-based therapy (MBT), which incorporates principles from Mindfulness-Based Stress Reduction (MBSR). MBSR is a self-regulation approach to stress reduction and emotion management that involves teaching patients meditation techniques that facilitate mindfulness (Bishop, 2002). Mindfulness is rooted in Buddhist meditation philosophy and involves being focused on the present with acceptance, without becoming overwhelmed with thoughts and emotional responses to current circumstances (Bishop, 2002; Kabat-Zinn, Lipworth, & Burney, 1985). A primary goal of MBSR is to train patients in mindfulness meditation and bring awareness to the present moment so that they gain the ability to experience stressful situations without intense emotional and autonomic arousal (Bishop, 2002; Kabat-Zinn, 1982). With practice, MBSR facilitates self-regulation of attention and emotions and increases awareness of present thoughts, emotions, and physiological sensations (Bishop, 2002). Because research suggests ruminative thinking is an important factor in the exacerbation and maintenance of depression (Nolen-Hoeksema, Morrow, & Fredrickson, 1993; Nolen-Hoeksema, Parker, & Larson, 1994), and MBSR reduces rumination (Jain et al., 2007; Ramel, Goldin, Carmona, & McQuaid, 2004), MBSR-based treatments theoretically should be beneficial toward attenuating depression. Furthermore, MBSR is thought to alleviate depression by enhancing concentration (Kabat-Zinn et al., 1992) and increasing the ability to cope with life stressors (Dobkin, 2008).
Recent meta-analytic reviews support the efficacy of MBT, including MBSR and Mindfulness-Based Cognitive Therapy (MBCT) in the treatment of depression and other psychiatric and medical conditions. Specifically, meta-analyses suggest that MBCT, an intervention combining MBSR and cognitive therapy strategies that focuses on preventing depression relapse, is efficacious in decreasing depression (Hofmann, Sawyer, Witt, & Oh, 2010; Segal, Williams, & Teasdale, 2002). In addition, MBT is moderately effective toward improving mood and anxiety symptoms in adults with psychiatric and medical conditions (Hofmann et al., 2010). Another meta-analysis by Grossman, Niemann, Schmidt, and Walachand (2004) demonstrated support for group-based MBSR in reducing psychological distress. Meta-analyses of randomized controlled trials also suggest MBSR has small but significant effect sizes in the treatment of anxiety, depression, and psychological distress among individuals with chronic somatic illnesses (Bohlmeijer, Prenger, Taal, & Cuijpers, 2010). Accordingly, there is encouraging support for MBT as effective in treating depression and anxiety in adults with medical and psychiatric problems.
Although there is promising support for MBT in the treatment of depression, little is known about the efficacy of MBT in treating depressed college students, a prudent question given unique environmental and psychological issues experienced in this population. There is some support for group-based MBSR programs toward alleviating psychological distress. For example, following an 8-week MBSR training for undergraduate students, individuals completing the program experienced reduced psychological distress relative to those assigned to a control condition (Astin, 1997). Similarly, group-based MBSR training for medical students suggested that those completing the 8-week program exhibited significantly less depression, anxiety, and overall psychological distress than control participants (Shapiro, Schwartz, & Bonner, 1998). Individualized treatments have also demonstrated positive outcomes, as a six-session one-on-one MBT was associated with decreased negative affect (Wahbeh, Lane, Goodrich, Miller, & Oken, 2012). Such findings are promising; however, it is still uncertain as to whether MBT may be an efficacious and cost-efficient treatment that can reduce depression among college students. Furthermore, no studies have examined whether individualized MBT may effectively treat depression in younger adults. Given the high prevalence of depression in college students and the high demand on limited university counseling services (Benton et al., 2003; Gallagher, 2007, 2012), additional research on the efficacy of MBT as a shorter term individualized treatment for depressed college students is warranted.
This case study examined the use of brief MBT for a freshman college student meeting diagnostic criteria for recurrent major depression. An abbreviated form of MBT based on the work of Stahl and Goldstein (2010) was utilized (McIndoo & Hopko, 2012). Treatment was conducted in four 1-hr sessions and progress was evaluated weekly, at posttreatment (5th-week follow-up), and a 1-month follow-up. Throughout treatment and follow-up, the patient’s progress was monitored via pre- and posttreatment assessment of depression and anxiety symptoms, rumination, stress, and mindfulness, as well as weekly self-reported depressive symptoms. Based on previous research supporting the efficacy of MBT for depressed individuals, it was hypothesized that the patient would improve on all primary clinical outcome variables.
2 Case Introduction
The patient was an 18-year-old Caucasian female undergraduate student at a southeastern state university. At the commencement of therapy, she was a full-time student in the midst of her freshman year. The patient received psychotherapy through a university psychology clinic as part of a randomized controlled trial examining the efficacy of two short-term psychological interventions for depressed college students (i.e., MBT and behavioral activation). The patient was not receiving any adjunctive psychological or psychiatric treatment during MBT.
3 Presenting Complaints
Prior to beginning treatment, the patient reported experiencing symptoms of depression and anxiety and indicated struggles with episodes of depression and anxiety since early adolescence. The onset of her current depressive symptoms occurred when she moved from home to begin college. Her symptoms of depression and anxiety had been increasing in severity for approximately 2 months prior to treatment. Since moving to college, she reported symptoms that included depressed mood, loss of interest in usual activities, decreased energy, sleep difficulties (insomnia and hypersomnia), loss of appetite, and impaired concentration. She also endorsed moderate feelings of guilt, decreased self-worth, and suicidal ideation. She experienced suicidal ideation approximately once weekly, but denied plan and intent. The patient also reported thoughts of self-harm (e.g., cutting), which was distressing to her as she had a history of self-harm. At the initiation of treatment, she also reported symptoms of generalized anxiety, including frequent worry, difficulty in controlling worry, feelings of irritability, tension, and difficulty sleeping. She indicated that symptoms of depression and anxiety severely interfered with her life, thereby making it difficult for her to engage in tasks and activities and resulting in an increased isolation and avoidance of social situations. When she attended social activities, she reported intense distress, pressure to participate, and frequent irritability toward other people. The patient reported that the symptoms of depression were severely distressing and also were noticed by her romantic partner, primarily her social avoidance. Although she experienced difficulties socializing, she stated that her symptoms had not impaired her academic functioning.
4 History
As noted, the patient’s symptoms of depression and anxiety had been present for approximately 2 months. The primary events that occurred just prior to the onset of symptoms included her transition from home and beginning her first semester of college. The patient reported that she was having a difficult time transitioning to her new environment and found it difficult to be away from friends and family. Although her parents lived less than an hour from campus, she was limited in her ability to visit home, as she did not have a vehicle. Furthermore, the patient’s move also coincided with the move of her best friend to another country, so she was simultaneously experiencing numerous changes in her social support network and proximity to family and friends as she began college.
The patient reported a history of depression and anxiety that began in early adolescence, with symptoms increasing in severity during her first two years of high school. She reported being diagnosed with major depression and generalized anxiety during her sophomore year of high school and that she had subsequently experienced recurrent episodes of depression and anxiety. The patient also described a significant life stressor during high school when she lost an immediate relative to suicide. She engaged in psychotherapy throughout high school but had not recently been in therapy because of a demanding schedule and logistical issues. She also reported that during high school, she had been prescribed an antidepressant medication she initially found beneficial but ultimately discontinued as it became less effective in symptom management.
5 Assessment
The patient’s progress throughout the treatment was monitored using two strategies. First, pre- and posttreatment assessment batteries were completed prior to the beginning of the first treatment session, at posttreatment, and at 1-month follow-up. Second, the patient completed the Beck Depression Inventory (BDI-II; Beck, Steer, & Brown, 1996) at the beginning of each treatment session to monitor changes in depressive symptoms throughout treatment as well as at posttreatment and follow-up assessment.
At the beginning of the first session, the patient was administered the Anxiety Disorder Interview Schedule for DSM-IV (ADIS-IV; Brown, Di Nardo, & Barlow, 1994). This semi-structured diagnostic interview revealed a primary diagnosis of recurrent major depression and a coexistent diagnosis of generalized anxiety disorder. Her multiaxial diagnosis was as follows:
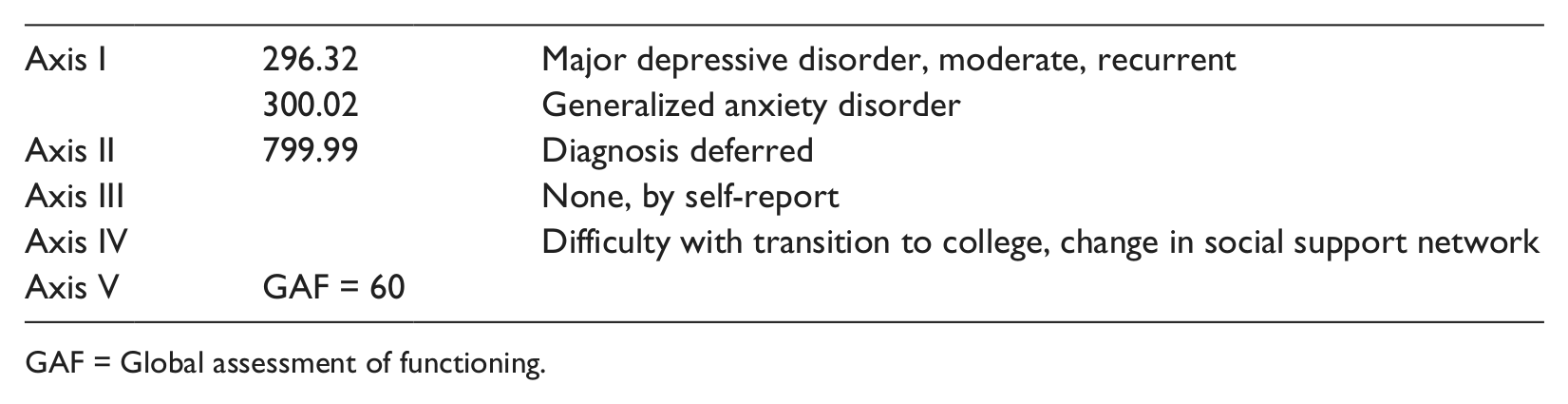
GAF = Global assessment of functioning.
The patient also completed several self-report assessment measures at pre- and posttreatment as well as the 1-month follow-up assessment.
The BDI-II (Beck et al., 1996) is a 21-item self-report measure used to assess the severity of depressive symptoms over the past 2 weeks. Participants rate the severity of symptoms on a 4-point Likert-type scale (range = 0 to 63), with higher scores indicating increased depression severity. Sample items include degree of “sadness” and “loss of energy.” Research suggests strong support for the reliability and validity of the measure with younger and older adults (Nezu, Ronan, Meadows, & McClure, 2000).
The Beck Anxiety Inventory (BAI; Beck & Steer, 1993) is a 21-item measure assessing the somatic and cognitive symptoms of anxiety. Items are rated on a 4-point Likert-type scale, with higher scores indicating increased anxiety (range = 0 to 63). Sample items include being “unable to relax” and feeling “shaky.” Good psychometric properties characterize the measure among community, medical, and psychiatric outpatient samples (Antony, Orsillo, & Roemer, 2001; Osman, Kopper, Barrios, Osman, & Wade, 1997).
The Five-Facet Mindfulness Questionnaire (FFMQ; Baer et al., 2006) is a 39-item self-report measure of five aspects of mindfulness: observing sensations, describing thoughts and feelings, acting with awareness, not judging inner experiences, and nonreactivity to inner experiences. Items are rated on a 5-point Likert-type scale ranging from “never or rarely true” to “very often or always true.” Sample items include “I’m good at finding words to describe my feelings” and “When I’m walking, I deliberately notice the sensations of my body moving.” The FFMQ has very good psychometric properties (Bränström, Kvillemo, Brandberg, & Moskowitz, 2010).
The Perceived Stress Scale (PSS; Cohen, Kamarck, & Mermelstein, 1983) is a 10-item self-report inventory measuring perceived stress over the past month. The PSS includes items concerning coping, control, irritating hassles, and unexpected events. Items are rated on a 5-point Likert-type scale from “never” to “very often” and include items such as “In the last month, how often have you felt that you were on top of things?” and “In the last month, how often have you felt nervous and stressed?” The PSS has good internal consistency (Cohen et al., 1983).
The Rumination Response Scale (RRS; Nolen-Hoeksema & Morrow, 1991) is part of the Response Styles Questionnaire and is a 22-item measure assessing rumination responses to depressed mood. Items are rated using a 4-point Likert-type scale that indicates whether individuals “almost never,” “sometimes,” “often,” or “almost always” engage in particular responses when sad or depressed. Items such as “think about how alone you feel” and “think about how angry you are with yourself” measure the extent that participants engage in actions that are self-focused, symptom-focused, and focused on the possible consequences and causes of the depressed mood (Nolen-Hoeksema et al., 1994). The measure has good convergent and predictive validity (Nolen-Hoeksema & Morrow, 1991) and high test–retest reliability (r = .80) over 1- and 6-month intervals (Nolen-Hoeksema et al., 1994).
In addition to these self-report measures, the clinician also completed the Hamilton Rating Scale for Depression (HRSD; Hamilton, 1960) at the pretreatment, posttreatment, and 1-month follow-up assessment. The HRSD is a 17-item semi-structured interview designed to measure symptom severity in patients with depression (Hamilton, 1960).
Pretreatment assessment occurred immediately prior to session one of the MBT protocol. The patient’s scores on pretreatment measures were as follows: BDI-II = 30 (severe depression; Beck et al., 1996); BAI = 16 (moderate anxiety; Beck & Steer, 1993); FFMQ = 130 (observing = 23; describing = 39; acting with awareness = 33; nonjudging of inner experience = 23; nonreactivity to inner experience = 12); PSS = 29; RRS = 59; and HRSD = 12.
6 Case Conceptualization
The case conceptualization was based on a cognitive-behavioral model of depression, which posits that individuals’ interpretations of situations and events influence emotions and feelings (Beck, 1964, 1995) and that decreases in response-contingent positive reinforcement increase vulnerability to depression (Lewinsohn, 1974). Specifically, depressed individuals experience automatic negative thoughts regarding themselves, the future, and the world (Haaga, Dyck, & Ernst, 1991). In addition to negative thoughts, depressed individuals frequently exhibit a ruminative response style that focuses on the causes and consequences of life events and depressive symptoms (Nolen-Hoeksema & Morrow, 1991; Nolen-Hoeksema et al., 1993). Individuals who engage in rumination often focus on their depressive symptoms without taking steps to alleviate symptoms (Nolen-Hoeksema et al., 1993). Moreover, environmental changes that restrict one’s access to pleasurable outcomes and contingencies predispose one to engaging in avoidance behavior and maintain depressive affect.
For this patient, proximal antecedent to depression was commencing college in a new environment away from her family and friends, resulting in a significant decrease in social reinforcement. During this transition, she began experiencing depressive symptoms and reported feelings of guilt, worthlessness, and decreased concentration. The patient engaged in frequent rumination on various topics, including the loss of her relative and how guilty she felt about the cost of her education. Her thought patterns contributed to her negative mood, which made it increasingly difficult for her to engage in normal activities. Consequently, she withdrew from many activities that were previously rewarding, such as socializing with friends. In addition, rumination and symptoms of depression contributed to feelings of irritability, which caused her to isolate, avoid, and withdraw from social settings. When the patient forced herself to participate in social events, she was frequently irritated by others and experienced a worsening of mood. Because of these aversive consequences, she participated in social interactions less frequently and her romantic partner commented on her lack of sociability, which further served to increase negative affect. Although her withdrawal from social interactions and previously rewarding activities contributed to rumination and feelings of self-dissatisfaction, her withdrawal behavior was reinforced in that she avoided exposure to negative social stimuli and aversive cognitive and physiological symptoms and situations that contributed to irritability.
7 Course of Treatment and Assessment of Progress
Based on this case conceptualization, the patient was treated with MBT, which is a manualized protocol for treating college students with depression (McIndoo & Hopko, 2012). This protocol was adapted from the workbook of Stahl and Goldstein (2010) and was designed so that training could be provided across four sessions. Important to highlight, in addition to its relative brevity of four sessions, is that the current MBT treatment differed from traditional MBSR in several important aspects. For example, MBT included a limited inquiry process that typically follows in-session meditation and movement activities in MBSR, there was no day-long mindfulness retreat and, given the individualized format, there was no opportunity to hear the experience of group members, a process considered valuable in MBSR treatment. Consistent with MBSR, however, much of the same treatment philosophy and rationale was maintained in MBT, the same mindfulness techniques were taught to the patient, and audio recordings were used to support the patient’s practice in between sessions with the therapist. Similar to MBSR, MBT involves training a new process of thinking and an attentional shift that involves increased awareness of the present moment that is nonjudgmental and directly focused on sensations, bodily states, thoughts, and the environment (Hofmann et al., 2010; Kabat-Zinn, 2003). The objective of treatment is to learn principles and skills of mindfulness and meditation to become adept at engaging in mindfulness, increasing self-reflection, and decreasing emotional reactivity in stressful situations. Thus, the acceptance and attentional shift inherent in MBT were hypothesized to shift the patient’s focus from cognitive errors, negative attributions, and rumination about the past and future toward becoming mindful and nonjudgmental of the present. Thus, MBT was posited to break the cycle of rumination dwelling on negative affect that prolongs depression and maladaptive cognitions (Nolen-Hoeksema et al., 1993). Furthermore, by gaining a greater acceptance of the present, the patient was expected to be more open to experiences, primarily social situations, less likely to assess them as aversive, and thereby more apt to experience social interactions as rewarding and reinforcing.
The goals of MBT were to (a) help the patient understand cognitive and behavioral symptoms of depression; (b) educate her on mindfulness and the rationale of MBT; (c) increase awareness of daily activities, including eating; (d) train the patient to be mindful and present-focused through meditation practices; and (e) increase her ability to recognize physiological, cognitive, and emotional responses in the present (McIndoo & Hopko, 2012). MBT was conducted over four weekly 1-hr sessions. The protocol involves an education and instruction on six forms of mindfulness meditation. Psychoeducation was provided during the first session and the patient was educated on symptoms of depression and anxiety, with the therapist promoting a discussion of symptoms specific to the patient and how the symptoms affected her functioning and quality of life. In the first session, the patient reported struggling with fatigue, sleep difficulties, loss of appetite, impaired concentration, irritability, and withdrawal from social activities. The patient was also educated on the treatment rationale of MBT and the experience of mindfulness. During the first session, she was also introduced to mindfulness practice through a mindful eating exercise, a 3-min mindful check-in exercise based on the work of Segal and colleagues (2002), and a sitting meditation exercise. After each exercise, the patient was asked to reflect on her physical, emotional, and cognitive experiences, and the therapist assisted the patient with any difficulties that arose during the exercise (e.g., judging or racing thoughts) by instructing the patient to focus on aspects of the exercise such as breathing. During subsequent sessions, the patient was introduced to the body scan, walking meditation, and mindful yoga. Throughout the sessions, she was led through meditation exercises and discussed experiences with the therapist. After each session, the patient was asked to practice meditation exercises demonstrated in the session over the following week. The patient was provided with an audio recording of each mindfulness exercise to aid in completing homework meditations. The homework for Session 1 included practicing mindful eating once, completing the mindful check-in once daily, and practicing the sitting meditation five times. After the first week, the patient reported that she had trouble completing all of the assigned homework because of her academic schedule but that she had completed the mindful eating exercise, three mindful check-ins, and two sitting meditations. Despite the incomplete homework adherence during the first week, in subsequent weeks she generally completed at least six mindful check-ins per week and at least four of the five lengthier meditation assignments (i.e., body scan, walking meditation, mindful yoga). The patient reported that she found the mindful check-in especially helpful as it provided her with a strategy to center and calm herself when she felt stressed or overwhelmed by emotional experiences.
As treatment progressed, the patient reported becoming more adept at focusing on the present moment and was able to redirect herself to the present during meditations. Her increasing ability to focus on the present was evident in her ability to report more fully on the sensations she experienced during meditations. In addition, she also reported becoming increasingly able to experience challenging situations without judgment and she was able to respond to situations without reacting with strong emotions. Furthermore, she stated that as treatment progressed, meditations became easier and increasingly relaxing and rejuvenating. As the patient integrated mindfulness into her daily life, she reported to have experienced less stress, fewer depressive symptoms, less anxiety, and less annoyance and avoidance of social situations. Furthermore, by the end of treatment she reported that she no longer experienced suicidal ideation or thoughts of self-harm.
Consistent with her verbal report, the posttreatment assessment revealed notable decreases in depression, anxiety, and stress. BDI-II scores as a function of treatment session are summarized in Figure 1. At the posttreatment assessment, the patient’s scores on outcome measures were as follows: BDI-II = 6 (minimal depression; Beck et al., 1996); BAI = 7 (normal anxiety; Beck & Steer, 1993); PSS = 10; RRS = 33; and HRSD = 8. The patient demonstrated increased mindfulness as measured by the FFMQ, particularly in the areas of observing, nonjudging of inner experience, and nonreactivity (FFMQ = 154; observing = 29; describing = 36; acting with awareness = 32; nonjudging of inner experience = 39; nonreactivity to inner experience = 18). She also no longer met criteria for major depressive disorder as assessed by the ADIS for DSM-IV (ADIS; Brown et al., 1994). Patient satisfaction with MBT was assessed with the Client Satisfaction Questionnaire (CSQ; Larsen, Attkisson, Hargreaves, & Nguyen, 1979), with data indicating strong patient satisfaction (CSQ; 29/32).
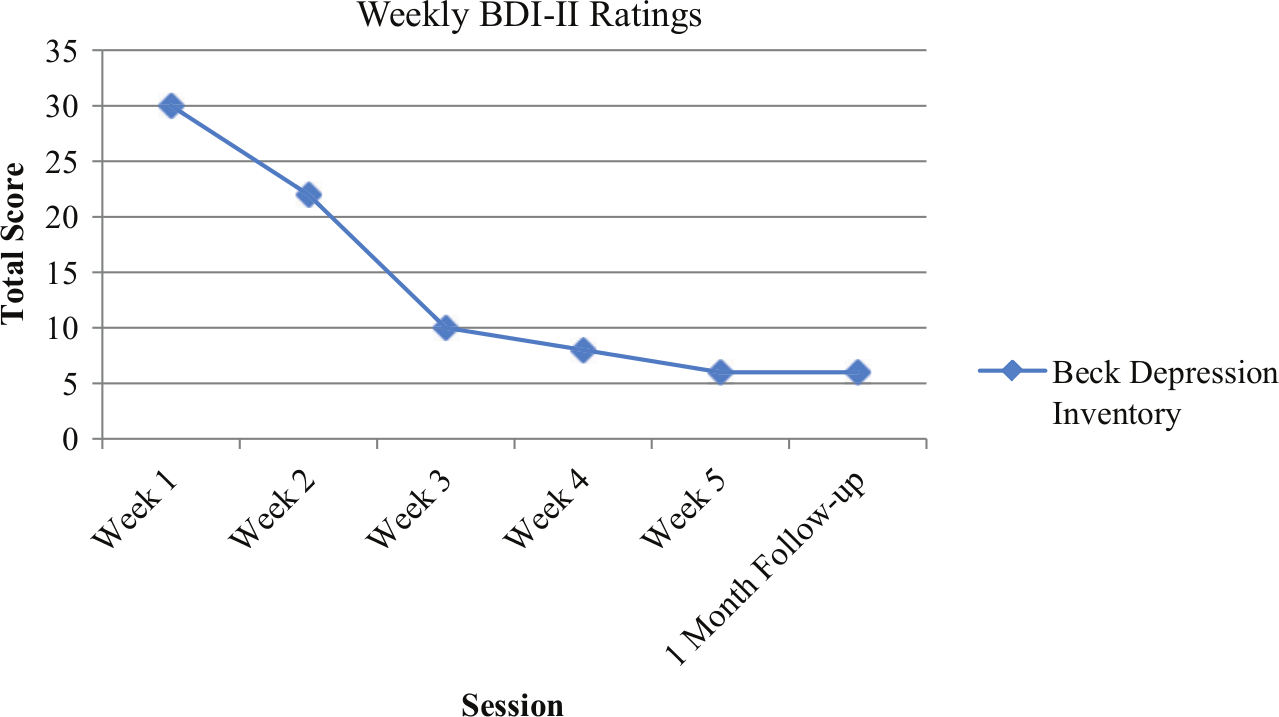
Weekly depression ratings on the BDI-II.
Percentage change in pre- to posttreatment scores were calculated for each measure. The largest improvement was demonstrated on the depression measure, as the BDI-II was associated with an 80% decrease in symptoms. Somatic anxiety also decreased substantially, with the BAI decreasing by 56%. Self-reported rumination also improved, as the RRS showed a 44% decrease in rumination. Perceived stress, as measured by the PSS, improved by a 66% decrease in symptoms, and clinician rated depression, as measured by the HRSD, improved by a 33% decrease in symptoms. Finally, mindfulness as measured by the FFMQ increased by 16%.
As an additional assessment outcome, the reliable change index (RCI) was calculated to determine the clinical significance of change in depressive symptoms (Jacobson & Truax, 1991). An RCI critical score is formulated based on the patient’s pre- and posttreatment scores and standard deviation and pre- and posttest scores and test–retest reliability scores from a treatment sample (Hopko et al., 2011; Jacobson & Truax, 1991). To determine whether the patient experienced clinically significant change in depression using the RCI, pre- and posttreatment BDI-II scores were used from a study examining the efficacy of behavioral activation on depression in university students (Gawrysiak et al., 2009: n = 30; pretreatment BDI-II M = 21.1, SD = 6.6; posttreatment BDI-II M = 8.1, SD = 3.0). Previous work examining BDI-II scores for college students seeking treatment through university counseling services estimates a test–retest reliability of .96 (Sprinkle et al., 2002). Accordingly, results suggest that the patient experienced clinically significant decreases in depressive symptoms as her RCI = 12.89 exceeded the threshold (RCI = 1.96) for clinically significant change.
To examine whether the patient experienced clinically significant change in anxiety using the RCI, pre- and posttreatment data (pretreatment BAI: M = 16.1, SD = 9.3; posttreatment BAI M = 14.3, SD = 7.7) were drawn from a university student sample (n = 70) who received cognitive-behavior therapy (Vázquez et al., 2012). Test–retest reliability of the BAI was estimated at .92 (Beck & Steer, 1993). Results suggested that the patient experienced clinically significant decreases in anxiety symptoms as her RCI (2.41) exceeded the threshold (RCI = 1.96) needed to demonstrate clinically significant change (Jacobson & Truax, 1991).
8 Complicating Factors
A major complicating factor for treatment was that the patient was in the midst of a major life transition, as this was her first semester of college, and she was residing away from home for the first time. In addition, the patient reported symptoms of unresolved grief related to the loss of her relative. There were no other complicating factors in the treatment of this patient, as she had no other comorbid psychological disorders, substance abuse problems, or medical issues.
9 Access and Barriers to Care
Because the patient sought treatment through the university’s psychology department and lived on campus, there were no access or barriers to care considerations. There were also no financial constraints, as treatment is provided pro bono to university students with symptoms of depression.
10 Follow-up
Assessment at 1-month follow-up revealed maintenance of gains in terms of reduced depression and anxiety symptoms and improved quality of life. Although decreases in depressive and anxious symptoms were maintained at the 1-month follow-up, the patient experienced mild increases in perceived stress and rumination. It should be noted, however, that the 1-month follow-up scores on these measures were still lower than those of the pretreatment assessment.
At the 1-month follow-up, the patient’s scores on all measures were as follows: BDI-II = 6 (minimal depression; Beck et al., 1996); BAI = 5 (normal anxiety; Beck & Steer, 1993); PSS = 15; RRS = 50; and HRSD = 4. Notably, the patient’s mindfulness score on the FFMQ had decreased since the posttreatment session as her score returned to a level similar to that of pretreatment (FFMQ = 129). However, there were changes in the facet scores, with the patient continuing to experience gains in nonjudging inner experience and nonreactivity (observing = 21; describing = 29; acting with awareness = 31; nonjudging of inner experience = 33; nonreactivity to inner experience = 15). Given that the patient reported symptoms of guilt, it may be that learning to experience herself nonjudgmentally was particularly important in the remission of her depressive symptoms. In addition, she did not meet criteria for major depressive disorder as assessed by the ADIS for DSM-IV (ADIS; Brown et al., 1994). The RCI also indicated that the patient continued to demonstrate clinically significant changes in depressive symptoms as measured by the BDI-II, as her score (RCI = 12.89) exceeded the threshold (RCI = 1.96) for clinically significant change. At 1-month follow-up, the patient met the threshold for clinically significant changes in anxiety symptoms (RCI = 2.95).
In addition, the patient verbally reported that she had experienced significant changes in her mood. Specifically, she stated that she felt depression and anxiety occurred less frequently and that episodes of feeling depressed lasted for shorter intervals (1-2 hr). She generally reported experiencing more anxiety than depression and was no longer having appetite or sleep problems. When she experienced depressive symptoms, she felt better able to cope and regulate her emotions. She reported continued irritability in social settings but indicated these feelings were more manageable. Importantly, she was no longer experiencing thoughts about death or self-harm at the 1-month follow-up. Thus, her verbal report was consistent with self-report measures and results of the ADIS-IV.
Finally, the patient also reported to have found the “mindset” of MBT to be most helpful in relieving distress, as she was better able to approach situations nonjudgmentally. She also reported to have used the mindful check-ins during times of stress and stated that this meditation was especially helpful when she experienced racing thoughts. She found the check-ins helpful toward slowing her thoughts and refocusing on relevant tasks.
11 Treatment Implications of the Case
This case provided convincing preliminary evidence of the potential efficacy of brief MBT for depression in college students. Given the prevalence of depression on college campuses (American College Health Association, 2011, 2012; Benton et al., 2003; Gallagher, 2007; Voelker, 2003), the development of short-term evidence based treatments for depression may provide a way for university counseling centers to better meet increasing demands for psychological services (Benton et al., 2003; Gallagher, 2007, 2012). Furthermore, although previous work has suggested that 8-week group programs are effective in reducing psychological distress, depression, and anxiety in college and medical student samples (Astin, 1997; Shapiro et al., 1998), this case is the first to support a 4-week individual MBT program as adequate for significant improvements in depression, anxiety, and quality of life. In addition, as a patient with a history of depression, anxiety, and current suicidal ideation achieved these gains, abbreviated MBT conceivably may be effective in reducing psychological distress, even among individuals with chronic negative affect.
12 Recommendations to Clinicians and Students
As this case and previous work have demonstrated (Astin, 1997; Bohlmeijer et al., 2010; Grossman et al., 2004; Shapiro et al., 1998), MBT is a promising treatment for alleviating depression and anxiety. Because depression is a prevalent problem in college settings, treatments that are short-term and cost-effective could greatly improve the ability of university counseling centers to meet the needs of students (Benton et al., 2003; Gallagher, 2007, 2012). The use of an abbreviated MBT could be helpful for students and clinicians who are looking to implement a short-term treatment that can alleviate the symptoms of chronic depression. Furthermore, the clinician was a graduate-level doctoral student in clinical psychology who had previously completed an 8- week MBSR program and was receiving supervision on the newly developed MBT protocol throughout the patient’s treatment. Thus, there is the possibility that abbreviated MBT could be conducted in other settings where individuals receive basic training in clinical skills and MBT and adequate supervision to maintain treatment competence and adherence. Further systematic research incorporating larger samples and randomized controlled trials should focus on investigating the efficacy of MBT for depressed college students and other clinical patient samples.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.