
Abstract
Although empirically supported treatments for posttraumatic stress disorder (PTSD) and depression have been available for some time, many Mandarin-speaking Chinese immigrants who seek treatment do not receive such services due to living in rural areas. Fortunately, advances in videoconferencing-based technologies are improving rural trauma survivors’ access to remote specialty clinics. Presently, little is known about feasibility and efficacy of psychotherapy provided through distance technologies for clients unable to access local services in their native languages. The present two case studies attempt to partially address this void by providing an account of treatment implemented via videoconferencing with two Mandarin-speaking women from a small Wyoming town. Not only was therapy effective in reducing the severity of PTSD and depressive symptoms for both clients, but treatment gains were also maintained for 4 months following therapy. Connecting and effectively treating two Mandarin-speaking clients using telehealth compellingly demonstrated innovations to expand services and tailor treatments.
1 Theoretical and Research Basis for Treatment
According to the National Comorbidity Survey, 20.4% of women trauma survivors and 8.2% of male survivors develop lifetime posttraumatic stress disorder (PTSD; Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995). Others have confirmed that women have at least double the risk that men do of developing PTSD following a traumatic event (Olff, Langeland, Draijer, & Gersons, 2007). Studies show that some interpersonal traumatic events can result in severe PTSD symptoms and explain a large percentage of PTSD. For example, one recent epidemiological investigation indicated that intimate partner violence (IPV) and sexual assault lead to more severe PTSD than does impersonal trauma (Darves-Bornoz et al., 2008). In addition, depression and posttraumatic stress disorder, which have substantial comorbidity, are the most prevalent mental health phenomena resulting from sexual assault (Krakow et al., 2002) and IPV (Campbell, 2002). Although excellent treatments exist to address these difficulties, many individuals are unable to access services due to a variety of barriers. One such barrier, for non-English speakers in the United States, is the lack of therapists locally who can provide services in the client’s native language. The present two case studies attempt to address the feasibility of bridging this lingual divide by providing telehealth-mediated treatment to sexual assault and IPV victims who speak only Mandarin.
According to the 2010 Census, the Asian population grew faster than any other racial group in the United States between 2000 and 2010 (Hoeffel, Rastogi, Kim, & Shahid, 2012). Chinese immigrants, as one of the fastest growing Asian groups in the United States, numbered 4 million in 2010. Most Chinese immigrants are fluent in Mandarin and live in metropolitan areas. However, some Mandarin speakers live in rural areas in the United States. Although empirically supported treatments (ESTs) for PTSD have been available for some time (Ruscio & Holohan, 2006), many treatment-seeking Mandarin speakers do not receive such service due to living in rural areas in the United States. Fortunately, advances in videoconferencing-based technologies are improving rural trauma survivors’ access to remote specialty clinics (Morland, Pierce, & Wong, 2004), thereby providing access to optimal PTSD treatment. Although videoconferencing has been suggested as a potential solution to delivering mental health services to Mandarin-speaking clients over distances (Wang, Tang, Wang, & Maercker, 2012), little is known about the feasibility, barriers, and efficacy of ESTs provided through distance technologies to rural Mandarin-speaking clients in the United States. The present two case studies attempt to partially address this void by providing an account of ESTs implemented via videoconferencing with two Mandarin-speaking traumatized women from a small Wyoming town.
Case 1
2 Case Introduction
Ms. Li (named changed to ensure confidentiality) is a 49-year-old married woman and first-generation Chinese immigrant. She presented to the Psychology Telehealth Clinic at the University of Wyoming for therapy addressing symptoms of PTSD related to an attack and a sexual assault attempt by a stranger in a parking garage. She connected with her Mandarin-speaking therapist via weekly sessions utilizing secure, encrypted videoconferencing equipment Polycom, Inc. (i.e., Polycom VSX3000 units). She received prolonged exposure (Foa, Hembree, & Rothbaum, 2007) as this is an optimal treatment for addressing post-assault PTSD.
3 Presenting Complaints
At the initial intake session, Ms. Li endorsed numerous, significant PTSD symptoms. She described regular intrusive, distressing memories of the attack. Furthermore, she reported extreme efforts to avoid the location of the assault as well as any and all reminders of the event. She reported becoming more alert to her environment and felt jumpy and startled whenever a stranger attempted to talk to her after the event. She also reported intense worry and concern that her daughter could be sexually assaulted in the future.
4 History
Ms. Li is currently married and resides with her husband and two children. She works as an associate accountant for a large agency. On August 3, 2009, the perpetrator attacked her and attempted to kidnap her in the parking garage adjacent to Ms. Li’s workplace. The perpetrator initially attempted to strike up a conversation with Ms. Li, pretending to ask her for directions. When Ms. Li turned around and was trying to answer his questions, the perpetrator repeatedly struck the back of her head with his hands. She fled the assailant on foot and began screaming for help. She encountered two bystanders who called 911 for her, and the assailant was apprehended. On medical examination, it was apparent that she had suffered some nerve damage as a result of the assault. The significance of the assault began to carry more significance for Ms. Li when she subsequently learned that the perpetrator had already served 20 years in the state penitentiary for a prior conviction of first-degree sexual assault. Ms. Li was worried that the perpetrator would not be convicted and would retaliate against her or her family.
Although the perpetrator was convicted for this offense and jailed as a repeat offender, Ms. Li was afraid that he would escape or be released and would cause harm to her or her family. Therefore, she gathered as much information about the perpetrator as she could, including information about previous court decisions and media depictions and commentary related to his prior assaults. Ms. Li went so far as to contact previous victims sexually abused by the perpetrator. She described the severity of the sexual violence the perpetrator inflicted on them. Therefore, she began having numerous negative thoughts about what could have happen to her if she had lost consciousness when that perpetrator attacked her. She repeatedly imagined horrific sexual assault scenarios that may have ensued had she lost consciousness during the assault. Although her brain function was largely intact, the physical pain related to her the physical violence served as a constant reminder of the assault. She described that her physical suffering cued and maintained her mental suffering.
5 Assessment
Posttraumatic Stress Disorder Checklist (PCL)
The PCL was used to evaluate the presence and severity of PTSD symptoms. The PCL is a 17-item rating scale instrument that assesses the degree of distress experienced within the past 30 days as a result of PTSD symptoms, which correspond to each symptom cluster as described in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994). Each item is ranked on a 5-point scale (1 = not at all, 5 = extremely). Sample items included in the PCL are “repeated, disturbing memories, thoughts, or images of the stressful experience” and “repeated, disturbing dreams of the stressful experience.” The minimum possible total score is a 17, and the established cutoff for PTSD is a 44. The PCL has demonstrated strong internal consistency, good test–retest reliability, and convergent validity, as PCL scores have been found to highly correlate with scores derived from other well-established measures of PTSD (Ruggiero, Del Ben, Scotti, & Rabalais, 2003).
The revised version of the Center for Epidemiologic Studies Depression Scale (CESD-R)
The CESD-R was used to evaluate the severity of depressive symptoms (Eaton, Smith, Ybarra, Muntaner, & Tien, 2004). This commonly used instrument is a psychometrically sound, 20-item scale that assesses the frequency of depression symptoms during the past week that correspond to the DSM-IV criteria for major depressive disorder. Scores range from 0 to 80 with respondents indicating how frequently they have experienced symptoms during the “past week or so” on a 5-point scale ranging from not at all or less than 1 day to nearly every day for 2 weeks. Items are summed with higher scores indicating greater depressive symptom severity. The CESD-R demonstrates adequate internal consistency (0.8-0.9), test–retest reliability (0.4-0.7), and high sensitivity and specificity for people with major depression (Eaton et al., 2004). Cronbach’s alpha for this measure of depression is .92, .93, and .94, at 1, 3, and 6 months, respectively.
Wyoming Telehealth Trauma Clinic Client Satisfaction Scale
The Telehealth Client Satisfaction Scale was created by the second author to assess client opinions and reactions regarding treatment delivery (Hassija & Gray, 2009). This measure consists of 11 items and requires participants to rate their telehealth-based treatment experience on a scale of 1 to 5 (5 = excellent, 1 = poor). Items include assessment of sound quality, video quality, ease of equipment use, confidentiality of services, helpfulness of the therapist, sensitivity of the therapist, scheduling of sessions, timeliness of scheduling the first appointment, matching of treatment to individual needs, respect for opinions about treatment, and overall service quality. Total scores can range from 55 (indicating a high satisfaction) to 11 (indicating poor satisfaction).
6 Case Conceptualization
Behavioral theories of PTSD suggest that a person exposed to a life-threatening experience may become anxious in response to a wide variety of stimuli that were present during the trauma through the process of classical conditioning; as a result, these previously neutral stimuli come to elicit intense anxiety (Keane, Zimering, & Caddell, 1985). In the present case, the parking garage where the attack happened came to elicit intense anxiety. Every time Ms. Li entered the parking garage, she suffered pronounced anxiety compatible with that experienced during the attack. Emotional processing theories propose that a fear structure is activated when information in the environment matches some of the information presented in the structure, which results in spreading activation to associated elements, thereby producing cognitive, behavioral, and physiological anxiety reactions (Foa, Huppert, & Cahill, 2006). Ms. Li was afraid that another attack could happen to her in the parking garage. As a result, she developed the safety behavior of avoiding parking in the parking garage when she was alone. Both the conditioning theories and the emotional processing theories of PTSD incorporate associations between stimuli and responses (Cahill & Foa, 2007). Since the associations between neutral stimuli and emotional responses (anxiety and fear) were established for Ms. Li, she experienced pervasive symptoms of posttraumatic stress disorder: re-experiencing, avoidance, and hyperarousal. In addition, she ruminated about what happened to her and what could have happened (i.e., sexual assault).
7 Course of Treatment and Assessment of Progress
Ms. Li was seen by a doctoral student in clinical psychology, who had been trained in cognitive behavioral therapy (CBT) and exposure therapy for PTSD. To access services, Ms. Li would call in to the therapist via a secure, encrypted videoconferencing unit (Polycom VSX3000). Ms. Li attended seven sessions of psychotherapy via telehealth. The first two sessions consisted of the initial diagnostic assessment, therapeutic rapport building, and psychoeducation. Sessions 3, 4, 5, and 6 were prolonged exposure therapy sessions. In addition, a culturally informed CBT was used to treat her depressive symptoms.
During Session 1, Ms. Li was asked to complete assessment measures sent to her by her next therapy session. She obtained a pretreatment score of 61 on the PCL and a pretreatment score of 31 on the CESD-R, indicating severe symptoms of PTSD and moderate depression (see Figure 1). During Session 2, the therapist explained a cognitive-behavioral conceptualization of PTSD and depression to Ms. Li and provided her with psychoeducation and rationale for prolonged exposure therapy and CBT.
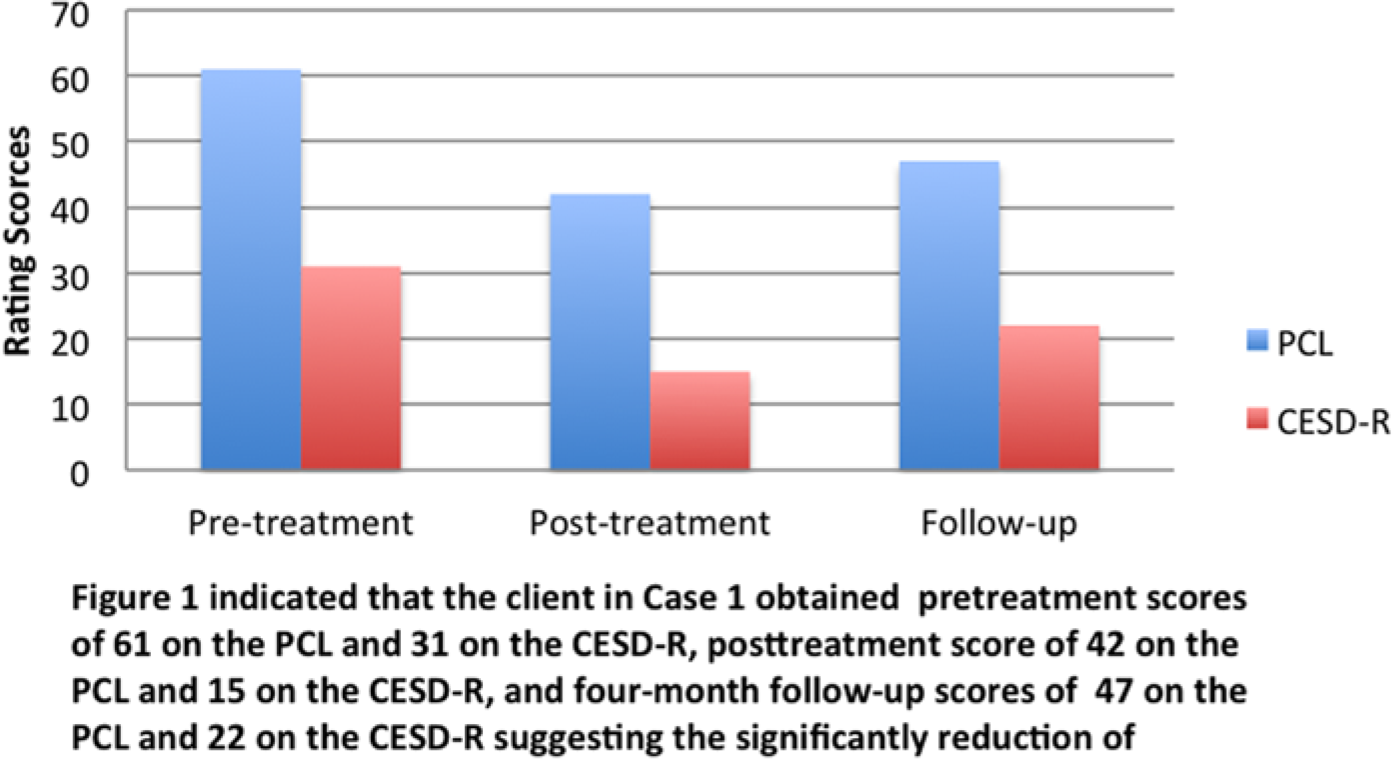
Pre- and posttreatment for PTSD and depression symptoms (Case 1).
During Session 3, Ms. Li began formal exposure therapy and imaginal exposure for the attack event that was the primary focus of the session. Using the protocol outlined by Foa and colleagues (Foa, Hembree, & Rothbaum, 2007)., the therapist told Ms. Li to close her eyes and begin recounting the details of her traumatic event. She was instructed to repeat the account once she had finished, until she was told by the therapist to stop. Ms. Li was informed that the therapist would be checking in every 5 min to obtain Subjective Units of Distress Scale (SUDS) ratings as an indication of the client’s current level of distress. The therapist allowed Ms. Li to tell her story with minimal interruption aside from general encouragement. While recounting her memories about the traumatic event, Ms. Li became highly emotional and cried several times. She began with walking into the parking garage and continued to the point when she was attacked by a stranger unexpectedly. This imaginal exposure exercise lasted 60 min. While “reliving” her accident, Ms. Li’s SUDS peaked at a 10 within the first 30 min and remained there for about 20 min. After that, her SUDS steadily declined until reaching a 7.
During Session 4, Ms. Li was presented with the rationale for the in vivo exposure exercise. The therapist helped Ms. Li establish her hierarchy of unpleasant situations she started to avoid after her traumatic event. According to Ms. Li’s description, her SUDS would reach a 10 if she stayed alone in the inside section of the parking garage for 5 min, which was the situation that frightened her the most. Her SUDS would reach an 8 if she stayed alone in the outside section of the parking garage for 5 min. She also indicated that her SUDS would be a 5 if she went to the inside of the parking garage with her colleagues, which was a situation associated with moderate anxiety. Ms. Li was asked to select a situation she thought would be a good one for the in vivo exposure exercise assigned as her homework. She selected the situation where she stayed alone in the outside section of the parking garage. She did the in vivo exposure exercise continuously for 6 days. Her SUDS initially peaked at an 8 and then declined until reaching a 6.
During Session 5, Ms. Li engaged in the imaginal exposure exercise again. The procedure of conducting the imaginal exposure exercise during Session 5 was the same as during Session 3. Her SUDS peaked at an 8 within the first 10 min and then declined steadily until reaching a 5 after 50 min.
During Session 6, the therapist evaluated whether Ms. Li’s hierarchy of unpleasant situations she started to avoid after her traumatic event had improved as a result of exposure. Her SUDS reached a 10 when she stayed alone in the inside section of the parking garage for 5 min, which was the situation that frightened her the most. Her SUDS for this situation during Session 6 was much lower than that during Session 4.
During Session 7, Ms. Li mentioned that she was busy with work and could not continue psychotherapy but that she had already improved significantly. Therefore, on mutual agreement, therapy was terminated, and the client completed posttreatment measures. Her posttreatment scores were a 42 on the PCL and a 15 on the CESD-R, indicating improvements in both PTSD and depression symptoms (see Figure 1). Although greater decrements would have likely resulted from continued therapeutic activity, it is clear that her distress was significantly reduced following treatment. Both posttreatment scores were below established cutoff scores for diagnoses.
In addition to exposure therapy, the therapist provided the client with culturally sensitive validation by acknowledging and processing the trauma according to Chinese traditional values, and reinterpreting the meaning of the client’s frightful experience according to these values during Sessions 1, 3, 4, and 5. Specifically, according to social norms of traditional Chinese ethical philosophies, chastity is considered a woman’s preeminent virtue (Hinsch, 2007). Unfortunately, many Chinese believe that no woman can be assaulted against her will. Stated differently, any extramarital sexual experiences, even including sexual assault, can be taken as evidence of her unchastity. Consequently, the Chinese expectation and conceptualization of chastity was a factor that increased Ms. Li’s tendency to imagine horrific sexual assault scenarios that may have ensued had she lost consciousness during the assault and what could have happened to her reputation if the perpetrator did sexually assault her. The therapist provided the client with validation and processing regarding the traditional Chinese value of female chastity, clarified the client’s maladaptive thoughts about what this event meant to her reputation via Socratic dialogue, and reassured the client that what happened to her was not her fault and that she would not be blamed by anyone. It is our belief that these culturally informed and sensitive considerations were essential in effectively alleviating the client’s distress. In all likelihood, it would not have been possible to effectively address her most pressing concerns and toxic appraisals without understanding Chinese cultural beliefs about assault and chastity.
8 Follow-Up
At a 4-month follow-up, Ms. Li obtained a 47 on the PCL and a 22 on the CESD-R suggesting the relative maintenance of treatment gains (see Figure 1). Not only was therapy effective in reducing the severity of PTSD symptoms for Ms. Li, but treatment gains were also large and maintained for 4 months following therapy.
Case 2
2 Case Introduction
Ms. Wang (named changed to ensure confidentiality) is a 44-year-old married woman and first-generation Chinese immigrant. She presented to the Psychology Clinic at the University of Wyoming (UW) to address her symptoms of depression related to her emotionally abusive relationship with her husband because of his extramarital affair and issues related to her relationship with her husband’s extended family. She received treatment for depression via videoconferencing-based telehealth. She received individual therapy targeting relationship stay–leave decision making based on a motivational interviewing approach (Miller & Rollnick, 2012) and targeting depressive symptoms using cognitive behavior therapy with particular emphasis on behavioral activation (Lejuez, Hopko, Acierno, Daughters, & Pagoto, 2011; Lejuez, D. R. Hopko, & Hopko, 2001).
3 Presenting Complaints
At the initial intake session, Ms. Wang was experiencing significant distress and especially elevated symptoms of depression. Ms. Wang described feeling betrayed by her husband because of his extramarital affair. She reported feeling hopeless and was experiencing difficulty in deciding what to do about her marital relationship. She conveyed the details of being emotionally abused and slapped by her husband and how badly her husband’s extended family members treated her, and also noted that as a result of these worries, she could not sleep well (rumination and insomnia).
4 History
Ms. Wang lives in a small town and works as a nurse in a hospital. About 10 years ago, she moved here with her husband and son. Because her husband’s family members own several restaurants in the United States, her husband was appointed to be the manager of one of their restaurants in this town. She married her husband 18 years ago when they were in China. At that time, Ms. Wang worked as a teacher in a middle school and her husband worked as an engineer in China. Ms. Wang had not met her husband’s family until she moved to the United States. She has a good relationship with her son (an 18-year-old boy) who has a positive relationship with his father. About a few months prior to therapy, when Ms. Wang found out her husband had been having an affair with a woman employee in his restaurant for 15 months, she felt angry, sad, and helpless. Ms. Wang described that her husband had kept all the information about their money away from Ms. Wang and possibly transferred their money to his mistress’s account since his extramarital affair started. Two months after this, Ms. Wang started to receive the therapy via telehealth. She described that she and her husband fought—both verbally and physically—because of his mistress. Ms. Wang was despondent because she and her husband had never fought during their 18 years of marriage until she learned about his affair. As a representative example of an argument, Ms. Wang’s husband once slapped her and was outraged when he learned that she had withdrawn a large sum of money after learning of his ongoing affair. Fearing for her safety, she called 911, and police came to the house. Her husband filed for a divorce immediately after that fight. Feeling disappointed about her marital relationship, she contemplated the implications of divorce from her husband. However, Ms. Wang was extremely sad and hopeless when contemplating this possibility and feared being alone.
In addition, Ms. Wang described that she did not get along with her husband’s extended family. Being close to an extended family is an important value in marriage in the traditional Chinese culture. Ms. Wang described that she sacrificed a great deal for her husband’s parents but that she did not get anything in return from them. She complained that her parents-in-law did not watch her son when he was little as most other Chinese grandparents usually do, even though her son is their only grandchild. However, she always took care of her parents-in-law whenever they needed her help. Ms. Wang said that her parents-in-law supported the divorce between her and her husband, and did not care about her feelings at all. Because of the great significance of such relationship difficulties in Chinese culture, she experienced significant depressive symptoms.
5 Assessment
The measures that were used for the first case were the same for the second case. The CESD-R was used to assess severity of depression symptoms. The Wyoming Telehealth Trauma Clinic Client Satisfaction Scale was used to assess client opinions and reactions regarding treatment delivery.
6 Case Conceptualization
Two cognitive theories explaining the development of maintenance of depression were deemed relevant to this case: Beck’s cognitive theory (Beck, 1976) and the response style theory (Nolen-Hoeksema, Girgus, & Seligman, 1992). Beck’s cognitive theory consists of four different cognitive constructs: schema, cognitive errors, cognitive triad, and automatic thoughts. Depressogenic schemata tend to yield negative and rigid attitudes about the relationship between the self and the world. Stress stimulates depressogenic schemata leading to extremely distorted beliefs and interpretations. As a result, the content of cognitions is dominated by a negative view of the self, the world, and the future—the so-called cognitive triad. The depressive style of thinking finds its expression in negative automatic thoughts. Ms. Wang had developed depressogenic schema about her relationships with her husband and her in-laws through her 18-year marriage. Knowing that her husband was having an affair with another woman, as a stressor, activated Ms. Wang’s depressogenic schema and led to her cognitive errors (e.g., she attributed her marriage failure to her poor decision making in her marriage 18 years ago and concluded that she lacked the ability to select a faithful husband). Ms. Wang felt that she devoted herself to her marriage but received nothing from it. She described that all her memories about her relationships with her parents-in-laws and her husband were negative. Her anger and sadness caused her to keep ruminating about those automatic thoughts: “I should have never been married to him [her husband]” and “They [her parents-in-law] have never respected me.” The response style theory proposes that the style with which an individual responds to depressed mood is the central factor determining the development, severity, and duration of a depressive episode. Ms. Wang responded to her stressful event through rumination and actions through which she took revenge against her husband (e.g., she refused to buy health insurance for her husband after she found out about his affair, and refused to go to her father-in-law’s funeral). Both cognitive theories postulate the relationship between rumination and depressive symptoms (Pössel, 2011). Consistent with the cognitive triad, Ms. Wang was pessimistic about future events. She was afraid of what was going to happen if her marriage eventually failed. At the outset of therapy, she completed measures of distress. Her CESD-R score of 24 indicates a moderate degree of depression.
7 Course of Treatment and Assessment of Progress
Ms. Wang was seen by a doctoral student in clinical psychology trained in behavioral activation for depression and motivational interviewing for behavioral changes. Ms. Wang attended 17 sessions of psychotherapy via videoconferencing equipment. The first 2 sessions consisted of the initial diagnostic assessment and therapeutic relationship building. The following 15 sessions were motivational interviewing, cognitive restructuring, and behavioral activation sessions.
During the first two sessions, an effective therapeutic relationship was established between Ms. Wang and the therapist. The therapist collected information related to Ms. Wang’s depression symptoms and mapped out treatment goals and plans to address Ms. Wang’s complaints. Ms. Wang completed the pretreatment measures, and obtained a score of 24 on the CESD-R, indicating the severity of her depression symptoms.
From Sessions 3 to 16, Ms. Wang was engaged in cognitive behavioral treatment consisting primarily of behavioral activation and cognitive restructuring. The therapist helped Ms. Wang identify potential enjoyable activities and created an environment that supported healthy behavior, for example, fishing, cooking, or doing yard work. The therapist suggested that she use documents to record her daily activity (the Daily Activity Record Form). Also, using a modified motivational interviewing manual (Miller & Rollnick, 2012), the therapist helped the client with her decision making about the status of her marriage.
Ms. Wang wanted to discuss whether to leave her marriage. Either choice had both positive and negative possibilities for her. She had “equipoise,” which is characterized by having no specific or clearly articulated goal or direction in mind (Rollnick, Miller, & Butler, 2008). Motivational interviewing philosophy and skills were utilized to support Ms. Wang’s consideration of relationship decisions and their varied consequences. The therapist expressed empathy for Ms. Wang and learned about the goals and values that Ms. Wang held deeply. Through the discussion and strategic reflections, the therapist assisted Ms. Wang to examine the conflict and discrepancy between the behavior and the values she held. For example, according to the traditional Chinese values, men have been seen as the core of the family and are supposed to be more capable than women. However, Ms. Wang’s English was much better than her husband’s, and so she was more social than her husband in American society. She pursued a bachelor’s degree in nursing and became an employee in a hospital. In contrast, her husband helped his family with their restaurant business but was not motivated to improve his English or find another job. Ms. Wang was a holder of traditional Chinese values, but she engaged more in American lifestyle than her husband did. Through discussion and reflection, Ms. Wang realized the discrepancy between her values and her behavior, and was motivated to adjust and make her values and her behavior compatible with each other.
In addition, strongly influenced by the traditional Chinese values, Ms. Wang’s husband appreciated one of the family-related virtues, filial piety. Ms. Wang described an important part of her husband’s everyday routine was to visit his parents in their apartment because they all lived in the same town. Ms. Wang described that her parents-in-law disliked her and her son, so she and her son did not go with her husband to visit them except on some special holidays.
During Session 11, the therapist clarified Ms. Wang’s emotions and needs during the therapy. The therapist provided psychoeducation about cognitive monitoring so that the client learned how to monitor her automatic thoughts and how to differentiate maladaptive thoughts from adaptive thoughts. The therapist suggested that Ms. Wang use the Automatic Thought Record Form to document her daily thoughts. The therapist helped Ms. Wang identify her automatic thoughts and rationally disputed her automatic thoughts with the Socratic method during the following session. For example, Ms. Wang reported that she repeatedly thought that she really hated her parents-in-law because they did not like her. Through a Socratic conversation, the therapist encouraged Ms. Wang to recall some positive situations that happened between her and her parents-in-law during the past 10 years. Ms. Wang indicated that she would have felt guilty if she had not taken care of her parents-in-law when they were sick. The therapist challenged Ms. Wang’s automatic thought by showing that there were some times when Ms. Wang did not hate her parents-in-law and treated them as family members. Also, the therapist analyzed the possible reasons why Ms. Wang repeatedly experienced those automatic thoughts. Ms. Wang realized that she was searching for reasons why her marriage brought her such pain.
From Sessions 12 to 16, emotional conflicts between Ms. Wang and her husband were aggravated and became more extreme. Ms. Wang described that she refused to pay for her husband’s health insurance since she found out that her husband betrayed her. Then, her husband refused to pay for the phone bills and house insurance without a notification. Ms. Wang’s husband filed for a divorce and claimed that the prerequisite of his accepting her as the single owner of the house was that she must give him US$100,000. Also, her husband claimed unemployment and simultaneously refused to pay alimony. They could not arrive at an agreement on their financial conflicts. Ms. Wang stated that she hid her husband’s bookkeeping records, which provided evidence that her husband and his family paid less tax than they should pay, to protect herself. This resulted in her husband getting progressively angrier and aggressive. Ms. Wang applied for a protection order with the assistance of the local domestic violence crisis center after an instance of physical violence perpetrated by her husband. The therapist provided Ms. Wang with supportive psychotherapy to help her deal with her fear of being abused by her husband emotionally and physically.
During the last session, Ms. Wang indicated that her lawyer was filing papers for divorce proceedings. As her protection order was executed and a decision regarding her marital relationship had been realized, she felt safer and more relieved. She indicated at the end of therapy that she was no longer ambivalent any more about her relationship with her husband and was satisfied with the decision to divorce. Her posttreatment score was a 14 on the CESD-R, indicating significant symptom improvement (see Figure 2).
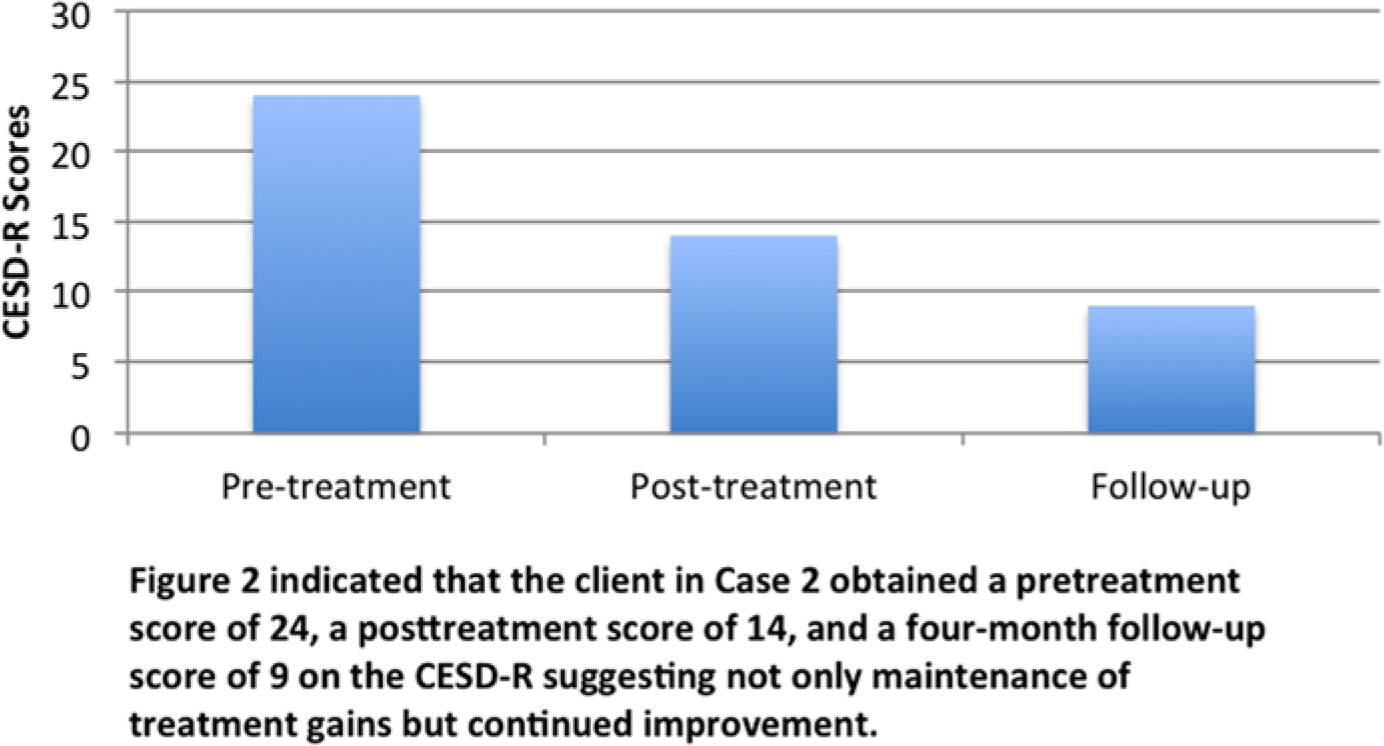
Pre- and posttreatment for depression symptoms (Case 2).
8 Follow-Up
At a 4-month follow-up assessment period, Ms. Wang obtained a 9 on the CESD-R suggesting not only maintenance of treatment gains but also continued improvement (see Figure 2). Not only was therapy effective in reducing the severity of depressive symptoms for Ms. Wang, but treatment gains were also large and maintained for 4 months following therapy.
9 Access and Barriers to Care
Distance is a barrier to accessing optimal treatment for trauma survivors. Fortunately, advances in videoconferencing-based technologies made it possible for rural trauma survivors in a small Wyoming town to access a specialty clinic that could provide such services without leaving their home community. The other conspicuous barrier to care that characterized these cases was language. There quite simply were no Mandarin-speaking counselors or psychologists in their home community. Without a telehealth solution, these individuals would not have received any services whatsoever—trauma-informed or otherwise. However, the availability of a Mandarin-speaking therapist with a specialization in treating trauma coupled with secure, encrypted videoconferencing technology allowed these Mandarin-speaking trauma survivors to access optimal PTSD treatment in their native language, effectively eliminating previously insurmountable barriers to care. In the present two cases, in addition to exhibiting significant symptomatic improvement, Ms. Li and Ms. Wang reported high satisfaction with services, partially due to the fact that they valued being treated by a therapist speaking their native language and cognizant of the values in their native culture.
10 Complicating Factors
A successful use of video-based conferencing to provide clinical service requires at least two conditions: reliability of the device providing the videoconferencing and the client’s willingness to accept clinical service via video-based conferencing. In our clinic, technicians are responsible for making sure that the secure, encrypted videoconferencing unit (Polycom VSX3000) works appropriately before every clinical session starts. In the present two cases, both clients had a favorable view of the way in which clinical services were delivered via videoconferencing. In this manner, they received clinical services without having to travel 1 or 2 hr to the Psychology Clinic at UW to meet the therapist in person. In addition, acculturation level and Chinese immigrants’ help-seeking behavior for mental health issues, which has been influenced by their traditional culture-related values, may complicate the situation where the Mandarin-speaking clients used clinical services in an unconventional way. Statistically, relative to Caucasians, Chinese immigrants have been found less likely to seek professional help regarding emotional distress (Kung, 2003). However, the special situation where two Mandarin-speaking clients were allowed to use their native language to communicate their emotional difficulties to a therapist in a country where English is the dominant language increased the two clients’ motivation to seek professional help. The combination of using both the clients’ preferred language and their preferred way of receiving clinical services made it easy to build good therapeutic relationships and to sustain treatment gains.
11 Treatment Implications of the Two Cases
These case examples illustrate the benefit of utilizing videoconferencing technology to connect non-native English speakers with distal therapists who can provide services in their native language—in this case, Mandarin. Specifically, victims of interpersonal violence were successfully seen using telehealth, and at follow-up, clinically significant reductions in PTSD and depressive symptoms were achieved and maintained. Importantly, neither individual would have been able to receive services in her local community as there are no Mandarin-speaking therapists in the region. University-based training clinics tend to specialize in evidence-based practices and are able to provide services in different languages. Until relatively recently, it was not possible for clients in rural or frontier areas to access such services. With the advent of distal technologies, previously underserved populations can now receive specialized services that would otherwise be unavailable to them.
The outcomes of the present two cases are consistent with the findings from previous research demonstrating that depression and sexual violence can be treated using distal technologies (Hassija & Gray, 2011). The present effort expands these findings by demonstrating the value of utilizing similar technologies to connect lingual minority therapists and clients. It has been found that Chinese American individuals exposed to events of IPV or sexual assault are less likely to report their traumatic experiences and to seek help from mental health professionals, relative to their American counterparts. Strongly influenced by the traditional Chinese values, the Chinese consider being chaste as one of the greatest qualities of women, symbolizing a loyalty to marriage. In addition, most Chinese consider the issues related to IPV as family issues, which should be solved by family members or intimate partners themselves. Relative to the traditional face-to-face mental health services, telehealth services provided via videoconferencing allow Chinese victims of sexual assaults and IPV to feel more comfortable working with professionals than they are in a distal locale. One reason why these particular Chinese victims reported receptivity to discussing these issues therapeutically is that they felt that it was easier to keep their privacy via videoconferencing. They also appreciated seeing a therapist who shared their cultural understanding of the presenting issues.
12 Recommendations to Clinicians and Students
Though promising, this study is not without limitations. Notably, as with all case studies and small sample size investigations, it cannot be known at present whether such findings would be representative of similar efforts with larger samples. The benefit of a case series is the demonstration of feasibility and promise of an untested approach. Based on this very preliminary evidence, it would appear that continued efforts to connect linguistically compatible therapists and clients over large distances—even when presenting with sensitive and difficult issues—would be warranted. However, the limitations of telehealth should be considered before large-scale efforts to extend such findings. A key component to telehealth success is the ability to ensure as controlled an environment as possible, such as in traditional face-to-face encounters that serve to maintain structure and therapeutic integrity (Barak, Hen, Boniel-Nissim, & Shapira, 2008).
Some limitations of telehealth service, such as office layout, ability to minimize interruptions of psychotherapy, availability of technical support, and so forth, may be of significant importance (Perle & Nierenberg, 2013). It is also important to bear in mind that Ms. Li and Ms. Wang were highly motivated, compliant clients. Their efforts and investment may not be representative of all clients. Also, technical difficulties are possible, and thus a back-up plan should be arranged. In the present two cases, the therapist informed the two clients that if the videoconferencing system was not working properly for a particular session, this session would be conducted over telephone. Though unlikely, it is important to have a plan in place prior to beginning videoconferencing-based sessions. In summary, Mandarin-speaking clients who would otherwise have received no mental health services for emotional difficulties relating to interpersonal violence and relational abuse were able to access specialized services in their native language via telehealth. Symptom reductions were large and maintained, attesting to the promise of this approach in connecting rural clients with culturally and linguistically compatible services.
Footnotes
Author’s Note:
This project was supported by the Verizon Foundation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This project was supported by the Verizon Foundation.