
Abstract
The integration of athletics into higher education enriches the experience of student-athletes, and the advantages are both immediate and lifelong. However, it is well-documented that athletes experience unique stressors, and a deficiency exists of evidence-supported programs to concurrently promote goal achievement in mental health and sport performance. Therefore, this case examination reviews efficacious implementation of The Optimum Performance Program in Sports (TOPPS) in a collegiate combat sport athlete evidencing alcohol dependence and concurrent elevations in mental health symptoms. An AB experimental design with follow-up assessments was utilized to determine the influence of intervention on the participant’s substance use, mental health, HIV/sexually transmitted infection (STI) risk behavior (i.e., unsafe sexual practices), relationships, and factors identified to interfere with sport performance. Unique to existing campus counseling programs, TOPPS incorporated significant other support to assist in goal accomplishment. The intervention program included innovative components that were built upon evidence-supported Family Behavior Therapy protocols, including Cultural Enlightenment, Dynamic Goals and Rewards, Performance Planning, Environmental Control, Self-Control, Reciprocity Awareness, and Positive Request. Intervention components were evaluated to be reliably implemented. The participant reported substantial improvements in mental health and reduced substance use from baseline to post-intervention assessment, and these improvements were sustained at 1- and 3-month follow-up assessments. Future directions in performance programming with student-athletes are discussed in light of the results including the incorporation of significant others in the intervention plan.
1 Theoretical and Research Basis for Performance Programming
College athletes face unique challenges in their psychosocial development. As compared with non-athlete counterparts, collegiate athletes have schedules that are more difficult to balance, academic pressures, limited opportunities for social interactions with individuals outside of their team, and physical or mental exhaustion (Saffici & Pellegrino, 2012). College athletes experience unique challenges that may lead to anxiety and emotional upset (Elison & Partridge, 2012). They are also at risk of experiencing identity conflicts (Pinkerton, Hinz, & Barrow, 2013), discomfort during untimely adjustments (Lu, Hsu, Chan, Cheen, & Kao, 2012), and fears related to failure (Elison & Partridge, 2012).
College athletes also interact within a culture that often reinforces substance use to commiserate losses and celebrate victories. They are at a significant risk to endanger themselves while using illicit drugs and alcohol (Hildebrand, Johnson, & Bogle, 2001; Martens, Dams-O’Connor, & Beck, 2006), with as many as 75% of student-athletes having reported binge drinking during the past 2 weeks (Brenner & Swanik, 2007). Heavy drinking patterns increase risk of driving under the influence of substances, sexual victimization (Leichliter, Meilman, Presley, & Chasin, 1998), engaging in unprotected sexual intercourse, and interpersonal concerns (Nelson & Wechsler, 2001). Therefore, substance abuse interventions for student-athletes are warranted (Donohue, Pitts, Gavrilova, Ayarza, & Cintron, 2013). Along these lines, professionals at university counseling centers report that the severity of student psychiatric problems has increased while resources for these programs have decreased (Benton, Robertson, Tseng, Newton, & Benton, 2003). This is particularly important for athletes because they are very unlikely to pursue college counseling services (Watson, 2005). Consequently, it is necessary to ensure that engagement and intervention services for mental health on college campuses are tailored to address the unique needs of athletes (i.e., adapt interventions to fit the culture of sport).
Inspired by the tenets espoused in Family Behavior Therapy (FBT; Donohue & Allen, 2011; Donohue & Azrin, 2011), The Optimum Performance Program in Sports (TOPPS) was initially developed in a clinical feasibility trial as an alternative intervention approach to traditional mental health service programs available to athletes (Donohue et al., 2014). In this initial pilot study, providers reliably examined TOPPS in the first 10 athletes who participated in the program. Results suggested that consumers were satisfied with intervention components while achieving concurrent goals specific to performance in both sports and mental strength and stability, including reduction of substance use and unsafe sexual activity. One of the cases in this study involved multiple baseline analysis to assist in the evaluation of specific components of TOPPS (Chow et al., 2014). The aforementioned case trial permitted details of intervention implementation to be disseminated and included systematic evaluation of intervention integrity, consumer satisfaction, and performance outcomes. However, intervention planning was restricted due to experimental design. Therefore, the current case examination depicts TOPPS administration in a collegiate combat sport student-athlete who participated in the Donohue et al. (2014) study. Unlike Chow et al. (2014), the current case was not limited by experimental restrictions, permitting an examination of intervention planning that was guided by the participant.
2 Case Introduction
Max presented to the program as an undergraduate combat sport athlete upon self-identification of alcohol use problems. At the time of the referral, Max was a full-time student and was not employed. Max aspired to win a national collegiate championship with his team and he reportedly enjoyed the physical aspects of combative sports.
3 Presenting Complaints
Max’s self-identified goal for seeking services at TOPPS was to cease his use of alcohol. He reported several recent negative consequences as a result of alcohol binge drinking, which included arguments with his friends and parents, a decline in his academic performance, loss of friendships, and an alcohol-related legal citation. Max was concerned about his desire to continue using alcohol despite his experiences with recurrent and aversive consequences. He experienced anger from his perceived inability to stop his use, indicating, “I am too weak to not want to do it” and upset with having to seek help to address his drinking behaviors. When he attended social activities, he reported pressure to use alcohol and discomfort when sober. He expressed that drinking alcohol had become a part of his life, and was regularly used to “deal with problems.” He reported blackouts, and that he was better off without his friends because they “turned their backs” on him due to his alcohol use.
4 History
The onset of Max’s alcohol use occurred when he was in high school. He reported that he initiated alcohol use as a way to “cope with life’s problems,” and he periodically drank to intoxicated states throughout high school and then “heavily” in college. He acknowledged that he felt pressured to drink alcohol because his social group was older than him and he wanted to impress them. He also experimented with cocaine, vicodin, oxycontin, Xanax, marijuana, psilocybin, codeine, and methyldioxymethamphetamine (i.e., “ecstasy”). The primary events just prior to Max seeking intervention services were negative consequences from alcohol use affecting his social relationships, a legal citation, and the urge to continue heavy alcohol consumption despite aversive consequences. Although Max reported that his grades in high school were affected by his use of alcohol, his academics in college had not yet been affected in the same way, according to him. Max reported that he enjoyed the feeling of letting his anger out through his combat sport.
5 Assessment
A comprehensive assessment battery was administered to the participant by a trained technician to establish a baseline, and assist in determining goals for the intervention program. Measures included (a) the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev; DSM-IV-TR; American Psychiatric Association [APA], 2000; SCID-IV) to determine the presence or absence of DSM-IV-TR Axis I disorders (First, Spitzer, Gibbon, & Williams, 2002); (b) a urine drug test to assess presence or absence of barbiturates, benzodiazepines, oxycodone, prescription amphetamines, and steroids; (c) a hair follicle drug test to assess the presence or absence of amphetamines, cocaine, marijuana, opiates, and phencyclidine (PCP); (d) the Timeline Followback (TLFB) to obtain information regarding the number of days of binge drinking, drug use, unprotected sex, the number of alcoholic drinks consumed and the number of legal citations (Sobell, Sobell, Klajner, Pavan, & Basian, 1986); (e) Beck Depression Inventory–II (BDI-II; Beck, Steer, & Brown, 1996) to assess mood during the past 2 weeks, with higher scores reflecting greater symptoms (items rated 0 to 3); (f) Symptom Checklist-90-Revised (SCL-90-R; Derogatis, 1994) to assess psychiatric functioning (items were rated on a scale from 0 = not at all to 4 = extremely); (g) Sport Interference Checklist (SIC; Donohue, Silver, Dickens, Covassin, & Lancer, 2007) to assess the extent to which various factors affect his training and competition in sport (items rated on a scale from 1 = never to 7 = always); and (h) Student Athlete Relationship Instrument (SARI; Donohue, Miller, Crammer, Cross, & Covassin, 2007) to evaluate problems in relationships of athletes with their teammates, family, coaches, and peers (items rated on a scale from 1 = strongly disagree to 7 = strongly agree).
Pre-Intervention Assessment Results
Table 1 includes pre-intervention assessment results. A standardized T score (M = 50, SD = 10) is presented for the SCL-90-R variables in parentheses next to the raw score and was based on the norms for male non-patients. TLFB results are presented as a ratio of the occurrence of each behavior per 30-day period to provide a standardized summary as the number of days included in the assessment period varied across time points.
Summary of Results for Substance Use and Mental Health.
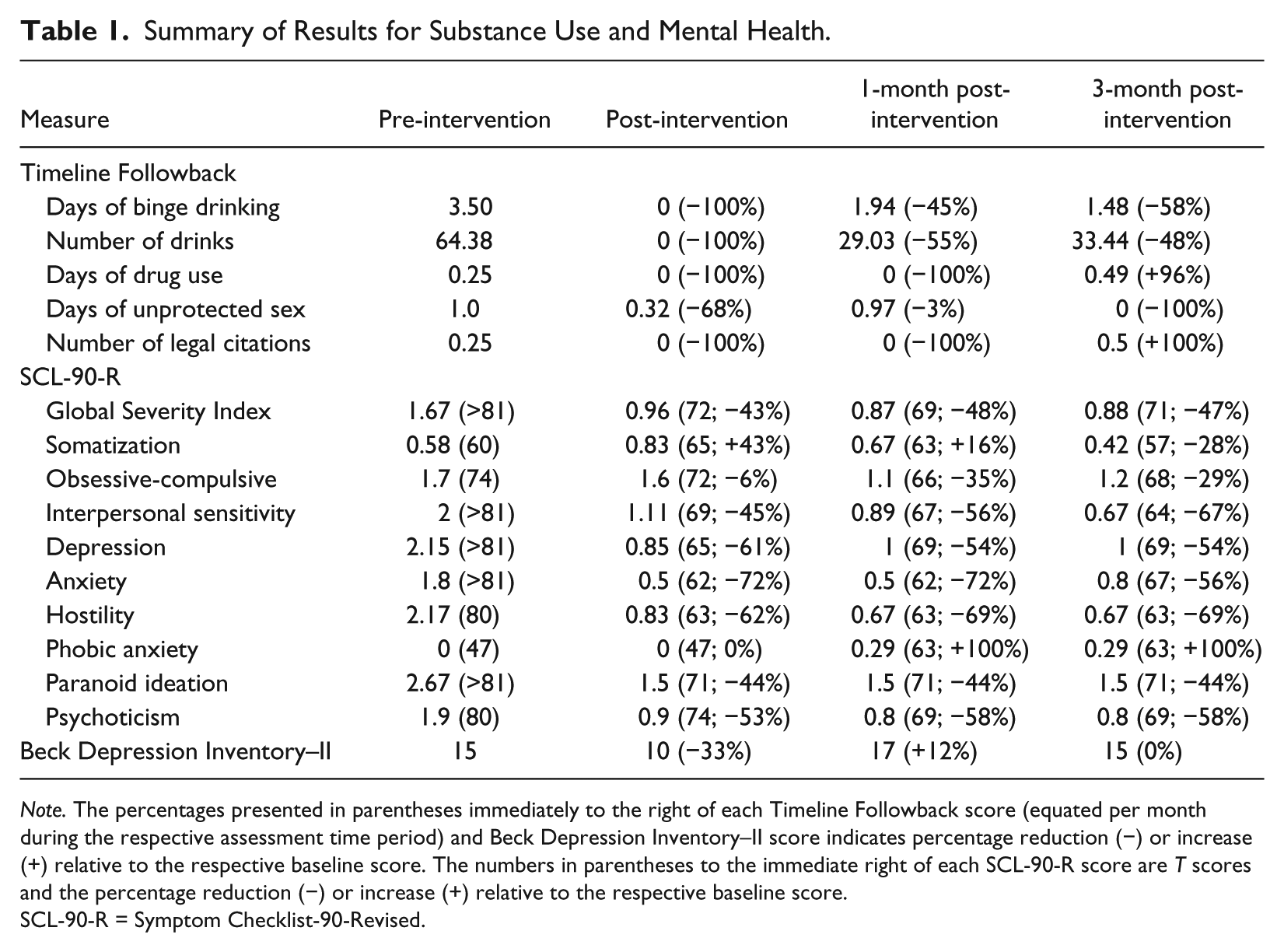
Note. The percentages presented in parentheses immediately to the right of each Timeline Followback score (equated per month during the respective assessment time period) and Beck Depression Inventory–II score indicates percentage reduction (−) or increase (+) relative to the respective baseline score. The numbers in parentheses to the immediate right of each SCL-90-R score are T scores and the percentage reduction (−) or increase (+) relative to the respective baseline score.
SCL-90-R = Symptom Checklist-90-Revised.
The SCID-IV pre-intervention assessment indicated that Max evidenced DSM (4th ed., text rev.; DSM-IV-TR; APA, 2000) diagnostic criteria for current alcohol dependence. On the TLFB, Max reported 3.5 days per month of binge drinking and 64 alcohol beverages per month. He also reported 0 days of cannabis use, 0.25 days per month of other drug use, one instance per 30 days of unprotected sex, and 0.25 legal citations per 30 days (1 legal citation during the 4-month period). Biological measures of substance use were negative and remained negative at the post-intervention assessments. Pre-intervention assessment T score results for the SCL-90-R were elevated (i.e., 1 SD or more above the mean of 50) on the Global Severity Index, which is a single quantitative indicator of the status of psychological distress. His score was highly elevated and corresponded to the 99.9th percentile. Max’s scores were also elevated on a number of symptom constructs including (listed in order of highest to lowest elevation: Interpersonal Sensitivity, Depression, Anxiety, Paranoid Ideation, Hostility, Psychoticism, Obsessive-Compulsive Symptoms, and Somatization). The elevated Depression construct was consistent with his BDI-II total score of 15, which corresponds to mild depression.
The SIC scores indicated that Max was generally experiencing interferences in his sport training and competition at average levels, although his scores on Dysfunctional Thoughts and Stress and Injury Concerns in the competition domain were elevated over 1 SD above the mean, indicating that he was experiencing interferences in these areas. SARI subscale scores for Family, Coach, and Peers and Teammates suggested an overall lack of problems in these relationships. However, examination of items indicated that Max did endorse teammates and peers encouraging him to drink alcohol, and feeling that he was not living up to the expectations of at least one of his family members.
6 Case Conceptualization
Max’s alcohol use was conceptualized to be influenced by a variety of factors, including social norming, modeling/social learning, desire for acceptance from others, and classical and operant conditioning, all of which maintained his use until recent negative consequences began to outweigh the reinforcing effects of alcohol. His alcohol use began in high school as a way to connect with older peers and engender feelings of acceptance. Max reported that his older friends introduced him to alcohol use and modeled acceptance and utility of drinking in social settings. In high school, his drinking was positively reinforced through his peer relationships and ability of alcohol to lessen anxiety and discomfort emanating from interpersonal insecurities (negative reinforcement). As Max transitioned into college, his alcohol consumption continued to elevate and became a normal part of his routine and activities with peers. Indeed, “hanging out” with other friends who used alcohol led him to erroneously believe that his heavy use of alcohol was a natural part of the culture of college. Although aversive consequences occurred due to alcohol use, such as hangovers or feeling upset with alcohol use, it was not until Max became alienated from his peer group due to frequent alcohol intoxication that he desired to reduce his use. Max’s alcohol use contributed to his engagement in unprotected sexual activity, placing him at risk for HIV/sexually transmitted infections (STIs). He also reportedly engaged in alcohol use to assist in managing worrisome thoughts.
7 Course of Intervention and Assessment of Progress
Max attended all 12 of his scheduled meetings at TOPPS. His parent attended most of these scheduled meetings, and a friend attended 1 of the meetings. Each meeting lasted between 60 and 90 min and occurred across a 3-month period. To integrate the field of mental health more fluidly with athletics, professionals at TOPPS utilized positively focused nomenclature (therapists instead of “performance coaches,” “intervention meetings” instead of “treatment sessions,” and problems were resurrected as goal-oriented behaviors). These changes were performed to assist in diminishing the stigmatizing nature many athletes ascribe to counseling (see Lopez & Levy, 2013). The intervention plan consisted of a battery of components that were administered successively and cumulatively based on Max’s intervention goals. That is, intervention components were added with the passage of time, but reviewed to a progressively lesser extent relative to their initial implementation. The primary behaviors targeted in each of these intervention components, his response to each of these components, and the support provided by the attendance of his significant others are summarized below.
Meeting Agendas
An agenda was established at the start of each meeting outlining the components to be implemented and the expected duration of each component. Max was encouraged to suggest potential modifications to agendas, although he did not request changes to any of the agendas. After the intended components were reviewed, the provider (i.e., performance coach) solicited a positive mind-set from Max. In this exercise, Max was instructed to provide an example of something that had gone well for him during the previous week and to indicate any outstanding efforts or personal accomplishments since the last meeting. Max appeared to enjoy this exercise and was quick to point out positive experiences or accomplishments, such as abstinence from alcohol over the past week or ample time spent studying. His parent provided additional positive experiences involving him and Max. The agendas assisted in maintaining meeting efficiency, limiting extraneous dialogue due to enhanced focus. Nevertheless, tangents occurred at times. His parent was clearly passionate about Max’s well-being and exhibited a tendency to provide lengthy advice as to how Max could better accomplish his goals. In these circumstances, his parent was redirected to focus on Max’s identified goals and the prescribed intervention component that was prepared for the agenda. Redirection techniques were implemented upon each instance of diversion from the prescribed topic, and the parent was able to enhance on-task support over time.
Meeting Conclusion
A prescribed meeting conclusion exercise was implemented in each of the last six meetings, providing an opportunity to ensure that assignments were understood, solicitation of supportive others to include during the upcoming meeting, construction of a tentative agenda and scheduling for the next meeting, solicitation of positive things that occurred during the meeting, and inquiring what Max looked forward to in the coming week. Max would often comment on a part of the meeting he found most helpful, for instance, planning how to have fun without using alcohol. He attended weekly meetings until the program concluded at 12 meetings.
Program Orientation (Meeting 1)
On the first meeting, a structured orientation was administered to provide information about the intervention program, including its structure and communication guidelines. During the Program Orientation, Max was queried regarding his feelings about the intervention program and his referral to the program, which assisted in better understanding his unique needs and his desire for improvements throughout the program. Program intervention components were briefly described. He expressed agreement to adhere to guidelines of the program, including attendance to all meetings, active participation in meetings, completion of program assignments, and compliance with communication guidelines.
Cultural Enlightenment (Meeting 1)
Cultural enlightenment involved establishing rapport by discussing Max’s perceived ethnic identity, important positive and negative experiences resulting from his ethnic culture, and how his culture could be considered during the implementation of the program. This conversation was facilitated by examining his responses to the Semi-Structured Interview for Consideration of Ethnic Culture Scale (SSICECS; Donohue et al., 2006) and subsequently discussing his responses to each item. Max was provided with validation and empathy for upsetting experiences, and positive experiences due to his ethnic background were embraced. His parent was present during Cultural Enlightenment and was instrumental in providing a full picture of how Max developed and interpreted his cultural identity. His parent provided perspective on the experience of observing Max come to an understanding of his cultural identity, which was described as a unique mix of cultural and ethnic backgrounds. This intervention component has been shown to enhance rapport and satisfaction with the interviewer (Donohue et al., 2006).
Dynamic Goals and Rewards (Meetings 2-12)
Dynamic goals and rewards are established collaboratively with the athlete and supportive other and monitored in all subsequent meetings. Results from the baseline assessment were reviewed regarding item and subscale elevations, and Max’s responses to these items were subsequently reviewed during the second meeting with him. The goals component was implemented in 11 meetings, utilizing the first 2 meetings to determine optimal goals and strategies for their attainment that were solicited from Max. Subsequent meetings were focused on goal progress. Max was also prescribed program goals that have been found to be important for college athletes (i.e., avoid alcohol and illicit drugs, maintain positive relationships, safe sexual behaviors, abstain from gambling, maintain positive communication, meeting attendance, ensuring a supportive other is available to attend meetings, completion of practice assignments). Throughout the program, some of Max’s goals changed to reflect differences inherent to sport training and the academic semester. Six of his goals were related to sport training (e.g., going to the gym) and five goals reflected academics and relationships (e.g., study time and activities). Once established, Max’s goals were reviewed in every meeting to determine progress in goal achievement and discuss how goals may be modified or prioritized from week to week. During meetings where Max’s parent was present, his parent provided feedback on how Max could optimally accomplish his goals. For instance, Max set a goal to engage in productive activities to assist in reducing boredom that would often act as a trigger for using alcohol, and his parent offered to assist in generating goal-compatible activities. Throughout the program, it was evident that Max made progress on his goals and that he was committed to reducing his alcohol use. This intervention component enabled Max to increase his skill in avoiding alcohol use and brainstorm options incompatible with drinking. The format of this intervention (i.e., having a list of potential goals and a menu of potential rewards for goal accomplishment) permitted Max to change his goal focus each week and to be contingently rewarded for exceptional efforts in accomplishing a higher percentage of goals. For instance, one week he accomplished about 80% of his goals, and he received about 80% of the available rewards from his parent. Thus, goals and rewards are dynamic from week to week.
Performance Planning (Meeting 3)
This collaborative approach to intervention planning provides an opportunity for the athlete to set the priority of intervention component implementation. Performance Planning was implemented in the meeting, following the establishment of dynamic goals. All TOPPS components were briefly described to Max, and he was queried to indicate how he believed each component might be able to assist him in reaching his goals. Next, he ranked all six components regarding implementation priority and indicated how he arrived at each ranking. Max ranked the following components, listed here in order of his priority: Environmental Control, Self-Control, Positive Request, Financial Management, Reciprocity Awareness, and Career Planning and Job-Getting Skills Training. Max was informed that the intervention components would be administered in the order in which he rated them and that he would have the opportunity to adjust the order and/or amount of time spent on the individual components in situ.
Environmental Control (Meetings 8, 10, and 12)
This intervention component protocol is utilized to identify, monitor, and eliminate or control stimuli that have led to goal-incompatible behaviors in the past, and identify, monitor, and increase time spent with stimuli that are goal-compatible people and activities. This component was implemented during three meetings, where Max exemplified skill in identifying goal-compatible behaviors that included specific family members and friends, athletic activities, and a variety of activities incompatible with alcohol use. During the first meeting this component was implemented, Max identified goal-incompatible behaviors, which were related largely to alcohol use and situations associated with upset in his relationships with others. After identification of goal-compatible and incompatible behaviors, Max brainstormed ways to ensure that he was spending more time engaged in behaviors on the goal-compatible list and less time engaged in behaviors on the goal-incompatible list. In subsequent weeks, Max demonstrated success in his ability to avoid many situations in which he typically would have consumed alcohol (i.e., attending parties and spending time with specific friends). Therefore, much of the discussion involved increasing plans to engage in goal-compatible activities that replace the social function of alcohol use. After creating the list of goal-compatible and incompatible behaviors and brainstorming ways to engage in goal-compatible behaviors while avoiding goal-incompatible behaviors, Max was instructed to mark the days he engaged in the behaviors on this list over the next week. Max tracked the listed behaviors for the subsequent 2 weeks, and these monitored behaviors were reviewed in Meetings 10 and 12. During the discussion of his behavior tracking, he reported how he was able to engage in his goal-compatible activities and was provided with descriptive praise. For instance, he participated in social events with his family, and avoided environments where he previously engaged in alcohol use and other problem behaviors and thoughts. He reported goal-incompatible activities and skills he utilized to avoid alcohol use and other problem behaviors and thoughts. He was assigned to practice these skills outside of meetings.
Self-Control (Meetings 7 and 9)
Self-control was utilized during two meetings and was utilized to teach the skill of gaining awareness, and then managing triggers for negative thoughts, images, feelings, and behaviors that lead to impulsive behaviors (e.g., substance use, negative thoughts that impede sport performance, arguments). Alcohol use was targeted in this intervention component, and Max was taught to engage in a sequence of actions to manage his triggers to drink, and included stating “stop” aloud forcefully upon the first image, urge or desire for alcohol use (i.e., thought stopping), thinking of a negative consequence specific to Max as well as others who are loved, relaxation (diaphragmatic breathing), generating non-alcohol-related alternatives, generating good things and bad things about each alternative, describing what it would be like to implement the chosen non-alcohol-associated alternative successfully (imagery), describing someone who is loved reacting positively to being told that Max had avoided alcohol use, and describing several reinforcing aspects specific to having avoided alcohol use in the respective situation. The steps involved in this component were first modeled in the meeting by the performance coach, and then Max demonstrated the steps using the scenario of arriving at a social event and avoiding alcohol use. He rated how well he felt when he accomplished each step during the role-play on a scale of 0 (forgot the step) to 100 (perfect, couldn’t get any better), and the performance coach and Max’s parent provided feedback specific to what was performed well and how he might improve his self-control skill sets in for the future. Max reported that utilizing self-control would significantly reduce his likelihood of drinking, and believed thought stopping and relaxation steps were the most important steps for him. Although Max was encouraged to use the self-control component to assist impulsive behaviors and thoughts that were not specific to substance use, Max desired to utilize self-control for alcohol use only.
Reciprocity Awareness (Meetings 11 and 12)
The underlying assumption of this intervention component is that positive relationships are based on reciprocal reinforcement. This component consists of Max and his supportive others exchanging things they “admired, respected, or loved” about one another, including personal qualities or actions performed. Reciprocity awareness is geared at enhancing or maintaining positive relationships between athletes and their significant others, as well as addressing underlying issues associated with resentment and miscommunication, and building positive atmosphere in meetings. Behavioral shaping was utilized to encourage Max and his parent to only express positive qualities about each other, and reframe from statements that suggested the other person was not meeting expectations or doing enough of the activity or quality appreciated.
Positive Request (Meetings 10-12)
This intervention component aims to improve positive communication by teaching effective and appropriate techniques when making requests of others. Positive request involves a series of nine implementation steps, each intended to increase the likelihood that the person receiving the request will be motivated to comply (i.e., request a specific action, state how it would be difficult for the person to do what is requested, state how it would be beneficial for other person if request performed, state how it would be good for you if request performed, offer to help the person get the request done, offer to do something for recipient, express appreciation if other person were to complete request, suggest something that would be an alternative action, ask the other person to suggest an alternative if request will not be performed). This skill was reviewed several times throughout intervention. The performance coach first modeled a request that was specific to Max asking his non-participating parent to stop asking him to repeatedly do a common task. Max then practiced making requests to supportive others. Upon receiving requests from others, Max was taught to report what he liked about how the request was made and to initiate a positive request of his own until compromise was achieved.
Post-Intervention Assessment Results
Post-intervention assessment results are presented in Table 1 with the exception of SIC and SARI results because these scores were essentially the same as those obtained on this measure during baseline. After intervention, a post-assessment was administered (91 days after pre-intervention assessment). Max reported complete abstinence from alcohol and drug use. A 68% reduction was indicated for instances of unprotected sex (from 1.0 to 0.32 per 30 days). Post-intervention assessment T score results for the SCL-90-R indicated that all of the pre-intervention elevated symptom constructs reduced with the exception of Somatization (T score increased from 0.58 to 0.83). Specific to his overall psychological distress, the Global Severity Index score was reduced by 43%, which corresponds to a T score reduction from over 3 SDs above the mean to just over 2 SDs above the mean. Symptom construct reductions were observed in Anxiety (72%), Hostility (62%), Depression (61%), Interpersonal Sensitivity (45%), Paranoid Ideation (44%), Psychoticism (53%), and Obsessive-Compulsive (6%). Max’s improvement from pre- to post-assessment on the Depression construct was reflected in a BDI-II total score reduction of 33% (from mild down to minimal depression).
8 Complicating Factors
One common factor that negatively affects comprehensive performance programming with student-athletes is the intensive time demands placed on them, which can act as a barrier to seeking assistance from programs such as TOPPS (Lopez & Levy, 2013). Indeed, Max reported intensive time commitments; he had to manage job shifts and schedule training, classes, homework, and personal time with others. His supportive others also reported busy schedules that were not consistent with Max’s schedule. Moreover, his supportive others initially appeared to underestimate the importance of their participation in Max’s intervention planning, perhaps lowering their enthusiasm for meeting attendance. To assist his supportive others in understanding why their meeting attendance was important, Max was instructed to indicate to them how their attendance was appreciated during Reciprocity Awareness, and that their support was important to his goal achievement when reviewing Dynamic Goals and Rewards. The role of significant others was also extensively reviewed during the initial engagement calls to both Max and his supportive others, and during the Orientation meeting. Time management issues were addressed by teaching Max to plan events during his review of Dynamic Goals and Rewards and Environmental Control.
9 Access and Barriers to Care
Research has demonstrated that when family members are incorporated into intervention planning more favorable outcomes can be obtained (Sisson & Azrin, 1986). However, parents and other close friends of student-athletes may reside out-of-town or evidence schedules that are very different from student-athletes, which adds an additional barrier for attendance. To enable Max’s parent to attend more meetings, conference phone calls were utilized in which his parent called during any portion of the meeting in which the parent was availabile. Phone participation was useful in supporting Max’s performance goals, even when these phone calls were brief. Problems getting to meetings were also minimized by permitting Max to attend meetings on-campus between classes and extending meeting availability as recommended by others (Lopez & Levy, 2013). Max requested to have more than 12 meetings in the program, but due to institutional review board policy, he was referred to a campus counseling program. His request, however, ultimately resulted in an extension of up to 3 meetings for all future participants when desired by athletes.
Meeting confidentiality of participants by mental health professionals is protected by both federal and state laws (with a few exceptions, including harm to self and others and court subpoenas). However, in conducting family-based interventions, this concern becomes difficult to manage. Therefore, the performance coach was trained to avoid disclosure of information provided in confidence by Max when supportive others were involved in the meetings, and meeting conversations were oriented to reviewing positive accomplishments and efforts to attain future goals through skill development.
10 Follow-Up
Summary Comparison of Pre-Intervention and Post-Intervention Assessments
Two follow-up assessments were administered approximately 1 month and 3 months after the conclusion of intervention to determine whether intervention effects were sustained over time (results are available in Table 1). There were substantial reductions in TLFB alcohol use from pre-assessment through the follow-up assessments, despite a small increase after the conclusion of intervention. At the first follow-up (1 month post-intervention), decreases from the pre-assessment were observed: Days of binge drinking decreased 45%, number of drinks decreased 55%, and instances of unprotected sex decreased 3%. Days of use of other drugs, cannabis use, and number of legal citations were all 0. At the second follow-up (3 months post-intervention), decreases from the pre-assessment were found: Days of binge drinking decreased to 58%, and number of drinks decreased to 48%. Days of cannabis use and instances of unprotected sex were 0 at the second follow-up. There was 1 day of other drug use and one legal citation reported at the second follow-up.
Reductions in psychiatric symptoms of the SCL-90-R were largely maintained at the two follow-ups. One exception was the Phobic Anxiety scale, which increased from the previous time points; however, at the pre- and post-intervention assessment, the score was the lowest subscale possible (0) and the follow-up assessment results (.29) were in the average range (T score = 63). After an initial large reduction from pre- to post-intervention, the BDI-II scores at the follow-ups were similar to the scores at baseline. Results for SIC and SARI did not show notable changes from pre- or post-intervention assessments to the two follow-up assessments.
11 Performance Programming Implications of the Cases
This case demonstrates the utility of parental involvement when attempting to accomplish life and sport goals in college student-athletes. The awareness of Max’s parent to specific intervention goals and the supportive behaviors that were explicitly identified during meetings enhanced generalization of Max’s cognitive and behavioral skills outside of meetings, and created an environment where Max was held accountable for goal progression. His parent provided contingent support for goal accomplishments that were meaningful and naturally present in the environment. This case exemplifies the importance of addressing sports as a central focus when managing concerns that are traditionally seen in campus counseling centers. Indeed, doing so appeared to enhance Max’s pursuit of intervention through the process of de-stigmatization. Along these lines, athletes often acknowledge the importance of managing mental aspects in their sport. However, utilization of programs that are aimed at developing their mental skill sets may be low due to anticipated stigma associated with psychologically based treatment programs (Donohue et al., 2013; Lopez & Levy, 2013). Therefore, intervention components within TOPPS, as well as the positive style of TOPPS’ performance coaches, offer a unique positive alternative to traditional counseling regimes.
12 Recommendations to Clinicians and Students
Max’s case adds to our knowledge-base that TOPPS can help collegiate athletes avoid alcohol use and accomplish other important pro-social goals. It is likely that the substantial declines in psychiatric symptoms were assisted by Max’s reduction in alcohol use, as ample research indicates that psychiatric symptoms co-occur with alcohol misuse. Although Max’s scores measuring potential interferences in his sport training and competition were not a central area of symptom reduction, the incorporation of sport performance into intervention likely contributed to intervention engagement and retention and bolstered his motivation for intervention goals outside of sports. Indeed, discussing Max’s athletic ambitions and involvement assisted in quickly building rapport and assisted in understanding his approach to goal achievement and life perspective. The goals Max selected for sport performance enhancement were apropos for comprehensive approaches recommended by many scholars who find intervention is most successful when a variety of health behaviors are simultaneously targeted in intervention.
Overall, this case demonstrates several important considerations. First, data in this case example suggest that TOPPS is adaptable in managing various mental-health-oriented goals. Targeting alcohol use through several types of intervention components was useful for Max to build skills in avoiding alcohol use as well as weekly tracking of behaviors that are incompatible with drinking. However, it is important to indicate that TOPPS, like other mental health programs, is not a definitive intervention. In this study, Max improved in most of the outcome measures across time, especially while he was receiving intervention. Nevertheless, relapse in substance use is a common phenomenon and Max’s case demonstrated recurrence of substance use. Given that he requested additional meetings, it may be that the dosage of TOPPS should be increased for some athletes, which may have prevented drug use that was detected during the last follow-up assessment. Occasional “booster” sessions would be another viable option to maintain intervention gains and support generalization of skill sets. In this study, booster meetings would have interfered with the AB study design. However, research indicates the utility of such methods to reinforce intervention gains (Whisman, 1990).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grant from the National Institute on Drug Abuse (1 R01DA031828, PI Donohue).