
Abstract
The current case study describes the longitudinal assessment of a young child diagnosed with Partial Fetal Alcohol Syndrome and pervasive developmental disorder–not otherwise specified. The patient participated in an applied behavior analysis (ABA)–based Verbal Behavior treatment program to target communication impairments and functional skill deficits. Because ABA-based interventions have demonstrated efficacy in improving levels of functioning across various developmental disabilities, it was reasonable to assess the clinical utility of these same strategies when applied to a patient presenting with fetal alcohol spectrum disorder and associated developmental delays. The current study relied on quasi-experimental single-subject design methods to measure treatment outcomes and to inform clinical decision making. Dependent measures in the study included standardized, norm-referenced assessments of cognitive and adaptive functioning, as well as behavioral data collected throughout treatment to measure gains across skill areas. Outcomes included rapid skill acquisition across several areas of functioning (e.g., expressive and receptive language, visual-performance, and adaptive emotional/behavioral functioning). The impact of treatment on global areas of functioning will be reported.
1 Theoretical and Research Basis for Treatment
Early and intensive intervention rooted in applied behavior analysis (ABA) is a widely utilized and researched area in the treatment of individuals with developmental disabilities. Defined as the scientific study of the effects of environmental variables on socially significant behavior, the field of ABA is devoted to assessing and treating socially significant behaviors to produce behavioral and developmental improvements (Cooper, Heron, & Heward, 2007).
Important components of most behavior analytic interventions include the systematic break down of skills into simpler parts that can be taught through behavioral contingencies. It is important to note that ABA is not one single intervention but, rather, an approach to treatment that encompasses a variety of empirically supported techniques and interventions. The application of ABA-based interventions can vary widely based on the needs of the individual with differing levels of treatment intensity (e.g., frequency of sessions, number of teaching trials per session), structure of teaching (e.g., in contrived teaching trials or within a more natural environment), therapist to child ratio (e.g., one-on-one instruction, small or large group), and setting (e.g., within the home, clinic, or school; Rogers & Ozonoff, 2006). The practice of ABA therapy is commonly recognized and promoted as the most evidence-based body of treatments for improving functioning in individuals with autism spectrum disorder (ASD; National Autism Center, 2015), though the application of ABA-based interventions is not limited to this population (Sturmey, 2002).
The Verbal Behavior (VB) approach is an ABA-based intervention aimed at improving language and adaptive skills in individuals with developmental disabilities (LeBlanc, Esch, Sidener, & Firth, 2006). The VB approach is derived from the work of B. F. Skinner (1957) who proposed that language is a learned behavior that is under the functional control of environmental variables and is socially mediated by others. The VB approach can be used to target both verbal and non-verbal behavior. Non-verbal behavior that is often targeted through a VB program includes receptive language skills, imitation skills, and visual-performance skills (Barbera & Rasmussen, 2007). Verbal behavior typically targeted for intervention includes requests, labels, conversation skills, and vocal imitation. As with many evidence-based behavioral interventions a variety of intervention methods based in ABA, such as incidental teaching, natural environment teaching, and discrete trial instruction are used to target verbal behavior skills.
Currently, most empirical literature supporting the VB approach consists of single-subject experimental designs that have demonstrated the impact of treatment on specific language skills (Sautter & LeBlanc, 2006). However, a recent survey of behavioral practitioners found that 23% described their programming using the term Verbal Behavior and almost 50% indicated their programming was based on Sundberg and Partington’s manual (1998), which is widely known as a VB manual (Love, Carr, Almason, & Petursdottir, 2009). Given the ubiquity of use of the VB approach, more research is needed to show outcomes associated with the approach.
Like autism, fetal alcohol spectrum disorder (FASD) is conceptualized as a spectrum disorder of alcohol damage and alcohol-related effects encompassing a range of diagnoses including fetal alcohol syndrome (FAS), fetal alcohol effect, partial fetal alcohol syndrome (pFAS), alcohol-related birth defects, and alcohol-related neurodevelopmental disorder (Clarke & Gibbard, 2003). FASD is a term used to describe the continuum of physical malformations and cognitive impairments caused by maternal alcohol consumption during pregnancy. Diagnostic criteria for a FAS diagnosis require documentation of facial abnormalities, growth deficits, and central nervous system (CNS) abnormalities (Bertrand et al., 2004). In addition to the physical features described above, diagnostic criteria for making an FAS diagnosis include global cognitive deficits (e.g., IQ two standard deviations below the mean), or deficits in at least three specific functional domains (e.g., specific learning disabilities, uneven profile of cognitive skills, discrepancy between verbal and non-verbal skills, academic underachievement, or poor information processing). A diagnosis of pFAS may be conferred if an individual has documented evidence of prenatal alcohol exposure and meets three out of the four aforementioned criteria for a diagnosis of FAS (i.e., facial dysmorphia, cognitive impairments, CNS abnormalities; Banakar, Kudlur, & George, 2009).
Language impairments are present in some children diagnosed with FASD and may include weakness in language production, oral-motor deficits, poor articulation, and difficulties with comprehension (McGee, Bjorkquist, Riley, & Mattson, 2009). Children affected by prenatal alcohol exposure may have difficulties encoding information that impacts their understanding, as well as organizing and presenting information to retell an event or present a cohesive narrative (Coggins, Timler, & Olswang, 2007). In addition, delays in social communication, complex language, and conversational speech may result in more significant impairments in social interactions, the development of friends, and academic success (Kelly, Day, & Streissguth, 2000).
Social deficits observed in children with FASD may include socially inappropriate behavior and difficulty with peers, rather than those social deficits that are characteristic of children with ASD (e.g., difficulty initiating social interactions, expressing and understanding emotion, and using non-verbal communication; Bishop, Gahagan, & Lord, 2007). Still, given the aim of ABA-based interventions to promote improvement in socially significant behavior, similar interventions used to target social deficits of children with ASD may be warranted in treating the unique social deficits characteristic of children with FASD.
2 Case Introduction
The current report offers a case study examining the outcomes of an ABA-based intervention over the course of a year and a half with a child diagnosed with pFAS and pervasive developmental disorder–not otherwise specified (PDD-NOS). Because ABA-based interventions have demonstrated efficacy in improving levels of functioning across various developmental disabilities, it was reasonable to assess the clinical utility of these same strategies when applied to a patient presenting with PDD-NOS and additional symptoms specific to her diagnosis of pFAS. The current study relied on scientifically based single-subject design methods to measure treatment outcomes and to inform clinical decision making.
3 Presenting Complaints
Kate was a 3 year-, 10-month-old female. Results of diagnostic evaluation confirmed prenatal alcohol exposure, evidenced by alcohol exposure–related dysmorphia and significant cognitive impairments. Kate exhibited significant communication deficits, impairments in social interactions, and emotional and behavioral problems. Upon initial evaluation, Kate was diagnosed with pFAS and PDD-NOS. Changes in diagnostic criteria according to the American Psychiatric Association (APA, 2013) resulted in a change in diagnosis from PDD-NOS to autism spectrum disorder (ASD), which occurred after Kate was discharged from treatment.
4 History
Medical records indicated that Kate was born at 39 weeks gestation through Caesarean section. Her birth weight, length, and head circumference fell within normal limits. Following her delivery, Kate experienced respiratory distress syndrome with pneumothorax and a collapsed lung; she was treated with oxygen. Kate came into the care of a relative at 3 years of age due to concerns of biological caregivers’ alcohol abuse and alleged neglect. Minimal information regarding Kate’s medical and developmental history prior to age 3 was reported.
5 Assessment
Prior to starting treatment, Kate underwent an interdisciplinary evaluation to gauge her overall level of functioning and determine the effects from prenatal exposure. The evaluation was conducted by a separate, independent clinic that specializes in the assessment of FASD. Clinicians who conducted Kate’s psychological evaluation had no involvement in the treatment decisions or procedures described in this report. Dependent measures reported in the current report included standardized, norm-referenced assessments that were collected by professionals who were not involved in Kate’s treatment. These assessments were administered on three separate occasions—prior to starting treatment, after 9 months of treatment, and one month before discharging from treatment (following 23 months of treatment). The battery of standardized assessments that examined changes in Kate’s level of functioning throughout the duration of her treatment included measures of intellectual, adaptive, and emotional/behavioral functioning.
Standardized Assessment of Intellectual Functioning
To gauge Kate’s level of intellectual functioning, she was administered the Differential Ability Scale, Second Edition (DAS-2) at the time of initial evaluation. The DAS-2 is a norm-referenced assessment used to report an individual’s level of cognitive functioning across several domains, compared with aged-matched peers. For all ability clusters (i.e., General Conceptual Ability, Verbal cluster, Non-Verbal Reasoning cluster, and Spatial cluster), scores are reported as standard scores, with a mean score of 100 (SD = 15). A summary of Kate’s scores on the DAS-2, assessed at each time point, appear in Table 1.
Standardized Assessment of Intellectual Functioning.
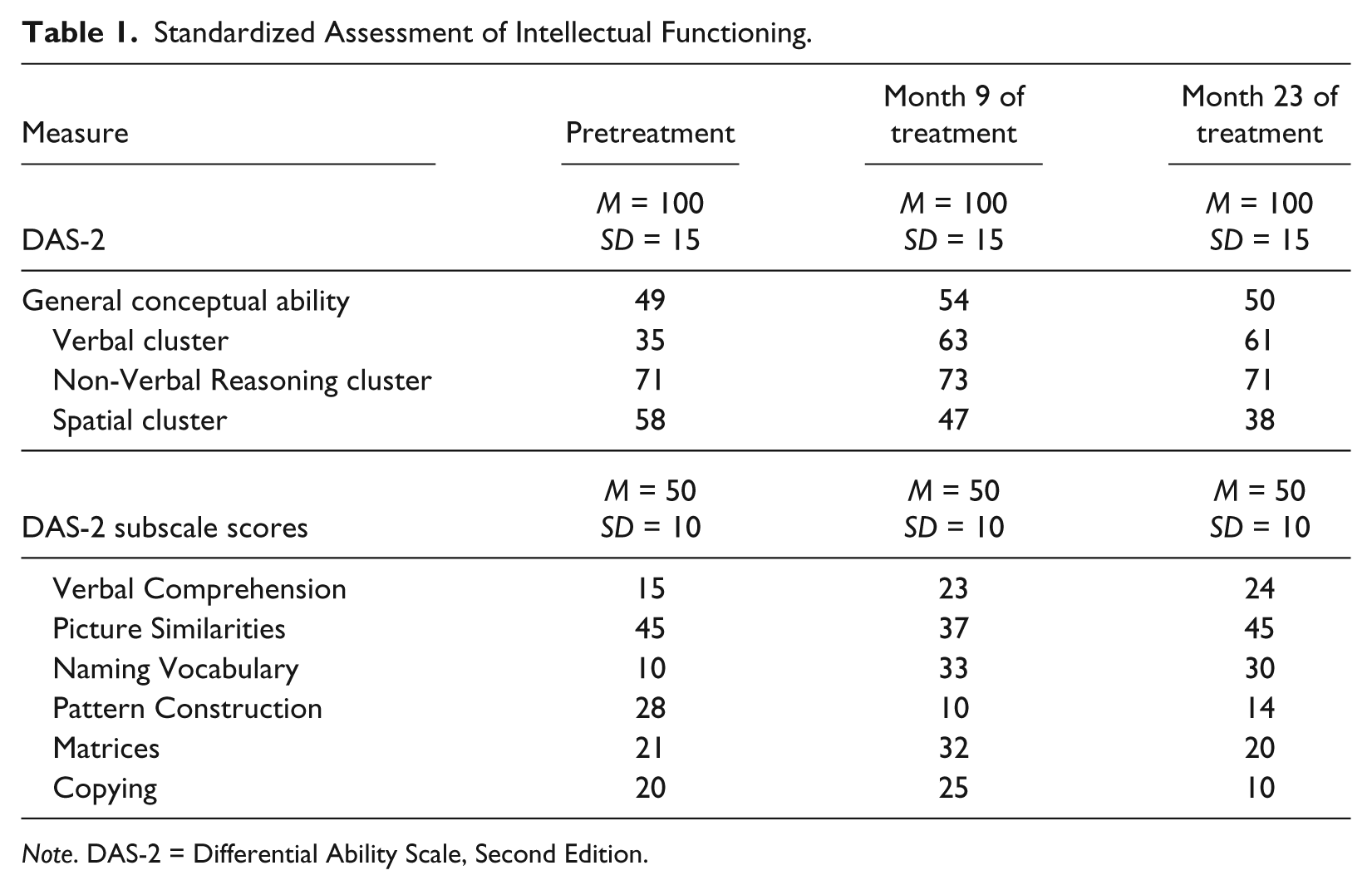
Note. DAS-2 = Differential Ability Scale, Second Edition.
The pretreatment assessment of Kate’s cognitive abilities, as reported on the DAS-2, indicated that her abilities across most measured domains fell within the extremely low range (i.e., General Conceptual Ability, Verbal cluster, and Spatial cluster). Of note, a review of medical records indicated there were no other medical factors or genetic conditions identified at the time of the evaluation that would impact her cognitive functioning, such as the presence of visual impairments that may negatively affect visual-spatial performance. An area of relative strength for Kate was reported in her Non-Verbal Reasoning skills, which fell within the borderline range. Overall, Kate’s intellectual functioning was significantly below those of her same-aged peers, indicating that she likely required high levels of individualized support in educational settings. Performance on cognitive assessments was consistent with Kate’s initial clinical presentation and her performance on behavioral assessments conducted prior to starting treatment; the results of the psychological evaluation were likely an accurate representation of her level of global functioning.
Standardized Assessment of Adaptive Functioning
Adaptive functioning describes an individual’s ability to complete daily-living tasks at a level that is expected based on age and developmental level. Adaptive behavior encompasses conceptual skills (academic skills, communication, and understanding of concepts such as time and money), social skills, and practical life skills (e.g., personal hygiene, feeding, and occupational skills). The Vineland Adaptive Behavior Scale, Second Edition (Vineland-2) is a measurement of adaptive functioning that is administered in an interview format; parents, caregivers, and teachers serve as respondents during the administration of the Vineland-2 and provide reports of the individual’s behavior and functioning. Kate was administered the Vineland-2 on three separate occasions and her primary caregiver was the informant. Scores on the Vineland-2 are reported as standard scores (M = 100; SD = 15) and include an overall Adaptive Composite, as well as four separate domains: Communication, Daily Living, Socialization, and Motor. Kate’s level of adaptive functioning as reported by the Vineland-2 appear in Table 2.
Standardized Assessment of Adaptive Functioning.
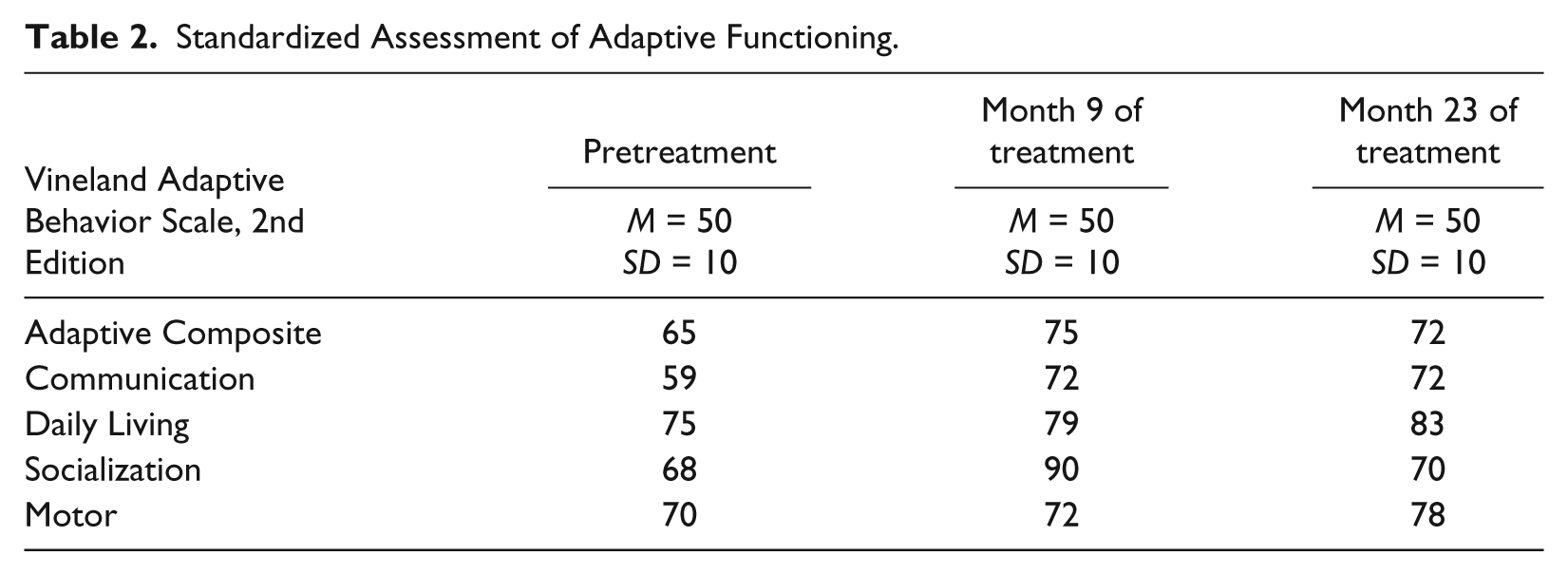
At the time of initial assessment, Kate displayed impaired levels of adaptive functioning and her performance on most of the assessed areas was significantly below those of same-aged peers. Her overall level of adaptive functioning (Adaptive Composite) was in the below average range, with most significant impairments present in the areas of Communication and Socialization. She also displayed lower-than-expected levels of functioning in the areas of Daily-Living Skills and Motor Skills. Overall, Kate’s initial level of adaptive functioning was consistent with her reported level of intellectual functioning, which suggested that she was likely to require high levels of support across most areas of functioning.
Standardized Assessment of Emotional/Behavioral Functioning
Several standardized measures of Kate’s emotional/behavior functioning were obtained throughout the course of her treatment and were reported by her parent and teacher on several occasions. The first set of parent and teacher ratings of Kate’s behavior included the Achenbach Child Behavior Checklist–Preschool (CBCL-Preschool), which assesses the behavior of children aged 18 months to 5 years of age and compares scores to a normative sample based on the child’s age. Scores on the CBCL are reported as T-scores, with the average score being 50 (SD = 10). A composite score is provided for Total Problems, as well as an Internalizing domain and Externalizing domain. Composite scores are derived from subscales including Emotional Reactivity, Anxious/Depressed, Somatic Complaints, Withdrawal, Sleep Problems, Attention Problems, and Aggressive Behaviors. Parent and teacher reports of Kate’s behavior, as measured on the CBCL-Preschool, are summarized in Table 3.
Standardized Assessments of Emotional/Behavioral Functioning.

At the time of the baseline assessment, Kate was not yet enrolled in school; as a result, a pretreatment report of behavior was not obtained from a teacher. Changes in behavior throughout treatment, as reported by Kate’s parent and teacher, appear in Table 3. Prior to starting treatment, Kate’s emotional/behavioral functioning, as reported by her caregiver, was significantly impaired. Kate was reported to display elevated levels of both Internalizing and Externalizing problems, resulting in a clinically significant level of Total Behavior Problems. Specific areas of problem behaviors were reported in the following areas: Emotional Reactivity, Somatic Complaints, Withdrawal, Sleep Problems, and Attention Problems. All of these reported areas of emotional/behavior problems commonly occur in clinically impaired populations, including individuals with developmental disabilities. No baseline level of emotional/behavioral functioning within the school environment was obtained because Kate was not yet enrolled in school and the time of initial admission.
Results of all standardized assessments conducted on three separate occasions (i.e., before and during treatment) are reported in Table 1, Table 2, and Table 3. Upon initial examination, Kate demonstrated lower-than-expected cognitive abilities and adaptive functioning, and clinically significant impairments in emotional and behavioral functioning. Given Kate’s level of impairment across cognitive and adaptive functioning, intensive intervention to target these deficits was warranted.
Criterion-Referenced Assessment of Behavior and Language
Upon initial admission, Kate was administered the Assessment of Basic Language and Learning Skills–Revised (ABLLS-R; Partington & Sundberg, 1998), which is a multi-method, multi-component criterion based assessment used to track skills in individuals with developmental delays. The ABLLS-R measures skills across 25 domains, assessing prerequisite communication skills and readiness to benefit from individualized instruction. Nine of the 25 domains were used to measure Kate’s language development, and subsequently used to develop an individualized treatment plan and monitor progress. The ABLLS-R was implemented by a clinical specialist assigned to Kate’s treatment team, under the supervision of a licensed psychologist.
Kate’s performance on the ABLLS-R at the time of initial admission indicated skill deficits across the nine assessed domains. Kate’s early language skills such as requesting preferred items/activities, labeling items/objects, making spontaneous vocalizations, and providing responses to questions and statements made by others were largely impaired. Kate indicated preference for items/activities by looking at items and reaching toward items. Preferred items were identified initially based on semi-structured parent interviews and behavioral observations of Kate in the natural environment. During session, Kate was presented with small arrays of two to three preferred items and given the opportunity to select an item; informal preference assessments occurred every 15 to 20 min throughout the session. Kate spontaneously vocalized sounds, but few recognizable words were emitted. Kate demonstrated slightly stronger receptive language skills, such that she was able to respond to her name, follow simple instructions, and was able to identify familiar items when presented in an array. For example, the therapist presented an array of objects and said, “Show me the car.” Kate was able to select the car, and therefore able to discriminate the car from other objects in the array. When examining Kate’s skills in visual performance, she demonstrated significant impairments in this area. Her existing skills were quite minimal, and although she was able to successfully complete simple visual-performance tasks (e.g., single-piece inset puzzles and matching identical items), she did not demonstrate fluent matching skills (e.g., matching non-identical items). Kate was unable to sort objects by their feature, function, or class; lacked seriation skills; and was unable to complete complex puzzles (e.g., puzzles with multiple/non-identical pieces).
6 Case Conceptualization
There is minimal research investigating interventions to address the range of deficits due to the effect of prenatal alcohol exposure (Bertrand, 2009). Much of the FASD literature emphasizes the need for clear treatment recommendations based on empirical research, yet a dearth of research indicating support for specific treatments remains. While there are well-established behavioral and educational interventions for decreasing specific symptoms common in patients with developmental disabilities (e.g., cognitive impairments, behavior problems, hyperactivity, and impairments in adaptive functioning), the efficacy of these intervention strategies has not been assessed specifically in individuals with FASD.
While the practice of ABA therapy has often been described in conjunction with the treatment of ASD, the application of behavior analysis is ubiquitous. In fact, ABA has been applied to the treatment of individuals with broad developmental disorders (e.g., intellectual disability, attention deficit/hyperactivity disorder, Down syndrome), and also applied to the general population through weight loss interventions, smoking-cessation initiatives, and other areas with similarly positive treatment effects (Cooper et al., 2007). Unfortunately, access to ABA-based interventions for individuals with ASD is largely influenced by state health care legislation, insurance policies, and cost of care (Holland, 2009). Health coverage for ABA treatment for disability populations apart from those with ASD (e.g., intellectual disability, Down syndrome) is even more uncommon. The focus of intervention when applied to individuals with disabilities is often improvements in language and communication skills, social interaction skills, adaptive/daily skills (e.g., toileting, hygiene), and the reduction of problem behaviors. Beyond the need for service providers to promote the use of ABA-based treatments in children with ASD, it would be of additional clinical value to explore the utility of ABA-based therapy with other populations that have similar presenting deficits in terms of language and adaptive skills delays, learning impairments, and cognitive delays. Application of ABA-based intervention may be particularly useful in those populations (outside of the autism spectrum population) with limited research on appropriate interventions to remediate deficits. Among these categories of developmental disabilities in which ABA-based interventions may be beneficial is FASD.
When identifying efficacious treatments for clinical populations, large randomized control trials provide valuable information regarding treatment effects. However, there is specific utility in relying on non-experimental and quasi-experimental single-subjects designs employed in a clinical case study, especially given the scarcity of research on treatments for FASD. When examining treatment approaches for specific populations, single-case designs and case studies have served as preliminary evaluations for research projects with larger sample sizes (Green, Brennan, & Fein, 2002).
7 Course of Treatment and Assessment of Progress
Following a comprehensive evaluation, Kate was admitted to an intensive intervention day treatment program, where she received one-on-one ABA services for 15-hr per week. The program utilized behavioral assessment and treatment procedures based in principles of ABA, by specifically emphasizing Skinner’s Analysis of Verbal Behavior (Skinner, 1957).
Supervision and Staffing
During her admission in the day treatment program, Kate’s intervention was developed and monitored by a team of clinicians. The director of the clinic, a licensed psychologist and doctoral-level board certified behavior analyst (BCBA-D), served as the primary case supervisor and provided clinical oversight for all decisions made regarding Kate’s treatment and planning. An experienced, master’s-level BCBA functioned as the case manager, provided daily treatment monitoring, and reported directly to the psychologist. Treatments were directly implemented by bachelor’s-level therapists including an entry-level clinician, responsible for treatment implementation, and an experienced bachelor’s-level clinician (i.e., Clinical Specialist) who was responsible for treatment implementation and oversight, data entry, and providing progress updates to the case manager. Staff training procedures for direct service staff are described below. The clinical team met weekly to discuss Kate’s treatment and progress.
Staff Training
To ensure a high level of treatment integrity, staff providing direct services to clients in the day treatment program participated in a comprehensive training program prior to implementing any clinical procedures. Behavioral Skills Training (BST), a behaviorally based instructional model (Reid & Parsons, 1995), was used to train staff to proficiency in implementing treatment protocols. BST consists of providing verbal/written instructions, modeling, role-playing, and coaching and feedback. Trainees were required to pass written competency exams on the content of the didactic training with 80% accuracy. In the next phase of training, trainees received 2 days of in-vivo training through modeling and role-playing. During role-plays, trainers modeled appropriate teaching and intervention procedures. Trainees were then provided with opportunities for practice and feedback with the trainer. Skills assessed during role-plays included session preparation, correct presentation of targets, pace of instruction, probing and recording responses, prompt fading, and behavior management procedures. To progress to subsequent role-play sessions, trainees were required to implement procedures with 100% accuracy across three consecutive sessions. After successfully passing all role-play assessments, staff were then systematically faded into the therapy sessions. During the first day on the unit, trainee–client contact was limited to data collection, while an experienced clinician conducted the therapy session while also collecting data. Trainees were required to demonstrate 80% inter-observer agreement with the primary data collector. Once trainees met this criteria, they then spent time systematically fading into the therapy session—the first day conducting one third of the session with 80% treatment fidelity and were then provided with positive and corrective feedback from the case manager. On the second day, the staff member was required to implement the entire session with 80% treatment fidelity before moving on, and the final day conducting the entire session with 80% accuracy under the observation of a case manager. Staff training continued throughout the entirety of Kate’s admission, such that remediation was provided when necessary and changes in treatment protocols were accompanied by specific protocol training for all treatment team members.
Overview of Treatment and Behavior Change Procedures
Kate received 15-hr of intensive one-on-one ABA therapy each week for 23 months. At the beginning of her admission, Kate participated in a thorough intake assessment and behavioral skills assessment. Performance during the baseline language and behavior assessments were used to inform the clinical team of Kate’s areas of strengths and weakness, and to identify intervention targets based on her level of skills deficit. Initially, formal treatment procedures took place in a highly structured clinical environment with a 1:1 therapist–child ratio (though at times additional clinical personnel observed, assisted with data collection, or provided the therapist with supervision). Kate had an area within a therapy room designated as her workspace for sessions in clinic that included a small table with preferred items and activities available and use of partitions when a less distracting teaching environment was needed. However, intervention also occurred outside of the therapy room, with teaching trials taking place in areas of the clinic that are more similar to the natural environment (e.g., playroom, playground). As Kate began to demonstrate mastery of targeted skills, these skills were practiced in other environments to ensure that generalization of these skills occurred outside of the highly controlled environment of the therapy room.
Target skills were identified based on deficits indicated in behavioral and functional assessments. The development of a functional communication system was of primary importance in Kate’s admission based on the referral concern and the nature of clinical services provided at the program in which she was admitted. However, many functional and daily-living skills were also targeted (e.g., toilet training and compliance) to enhance Kate’s level of independent functioning. As in most intervention programs targeting deficits in verbal behavior, requesting skills were among the first language skills targeted for Kate. It was of primary importance that Kate develop skills in requesting preferred items and activities to establish Kate’s motivation to participate in other instructional activities.
Another skill that was targeted upon initial admission was Kate’s motor imitation skills. Motor imitation skills are often included in the instructional programming for patients with minimal functional skills because the target responses can often be easily prompted and acquired. When teaching motor imitation, the therapist may say, “Kate, do this . . . ” while the therapist knocks on the table. If Kate was not able to independently emit the response of knocking, the therapist could use hand-over-hand physical prompting by taking Kate’s hand and knocking it on the table. As soon as Kate emitted the response, albeit prompted by the therapist, she was provided with access to reinforcement (i.e., the therapist immediately handing Kate a preferred item) so she begins to pair the response (knocking when the therapist says “Do this” while knocking) with reinforcement. As Kate began to demonstrate mastery of motor imitation skills, the therapist was able to fade to less intrusive prompts until Kate was able to independently provide the correct response. The development of skills such as motor imitation could then be used to develop a general imitative repertoire (being able to mimic any action demonstrated by another person) to be transferred to other imitation skills (such as imitating others’ language).
Once requesting and imitation skills were established within Kate’s behavioral repertoire, therapists were able to begin to target more complex skills such as vocal imitation (e.g., The therapist states, “Say what I say . . . ” and Kate repeats what is said by the therapist), expressive labeling (e.g., Kate correctly labels an item when therapist asks, “What is it?” while showing a picture/object), receptive identification (e.g., Therapist presents an array of three objects and tells Kate to “point to the car.” Kate points to the car), visual performance (e.g., match-to-sample tasks in which the therapist tells Kate to “match it”; sequencing, puzzles, etc.), and more sophisticated language skills (e.g., requiring Kate to request preferred items by saying, “I want cookie” instead of “Cookie,”). These skills were targeted using similar procedures to those described above for teaching motor imitation skills. When teaching new skills, the therapist presented a demand (e.g., “Match it”) and the correct responses were prompted by the therapist (e.g., providing hand-over-hand prompting to match the objects). As Kate demonstrated increasing independence in correctly responding, the therapist was able to fade to a less intrusive prompt (e.g., gesturing, rather than doing hand-over-hand physical prompting).
Daily Progress Data
Data on skills targeted as part of Kate’s VB program were collected during every treatment session. Most often, data were collected at the start of Kate’s session, through a data collection procedure known as a “cold probe” (Lerman, Dittlinger, Fentress, & Lanagan, 2011). The cold probe was conducted at the beginning of the session, before any formal opportunities for teaching and practice were conducted within the session. The purpose of measuring Kate’s performance through a cold probe assessment was to determine whether she had truly acquired and maintained the skill, and to ensure that successful responding was not the result of repeated practice immediately prior to data collection. Specifically, at the start of Kate’s therapy sessions, the treatment team probed the target skills and recorded whether Kate provided a correct or incorrect response. If she responded correctly, this may have suggested that Kate had begun to maintain skills that were taught in the previous therapy sessions. For most targets, criteria for mastery were set at three accurate responses; that is, for three consecutive days, Kate had to provide the correct response to the cold probe. At the conclusion of daily data collection, the treatment team spent time teaching Kate and practicing any skills missed during the cold probe using teaching procedures such as most-to-least prompting (Libby, Weiss, Bancroft, & Ahearn, 2008) and interspersing of mastered tasks (Koegel, Koegel, & Carter, 1998). Members of the treatment team served as the primary data collectors. Data were frequently reviewed by the case manager, with the oversight of the licensed psychologist assigned to the case. If data indicated that Kate was not making progress toward mastery, as expected, instructional procedures were adjusted to ensure that Kate was participating in the most efficient interventions and to promote generalization of these skills to other settings. The duration of each targeted skill area appears in Figure 1.
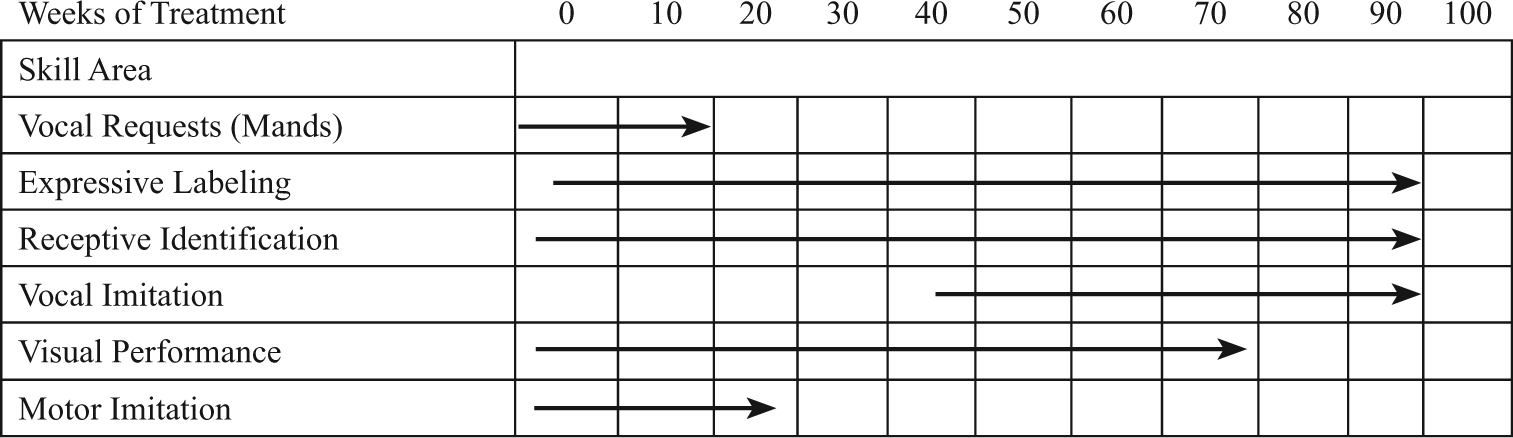
Skill areas targeted during day treatment admission.
Treatment Progress
When placed in a structured teaching environment in which Kate’s verbal behavior was intensely targeted, Kate nearly immediately began acquiring new language and related skills at a rapid rate. Given the complexity of a comprehensive treatment program, such as the one that Kate participated in, it is not uncommon for priorities of the treatment to shift over time. As a result, plateaus in treatment progress may be observed across skill areas at particular times throughout the admission (Figure 2). Oftentimes, the clinician may prioritize a particular skill that will have a positive effect on the child’s overall level of adaptive functioning. For example, teaching a child to request may be heavily targeted at the beginning of the admission, given the functional utility of this skill (i.e., the child is able to request preferred items and activities), while programming of other skill areas (e.g., expressive labeling, visual-perceptual skills) may receive less attention until the child has a sufficient repertoire for requests. Then, the clinician may integrate the child’s vocal requesting skills into the teaching of other skills (e.g., expressive labeling, visual-perceptual skills) as preferred items can be requested by the child, and potentially serve as reinforcement for teaching new skills. As Kate developed more verbal skills, treatment priorities shifted toward vocal/verbal skills based on parent priorities and treatment planning, with less emphasis placed on visual-perceptual or motor imitation tasks.
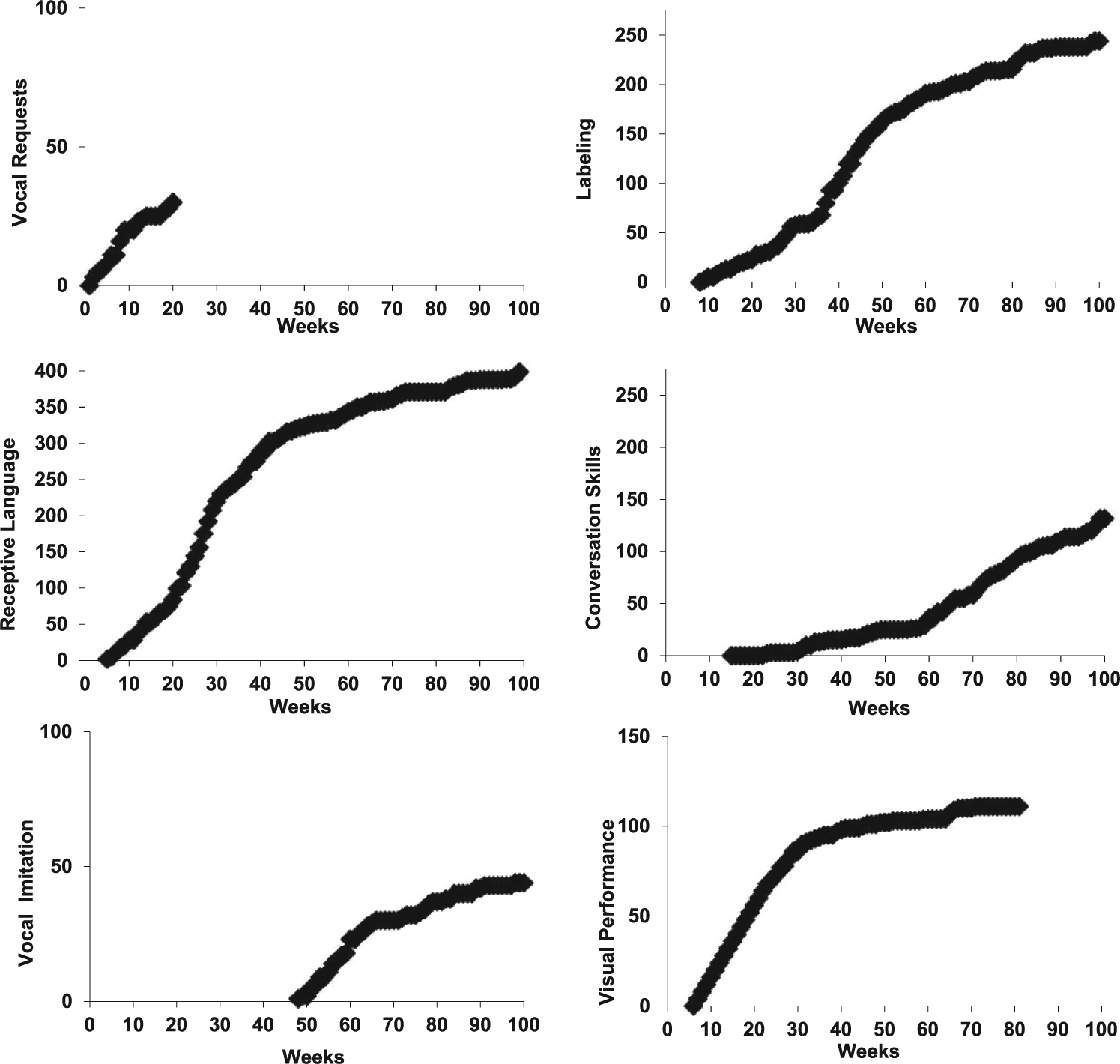
Cumulative progress of verbal behavior.
A summary of Kate’s progress is illustrated in Figure 2, which reflects Kate’s progress in response to treatment. Data in Figure 2 are presented as a cumulative graph, a type of visual representation common in single-case research conducted by behavior analysts (Kazdin, 2011). Using cumulative record graphs, the level of performance of the participant over time is graphed in an additive fashion. In the current study, the impact of the intervention is displayed through the cumulative number of skills (e.g., vocal requests, labels, etc.) that Kate acquired throughout her treatment admission.
Vocal requests
Kate’s ability to vocally request preferred items and activities was identified as an area of primary importance for establishing motivation to respond to teaching trials. Kate demonstrated an immediate response to treatment and began requesting preferred items and activities within the first few weeks of treatments. Target requests were considered mastered when Kate demonstrated that she was able to independently request preferred items and activities during cold probe assessments on three consecutive days. After 7½ months of treatment, the treatment team discontinued intervention targeting single-word vocal requests because Kate was able to sufficiently request preferred items.
Expressive labels
Once Kate demonstrated that she was able to vocally request preferred items, her skill in expressive labeling was targeted. Initially, Kate was taught to label pictures and three-dimensional (3D) objects (e.g., Kate names the object when the therapist presents the object and says, “What is it?”). As she demonstrated mastery of this skill, more complex targets were added, such that Kate was taught to label familiar people by name, label 2D actions (e.g., Kate responding to the therapist asking, “What’s he doing?” while showing Kate a picture of someone sleeping), correctly labeling letters and numbers, labeling parts of a whole (e.g., Kate correctly names the correct body part when the therapist points to a body part and says, “What part is this?”), labeling emotions, accurately answering yes/no questions, and increasing the mean length of utterance to multiple words. Kate demonstrated progress in developing this skill throughout treatment.
Receptive language
Kate’s ability to accurately respond to verbal instructions was targeted within the first few weeks of her admission. Initial receptive targets included the identification of a 3D object or 2D picture after being given verbal instructions (e.g., Kate selected the correct item in the array when the therapist said, “Point to the dog.”). As Kate demonstrated mastery in responding to verbal instructions to identify objects or pictures, she was then taught to identify parts of objects (e.g., Therapist said, “Show me the wheel.” Kate pointed to the wheel), body parts, people, actions of others (e.g. Therapist said, “Point to the girl jumping.” Kate pointed to the picture of the girl jumping), as well as single-step commands (e.g., Therapist said, “Show me stomping.” Kate responded by stomping her feet). Kate’s repertoire of receptive responding gradually expanded such that she was able to identify objects when given a description of their feature, function, or class (e.g., Therapist said, “Show me the one you wear.” Kate selected the coat in an array of non-clothing items), with the aim of increasing her skill in responding to multi-component directives.
Imitation
At the time of her initial admission, Kate did not yet demonstrate the ability to imitate the behavior of others. Therefore, Kate was taught to imitate the actions of others following a model and verbal directive (“Do this . . . ”). Behaviors that could be easily prompted by the therapist were first targeted, including gross motor imitation (e.g., therapist modeling clapping while giving instruction, “Do this.”). As Kate demonstrated mastery of imitation, she was instructed to imitate more complex actions, such as fine motor imitation (e.g., imitating a “thumbs up” sign), the imitation of actions using objects (e.g., stacking blocks or drawing shapes following a model), and pattern sequencing.
At the time of initial admission, Kate emitted some sounds and words, but these responses were largely non-functional, and she was unable to vocally respond to the tasks in which she was asked to “Say what I say . . . ” As Kate started demonstrating increases in her expressive language skills through her ability to request and label objects (and these responses were paired with reinforcement), she also began to echo the vocalizations of others. As Kate demonstrated increased skill in echoing the sounds and words of others, the treatment team was able to teach increasingly complex vocalizations (e.g., more complex phoneme blends, words with multiple syllables). For these more complex words, accurate articulation became a focus of Kate’s intervention.
Visual performance
Kate’s skill in visual performance was also an area targeted within the first few weeks of admission. Visual-performance tasks initially included tasks such as inset puzzles and progressed to skills in identical matching of 2D pictures and 3D objects. Kate initially responded to treatment targeting visual-perceptual skills and data indicated a stable, ascending trend. However, after approximately 7½ months, skill acquisition in the area of visual performance did not occur as rapidly, and her performance eventually began to plateau after approximately 15 months of treatment. Intervention targeting this skill was discontinued and replaced with other functional target areas. Kate’s visual-perceptual performance, as measured through behavioral data during treatment, was consistent with her assessed cognitive profile, which indicated a personal weakness in visual-spatial processing. Clinical interpretations of these findings, with specific consideration of patients with FASD, are discussed below.
8 Complicating Factors
One skill area that may warrant specific consideration in children with FASD is that of visual performance. During the course of treatment, Kate initially demonstrated significant gains in visual performance and rapidly acquired new skills. However, near the end of Kate’s first year in treatment, her progress in visual performance plateaued and her rate of acquisition in this area was not as rapid as initially observed at the outset of treatment. Weakness in visual-spatial performance was also reflected during longitudinal assessments of cognitive functioning, indicated by a substantial decline in this cognitive domain. Children with FASD often exhibit deficits in the area of visual-spatial processing and visual-motor integration (Kodituwakku, 2009). It is possible the limited changes may reflect the specific cognitive deficits associated with prenatal alcohol exposure as well as changes with intensity and focus of interventions. Future research may aim to identify ABA-based interventions to specifically target deficits in visual-spatial processing, specifically those experienced by individuals with FASD. Alternatively, clinicians may consider the need for additional environmental modifications (e.g., emphasizing verbal instruction over visual instruction) when working with children with FASD.
9 Access and Barriers to Care
Although Kate was able to participate in treatment over the course of 23 months, the clinic was not considered to be a permanent learning environment for Kate. One prominent barrier of the use of the structured teaching procedures described in this report is the difficulty that some clients face when transitioning from the clinic setting to a more natural setting, such as their public schools. Although children with disabilities affecting academic performance are provided with special education support through individualized education plans, a traditional school setting may not be able to provide the same intensity of intervention as those provided in a 1:1 clinical setting. Therefore, Kate may not have been able to maintain all of the skills acquired during her treatment admission when she discharged from treatment.
10 Follow-Up
Intellectual Functioning
Following 9 months of treatment, Kate underwent a follow-up psychoeducational evaluation to assess any changes in cognitive functioning as measured by a standardized, norm-referenced assessment of functioning that could be attributed to her participation in an intensive ABA intervention. Change scores are presented in Table 1. Although Kate’s overall cognitive functioning remained stable, clinically significant increases in her verbal abilities (approximately two standard deviations) were observed after only 9 months of treatment. The most prominent area of improvement in Kate’s verbal abilities occurred in the area of naming vocabulary, which is consistent with the behavioral data that tracked Kate’s daily acquisition of labeling skills. Kate also demonstrated a slight improvement in her level of verbal comprehension, though these changes were minor. Kate’s overall level of verbal abilities remained in the below average range at the time of the follow-up assessment, but marked improvements were observed. No clinically significant changes occurred in Kate’s non-verbal or spatial abilities; though these skills were not targeted at the same level of intensity as interventions used to target Kate’s verbal ability based on the nature of the treatment program.
Kate’s intellectual functioning was, again, assessed after 23 months of treatment (Table 1). The assessment was administered 1 month before Kate was discharged from treatment. Changes that were observed in Kate’s verbal abilities at 9 months of treatment remained stable during the final assessment, suggesting that she continued to acquire verbal skills at a similar rate as demonstrated in her first 9 months of treatment. Her non-verbal reasoning skills remained stable across all three assessment points. There was a decline in Kate’s visual-spatial and spatial-motoric abilities, which can be partially explained by her deficits in visualization and spatial skills, characteristic of children with FASD, as well as low global cognitive functioning.
Adaptive Functioning
Throughout her treatment admission, Kate demonstrated substantial gains across all areas of adaptive functioning, based on caregiver report on the Vineland-2 (Table 2). Although Kate initially was reported to have significant impairments across nearly all adaptive domains at the time of baseline, after 9 months of treatment her caregiver reported improvements in all areas of adaptive functioning. Areas of greatest change occurred in the areas of Communication (borderline range) and Socialization (average range), which were areas of primary importance in the development and implementation of Kate’s treatment. Upon discharge, all improvements in adaptive functioning were maintained, with the exception of Socialization, which was in the borderline range. Kate’s reported levels of adaptive functioning across all domains were consistent with her intellectual functioning, with some areas exceeding her reported cognitive abilities (e.g., Daily-Living Skills).
Emotional/Behavioral Functioning
Kate’s level of emotional/behavioral functioning was again assessed after 9 months of treatment through both caregiver and teacher report. Clinically significant improvements in all assessed areas of emotional/behavioral functioning were reported by Kate’s caregiver after 9 months of treatment. No elevated levels of emotional/behavioral problems were reported by Kate’s caregiver, and all scores fell within the average range (Table 3). Teacher ratings of emotional/behavioral functioning were also obtained after 9 months of treatment (Table 3), and no significant problem areas were reported to occur within the school environment.
On discharge (i.e., 23 months of treatment), reports of emotional/behavioral functioning were largely consistent across caregiver and teacher reports. At the time of treatment discharge, Kate no longer met the age requirements of the CBCL-Preschool assessment and her parent and teacher, instead, completed the CBCL-School Age form. All composite scores for the School Age form are consistent with those on the Preschool form (i.e., Total Problems, Internalizing, and Externalizing), with some minor differences in subscale scores, including the addition of a Rule-Breaking Behavior scale and omission of the Emotional Reactivity scale. Internalizing and Externalizing behaviors were reported to fall within the average range. However, both caregiver and teacher reports indicated elevated levels of Thought Problems and Attention Problems. These findings were not surprising, given that children with lower-than-average cognitive functioning often exhibit problems with attention. Kate’s teacher also reported an increase in Kate’s Rule-Breaking behavior. It is not clear if the increases in problem behaviors reflected changes in classroom demands as Kate progressed in grade levels, differences in teachers’ expectations, or developmental changes.
11 Treatment Implications of the Case
ABA-based interventions targeting deficits in verbal behavior have been reported by behavioral practitioners as one of the primary methods of treating language delays in children with ASD (Carr & Firth, 2005). However, this treatment approach has not yet been implemented with individuals with FASD. Providers responsible for the diagnosis and treatment of patients with FASD are often limited by the lack of published research on successful treatment approaches, which subsequently limits optimal treatment recommendations. The current case study presents promising findings of the effects of the VB approach when applied to a child diagnosed with FASD. Through participation in an intensive VB treatment program across a period of 23 months, Kate demonstrated significant gains in functioning across several skill areas. This progress was not only evidenced through behavioral skill data collected throughout the duration of her treatment, but also documented through standardized, norm-referenced assessments that were administered by independent evaluators who were not involved in Kate’s treatment. At the time of discharge, Kate was equipped with many functional skills that would be advantageous as she transitioned to a full-time public school placement. Although caregiver training and school consultation was provided throughout Kate’s admission, it is recommended that, in future cases, follow-up consultation services be emphasized postadmission, to ensure that the participant is able to maintain and generalize the skill in settings outside of the clinic.
The development of verbal skills was among the most prominent areas of growth for Kate. While Kate’s expressive language skills remained below average compared with typically developing peers at the time of her discharge, the benefits of the language skills she gained during her admission should not be understated. Upon initial admission, Kate possessed minimal verbal language skills and was unable to request preferred items and activities. Teaching Kate to vocally request preferred items was a skill targeted early in treatment, which is consistent with recommendations from existing literature on VB programming. While other types of verbal language (e.g., labeling items, responding to questions) are also important during early stages of VB programming, teaching a child to request provides him/her with some control over the environment (Sundberg & Michael, 2001). The ability to make requests allows the child to control access to their wants and needs and also allows the child to understand the roles of speakers and listeners, which is useful in teaching other expressive and receptive language skills. Within the first few weeks of treatment, Kate was able to vocally request preferred items. Providing children with a functional method of communicating wants and needs often serves as a bridge to teaching additional skills. In addition, problem behaviors that had been previously emitted as a means of accessing preferred items had now been replaced with more functional communication, thereby resulting in a decrease in problem behavior.
12 Recommendations to Clinicians and Students
Although the current report includes the case study of an individual participant, the findings generally support a valid inference that the observed outcomes can be attributed to the treatment. Data were continuously collected during treatment, and multiple measures were administered by multiple independent evaluators who played no role in Kate’s treatment. Almost immediately after beginning treatment, Kate displayed rapid gains when structured ABA interventions were in place. Given the lack of empirically supported treatments for FASD, the positive outcomes demonstrated in the current study suggest a need to apply similar intervention approaches to a broader sample of individuals with FASD.
The current study provides one example of how behavior analytic interventions were successfully applied to a child with pFAS. It further suggests a need for clinicians and researchers to explore the clinical utility of ABA interventions to other disability populations (e.g., Down syndrome, ADHD) who have not traditionally had access to these services. Although ABA has historically been widely utilized to treat the core symptoms of ASD, it may be appropriate for clinicians and researchers to design tailored interventions to effectively treat characteristics of learners (e.g., the visual-spatial deficit characteristic of individuals with FASD).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.