
Abstract
This clinical case describes the assessment and treatment of Roger, a 31-year-old veteran who served in Operation Iraqi Freedom. In addition to combat-related post-traumatic stress disorder (PTSD), Roger presented with a conversion disorder (globus pharyngeus) and avoidance of consuming solid food without also consuming alcohol. A multicomponent treatment program for PTSD, trauma management therapy (TMT), was provided 5 times per week over a 3-week period. TMT included daily-exposure therapy (EXP) as well as daily social and emotion regulation (SER) group therapy to target anger, social withdrawal, and depression. In addition to TMT, exposure to food consumption in the absence of alcohol was provided in the final week. PTSD symptoms were assessed via semi-structured interview and self-report measures, while food intake was assessed via behavioral observation. PTSD symptoms as measured by the Clinician-Administered PTSD Scale (CAPS) decreased from 63 at pre-treatment to 17 at post-treatment, indicating that Roger no longer met criteria for PTSD. Exposure to food intake was equally successful with Roger consuming full meals (e.g., hamburger and french fries) without consuming alcohol. This case study exemplifies the successful use of intensive exposure therapy to target comorbid anxiety-based disorders in a short period.
1 Theoretical and Research Basis for Treatment
As far back as the 1960s, Wolpe discussed the development of psychiatric symptoms in response to a negative stimulus and provided one of the first accounts of successful treatment of phobias by direct exposure (Wolpe, 1968). Post-traumatic stress disorder (PTSD) is conceptualized as a disorder stemming from exposure to a traumatic event(s) wherein individuals reexperience the event in the form of intrusive thoughts, nightmares, or, in severe cases, flashbacks. In addition, individuals with PTSD have heightened arousal, hypervigilance, and behavioral avoidance. By preventing memories of the traumatic event from surfacing, avoidant behavior can also prevent the occurrence of negative and fearful thoughts and feelings associated with the traumatic memory thus protecting the individual from perceived danger and further harm. However, by avoiding those same thoughts and feelings, new and more appropriate response patterns cannot be learned (Foa, Huppert, & Cahill, 2006; Foa & Kozak, 1986). Ehlers and Clark (2000) describe avoidance as a maladaptive control strategy that short circuits disconfirmation of negative appraisals, which result in the maintenance of perceived current threat. This type of behavior has been documented in various populations with PTSD, including victims of sexual assault (Fleurkens, Rinck, & van Minnen, 2014), motor vehicle accident victims (Delahanty et al., 1997), and combat veterans (Pietrzak, Harpaz-Rotem, & Southwick, 2011).
PTSD is somewhat common, with lifetime prevalence among adult Americans estimated to be 6.8% and past year prevalence estimated at 3.5% (Kessler, Berglund, et al., 2005). There is a sex difference, with lifetime prevalence among men estimated at 3.6% and among women at 9.7% (Kessler, Chiu, Demler, & Walters, 2005). With regard to veterans, lifetime prevalence is estimated at 8%, with 4.8% currently suffering from the disorder (Wisco et al., 2014). This rate holds steady for those deployed to Somalia (Litz, Orsillo, Friedman, Ehlich, & Batres, 1997) as well as Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF; Smith et al., 2008). However, veterans with combat exposure have a 12.1% probability of developing PTSD, with the chance increasing from 25.3% to 34.9% with moderate and heavy combat exposure, respectively (Wisco et al., 2014). Those who suffer from PTSD also often suffer from comorbid conditions, including substance abuse, depression, and other anxiety disorders (Galatzer-Levy, Nickerson, Litz, & Marmar, 2013). In addition to its high prevalence, PTSD is associated with substantial costs to society. PTSD associated with OEF and OIF veterans alone was estimated by Kilmer, Eibner, Ringel, and Pacula (2011) to account for $923 million dollars over 2 years in societal costs.
Conversion disorders may also develop in response to an anxiety-provoking event, stressor, or trauma (American Psychiatric Association [APA], 2013) and like PTSD, may involve avoidant behaviors. Conversion disorder, also called functional neurological symptom disorder, is perhaps most simply described as a condition in which psychological stress manifests as a physical symptom(s). To provide an example, consider a man repairing his roof who stumbles and falls to the ground. He escapes the fall with minor cuts and bruises, but his leg remains paralyzed despite no neurological damage and/or broken bones. The loss of function in the leg, unexplained by medical or physical examination, would be classified as a conversion disorder. Globus pharyngeus (GP), a type of conversion disorder, is a persistent or intermittent non-painful sensation of a lump or foreign body in the throat that is not accounted for by a physiological abnormality. GP is thought to be long lasting, difficult to treat, with a tendency to recur.
Conversion disorders as a whole are relatively rare, with a reported prevalence rate of 11 cases per 50,000 people in clinical settings (Guggenheim & Smith, 2000). The exact prevalence for conversion disorder is unknown, but appears in 5% of neurology clinic referrals (APA, 2013). Onset of conversion disorders may be associated with stress or trauma that may be either psychological or physical in nature (APA, 2013). There is little information regarding the occurrence of conversion disorders that may be rooted in comorbid anxiety. GP is one such disorder.
Differential Diagnosis
Time elapsed since the traumatic event is one diagnostic criterion used in the differential diagnosis of PTSD. Acute stress disorder is appropriate if the trauma occurred within 1 month of presentation, whereas PTSD requires symptom duration of at least 1 month. Anxiety disorders, such as obsessive-compulsive disorder, may involve intrusive thoughts but other PTSD symptoms are not evident (e.g., emotional numbing). Episodes of depression may occur following a traumatic event but, again, intrusion and arousal/avoidance symptoms are lacking. With depression, previously enjoyed activities might be avoided but usually due to fatigue and loss of interest rather than anxiety. Dissociative disorders and conversion disorders may also be preceded by a traumatic event but also lack PTSD co-occurring symptoms. Dissociative symptoms may be present in PTSD, and should be specified, if other PTSD symptoms are met. With regard to conversion disorders, new onset somatic symptoms, with no biological basis, that occur within the context of post-traumatic distress should be considered as PTSD if other symptoms of PTSD are present. For example, many individuals with PTSD (especially combat veterans) express difficulties with pain that may be undiagnosed. Lastly, traumatic brain injury (TBI) should be considered as a differential diagnosis if head trauma occurred in the context of the traumatic event. There is considerable overlap in neurocognitive symptoms (e.g., concentration difficulties, memory problems, irritability) but in most cases of TBI (without PTSD), the intrusion and avoidance symptoms are absent.
Differential diagnosis of conversion disorders may be complex and should begin with a thorough assessment to rule out neurological disease or physiological abnormalities. The Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) requires clear evidence of incompatibility between a patient’s reported symptoms and potential neurological disease; however, diagnosis of conversion disorders must be based upon the entire clinical presentation as opposed to a single clinical result. Conversion disorder may be diagnosed in addition to somatic symptom disorder but compared with somatic symptom disorder; conversion disorder requires incompatibility between somatic symptoms and pathophysiology. In addition, the excessive thoughts, feelings, and behaviors characterizing somatic symptom disorder are often absent in conversion disorder. Differential diagnosis must include factitious disorder and malingering; however, diagnosis of conversion disorder does not require judgment that the symptoms are not intentionally produced. If feigning of symptoms can be determined, conversion disorder should not be diagnosed. Dissociative symptoms are common in individuals with conversion disorder and, in some cases, both diagnoses are appropriate. Other disorders to consider in differential diagnosis may include body dysmorphic disorder (specific body part is focus but no loss of sensory or motor functioning in that body part), depressive disorders (where heaviness of limbs may be present), and panic disorder in which neurological symptoms may occur but are transient.
With regard to differential diagnosis of GP specifically, there has been confusion regarding labeling the condition. GP has been described in the literature by many terms, including “globus hystericus” (Finkenbine & Miele, 2004; Ravich, Wilson, Jones, & Donner, 1989; Stacher, 1983, 1986) or “phagophobia” (Çiyiltepe & Turkbay, 2006; Suraweera, Hanwella, & de Silva, 2014). GP is characterized by the sensation of a mass in the throat, difficulty swallowing, choking sensations, suffocation, and dyspnea (difficult or labored respiration). Often, patients complain of difficulties initiating swallowing and may avoid eating solid foods, or may require liquefying solid foods prior to consumption. In addition, those with GP are often preoccupied with throat sensations throughout the day, even in the absence of food.
As previously stated, GP diagnosis requires that physical dysfunction or abnormalities be ruled out. To illustrate the need for exhaustive assessment, Ravich et al. (1989) reexamined 23 patients with diagnoses of either psychogenic dysphagia or globus hystericus. As a result of this reevaluation, 65% (n = 15) were found to have an underlying physical condition, including pharyngeal dysfunction, structural obstruction, or esophageal dysmobility. Given the high rate of misdiagnosis, multidisciplinary approaches to diagnosis are recommended and a comprehensive review of medical history should be obtained. Physical examinations may include techniques such as barium swallow, esophagoscopy, manometry, and endoscopy.
Treatment of PTSD and GP
Several case studies have shown feasibility of behavioral treatment of PTSD and comorbid disorders. Chaison, Dunn, and Teng (2010) reported treatment of panic disorder with agoraphobia in a case in which combat PTSD was present. Although PTSD symptoms were still present at follow-up, treatment of panic disorder was successful. PTSD treatment was also combined with treatment of disordered eating following military sexual trauma (Mott, Menefee, & Leopoulos, 2012). An increasing body of research has demonstrated the effectiveness of exposure-based cognitive-behavioral therapy for PTSD (Powers, Halpern, Ferenschak, Gillihan, & Foa, 2010) and specifically for combat-related PTSD (Beidel, Frueh, Uhde, Wong, & Mentrikoski, 2011; Frueh, Turner, Beidel, Mirabella, & Jones, 1996; Yuen et al., 2015). Exposure therapy is analogous in humans to fear extinction models used in animals (Myers & Davis, 2007) and is based upon the principles of classical conditioning discovered by Pavlov and Thompson (1902) and later explored by Watson and Rayner (1920).
An example of classical conditioning in PTSD might include avoidance of crowded places after coming into close combat with the enemy in crowded urban environments, such as marketplaces frequently seen in Iraq. Exposure therapy seeks to extinguish learned behaviors that are or have become maladaptive by exposing patients to the anxiety or fear-producing stimulus (or a facsimile of that stimulus) without exposing them to the danger, thus allowing new information and expectations to be learned. Similarly, exposure therapy has been shown to be effective for several other disorders, including panic disorder (Opriş et al., 2012), social anxiety (Anderson et al., 2013), and specific phobias (Hamm, 2014). If exposure therapy seeks to extinguish learned behaviors, its application to GP is theoretically sound; particularly if an anxious preoccupation with the symptomology of GP has developed.
2 Case Introduction
To protect client confidentiality, we have changed identifying details and discuss the patient under a pseudonym. The current clinical case describes the assessment and treatment of “Roger,” a 31-year-old, married, Caucasian male. Roger served as an active duty service member of the U.S. Army for 6 years before transferring to the National Guard where he was on reserve status at the time of treatment. Among his multiple deployments, he served as a broadcast journalist in OIF. He developed PTSD after experiencing several combat-related traumatic events 11 years prior to treatment. In addition to PTSD, Roger has suffered from GP (feeling of a lump in the throat) that developed 2 years prior to treatment and was preceded by a choking incident. At the time of initial assessment, Roger was liquefying his meals or sustaining on soup and nutritional beverages (e.g., Ensure). Roger was able to consume some solid food, but only when he had ingested enough alcohol to be intoxicated prior to eating.
3 Presenting Complaints
Roger presented for a 3-week comprehensive treatment program for combat-related PTSD. He reported PTSD symptoms that began approximately 9 months after deploying to Iraq. He endorsed reexperiencing symptoms, avoidance, and hyperarousal symptoms that have led to dysfunction in his marriage and employment. Although prescribed medication, Roger indicated that he consumed an “excessive” amount of alcohol to help alleviate distress associated with PTSD symptoms. In addition to PTSD symptoms, Roger reported an inability to eat solid food without consuming alcohol. He explained that his solid food avoidance was due to a lump in his throat that caused him considerable discomfort and a related fear of choking. He typically consumed liquids and soft foods (protein shakes, soups) during the day and solid foods in the evening (burger, pizza), but only after consuming four or five alcoholic beverages. Roger described his inability to swallow solid foods without alcohol as very disruptive in his social life (marriage) and employment (waiter). At the time of the assessment, Roger reported that his wife was expending considerable effort in preparing his meals and that he often avoided social encounters due to symptoms of PTSD and a desire to hide his solid food avoidance. Roger met criteria for conversion disorder, specific phobia (flying), alcohol abuse, and PTSD at presentation.
4 History
Roger deployed as part of the U.S. Army from 2001 to 2007. During this time, he experienced multiple traumatic events including direct mortar fire, evasive maneuvering while riding on a transport plane, and responding to the scene of an overturned Humvee. Soon after his deployment Roger experienced intrusive vivid memories related to the victims of this accident that were accompanied by persistent avoidance of thoughts, people, and places related to the event. He reported that he also experienced significant emotional numbing as well as hypervigilance. Roger reported that these symptoms strained his marital and personal relationships and significantly affected his occupational functioning. He reported consistent attempts to minimize and hide his anxiety from his co-workers and fellow soldiers, a task that became increasingly difficult and resulted in excessive alcohol consumption with the goal of masking and reducing anxious symptoms.
Roger’s food aversion began with a choking incident that occurred approximately 2 years before he presented for treatment. He described that while alone in a hotel room, eating and watching television, a chicken bone became lodged in his throat. After several minutes attempting to dislodge the bone, he was ultimately successful. The next morning Roger experienced throat discomfort and presented to a local emergency room where he underwent esophageal dilation and several other medical tests. Roger reported that the doctors found no blockage or medical cause for the continued discomfort in his throat.
Over the next few months, Roger reported a constant feeling as if there was a “lump in his throat” and being unable to eat more than a few bites of solid food. Over the following months, Roger underwent several medical tests including a biopsy, laryngoscopy, bronchoscopy, as well as additional esophageal dilations. Although being medically cleared of any underlying problems (e.g., acid reflux, laryngitis, cancer), he continued to have a preoccupation with throat sensations and an aversion to solid foods.
Roger described his family as sympathetic and supportive and reported that his wife prepared several types of soup for him to eat. Despite these efforts, he began to feel the effects of significant nutrient loss. Over approximately 12 months, he lost 35 pounds and experienced dizziness and light-headedness. Roger compensated for these symptoms by taking liquid vitamins and eating certain solid food only while intoxicated. At the time Roger presented for treatment, he was liquefying approximately 80% of his food intake and sustaining on yogurt, pudding, smoothies, and soups.
5 Assessment
Roger signed an informed consent document prior to initiating treatment. He completed a comprehensive assessment battery consisting of clinician-administered semi-structured interviews and self-report measures. The Clinician-Administered PTSD Scale (CAPS) for Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994; Blake et al., 1995) was used to diagnose PTSD. The CAPS interview contains 17-items and is designed to assess both the frequency and intensity of PTSD symptoms. For the purposes of the CAPS, Roger identified three combat-related traumatic events that fulfilled Criterion A1 for a diagnosis of PTSD (Diagnostic and Statistical Manual of Mental Disorders [4th ed., text rev.; DSM-IV-TR; APA, 2000]). According to Roger, the worst event throughout his deployments occurred when he was the first person on the scene of a Humvee accident which killed a soldier and horrifically injured survivors sometime in 2005. He experienced intense fear for the lives of his soldiers and feelings of helplessness and horror during this event (Criterion A2 for PTSD). Roger obtained a total score of 63 on the CAPS, which is indicative of moderate-severe symptomology. Specifically, he endorsed four out of five reexperiencing symptoms: intrusive distressing memories of the events, distressing dreams, psychological distress at exposure to cues related to the events, and physiological reactivity on exposure to cues. With regard to avoidance and numbing symptoms, Roger endorsed all seven symptoms as significant: avoidance of thoughts or feelings; avoidance of activities, places, or people that remind him of the events; reduced interest in previously enjoyed activities; feelings of detachment or estrangement; experiencing a restricted range of affect; an inability to recall certain aspects of the traumatic events; and a sense of a foreshortened future. Furthermore, Roger endorsed all five hyperarousal symptoms: difficulty falling asleep, irritability or outbursts of anger, difficulty concentrating, hypervigilance, and an exaggerated startle response. These symptoms persisted for more than 6 months and appeared to be directly related to the combat-related traumatic events.
The Structured Clinical Interview for the DSM-IV (SCID-I; First, Spitzer, Gibbon, & Williams, 1997) was administered to assess for co-occurring disorders. In addition to PTSD, Roger met criteria for conversion disorder (globus hystericus or “lump in throat”), specific phobia (situational type, fear of flying), and alcohol abuse. He also met criteria for major depressive disorder, recurrent, lifetime diagnosis (not current).
PTSD Checklist–Military Version (PCL-M; Weathers, Litz, Herman, Huska, & Keane, 1993) is a 17-item self-report measure of the DSM-IV PTSD symptoms. The military-specific version of the PCL was used as a secondary measure of PTSD symptom severity administered to track treatment progress at baseline, Session 6, and Session 11. The PCL-M was administered once per week.
The Throat Questionnaire (TQ; Deary, Wilson, Harris, & MacDougall, 1995) was used to assess how much Roger was affected by throat sensations throughout treatment. Symptoms that were endorsed at pre-treatment as moderately to severely bothersome include feeling of something stuck in the back of the throat, discomfort/irritation in the throat, and difficulty in swallowing food. On the TQ, he was also asked to indicate the time he spent thinking about his throat and the annoyance caused by the throat sensations. At pre-treatment, Roger endorsed a five (7-point Likert with seven as most extreme) for both items.
In addition to monitoring PTSD symptoms, Roger was asked to complete daily food and alcohol monitoring sheets. He was asked to indicate the meal/time of day, food consumed, the amount and type of alcohol consumed with food, subjective ratings of distress while eating (subjective units of distress [SUDS], 0-8), and a brief description of the distressing symptom(s). At pre-treatment, Roger recorded only liquid shakes in the absence of alcohol and four to five alcoholic beverages at each occasion solid food was consumed. SUDS ratings while following this behavior pattern (solid food only with alcohol) were mild to moderate at baseline.
6 Case Conceptualization
The results of the pre-treatment assessment indicated that Roger was experiencing a significant level of distress due to repeated intrusive thoughts related to military combat as well as emotional and physiological reactions to trauma-related cues. Roger reported that he often drank heavily to avoid thoughts related to his combat experiences and avoided crowded areas in which it would be difficult to monitor surrounding activities. He reported extreme helplessness during his traumatic event and stated he believed that this event was also related to his current emotional numbing symptoms that included anhedonia, feelings of emotional detachment and estrangement, and a restricted range of affect. Roger reported that these symptoms began shortly after returning home from deployment and were associated with a chronic course and significant social, interpersonal, and occupational impairment. Collectively, the assessment indicated that he met full criteria for PTSD with moderate to severe impairment.
During the initial assessment, it became clear that Roger was experiencing significant anxiety related to multiple situational and physiological cues (e.g., solid food intake, throat sensations, flying, and trauma reminders) in addition to symptoms of PTSD. Roger’s diverse reports of anxiety-provoking stimuli complicated differential diagnosis; however, he did not meet criteria for generalized anxiety disorder as his anxious avoidance was related to specific stimuli that was usually associated with a precipitating event. For example, Roger developed a fear and avoidance of flying after a single event in which a military transport plane on which he was traveling was forced to make a rapid descent to avoid enemy fire. Although this event led to anxious symptoms and avoidance, it was not accompanied by repeated intrusive thoughts, nightmares, or other trauma-related symptomatology and therefore better conceptualized as a situational flight phobia.
Perhaps most impairing and distressing was the anxiety and subsequent avoidance of solid food that was again precipitated by an identifiable event. When considering the best diagnostic conceptualization to inform the rationale and monitoring of Roger’s treatment, the differential diagnosis between choking phobia (CP) and GP was of crucial importance. Although both GP and CP are associated with avoidance of solid food and can be preceded by a stressful event involving the phobic stimulus, Roger reported significant throat sensitivity and irritation after consuming solid food without alcohol. In addition, Roger reported an almost constant sensation of a “lump in his throat” and a significant preoccupation with throat sensation (e.g., constantly clearing and rubbing his throat). Numerous medical procedures prior to the initial assessment had ruled out a physical cause for Roger’s aversive throat sensations. Providing credence to the absence of a medical cause was Roger’s report that excessive alcohol consumption not only reduced his anxiety when consuming solid food, but also reduced his preoccupation with throat sensations. It appears that after a precipitating choking event, Roger developed a preoccupation related to throat sensations possibly similar to a preoccupation in obsessive-compulsive disorder or a heightened physiological awareness associated with panic disorder.
Given Roger’s co-occurring throat preoccupation and sensitivity, in addition to numerous medical procedures ruling out physical cause of these symptoms, a diagnosis of a conversion disorder based on underlying anxiety, specifically GP, best fits Rogers reported symptoms. Overall, it appears that Roger may have had an underlying predisposition for anxiety as multiple stressful events served as cuing events for anxious symptoms and avoidance. Several studies have provided evidence for individual differences in physiological reactivity to stressful events and subsequent ease of fear conditioning (Shiba et al., 2014). This line of research not only assisted with Roger’s case conceptualization, but also informed the rationale for Roger’s exposure-based treatment.
7 Course of Treatment and Assessment of Progress
Trauma management therapy (TMT), a comprehensive treatment protocol for PTSD (Beidel et al., 2011) that includes exposure therapy (EXP) and social and emotional rehabilitation (SER), was delivered in an intensive 3-week format. The EXP in this treatment program includes the use of virtual reality software (Rizzo et al., 2010) to augment immersion in the imaginal scene. SER includes skill-based training in the areas of social reintegration, anger management, and behavioral activation. Roger received individual EXP each morning and group SER each afternoon, 5 days per week, for 3 weeks.
Individual EXP Session 1
An initial education/treatment planning session was conducted in which the nature of PTSD and its treatment was explained. During this session, details of the traumatic event(s) were obtained to aid in the development of the script for use in the imaginal exposure sessions. The script was prepared using factual details of the trauma as well as thoughts, emotions, and physiological reactivity experienced during the traumatic event. The visuals, sounds, and smells of the virtual reality software were assessed to determine suitability, based on Roger’s unique trauma experience. For Roger, the scene was augmented by VR sounds (Humvee motor; compressor) and VR odors (body odor, garbage, and diesel). An air compressor was used to drive the odor presentations but acted as a stimulus in that it sounded like the generator at the forward operating base (FOB). To further aid in understanding the treatment process, a segment of the imaginal trauma script follows: When you arrive on the scene, the smell of fuel is overwhelming
SUDS were collected every 5 to 10 min throughout the session. The SUDS ratings were graphed and the treatment team utilized the graphs to inform treatment. Specifically, between-session and within-session habituation was analyzed to ensure that Roger was making progress during individual EXP Sessions 2 to 15
Each EXP session lasted between 90 to 120 min, and included a clinician review of functioning since last session, including level of distress experienced, number of alcoholic beverages consumed, presence of suicidal ideation, and number of verbal or physical anger episodes. Roger rated his level of distress between sessions as Moderate (4) until Session 7; remaining sessions were rated as Mild (2) to No Distress (0). No suicidal ideation was endorsed at any session.
In addition to receiving EXP on a daily basis, Roger participated in daily group therapy (SER) designed to target anger management, social isolation, and depression, three primary areas associated with PTSD that are often not targeted by EXP. The group in which Roger participated included four members, all of who met criteria for combat-related PTSD. The group leaders were doctoral-level graduate students who were experienced group leaders. The group sessions were skill based, with role-plays in session and homework assignments in which participants were instructed to practice the skills outside of the therapy environment.
As can be seen in Figure 1, the patient had a significant decrease in PTSD symptoms from baseline (CAPS score of 63) to post-treatment (CAPS = 17), which was largely maintained at 3-month follow-up. A CAPS score of 50 or greater is consistent with a diagnosis of PTSD; Roger was significantly below the cut-off at post- (17) and at 3-month (25) assessment. The PCL-M also decreased from baseline (41) to the final week of treatment (31). Although consistent with Roger’s CAPS score, symptoms on the PCL-M may have been somewhat minimized as Roger’s Cluster C (Avoidance and Numbing) scores on the CAPS and PCL-M were the most elevated. This indicated that other symptoms may also be minimized due to avoidance of relevant triggers. Roger’s follow-up assessments were done by phone and therefore PCL-M information is not available.
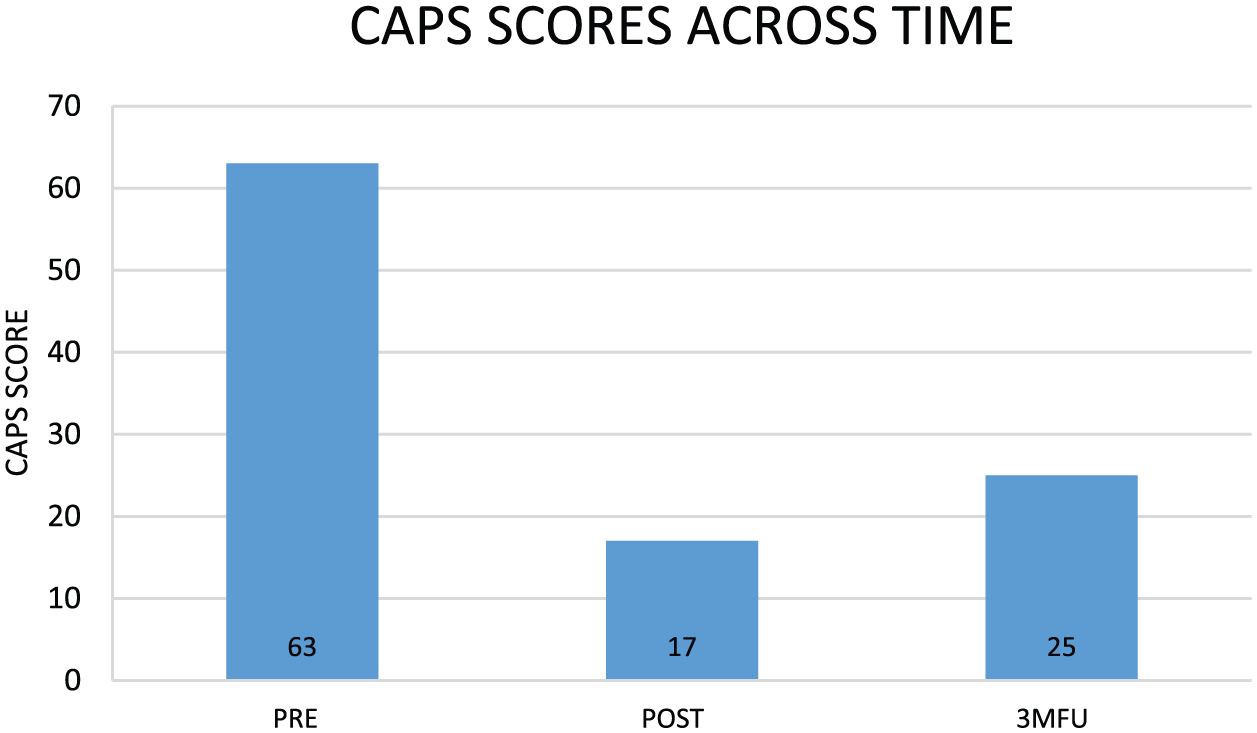
Changes in CAPS scores.
In addition to the standard TMT 3-week protocol, Roger received additional therapy to target fear of choking and avoidance of eating solid foods (without alcohol). The treatment was delivered in a stepwise fashion with TMT only Week 1, TMT, relaxation training, and breathing retraining (RT) Week 2, and TMT and solid food exposure (FE) Week 3. Relaxation training and relaxation training was delivered in Week 2 to control for the added therapist time and attention that would occur in Week 3 during food exposure. It is important to note that relaxation was not used during exposure therapy and that eating solid foods in the absence of alcohol was not targeted until Week 3. TMT was delivered across all 3 weeks.
Individual Food EXP 1 to 9
Food exposure sessions were modeled after TMT exposure sessions and consistent with flooding principles. In collaboration with the therapist, Roger selected a meal that would be “extremely” anxiety provoking for him to eat without consuming alcohol. Roger selected a hamburger and french fries and this meal was kept consistent across lunch exposure sessions to facilitate habituation. Dinner exposure sessions were conducted with various meals that Roger’s hotel provided to promote generalization. Each session began with Roger identifying his baseline SUDS rating. Food exposure sessions varied in length (between 15-45 min), but would end when a 50% reduction in Roger’s SUDS ratings was observed or Roger’s ratings returned to baseline. Importantly, Roger did not require constant food swallowing for the entire exposure session as his anxiety centered on a preoccupation with the food remaining lodged in his throat and would remain anxious without the need for continued food consumption or swallowing.
With regard to the symptoms of GP, Roger showed a pattern of change that was directly related to the phase of treatment. To understand the TQ scores shown in Figure 2, it is important to remember that Roger did not consume solid food without consuming alcohol until the beginning of Phase 3, which directly targeted solid food intake in the absence of alcohol consumption. Although his score of 17 at baseline was somewhat mild with moderate to severe endorsement of “feeling something stuck in the throat,” “discomfort/irritation of the throat,” and “difficulty swallowing food,” he did not experience more severe symptoms until food was introduced in the absence of alcohol. At that point in treatment, he had a TQ score of 29 (see Figure 2), which included two additional symptoms that were rated as severe (“can’t empty throat when swallowing” and “food sticking when swallowing”). It is also important to note that this increase supports the therapist conceptualization of Roger’s throat sensations being linked to anxious symptomatology as TQ and SUDS ratings were highly correlated (r = .92) across treatment. By post-treatment, his TQ was below baseline (7) and gains were maintained at 3-month follow-up (5), with no symptoms rated at a moderate or severe level. Perhaps more importantly, Roger’s response to the item “How much time do you spend thinking about your throat” was rated as a five (scale of 1-7) at baseline, as a two at post-treatment, and a zero at 3-month follow-up.
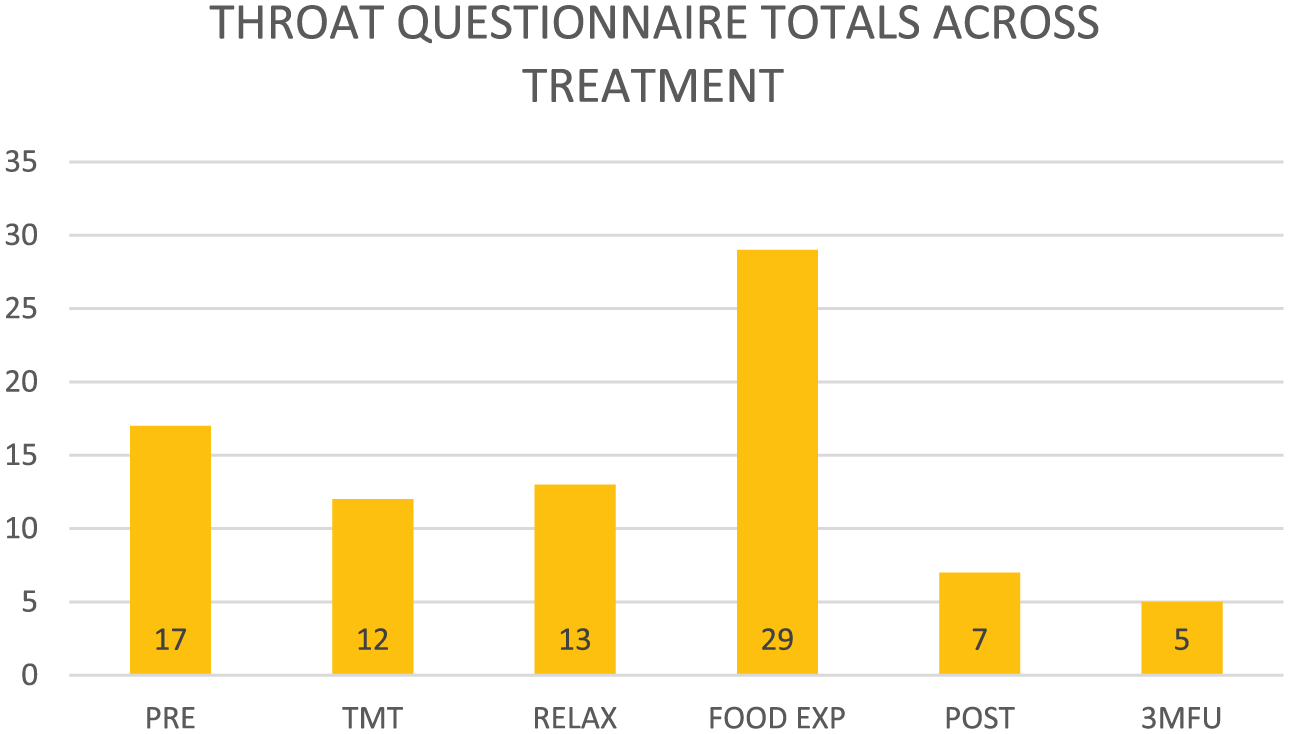
Throat Questionnaire scores.
During the food exposure sessions (Phase 3 of treatment), Roger’s peak SUDS can be seen in Figures 3 and 4 representing the lunch and evening meals, respectively. It is clear that the patient’s rating of distress while eating solid foods without alcohol decreased quickly over that week. The noon meal consisted of a burger and fries each day while the evening meal was provided to guests of the hotel in which Roger was staying. Thus, the particular food stimulus at the evening meal varied and was not under the control of the therapist or the patient, hopefully leading to generalization across food types.
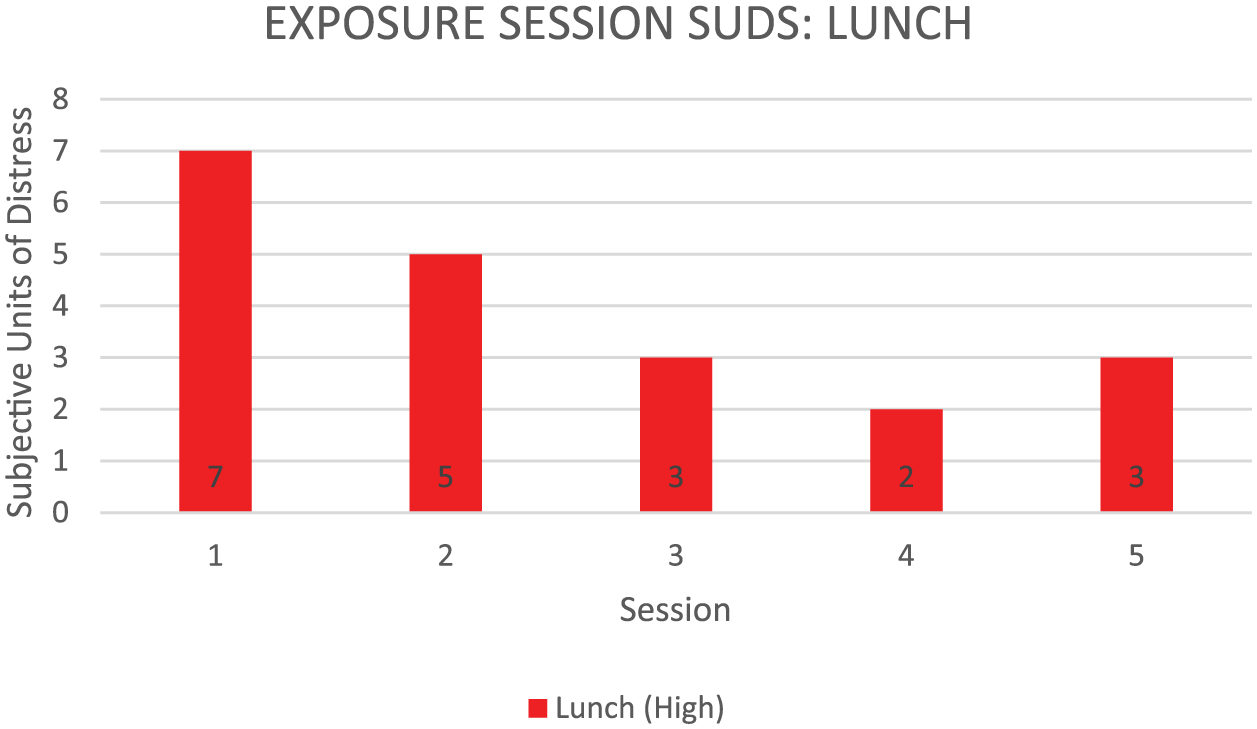
Peak SUDS ratings during lunch food exposure.
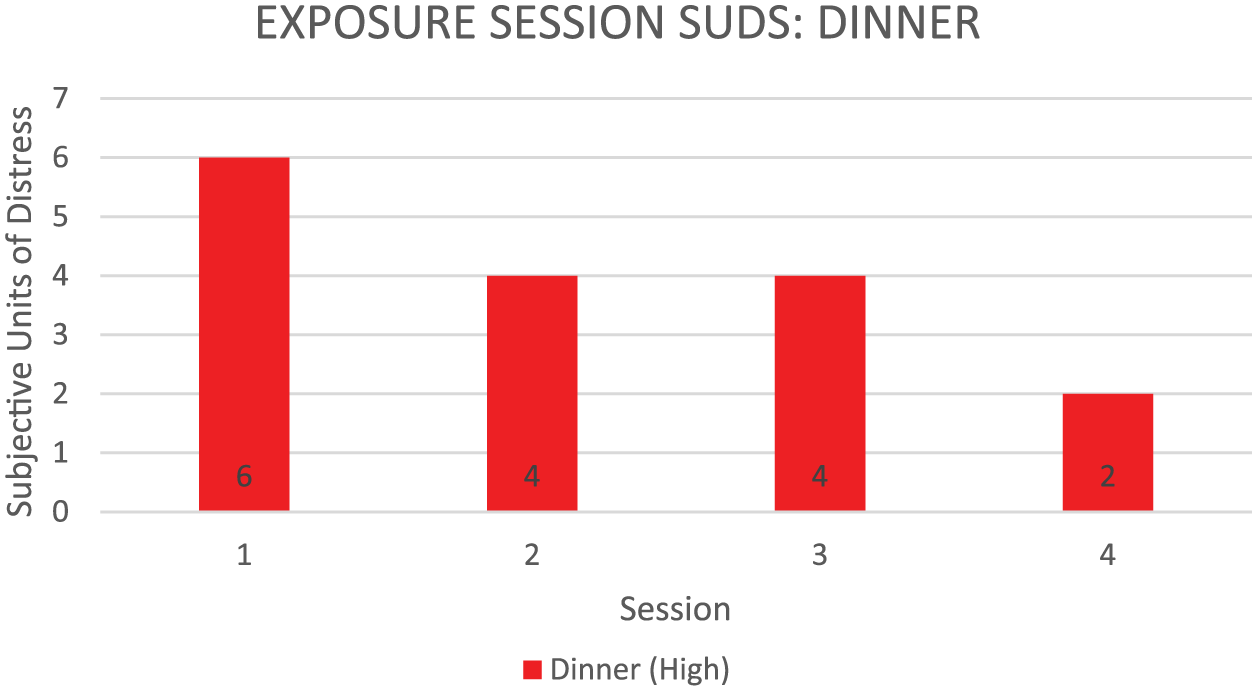
Peak SUDS ratings during dinner food exposure.
Amount of food consumed during the noon food exposure sessions can be seen in Figure 5. The therapist was able to photograph the actual food consumed in the clinic at lunch.

Food consumed during noon exposure sessions.
Roger consumed evening meals in a public restaurant, so we did not take photographs of the food consumed. Of great interest is the fact that as Roger consumed greater quantities of food, his distress level decreased. As shown in Figure 5, Roger was able to consume an entire hamburger and order of french fries by the end of treatment for GP with little or no distress.
Given Roger’s fear of consuming solid foods without drinking alcohol, we initiated self-monitoring of alcohol consumption at the beginning of the 3-week treatment program. Figure 6 depicts alcohol consumed when eating solid foods throughout the course of treatment. Food exposure started at Session 12, at which point Roger was instructed not to drink prior to consuming solid foods. Roger consumed from three to five alcoholic beverages to eat solid foods until the initiation of Phase 3 in which eating solid food (without alcohol) was directly targeted. The drinks consumed prior to this phase were self-reported. In the case of drinks consumed during Phase 3, the therapist being present during both lunch and dinner confirmed the absence of alcohol. Prior to this treatment phase, Roger consumed alcohol prior to every meal. However, on the day of Session 9, Roger abstained from solid food and consumed only liquids. Self-report of alcohol consumption to reduce anxiety related to solid food intake was denied at 3-month follow-up assessment. It is important to note that alcohol consumption was measured only in relation to solid food consumption. Other alcohol consumption was minimal and was not targeted in this treatment program.

Alcoholic drinks consumed with food.
8 Complicating Factors
It is important to note that Roger was a compliant patient and did not demonstrate agitation or treatment refusal that a clinician might expect from a patient participating in multiple daily-exposure sessions. This may be partially explained by the treatment protocol, as Roger was able to see a reduction in PTSD as a result of exposure sessions before beginning food exposure. The graduated session treatment protocol may have provided Roger with sufficient motivation and facilitated treatment adherence.
Due to the intensive nature of the TMT treatment program, which included EXP in the morning and SER group therapy in the afternoon, adding the treatment for GP required increased time and coordination. The therapist was required to be present at both lunch and dinner hours to implement the exposure to food. Given that alcohol was readily available at the hotel during the dinner hours, the therapist was required to monitor that the food was consumed in the absence of alcohol. Follow-up assessment was also complicated in that Roger lived 8 hr from the clinic, so telephone and United States Postal Service mail were utilized to collect follow-up information.
Other complicating factors included Roger’s place of employment as he worked as a waiter in a restaurant/bar. He typically consumed his evening meal at the restaurant where alcohol was readily available. Although he denied consuming alcohol to eat solid foods following treatment, there is no verification. Marital issues continued to be a complication for Roger when he returned to his home environment. Marital therapy was recommended.
9 Access and Barriers to Care
There were no significant barriers to care. Treatment was provided on a daily basis and addressed both PTSD and GP directly, albeit in a stepwise fashion. Roger was financially able to purchase each noon meal for the food exposure and the hotel provided the evening meal. Roger returned to his home and continued food exposure in his environment.
10 Follow-Up
To assess functioning in his usual setting, Roger was contacted by phone for his post-assessment 1 week after completing the 3-week treatment program. The CAPS was completed to determine level of PTSD symptomatology. At the 3-month assessment, we completed the CAPS over the phone as well. Information regarding food intake and throat sensitivity was based on self-report at both follow-up time points. Roger indicated that he had no difficulty consuming solid food in the absence of alcohol and that he had little or no distress regarding throat sensations.
11 Treatment Implications of the Case
The case study outlined above details the successful treatment of a veteran with PTSD using an intensive 3-week treatment modality referred to as TMT. In addition to the intensive TMT protocol, the veteran was provided with relaxation training and exposure therapy to reduce anxiety related to solid food consumption and throat preoccupation. Given the intensive PTSD (3-week) and GP (1 week/2× per day) nature of treatment, for PTSD (2× per day for 3 weeks) and GP (3rd week/2× per day), perhaps the largest implication of this case study is the validity of short-duration, intensive exposure-based treatments. Not only was an intensive 3-week treatment modality shown to be effective in this case, the treatment gains were maintained at follow-up. An effective intensive treatment modality has specific implications for the health care community as efficacious short-duration treatments can assist in reducing the cost and health care burden associated with treatment.
Given the low base rate of GP, research is significantly lacking in this area especially considering the role of anxiety that may underlie this condition. Furthermore, research is needed in the area of identifying individuals with a predisposition for fear conditioning and if this predisposition may be associated with an amenable outcome for exposure-based therapies.
12 Recommendations to Clinicians and Students
The lack of literature and specified treatment protocols for conversion disorder is not surprising given the low prevalence and diversity in presentation. However, the absence of guidance for treatment coupled with psychiatric and medical comorbidities increase the difficulty of treatment decisions for clinicians and raise questions as to the structure and order of treatments. Several details of Roger’s case provide the basis for beneficial recommendations for clinical professionals and students.
Roger’s case demonstrated the efficiency, feasibility, and efficacy of intensive multicomponent behavioral treatments for anxiety-based disorders. The entirety of Roger’s treatment was carried out over 3 weeks, the beneficial effects of which were observed at 3 months post-treatment. Although it may not be feasible in some treatment settings to conduct multiple exposure sessions per day to target comorbidities, Roger’s case demonstrated the efficacy of treating anxiety-based disorders simultaneously. In addition, if individuals are provided with adequate instruction, they may easily generalize exposure techniques and implement them independently outside of session.
The present case study also illustrates the importance of thorough and on-going assessment, as the underlying cause of Roger’s conversion disorder appeared rooted in anxiety and was associated with a preoccupation and monitoring of throat sensations. A thorough review of Roger’s medical records ruled out a possible medical cause for Roger’s condition. This information coupled with Roger’s report of worsening throat sensations during times of heightened stress lead to an anxiety-based case conceptualization and recommendation of exposure therapy as the appropriate treatment. This conceptualization was supported by Roger’s self-reported increase in anxious symptomatology and throat irritation in the early phase of food exposure treatment.
In conclusion, the current case study demonstrates the successful implementation of multicomponent TMT for PTSD in conjunction with additional exposure sessions targeting co-occurring conversion disorder and food avoidance. Roger maintained treatment gains 3 months post-treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The patient was part of a study funded by the Military Operations Medicine Research Program, U.S. Army Medical Research and Materiel Command (USAMRMC), Award Number W81XWH-11-2-0038.