
Abstract
Given the long-term negative outcomes associated with depression in adolescence, there is a pressing need to develop brief, evidence-based treatments that are accessible to more young people experiencing low mood. Behavioral Activation (BA) is an effective treatment for adult depression; however, little research has focused on the use of BA with depressed adolescents, particularly with briefer forms of BA. In this article, we outline an adaptation of brief Behavioral Activation Treatment of Depression (BATD) designed for adolescents and delivered in eight sessions (Brief BA). This case example illustrates how a structured, brief intervention was useful for a depressed young person with a number of complicating and risk factors.
1 Theoretical and Research Basis for Treatment
Behavioral Activation (BA)
BA is an established evidence-based treatment for major depressive disorder (MDD) in adults, based on long-standing behavioral models of the development and maintenance of depression (e.g., Fester, 1973; Lewinsohn, 1974). Although cognitive therapeutic approaches gained popularity toward the end of the 20th century, a landmark dismantling study of cognitive-behavioral therapy (CBT) for adult depression by Jacobson et al. (1996) showed that the full CBT package (i.e., including both cognitive and behavioral components) was no more effective than the behavioral components alone. This reignited interested in purely behavioral interventions and led to the development of two contemporary BA approaches. Behavioral Activation (BA: Martell, Addis, & Jacobson, 2001; Martell, Dimidjian, & Hermann-Dunn, 2010) includes detailed idiographic functional analysis, while Brief Behavioral Activation Treatment for Depression (BATD: Lejuez, Hopko, & Hopko, 2001) and the revised version (BATD-R: Lejuez, Hopko, Acierno, Daughters, & Pagoto, 2011) provide a more concise targeting of reinforcement for depressed/nondepressed behavior. Both BA and BATD acknowledge the possible role of cognitions in the development and maintenance of depression but address only behavioral change and reinforcement.
The Martell and colleagues’ model of BA (Martell et al., 2001; Martell et al., 2010) comprises 20 to 24 sessions and is based on a functional analytic rationale, including consideration of both avoidance and approach behaviors. Additional strategies such as mindfulness, rumination, and/or relaxation exercises have also been included. There is a strong evidence base for the effectiveness of this approach for adult depression (e.g., Dimidjian et al., 2006). Less work has focused on young people although Ritschel, Ramirez, Jones, and Craighead (2011) adapted this BA approach and reported on its use with six depressed adolescents aged 14 to 17 years. Parents were invited to join sessions at least 3 times (at the beginning, middle, and end of treatment). Up to 22 sessions were available over 18 weeks. The mean number of sessions attended was 14, with a maximum of 16; no participant attended the full number of treatment sessions. Depression symptoms significantly improved, and four of the six participants were scoring in the normal range on the depression measures at the end of treatment. The same research group also reported a successful case series of BA with three African American adolescents (Jacob, Keeley, Ritschel, & Craighead, 2013), suggesting the approach can be further tailored to different populations. Another small study reported a group BA adaptation for five young people (aged 12-14 years) with comorbid depression and anxiety (Chu, Colognori, Weissman, & Bannon, 2009). By the end of treatment, three of the four treatment completers no longer met criteria for their primary anxiety or depression diagnosis.
McCauley, Schloredt, Gudmundsen, Martell, and Dimidjian (2011) have also adapted the adult Martell version of BA for depressed adolescents. The “Adolescents Taking Action” BA program involves 14 sessions over 12 weeks and includes much of the adult Martell-based protocol. McCauley et al. (2011) reported a successful case to highlight developmental issues in adapting BA for adolescents, including a need to consider working with rumination, balancing structure with flexibility, assessment of suicidal ideation, and including the family as part of the engagement process.
In the largest published study of BA with adolescents, McCauley et al. (2016) conducted a randomized controlled trial with 60 depressed adolescents. Participants were randomized to a 14-session Adolescent Behavioral Activation Program (A-BAP, n = 35) or to Evidence-Based Practice for Depression (EBP-D, n = 25), which was up to 14 sessions of either CBT (n = 21) or interpersonal psychotherapy (IPT; n = 4). Of the 27 young people who completed A-BAP and the posttreatment assessment, 21 did not meet diagnostic criteria for depression at the end of treatment, compared with four of the 16 in the EBP-D group who completed the posttreatment assessment. There were significant reductions in depression symptoms in both groups and no significant difference between treatments. However, data were reported only on those participants who completed treatment and the research assessments. This will tend to exaggerate the overall benefits of treatment because young people who dropped out of treatment and/or research are not included, and are more likely not to have recovered or significantly reduced symptoms. However, the study results demonstrate that BA can be delivered to adolescents and may have similar efficacy as existing evidence-based treatments.
BATD and BATD-R
The second BA approach, BATD, was developed at around the same time as BA by another research team led by Lejuez et al. (2001), and a revised treatment protocol was published in 2011 (BATD-R; Lejuez et al., 2011). This focuses on both increasing reinforcement for nondepressed behavior and decreasing reinforcement for depressive behavior. This simplified and brief approach consists of five to 10 manualized sessions that can be delivered by a nonspecialist therapist. Sessions include a collaborative exploration of each client’s idiosyncratic motivations and interests to identify “value-based” (and therefore, personally rewarding) activities unique to that individual.
The BATD protocol has been adapted for a range of settings and clients, including adults with substance misuse (Banducci, Long, & MacPherson, 2015; Daughters et al., 2008) and depressed or newly enrolled college students (Gawrysiak, Nicholas, & Hopko, 2009; Reynolds, MacPherson, Tull, Baruch, & Lejuez, 2011). Individual case studies have been reported on the successful use of BATD for a variety of presentations, including with those who have ethnic minority status (Kanter, Hurtado, Rusch, Busch, & Santiago-Rivera, 2008; Vergara-Lopez & Roberts, 2015) and coexisting medical problems such as breast cancer (Armento & Hopko, 2009) and colitis (Hopko, Lejuez, & Hopko, 2004).
The evaluation of BATD suggests that this relatively brief, simple intervention (that can be delivered by therapists with minimal training) is associated with good adherence to treatment, significant reductions in symptoms of depression, and (where relevant to the study in question) smoking and problem drinking. Where control conditions were included in study designs, BATD evidenced significantly greater improvements on outcome measures compared with no treatment (e.g., Gawrysiak et al., 2009) or treatment as usual (e.g., Daughters et al., 2008).
One case study reported the successful use of BATD with a 17-year-old (Ruggiero, Morris, Hopko, & Lejuez, 2005), suggesting it may be suitable to use with young people, although this requires further investigation.
Adapting BA for Adolescents: Brief BA
MDD in adolescence is a common and debilitating disorder, affecting 2.6% of young people at any one time worldwide (Polanczyk, Salum, Sugaya, Caye, & Rohde, 2015). In the United States, a large-scale population survey of more than 10,000 adolescents found a 12-month MDD prevalence of 7.5% in 13- to 18-year-olds, with a lifetime prevalence of 11.0% (Avenevoli, Swendsen, He, Burstein, & Merikangas, 2015).
Adolescent depression is a major risk factor for depression in adulthood (Naicker, Galambos, Zeng, Senthilselvan, & Colman, 2013), as well as placing individuals at increased risk of substance misuse (Asarnow et al., 2014) and suicide (Bridge, Goldstein, & Brent, 2006). As depression is so common during adolescence and has such adverse long-term impacts, it is vital to make effective treatments available promptly and to make them appealing and engaging to young people. The recommended treatments for depression in young people include CBT and IPT in both U.K. (National Institute for Health and Care Excellence [NICE], 2015) and U.S. (Birmaher, Brent, & AACAP Work Group on Quality Issues, 2007) guidelines.
There is substantial treatment drop-out rate across all types of psychological therapy with young people (de Haan, Boon, de Jong, Hoeve, & Vermeiren, 2013). Access to treatment is limited by a lack of trained therapists to deliver evidence-based approaches in most developed countries. There is also evidence that adolescents with depression have deficits in abstract cognitive reasoning and executive functioning (Wagner, Müller, Helmreich, Huss, & Tadić, 2014) that may interfere with their ability to engage fully in CBT. On the basis of data suggesting that young people did not complete all sessions of lengthy therapies, we reasoned that a brief treatment would be more acceptable to adolescents and their families, especially as this would mean less interruption of activities adolescents are managing to continue (e.g., school/college). An additional feature of BATD is that the client’s values are explored collaboratively to identify value-based (and therefore, personally rewarding) activities unique to that individual. This may be of particular salience to adolescents given their desire for autonomy; their developing understanding of their priorities, ambitions, and motivations; and sensitivity to rewards. For these reasons, BATD, which is brief in duration, focuses on identifying the young person’s own values, and is simple to grasp and deliver, may be an effective and cost-effective treatment for adolescent depression.
Pass, Brisco, and Reynolds (2015) reported how BATD was adapted for adolescents in the United Kingdom. The developmentally appropriate changes made to the protocol resulted in a structured treatment manual of eight sessions (Pass & Reynolds, 2014). The manual includes illustrated materials specifically designed for young people with case study examples, and explicit consideration of the role of parents/caregivers. All BA approaches aim to increase positive reinforcement of nondepressed behavior. For adolescents, parents or caregivers are usually a vital source of reinforcement, and they are therefore incorporated in therapy, given a treatment manual, and are involved in co-monitoring their child’s symptoms and functioning. Within treatment, parents are specifically involved in psycho-education and understanding the treatment rationale (Session 1), contracting and problem solving (Session 6), and relapse prevention and planning (Session 8 and review session). Parents are involved in contracting and problem solving to increase parental engagement, and to address barriers to change that they may be contributing to or could help their child overcome.
2 Case Introduction
Client Characteristics
“Amy” (a pseudonym) was a 16-year-old Caucasian girl who lived with her mother in a large town in the United Kingdom. She was in full-time, mainstream education and from a family of average socioeconomic status for the area. This case was one from an open case series, where pilot Brief BA data were being collected in a local Child and Adolescent Mental Health Service (CAMHS). Amy was one of the first young people to complete Brief BA and provided consent to share her story with others.
Clinician Characteristics
The first author (L.P.) was the Brief BA clinician who worked with Amy. She is a qualified clinical psychologist, working in a research setting alongside the local CAMHS. L.P. was supervised by H.W., a qualified clinical psychologist. L.P. and H.W. had attended training on BATD by Carl Lejuez, and all authors were involved in adapting the adult BATD manual for adolescents (Pass & Reynolds, 2014).
3 Presenting Complaints
Amy had been referred by her primary care physician to her local CAMHS due to persistent low mood and feelings of worthlessness.
4 History
Amy described a 3-year history of depressive symptoms. Within this time period, she reported variations in the level and types of symptoms experienced; for example, she had previously self-harmed on a weekly basis (using a pencil sharpener blade to create superficial cuts on her arms and thighs, which led to bleeding but no need for medical attention). She had not engaged in this behavior for the past 4 months. However, Amy and her mother reported that over the last year, Amy’s mood had been consistently low and, before presenting to her primary care physician, they reported worsening difficulties with excessive sleeping, poor appetite, and impaired concentration. At the time of starting Brief BA, Amy had been on a stable dose of 20 mg Fluoxetine for 3 months. Amy had also experienced extreme fatigue for 4 years and had undergone repeated tests for type 2 Diabetes. Although her test results were negative, her mother was careful to monitor Amy for signs of low blood sugar between meals and encouraged a healthy diet, including cutting out sugary drinks.
Amy was born after a full-term pregnancy with no complications and had met all developmental milestones. In her adolescent years, Amy had experienced a number of significant stressors. Four years before her referral to CAMHS, Amy’s father had died from cancer, and 6 months before the referral, Amy’s mother had been diagnosed with bowel cancer and non-Hodgkin lymphoma (they were awaiting news about her prognosis at the time of referral). Amy received bereavement counseling after her father’s death, and she and her mother also received family therapy, which they described as helpful. There was a significant history of mental health difficulties within the family. Before his death, Amy’s father had been diagnosed with bipolar disorder and had been admitted to an inpatient ward following an episode of mania. Amy’s mother reported a history of recurrent MDD.
Amy lived with her mother and reported a very close and supportive relationship with her. She had an older half brother (14 years older than her) who lived locally with his wife and young children. Amy had missed a significant amount of school in recent months due to her mood. Before the onset of depression, she was popular at school and had been receiving excellent grades. In the current school year, Amy had been feeling overwhelmed by coursework, and Amy’s mother reported that Amy was more stressed and anxious.
5 Assessment
Measures
Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS)
As routine practice in the service, Amy and her mother completed the K-SADS (Kaufman et al., 1997). This structured diagnostic interview includes assessment of mood and anxiety disorders, behavioral disorders, and schizophrenia. The young person and their parent(s) are interviewed separately, and then a consensus is agreed between their reports (for older adolescents, self-report is given greater weighting than parental report for emotional disorders; however, Amy and her mother reported very similar views). The K-SADS was completed by two graduate researchers, and the diagnostic decision was made in discussion with a clinical psychologist. Amy met criteria for moderate MDD with six symptoms: depressed mood/irritability, suicidal ideation, sleep disturbance, cognitive difficulties, appetite disturbance, and negative self-perceptions, including feelings of worthlessness. Amy did not meet criteria for any anxiety or other mental health disorders.
Amy and her mother also completed the following questionnaires, which are routinely used in the clinic and more widely in CAMHSs in England.
Revised Child Anxiety and Depression Scale (RCADS) and Revised Child Anxiety and Depression Scale-Parent Version (RCADS-P)
The RCADS (Chorpita, Yim, Moffitt, Umemoto, & Francis, 2000) and RCADS-P are 47-item questionnaires that assess anxiety and low mood in young people aged 8 to 18 years. There are subscales for five anxiety disorders (Social Phobia, Panic Disorder, Separation Anxiety, Generalized Anxiety, and Obsessive-Compulsive Disorder) and MDD; these subscales can be summed to create a total anxiety and total internalizing score. The full RCADS and RCADS-P were completed at initial assessment and at Session 8. The self- and parent-report RCADS MDD subscales were completed immediately before every BA session, and an additional question (“I thought about killing myself”/“My child thought about killing himself or herself”) was added to monitor risk. The RCADS and RCADS-P have good construct validity (Chorpita et al., 2000), high internal consistency (Chorpita, Moffitt, & Gray, 2005), and test–retest reliability (Chorpita et al., 2000; Ebesutani, Bernstein, Nakamura, Chorpita, & Weisz, 2010).
Outcome Rating Scale (ORS)
The ORS (Miller & Duncan, 2000) was used to assess Amy’s functioning. On the ORS, clients (and parents) are asked separately to rate, on a 10-cm scale, the young person’s functioning in four key areas: Individual, Interpersonal, Social, and Overall. Placement of a mark on each line is used as a score for each area, which are measured to the nearest mm from the left hand point (so marks further towards the right indicate higher scores). The four scores are summed to give an index of overall functioning. The ORS has high internal consistency and test–retest reliability, and good concurrent validity with other treatment outcome measures such as the Youth Outcome Questionnaire (Duncan, Sparks, Miller, Bohanske, & Claud, 2006). The ORS was completed before every BA session by Amy and her mother.
As per standard care in the service, questionnaire scores were reviewed at every session to consider progress and/or any particular areas of difficulty, and reflect on agreement/conflict between adolescent- and parent-report.
6 Case Conceptualization
While the longitudinal formulation of the development of Amy’s difficulties was not explored during sessions, the therapist held in mind the likely impact of negative life events on the level of positive reinforcement for healthy behavior in Amy’s life. From a behavioral perspective, the loss of Amy’s father, her mother’s illness, Amy’s symptoms of fatigue, and a recently increased academic workload were likely to have caused a reduction in positive reinforcement. It is also possible that following her father’s death, Amy was negatively reinforced for avoiding academic and social demands, and positively reinforced for this by the time and attention she received from her mother. As with all Brief BA cases, the therapist was mindful of their own role in positively reinforcing healthy behavior through brief BA and the potential loss of this at the end of therapy. Amy’s mother was identified as being a possible key facilitator of brief BA given her supportive relationship with Amy, and her role in reinforcing healthy behavior beyond the end of Brief BA sessions was noted.
Brief BA uses a simple maintenance cycle to illustrate to young people how lack of positive reinforcement increases low mood (see Figure 1), which is illustrated and personalized for each client. Amy recognized how her withdrawal was keeping her feeling low and reducing rewards/positive reinforcement. The therapist and Amy also discussed her symptoms of fatigue in relation to this cycle; Amy felt too tired to go out with friends, which further reduced opportunities to get the “feel good factor” from life and maintained her low mood and fatigue.
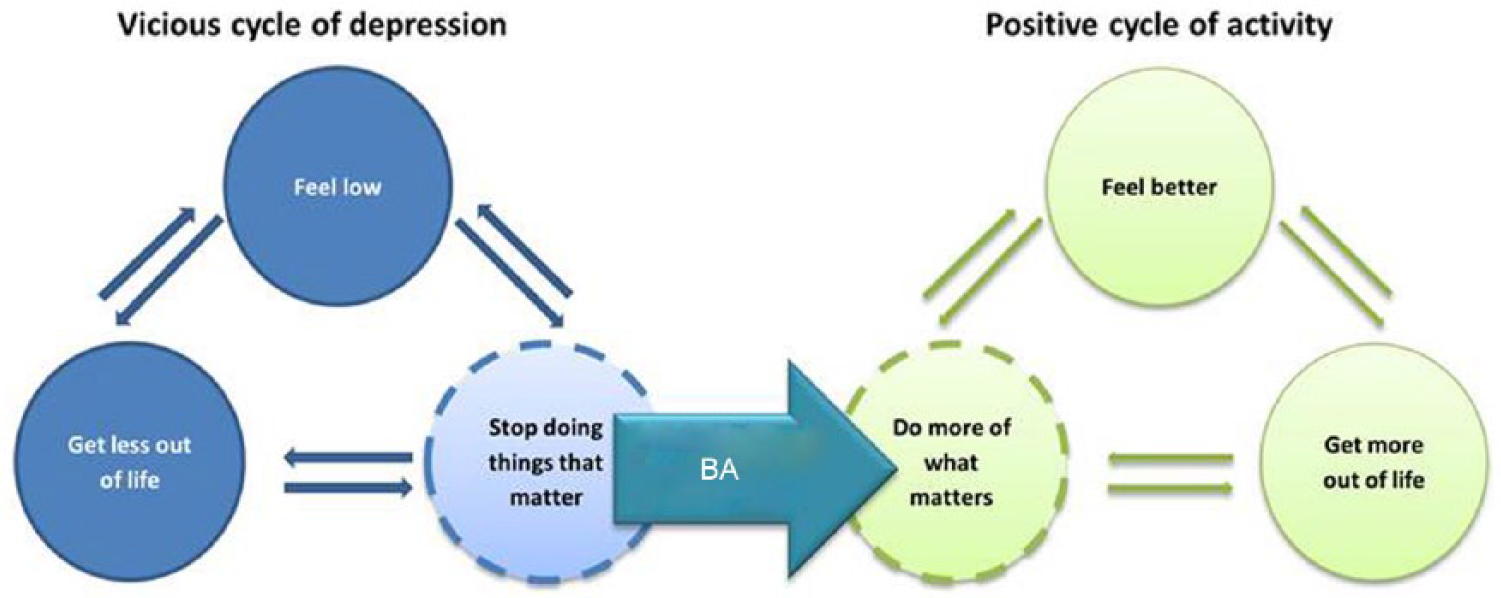
Simplified old versus new behavioral maintenance cycle used in Brief BA.
Amy had stated in her assessment that she wanted something more “practical” than the bereavement counseling she had received previously. She felt that she had already had an opportunity to explore her feelings toward her father’s death, and this was not her aim for the current work.
7 Course of Treatment and Assessment of Progress
Brief BA is structured (see Pass et al., 2015) but allows for material to be covered at a varying rate, depending on individual clients. Here, we will focus on how Brief BA was used with Amy and in particular how it was delivered in the context of risk and additional complexity. The course of treatment began during the break between Amy finishing school and starting college.
Sessions 1 and 2: Engagement and Treatment Rationale
In the first session, the Brief BA approach was discussed with Amy and her mother, both of whom seemed keen on this type of intervention. The behavioral model and the key principles of reinforcement were highlighted (see Figure 1), and Amy and her mother reported that Amy’s “motivation levels” had improved since her assessment. They linked this to the end of her examinations and to her starting antidepressant medication. In Session 1, Amy identified her primary goal was “to be more confident,” which she operationalized as meaning: “Talk to people.” Amy felt she was 3 to 4/10 toward achieving this goal at this time. In Session 1, Amy agreed to keep an activity log, and to consider whether activities gave her a sense of Achievement, Closeness, and/or Enjoyment (ACE; Vivyan, 2014) and whether they were important to her. Amy’s mother was given an additional parental handout on the importance of providing positive reinforcement for nondepressed behavior.
In Session 2, Amy reported that she thought “BA is what I need,” as she considered “doing stuff” would be helpful. She compared this with counseling which she described as “upsetting.” Between Sessions 1 and 2, Amy had found it difficult to complete the activity log fully but reported specific helpful activities (e.g., making bracelets was calming when she felt stressed and making the effort to get in touch with friends had been experienced as “worth it”). In Session 2, Amy reported that she was now thinking more actively about “trying to fill days more” (especially as she no longer had school and did not have a job), suggesting that she had understood the key elements of the Brief BA model.
Session 3: Risk Management
In Session 3, Amy disclosed that she had self-harmed and taken an overdose 2 days previously. In line with the clinic protocol, Session 3 was therefore used for risk assessment and safety planning. The Brief BA content was moved to the following session.
Amy explained she had taken an overdose of Paracetamol (U.S. generic name, Tylenol) in response to feeling abandoned by her friends. During a trip to the beach, she had fallen asleep sunbathing and her friends had left her alone to go get ice creams. This incident followed conflict with her half brother earlier in the week, where he had retracted his offer to go on a family holiday with Amy, their mother, and his family. Amy said that the trigger for the overdose was her belief that that “everyone leaves me” and that she had “lost everyone.” She said that the overdose was not an attempt to end her life but “to shut everything out.” However, she also reported that at the time she took the overdose, she did not care whether she survived.
A risk management plan was agreed with Amy and her mother. This involved (a) Amy agreeing to the therapist sharing information about her suicidal thoughts with Amy’s mother, (b) reiterating advice to remove any medication from easily accessible places, (c) agreeing that Amy’s mother would ask Amy directly whether she was having thoughts about suicide, and (d) Amy agreeing to let her mother know when she needed help to stay safe. Amy and her mother were also advised to visit their family physician for a physical health check. It was discussed that if Amy’s mother did not feel confident in the risk management plan and the associated reduction in Amy’s risk, she should reconsider whether to allow Amy to go on an upcoming volunteering trip to Sri Lanka. Following this session, Amy and her mother reported feeling more confident in her staying well and Amy went on the preplanned 2-week trip.
Sessions 4 to 6: Identifying Values and Activities Across Life Areas
Session 4 took place after a 2-week break following Amy’s trip to Sri Lanka. Amy reported feeling “really good,” and her ORS score indicated improved functioning (see Figure 3). She reported higher symptoms of depression on the RCADS subscale but attributed this to jet lag; she did not feel these accurately reflected her current mood. Amy reported that both her sleep and eating routine were severely disrupted due to jet lag, therefore inflating her responses on a number of items, including “I have trouble sleeping,” “I am tired a lot,” “I have no energy for things,” and “I feel like I don’t want to move” (due to tiredness as a result of sleep disruption), and “I have problems with my appetite” (due to the time difference affecting her eating patterns). These ratings were therefore not used for the session. Amy reported that her volunteering trip had been a great success, filled with activities that gave her a sense of ACE, as well as being Important to her (ACE-I). The link between these activities and her improved functioning and mood was highlighted to illustrate the BA rationale, and how Amy could apply the same principles in her day-to-day life to maintain these gains.
In Sessions 5 and 6, the therapist introduced the idea of values and linking these to Amy’s activities (see Table 1). In Brief BA (Pass & Reynolds, 2014), young people are encouraged to identify values focused on three key areas; “me,” “the things that matter,” and “the people that matter.” Amy was able to identify values in each area. She felt that she wanted to focus on values associated with her own well-being such as “putting myself first” (rather than things and/or people that matter). She stated that this was because it was an area she normally neglected and that, although it would be difficult to prioritize activities that would support her own well-being, this would be more useful to her in the long term.
A Selection of Amy’s Values and Associated Activities.

Discussing Amy’s values in Session 5 also highlighted areas in which she was acting contrary to her values, as well as areas in which she had minimal value-based activities. For example, Amy recognized that “helping others who [she perceived] need help” was an important value for her. This was in contrast to her tendency to try to help others indiscriminately. She also recognized that she did not value her usual behavior of accommodating other people before herself (e.g., always going along with her friends’ plans for socializing).
Sessions 5 and 6 also identified new or additional behaviors that Amy was able to link to her values. These included concrete and time-limited behaviors (e.g., “have a smoothie for breakfast”) as well as more ambitious and abstract behavioral goals (e.g., “arrange seeing friends on my terms”). The therapist and Amy worked collaboratively to identify concrete activities that would contribute to the more ambitious and abstract goals, and to schedule specific times to try these. Amy also found opportunities independently to enact her values; for example, between Sessions 5 and 6, she assertively negotiated a meeting with a friend at a time and place convenient for her, rather than meet at a place chosen unilaterally by her friend. She also applied for a number of jobs (which she felt was working toward her value of putting herself first).
Session 7: Progress Review With Amy and Her Mother
Before Session 7, Amy moved to a new sixth form college (equivalent to senior high school in the United States) and began a new program of studies. During Session 7, Amy reported “hating” the new college; she reflected that she felt overwhelmed in the new situation and under stress from the additional demands on her time. After discussion, she recognized that there were some positives in the experience; she had begun to make new friends and was also starting a new part-time job. These new demands of working and friendships were explored in relation to her values, in particular the value of “looking after myself.” Amy’s mother voiced concerns that “Amy doesn’t have a life beyond work and school” but felt that this was something they were both conscious of and needed to address if it continued. Problem-solving was introduced as a concept, and the family was encouraged to use their problem-solving skills to think about possible solutions to Amy’s sense of being overwhelmed. Amy and her mother came up with a number of ideas, including Amy doing her homework in her free periods, asking for fewer hours at her part-time job, and texting friends to meet up.
Sessions 8 and 9: Continuing Progress and Relapse Prevention
The final sessions focused on consolidating the link between Amy’s activities and values and keeping a balance between necessary and optional activities. Amy successfully used problem-solving outside sessions to tackle difficulties with the workload at college. She discussed her problems with her teacher and suggested a solution (she asked for extra study support from school and discussed these plans with her mum). Amy’s mother identified that the combined demands of school and Amy’s job were difficult to manage. However, she felt that these concerns were typical of many teenagers in Amy’s position and felt that these difficulties were not related to Amy’s mental health.
In the final Brief BA session, Amy completed a relapse prevention plan (a “healthy me” worksheet). This included noting what she had learned, that is, the importance of putting myself first, do things for me, do things I enjoy, stay busy, look ahead. These were things she wanted to continue working on, along with taking her medication, attending college/work, and planning her university move. Amy identified that a potential trigger for relapse included losing people (in various ways, including friendship conflicts), and she identified a number of early warning signs for depression. These included skipping lessons, being quiet and withdrawn, and experiencing panic symptoms. Her plan of action when she noticed these signs was to speak to her tutor at college, do something constructive to keep herself busy like revising, and use modeling clay to relax. She identified her mother as someone who could help her keep well, confirming the therapist’s hypothesis that this relationship could be a useful source of reinforcement following the end of therapy.
8 Complicating Factors
Risk assessment and management with adolescents who are depressed must always be a routine part of any therapeutic work. Risk assessment can be introduced in simple ways. For example, in the case presented in this article, a question about suicidal thoughts was included at every session as part of the routine outcome measures, and the responses were discussed with Amy at each session. The simple question has now been included as routine practice in using Brief BA in our clinic. In managing risk, Brief BA therapists working with adolescents must also judge if, how, and when to share information about risk with parents or carers, in line with service and national guidelines. Regular clinical supervision is essential to support therapists appropriately to make these judgments and to minimize harm to the young person. The potential increase in parental attention via risk monitoring and management should also be considered as a possible reinforcer for more adaptive behavior (e.g., speaking about their low mood, rather than self-harming), along with recognition that parental responses vary and might not always be helpful for all young people.
Given Amy was on a stable, active dose of antidepressant medication at the start of Brief BA, it is possible that her improvements in symptoms and functioning could be at least partially attributable to medication rather than the psychological intervention. Indeed, from the family’s report, it is likely some positive impact had occurred by the start of Brief BA (e.g., increased motivation). It is not possible to separate out the effects of the medication and Brief BA in the current case study. However, the duration of a stable active dose prior to Brief BA, but plateau of improvement, does suggest Brief BA provided an additional therapeutic benefit. Further research is needed to examine the potential combined effects of Brief BA and antidepressant medication compared with either treatment alone in young people.
Similarly, the effect of the volunteering trip on Amy’s mood and functioning, in isolation to the Brief BA input, cannot be established. It is possible that this would have resulted in similar improvements on its own, although the likelihood of these being maintained is questionable. While the volunteering occurred prior to discussion of values and valued activities, this experience was explicitly drawn on throughout Brief BA to illustrate the benefits of engaging in valued activities, and how to schedule daily activities that fit with the same values.
Another complicating factor in this case was the prominence of Amy’s negative cognitions. These were pervasive and included her belief that “everyone leaves me,” which triggered her overdose. In early sessions, Amy often described negative thoughts that appeared to reflect a pervasive negative bias, and these would have been highly salient in CBT. However, in this Brief BA case, the therapist made no reference to Amy’s cognitions, and cognitive change was not measured. As therapy progressed and Amy’s mood and functioning improved, she spontaneously referred to cognitions that were less negatively biased; for example, she stated that volunteering made her “feel like a worthwhile person.” Thus, Amy’s cognitions related to self-evaluation appeared to change alongside, or even perhaps as a consequence of, her improved mood.
9 Access and Barriers to Care
There is increasing awareness that mental health problems are highly prevalent among young people, and their access to evidence-based mental health interventions and services is often deemed inadequate (Department of Health, 2015). Of particular concern is that a lack of prompt and effective treatment may exacerbate and amplify early difficulties and complicate future treatment. Developing brief, simple, clinical, and cost-effective interventions is one way of tackling problems with access. Brief BA is a highly focused and structured treatment for depression that requires less input from patients and therapists. In addition to involving fewer sessions than standard evidence-based psychological treatments (e.g., CBT), Brief BA can be delivered by staff who do not need extensive training or experience in psychological therapies or mental health (e.g., graduate psychologists with minimal training; Daughters et al., 2008). Given that most young people with emotional difficulties do not present to health care settings (e.g., Costello, He, Sampson, Kessler, & Merikangas, 2014), the potential benefits of offering a brief intervention for mild to moderate depression in community settings (e.g., schools) is of great potential benefit.
This case study adds to the emerging evidence base for Brief BA and demonstrates that it can be effective for a case of MDD with suicide risk. Risk management was integrated into standard Brief BA with good outcomes. Amy and her mother reported significant benefits and did not identify significant harm or adverse effects of Brief BA. However, the potential benefits of this protocol for adolescents with depression must be considered with some caution as there is not yet any formal randomized evaluation of treatment effectiveness or safety. Single case studies such as this can only provide provisional conclusions and highlight the need for larger scale, systematic comparisons of Brief BA with control or other active treatment groups.
10 Follow-Up
Amy and her mother returned for a review session after 6 weeks. At this review, Amy rated herself as 8/10 toward achieving her goal of being more confident and talking to people more, describing situations both at college and at work where she was interacting with others in a more confident manner. Amy described her mood as “alright” in general, despite having just had a bad day at college. She was able to reflect on the challenges of attending college and holding a very busy part-time job. She stated that at times it felt like “everything sucks,” but she was able to keep in mind that her college work “gets me to where I want to be.” She had decided what she wanted to study at university and was actively planning her applications. Amy reported that fatigue was still a problem but that she had started to pace herself more carefully. Promisingly, during the 6-week gap in therapist contact, Amy had maintained her gains from therapy, suggesting that therapeutic reinforcement was not a key driver in her improvement. Amy’s mother also stated that Amy’s mood had improved during therapy and that this had been maintained. She identified ongoing difficulties in Amy balancing work, college, and her social life but again reflected that these were concerns typical of many teenagers, and she was supporting Amy in finding a balance that worked for her.
At the review session, the family were also asked about their views on the Brief BA treatment using a feedback form. Amy reported “liking it” (range = “really liked it” to “hated it”), stated she found it “fairly” useful (range = “very” to “not at all”), and said she would “yes definitely” recommend Brief BA to a friend (range = “yes definitely” to “definitely not”). Amy’s mother also completed a feedback form, where she reported equally positive views on the treatment. She added additional comments about things she liked best about Brief BA, in which she stated “the activity planning element was really good with the importance of identifying activities that mean something to you.”
As part of routine care in the local CAMHS for all adolescents taking antidepressants, Amy and her mother attended a medication review with a team psychiatrist 2 months after she completed Brief BA. As she was now 17 years old, the Patient Health Questionnaire–9 items (PHQ-9; Kroenke, Spitzer, Williams, Monahan, & Löwe, 2007) was used to assess symptoms of depression. Amy scored 3/27 (nonclinical range). This included a score of 0 for suicidal ideation.
Progress and Outcome of Brief BA
Reliable and Clinically Significant Change
Amy’s symptoms of depression showed both reliable and clinically significant change on the RCADS Depression subscale competed by herself and by her mother (see Figure 2). Her scores moved from within the clinical range at assessment to a normal (i.e., nonclinical) range at the review session. Amy also showed reliable and clinically significant change on both self- and maternal-report of the ORS, moving from a clinical to normal range of functioning across the Brief BA treatment (see Figure 3).
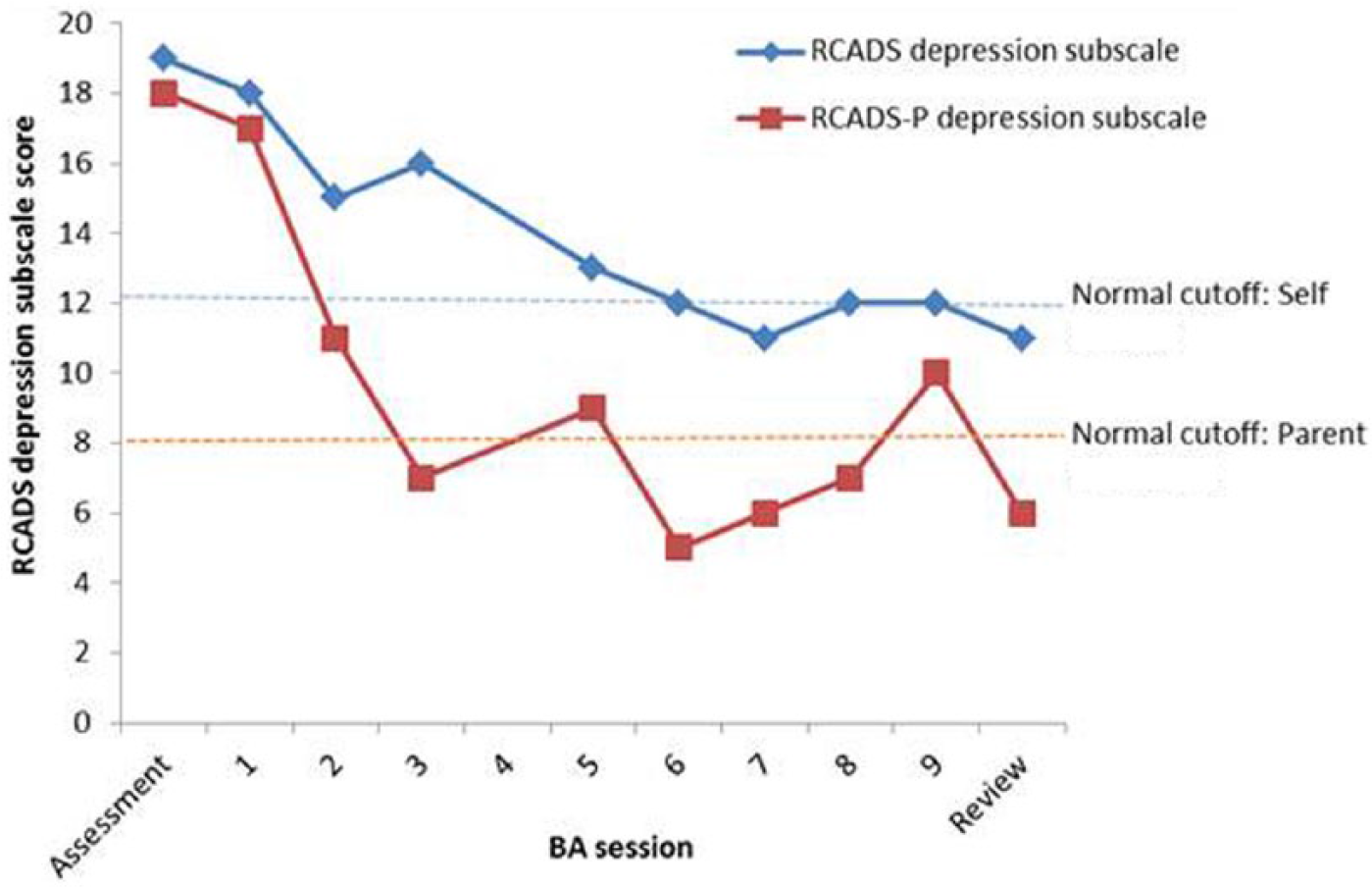
Self- and parent-reported depression symptom scores across Brief BA.

Self- and parent-reported functioning scores across Brief BA.
Amy and her mother completed the full RCADS again at the final Brief BA session. On this measure, Amy also showed a reliably and clinically significant decrease on the Separation Anxiety and Panic Disorder subscales, where she moved from the clinical range to the normal range on both self- and parent-report in the course of treatment. The other anxiety subscales remained in the normal range for the duration of Brief BA.
11 Treatment Implications of the Case
This case study illustrates how a structured program of brief BA for adolescent depression can be effective even when there are complicating factors, strong negative cognitions, and risk. Although only tentative conclusions can be made from a single case, the current article (in combination with the previous case reported: Pass et al., 2015) provides preliminary support for Brief BA with adolescents and indicates further evaluation is warranted. In particular, the role of parents in Brief BA as facilitators (as in the current case) or potential barriers (e.g., by not reinforcing the young person’s valued activities) would be of key interest in future research.
Given the high number of adolescents seeking treatment for depression and low mood (as well as the much greater population of nontreatment-seeking depressed adolescents), Brief BA could be a viable first-line intervention within a stepped care framework as has been introduced in adult psychological therapy services in the United Kingdom (Clark, 2011).
12 Recommendations to Clinicians and Students
It is essential that all clinical work with depressed young people involves careful and regular supervision, which maintains a focus on risk as well as treatment. In this case, supervision enabled detailed consideration of how to manage risk within a brief, structured intervention and how to maintain a fully behavioral focus in the context of explicit negative cognitive biases.
The concept of “flexibility within fidelity” (Kendall, Gosch, Furr, & Sood, 2008) was used in supervision and supported therapist self-reflection around this case. The balance of maintaining a focus on the client’s wishes and needs while offering a structured intervention was carefully considered. Due to the additional risk assessment and management session, Amy completed the Brief BA treatment over nine, rather than eight, sessions. This reflected the need to spend time with Amy and her mother on a risk management plan following her overdose. No additional content was included (e.g., cognitive restructuring of Amy’s catastrophic belief that “everyone leaves me”), but practical behavioral strategies were discussed as alternative actions in response to negative thoughts (e.g., speaking to new people in a college class).
Further research is needed to examine the acceptability, feasibility, and effectiveness of Brief BA with larger samples, and to investigate the mechanisms of change. Ideally, this should include clients who do not access traditional mental health services. Future work on alternative treatment delivery modes (e.g., at school, through Internet or mobile applications) is also warranted to explore the potential benefits of offering the intervention in ways that may be of particular relevance to adolescents.
Footnotes
Acknowledgements
The authors would like to thank Amy and her mother for their hard work through the Brief BA sessions, and for their consent to share their experiences of therapy. Thanks also are due to Professor Carl Lejuez for his comments on the Brief BA manual and approach, to Gemma Brisco who helped develop the Brief BA resources, and to the Child and Adolescent Mental Health Service that collaborated in this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Shirley Reynolds is supported by the Charlie Waller Memorial Trust.