
Abstract
Individuals with intellectual disability (ID) are at increased risk of presenting challenging behaviors and comorbid mental illness. Preliminary findings show decreased challenging behaviors and overall increased functioning in individuals with ID and mental health problems who receive adapted dialectical behavior therapy (DBT). However, more research and documentation on how to adapt DBT in this population is warranted given that DBT is a promising intervention in individuals with ID. This article presents the case of an individual with mild ID who received adapted DBT for the treatment of challenging behaviors, emotional dysregulation, and generalized anxiety disorder. Treatment lasted 1 year and was conducted in a residential facility for individuals with ID. Improvement of symptoms and decrease in frequency of challenging behaviors were observed throughout the case. This case study demonstrates the potential utility of adapted DBT for individuals with ID and underscores the importance of teaching skills to clients with ID to help them become agents of their own change.
Keywords
1 Theoretical and Research Basis for Treatment
For some individuals with intellectual disability (ID), the presence of challenging behavior is a significant concern (Fox, Holtz, & Barcelona, 2008; Grey, Pollard, McClean, MacAuley, & Hastings, 2010; McCarthy et al., 2010). It is estimated that more than 20% of these individuals engage in problematic behaviors (American Psychiatric Association [APA], 2013; Grey et al., 2010), such as aggression, self-injury, or emotional outbursts (Cooper et al., 2009; Crocker et al., 2006; Fox et al., 2008). These behaviors may result in significant impairment of the person’s functioning, disruptions in the environment, and lower individual and caregiver well-being (Cooper et al., 2009; Crocker et al., 2006; Grey et al., 2010). The function and intensity of the behavioral problems may vary depending on factors such as the severity of ID, environmental contingencies, and mental health issues (Crocker, Prokić, Morin, & Reyes, 2014; Poppes, Putten, Post, & Vlaskamp, 2016).
Deficits in emotion regulation, communication, and problem-solving skills contribute to challenging behavior among individuals with ID (Crnic, Hoffman, Gaze, & Edelbrock, 2004; McClure, Halpern, Wolper, & Donahue, 2009; Tyrer et al., 2006). Deficits in emotion regulation skills result in problems such as identifying emotions, coping with frustration, and tolerating emotional distress (Linehan, 2014). Thus, under emotional triggers, these individuals engage in maladaptive coping strategies to attempt to escape or attenuate the emotional response (Crnic et al., 2004). Cognitive impairment can also contribute to deficits in communication and problem-solving skills. Individuals with ID with communication skill deficits may engage in challenging behavior as a means to communicate personal needs or wants (Crnic et al., 2004).
In addition to the aforementioned skill deficits, individuals with ID are at increased risk of having mental health disorders (APA, 2013). It is estimated that the likelihood of experiencing psychiatric disorders is 2 to 4 times greater in people with ID than in people without ID (APA, 2013). Furthermore, 10% to 80% of individuals with ID who exhibit problematic behaviors also endorse symptoms suggestive of a mental illness (Crocker et al., 2014). When there is a comorbid mental illness, problematic behaviors may be more intense and less sensitive to standard interventions (Koch et al., 2015). For example, higher levels of mental health problems have been correlated with a higher likelihood of aggressive behavior in individuals with ID (Crocker et al., 2014). Along the same lines, emotional and cognitive deficits are associated with a higher prevalence of psychiatric problems among individuals with ID (Crocker et al., 2006; Tyrer et al., 2006).
A growing body of research suggests the effectiveness of adapted cognitive-behavioral interventions and mindfulness-based techniques for the treatment of mood disorders in individuals with mild and moderate ID (Brown, Brown, & Dibiasio, 2013; Dagnan, & Jahoda, 2006; Kozlowski, Mahan, & Matson, 2010; Lew, Matta, Tripp-tebo, & Watts, 2006; Pert et al., 2013; Robertson, 2011). Dialectical behavior therapy (DBT), for instance, is a promising psychotherapeutic intervention to target both challenging behaviors and mental illness (Brown et al., 2013; Lew et al., 2006; Robertson, 2011; Sakdalan, Shaw, & Collier, 2010). DBT was originally developed for the treatment of borderline personality disorder and has shown to be effective in a wide range of mental health problems (Glisenti & Strodl, 2012; Robins & Chapman, 2004). In the present study, we document the results of using DBT in an individual with mild ID and comorbid mental health problems. Prior to introducing the case, an overview of DBT premises and research findings in individuals with ID is presented.
DBT
DBT is a behavioral approach that incorporates skills training, contingency management, exposure, and cognitive restructuring (Linehan, 2014; Robins & Rosenthal, 2011). DBT is based in three different theories that guide treatment: biosocial theory, behavioral theory, and dialectal philosophy (Crowell, Beauchaine, & Linehan, 2009). According to the biosocial theory, emotional dysregulation is caused by the interaction of an invalidating environment and a biological predisposition for a heightened emotional sensitivity, greater emotional reactivity, and a slower return to emotional baseline (Crowell et al., 2009; Reeves, James, Pizzarello, & Taylor, 2010). This vulnerability may predispose an individual to use maladaptive strategies as attempts to attenuate aversive emotional experiences. In addition, behavioral theory states that beyond this biosocial vulnerability, behavioral problems are maintained by skill deficits, maladaptive environmental contingencies, and deficiencies in emotional processing and cognitive factors (Crowell et al., 2009). Finally, dialectical theory proposes that there is a set of communication strategies that the therapist can use to promote better treatment adherence and elicit change (Linehan, 2014; Robins & Rosenthal, 2011). These strategies are known as dialectics and involve the use of persuasion and validation to address conflicting worldviews and acknowledge the existence of opposite realities that are interconnected in the client.
DBT is a manualized intervention that has specific goals, techniques, and components. It is a multimodal treatment that involves individual therapy, group therapy, telephone coaching, and therapist consultation (Chapman, 2006; Linehan, 2014; Robins, & Rosenthal, 2011). Moreover, DBT is organized into targets, stages, and modules. The first target of treatment is to ensure client safety. The second target is to motivate the client to stay in therapy, and the third target involves fostering a “life worth living” (Linehan, 2014). The four modules of skill training are mindfulness, interpersonal effectiveness, emotion regulation, and distress tolerance (Linehan, 2014). The focus of the sessions and the order of the modules can be modified according to the client’s needs (Rizvi, Steffel, & Carson-Wong, 2013).
In individuals with ID, some studies have evidenced potential benefits in conducting DBT to reduce challenging behaviors and alleviate emotional problems. For instance, Brown et al. (2013) designed a longitudinal single-group pilot study in which individuals with intellectual deficits received DBT to treat challenging behaviors (e.g., aggression, self-injury, inappropriate sexual behaviors). They adapted standard DBT to meet the specific needs of individuals with IDs and monitored changes over 4 years of treatment. During this period, significant reductions in the frequency of challenging behaviors were observed. Interestingly, treatment was significantly more effective in reducing challenging behaviors in participants who were 20 years old than in participants who were aged 45 years. The authors called for more papers exploring age as a moderator of DBT treatment effectiveness in individuals with ID.
In another study by Lew et al. (2006), the authors describe how DBT was modified to their residential placement to treat challenging behaviors of individuals with mild to moderate ID also diagnosed with comorbid mental disorders such as depression and personality disorders. Overall, changes to the standard DBT were made to simplify material, activities, and language used in psychoeducation (see Lew et al., 2006). Lew et al. (2006) reported improvement of symptoms in a group of eight women that received modified DBT treatment. As in the Brown et al. (2013) study, DBT treatment appeared to produce a significant reduction in self-injurious behavior. In addition to this study, in a forensic setting, a pilot study of DBT in male offenders with mild and moderate IDs also suggested the potential benefit of using DBT treatment in this population. Specifically, after receiving DBT-adapted skills training, the majority of participants showed improvement in measures of global functioning and distress, coping skills, risk of offending, and clinical symptoms (Morrissey & Ingamells, 2011).
In summary, there is a growing body of research supporting the use of DBT and other mindfulness and acceptance-based therapies for the treatment of challenging behaviors and mental illness symptoms among individuals with ID (Lew et al., 2006; Pert et al., 2013; Robertson, 2011). The potential benefit of these interventions lies in the possibility of addressing mental health symptoms from a comprehensive evidenced-based treatment that combines individual and group psychotherapies, validation techniques, and behavioral interventions based on applied behavior analysis (ABA). Based on the promising results, increased efforts should be directed to validate adapted DBT in this population as well as to document guidelines, recommendations, and limitations on the intervention of DBT with individuals with ID across different settings of treatment (Baillie & Slater, 2014; Lew et al., 2006). Thus, the aim of this article is to present a case study of an individual diagnosed with mild ID who experienced challenging behaviors, emotional dysregulation, and generalized anxiety disorder (GAD) symptoms, and who received dialectical behavioral treatment. The case study illustrates how to adapt DBT in individual therapy to treat a cluster of symptoms in an individual with ID. Furthermore, the study highlights the potential relevance of integrating psychotherapy with standard ABA to treat challenging behaviors in individuals with mild ID.
2 Case Introduction
Gaby is 28-year-old single Caucasian female diagnosed with mild ID, GAD, and intermittent explosive disorder (IED). These diagnoses were given to her by the psychiatric committee of her current residential placement and were based on Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) criteria. Gaby had been living in a residential intermediate care facility for individuals with ID for approximately 10 years. She was referred to the first author for psychotherapy because her previous counselor moved to a different job. Moreover, at the time, Gaby was displaying increased intensity and frequency of challenging behaviors.
3 Presenting Complaints
Gaby exhibited challenging behaviors that kept her from advancing to a more integrated treatment setting. According to her history of symptoms as well as staff’s reports, four target behaviors disrupted her functioning: uncooperative behavior, aggression, self-injury, and elopement. Uncooperative behavior refers to times in which she refused to engage in programmatic tasks such as going to school, exercising, or taking her medicine. Often times, uncooperative behaviors were followed by other challenging behavior such as verbal aggression or elopement. In Gaby’s case, aggression was present in the form of verbal offenses and physical violence (e.g., kicking, hitting, biting, spitting, throwing things at others, and pulling hair). Usually, Gaby engaged first in verbal aggression that escalated into physical aggression. Her self-injurious behavior consisted of head-banging, skin picking, and attempts to asphyxiate herself. Most of the time, self-injury followed intense episodes of aggression to others. Finally, Gaby’s elopement refers to attempts to run away from the facility or her assigned area. This behavior was especially concerning, because when she eloped, she put herself in danger, and staff were unable to assist her, if needed. At the outset of therapy, Gaby reported distress associated with these challenging behaviors as well as motivation to change.
4 History
According to Gaby’s case history, behavioral problems have long been present in her life. The first reported incident of aggression was when she was in first grade, at which time, Gaby was placed in a self-contained classroom as her aggression was disrupting the typical classroom setting. Growing up, she required specialized educational contexts and close supervision. She reported that during her childhood, she was prescribed psychotropic medication for mood disorders. Her aggressive episodes became more intense during adolescence. She often was aggressive to the point that she was physically restrained, which sometimes resulted in encounters with the police. Before coming to her current placement, she had been in several psychiatric facilities and juvenile detention centers. Prior to her current placement, Gaby had a failed attempt to live in a group home due to extensive elopement and aggression.
At the outset of treatment, Gaby was receiving psychotropic medication, and a behavior modification program was in place to address her challenging behaviors. She was prescribed a mood stabilizer (Depakote, 250 mg), an antidepressant (Zoloft, 150 mg), and an antipsychotic (Seroquel XR, 500 mg). In terms of her behavioral program, Gaby was offered daily, weekly, and monthly reinforcement opportunities when she did not engage in any of the challenging behaviors targeted in her program (uncooperative behavior, aggression, self-injury, and elopement). In addition, staff prompted her in specific ways to redirect her when she was being uncooperative or when aggression was escalating. Gaby was asked to go to a quiet area when she exhibited signs of frustration and to relocate to an area away from others when she engaged in physical aggression. She was physically restrained when she eloped from the facility or when her aggression continued to escalate despite previous efforts to help her calm down.
5 Assessment
The assessment phase started with an extensive review of her case file, which contained her developmental history, background information, detailed description of presenting problems, as well as intervention procedures in place. A standard intake interview and a brief structured interview for differential diagnoses (The Mini-International Neuropsychiatric Interview [MINI]; Sheehan et al., 1998) were conducted, as well as a functional assessment of her challenging behaviors (Yoman, 2008). During the administration of the MINI, it was noticeable that Gaby had difficulties self-reflecting on her emotions and patterns of thinking. Some of these difficulties were likely to be associated with lack of awareness characteristic of individuals with mild ID and posed limitations to the use of self-report measures for psychiatric assessment. Nonetheless, the administration of this measure was useful as an examination of Gaby’s use of emotional language, insight, and level of self-appraisal. Based on Gaby’s responses to the MINI and behavioral observations, it was evident that Gaby was experiencing ongoing worry and anxiety symptoms consistent with GAD (e.g., fidgeting, hyperalertness, constant questioning about future situations, and worry about multiple areas of her life), as well as difficulties recognizing and monitoring her mood.
Results from the functional assessment suggested that Gaby’s challenging behaviors were associated with deficits regulating negative emotional states as well as implementing adaptive coping strategies to communicate distress. All the situations that preceded the challenging behaviors were those that appeared to elicit negative emotional states such as anxiety, sadness, anger, or frustration. Some examples of proximal and distal antecedents of her behavior were being denied going to the patio or playing her favorite game, returning from home visitations, and unexpected changes in her schedule. In terms of consequences, her challenging behaviors allowed her primarily to attenuate emotional pain, obtain staff’s attention, and communicate that she was under significant distress. Thus, these behaviors (uncooperative behavior, aggression, self-injury, and elopement) had the function of escaping from aversive emotions, obtaining attention from staff members, and communicating and validating her emotions (letting others know that her emotions were strong, important, and real). In the functional assessment of her behaviors, it was apparent that even though her behavioral program was designed to differentially reinforce appropriate behavior, the plan did not address deficits in emotional coping skills or include antecedent interventions to prevent escalation of problem behaviors. Moreover, the assessment indicated that her challenging behaviors co-occurred in time, and therefore, the occurrence of one challenging behavior signaled the occurrence of another challenging behavior (e.g., uncooperative behavior was an antecedent of physical aggression, and physical aggression was an antecedent of elopement, and elopement was an antecedent of self-injurious behavior). We concluded that in Gaby’s case, the intensification of her challenging behaviors represented escalation of distress.
In terms of her strengths, the intake interview and behavioral observations evidenced that Gaby had good verbal skills, valued learning, and was motivated to change. Regarding therapeutic goals, Gaby expressed that she wanted to be able to solve problems without engaging in her challenging behaviors. As a long-term goal, Gaby reported that she wanted to move to a group home.
6 Case Conceptualization
From the assessment data, it appeared that Gaby’s challenging behaviors were related to coping skill deficits in the area of emotional regulation. Gaby experienced problems down-regulating her emotions to provide adequate behavioral responses based on environmental demands. In addition, she struggled to identify and monitor her emotional states. This meant that she usually did not realize when she was upset, anxious, or sad, and the contextual or internal factors that were likely to be influencing her affect . As stated above, some of these difficulties were likely to be associated with limitations in her intellectual functioning, which hinder her self-awareness ability. Because it was difficult for Gaby to recognize when her emotions were intensifying, her physical discomfort was significantly stronger, and thus harder to regulate once she realized she was in distress. Therefore, whenever she experienced a negative emotion, she had difficulties implementing self-soothing strategies to calm down and provide an adaptive response. Furthermore, she perceived emotions as punishing and aversive.
Gaby’s emotional regulation deficits were further maintained by her learning history, contexts of invalidation, emotional avoidance strategies, and GAD symptoms. These variables interacted to reinforce the occurrence of challenging behaviors and keep her from learning healthy emotional regulation strategies.
In Gaby’s learning history, her maladaptive behaviors had allowed her to escape from aversive emotional states, as well as the contexts which elicited those emotions. Although these behaviors were associated with negative external consequences (e.g., loss of privileges, physical restraint), they permitted her to express distress and escape from immediate problems and physical discomforts. This immediate short-term relief increased her likelihood of using maladaptive strategies in the future. Apart from this, in her learning history, she had often experienced invalidation of emotions. Gaby’s normal emotional expressions were likely to be ignored or punished, whereas escalation of emotions was reinforced by others’ attention. Furthermore, reinforcement of escalation of behavior had maintained the presentation of challenging behaviors as an effective strategy to obtain attention.
Because in the past, Gaby had associated emotions with crisis, punishment, and disappointment, she felt guilty and anxious when she had an emotional reaction and engaged in constant efforts to avoid negative emotions (e.g., distracting herself when she was upset, pretending things did not bother her, failing to communicate distress; Hayes-Skelton, Roemer, & Orsillo, 2013). Emotional avoidance kept Gaby from learning new coping strategies and from delinking aversive stimuli from emotional reactions (Hayes-Skelton et al., 2013). Gaby’s emotional avoidance was manifested in ongoing efforts to “let go of things” and undermine her emotional experience. Whenever she had a problem, she tended to ignore what she was feeling and justify why she should not communicate unconformity or distress. This cycle further reinforced a learning history of inadequacy to down-regulate emotions and strengthen strategies to avoid emotions (Hayes-Skelton et al., 2013). Emotional avoidance may also have been inadvertently maintained by staff members who may have redirected, ignored, or invalidated Gaby’s signs of normal distress.
Finally, symptoms of GAD are likely to be associated with her deficits in regulating emotions and with her challenging behaviors as emotional coping strategies. Theories on the etiology and maintenance of GAD suggest difficulties in emotional regulation as a core causal factor of worry and somatic symptoms (Newman et al., 2011; Newman, Llera, Erickson, Przeworski, & Castonguay, 2013). Empirical findings have shown that individuals with GAD are likely to sense negative emotionality as more intense and stronger when compared with a normal population. In fact, in GAD, worry appears to be a coping strategy to generate sustained negative emotionality and avoid drastic emotional contrasts that are likely to lead to greater discomfort (Newman & Llera, 2011). These deficits in regulating emotions in individuals with GAD are suggested to lead to the occurrence of maladaptive strategies such as worry or other attempts to control emotional distress. In Gaby’s case, worry allowed her to cognitively anticipate potential aversive situations (e.g., My mom is not going to visit me) and feel emotionally prepared in case they occur. In addition, GAD symptoms (e.g., hyperalertness, difficulties sleeping, and constant tension) made it more difficult for Gaby to identify her emotions because she was already habituated to the physical symptoms of anxiety. Furthermore, her hyperalertness and worry made her more sensitive to interpret neutral cues in the environment as threatening, generating more situations that were upsetting to her. Therefore, Gaby’s GAD created a context where maladaptive challenging behaviors and difficulties in emotional awareness were more likely to occur.
Based on assessment data and case conceptualization, treatment targets were as follows: to decrease frequency and intensity of target behaviors and crises, to unchain challenging behaviors from one another and intervene promptly in antecedents that are likely to trigger a crisis, to increase emotional awareness and emotional regulation skills, to widen the repertoire of adaptive coping skills to challenge worry and increase distress tolerance, and, finally, to enhance acceptance of emotional experiences. The ultimate goal of treatment was for Gaby to increase her functioning so she would eventually to be able to live in a group home.
To meet these therapeutic goals, the treatment of choice was DBT. As mentioned before, this treatment is designed to address deficits in emotional regulation. Furthermore, DBT integrates ABA to target Gaby’s challenging behavior, skill training to address GAD symptoms and emotional regulation deficits, and validation techniques to reinforce her emotional expressivity and adherence to treatment. Moreover, DBT is a comprehensive treatment that provides guidelines to deal with crises in individuals like Gaby, who have exhibited intense behavioral problems and require a systematic, consistent, and long-term treatment.
7 Course of Treatment and Assessment of Progress
DBT treatment was implemented after the assessment phase (Linehan, 2014). Before starting treatment, agreements were established with Gaby (Linehan, 2014). These agreements emphasized Gaby’s and the therapist’s commitment to therapy, as well as Gaby’s agreement to attempt to decrease any behavior that could interfere with therapy or her safety (see Linehan, 2014). The treatment was structured to be administered in two weekly sessions: one for individual therapy and one for social skills training. The skills training was held individually and not in a group format because it was not feasible to do a DBT group skills training. Moreover, due to placement restrictions and Gaby’s behavioral program, telephone consultation with the therapist was not implemented. However, Gaby was allowed to communicate with her behavioral health specialist, or behavioral technician, and other staff members when needed. Gaby met with her behavioral technician weekly to review progress on her behavioral goals, and she was also allowed to call her when feeling distress. The treatment plan was coordinated with the behavioral technician to prompt and reinforce appropriate coping skills in Gaby. In addition to her therapy sessions, Gaby was asked to complete a weekly diary card for her challenging behaviors, establish a weekly behavioral goal that was challenging to her (e.g., go to school on Mondays), do a practice activity to rehearse skills (e.g., identify emotions 3 times a day), and complete a crisis log every time she engaged in any of her challenging behaviors. In her diary card, she had to indicate if the challenging behavior was present during the week by writing yes or no each day. She was able to complete her diary card without assistance. For some practice activities that required more advanced writing such as the crisis log, she requested the assistance of preferred staff members. Her weekly behavioral goal was established during the individual therapy.
Handouts and recording forms were adapted to contain more concrete images and simpler language to match her intellectual functioning. Similarly, all skills were taught through multiple experiential exercises (i.e., mindful walking, body scan, paying attention to her senses), illustrative examples, and role-playing. During treatment, sessions of skill training were briefer (approximately 45 min compared with the standard 2-hr sessions of DBT skill training), and less content was given during the session. Because Gaby had difficulties understanding abstract concepts, psychoeducation on the active factors of treatment was kept to the minimum, and practice activities were maximized during sessions. Staff members often helped her complete the homework, and Gaby was asked to monitor daily completion of the practice activities. To facilitate implementation of skills in crisis, a “tool box” was designed using a card board box that contained each of her learned skills. Initially, Gaby was requested to carry the “tool box” with her at all times to remind her of her skills. After carrying her tool box for approximately 2 weeks, a set of cards containing visual prompts of the coping skills was designed. These cards were not only practical and useful for Gaby, but they were also beneficial for staff members to remind Gaby to access the skills in challenging situations. This set of cards remained with her until the end of treatment. Finally, the therapist created a document for staff members detailing how to adequately prompt Gaby when she was signaling that something was wrong. This document included behaviors and antecedents that usually signaled the occurrence of Gaby’s challenging behaviors and difficulties regulating emotions, skills that Gaby learned in therapy, and strategies to validate her feelings and facilitate expression and recognition of emotions.
Treatment lasted 12 months. The first month was allocated to assessment, agreements, and building rapport. During the second and third months, mindfulness skills were introduced. Then, 3 months were spent in emotional regulation skills. Gaby had a break from therapy for 1 month during the winter holidays. Following the break, mindfulness skills were reinforced to address skill deficits in this area. Next, the interpersonal effectiveness module was implemented during the next 3 months, and finally, the distress tolerance module was delivered in the last 2 months of treatment.
Gaby’s hour of weekly individual therapy was allocated to attend to her specific needs or concerns and address crisis and occurrences of challenging behavior (Linehan, 2014). During this weekly hour, her diary card and her weekly goal were revised. If Gaby had engaged in any of her problematic behaviors during the previous week, behavioral chain analyses were conducted to identify the antecedents of the event and design a behavioral plan in which she could interrupt the chain of events and cope adequately (Linehan, 2014). A drawing of a chain was presented to Gaby to engage in chain of analysis. She was asked to narrate in details the situation surrounding her challenging behaviors and to explore what she was feeling in each of the antecedents of her challenging behavior. As she narrated what happened before she engaged in each challenging behavior, the therapist drew each situation in the corresponding chain link for her to be aware of the connection of the events, behaviors, and feelings. Together, the therapist and Gaby identified behaviors that could have prevented undesirable situations and challenging behaviors. Chain behavioral analyses were very useful in identifying treatment gaps as well as in increasing generalization of skills outside of therapy. For example, through chain behavioral analyses, it was identified that when Gaby did not go to school on Mondays after coming back from home visitation, she felt guilty for not going to school, had negative thoughts about her ability to cope with her situation, and eventually engaged in a challenging behavior. Not going to school after her home visitations was a situation that could be avoided to prevent a challenging behavior. Therefore, the behavior of not going to school on Monday was analyzed, and a detailed written behavioral plan to increase the likelihood of her attendance on Monday was developed. Gaby read the plan every Sunday night and Monday morning. This plan was very effective, and Gaby stopped having challenging behaviors as a result of not going to school on Mondays.
When she did not engage in any challenging behaviors, her use of appropriate coping skills during the previous week was reinforced during session by allowing her to choose the content of focus of the therapy session. In addition to this, during the individual session, breathing exercises and other skills which she was having problems practicing outside of therapy were practiced. Toward the end of the session, Gaby established her weekly goal (e.g., to obtain her daily rewards, to call her mother only 3 times a day, to do a puzzle) and was praised for her progress.
In summary, during the individual session, the therapist revised her diary card and weekly goal, conducted chain analyses if she engaged in a challenging behavior during the previous week, addressed personally relevant situations (e.g., being worried about a sick family member) and difficulties practicing a specific skill, and established her weekly goal related to a small, realistic, and feasible positive change that Gaby wanted to implement.
In the skills training sessions, Gaby and her therapist first reviewed the practice activity or homework which was directly related to the skill being learned, addressed any questions regarding previous skills learned, and then introduced a new skill (Linehan, 2014). During these sessions, Gaby’s challenging behaviors were not discussed unless they were pertinent for the topic of the class. As mentioned previously, the modules were implemented in this order: mindfulness, emotional regulation, interpersonal effectiveness, and distress tolerance (Linehan, 2014). The therapist decided to administer the modules in this order based on Gaby’s needs.
Mindfulness skills consisted of teaching Gaby to observe and describe her thoughts and physical sensations, be in the present moment, as well as to use her wise mind, a DBT term used to explain the balance between the emotional mind and the rational mind. The wise mind was taught using a pictorial item representing a heart as the emotional mind, the brain as the rational mind, and the combination of both as the wise mind. Several examples of the wise mind were provided and elicited from Gaby (e.g., a wise mind expresses his or her emotions to someone that they trust, a wise mind considers the situation before reacting). In terms of mindfulness practice, due to cognitive impairments associated with Gaby’s ID, teaching the mindfulness skills to Gaby was very challenging. Because she had difficulties observing and describing her private experience (e.g., thoughts and emotions), a bigger emphasis was allocated to the practice of concrete exercises of being aware of the present moment with her five senses and using her breathing as an anchor to the present moment. Gaby participated in a mindful eating activity using a raisin, engaged in mindful walks, and was frequently asked to observe her physical sensations and to describe her surroundings. Gaby was constantly reminded of her mindfulness skills as a prerequisite to identifying her emotions and noticing what was going on around her. It was easier for Gaby to first start practicing mindfulness by observing and describing things that were outside of her, and then translate these skills to observing and describing her private experience.
Emotional regulation skills were taught to increase understanding of emotions, enhance emotional identification and monitoring, and teach a variety of strategies to adequately deal with emotions and triggering events (e.g., problem solving, doing the opposite of the emotion, talking to someone, etc.). In this module, psychoeducation about emotions was reduced to the minimum to focus more on the practical implementation of the skills. Once again, given that Gaby had difficulties understanding abstract concepts and reflecting on her emotions, this module was adapted using visual and concrete prompts that Gaby could associate with escalation of emotions and systematic steps on how to identify her emotional state. For instance, Gaby and her therapist designed an emotional thermometer in which a pictorial prompt of a thermometer is used as a metaphor to help differentiate levels of emotional arousal. This thermometer was visually available in her room and indicated three emotional zones (green, yellow, and red). The therapist and Gaby indicated cues that were likely to signal escalation of negative emotions and maladaptive behavior as well as specific healthy coping strategies for each zone of the thermometer. Gaby used this thermometer as a frame of reference to identify her emotions. In another activity in this module, Gaby generated a list of positive activities and daily positive practices to reduce her vulnerability to distress. For homework, she frequently engaged in these positive activities. A module of cognitive reappraisal was included in the emotional regulation module to address Gaby’s ongoing worry and worry-driven behavior (e.g., calling her mother multiple times, asking the same question to staff members throughout the day). To teach the skill related with cognitive reappraisal, Gaby had a card with a list of three questions and pictures that she would ask herself when getting stuck in challenging situations: (a) What are my thoughts about the situation? (b) How can I find out if what I am thinking is true? and (c) What are some other ways of thinking about the situation?. This particular skill was hard for Gaby to grasp because she had difficulties engaging in metacognition. Due to these cognitive deficits, Gaby was not able to implement appropriately this skill on her own, but instead she needed another person to help her navigate through these questions. However, she was able to use these questions as a prompt to approach the situation differently and to use the assistance of preferred staff members to engage in cognitive reappraisal.
Interpersonal effectiveness referred to skills targeted to increase Gaby’s adequate communication of distress, recognize her wants and needs, and identify appropriate ways of expressing emotions and opinions. Gaby’s main problem was associated with not being able to express her feelings and wants in an appropriate and timely manner. In this module, therefore, we focused primarily on implementing the DEAR MAN skills (describe, express, assert, reinforce, mindful, appear confident, and negotiate) to express emotions and requests effectively. The term reinforce was replaced by rewards, and the term mindful was replaced by manners as Gaby was more familiar with these terms. DEAR MAN skills were taught by using situations previously experienced by the client as examples (e.g., How to tell her teacher that she wants to engage in another activity), modeling of the DEAR MAN skill, role-playing of several situations, and shaping of the skill providing immediate feedback and constant repetition. Moreover, for homework, Gaby practiced DEAR MAN with staff members and behavioral technicians. Gaby did not learn the other acronyms of the DBT module of interpersonal effectiveness, as it was difficult for her to retain so much information. Moreover, the DEAR MAN was judged to encompass the skills that Gaby needed. During this module, Gaby also learned other communication skills to carry on appropriate conversations (e.g., active listening, giving compliments, asking for clarification, and maintaining a conversation) to facilitate positive interactions with peers and staff members.
Finally, distress tolerance consisted of introducing skills for crisis survival to deescalate emotions and promote acceptance of uncontrollable events (see Linehan, 2014). To teach these skills, during session, Gaby practiced different activities to promote relaxation and self-soothing (e.g., half-smiling, deep breathing). Moreover, Gaby created a survival kit containing things that could calm her down when she was upset. Her emergency kit consisted of a box titled survival kit with a picture of her family, the Bible, and her favorite CD. During skill training sessions, she practiced imaginal relaxation techniques such as visualizing herself at the beach (her relaxing place) or in her favorite room at home. She also wrote a short prayer to be used when she was having a difficult time coping with situations. The DBT skills of radical acceptance and willingness were taught using the terms of acceptance and change. Gaby practiced acceptance through mindfulness and constant expression of her emotions. Furthermore, Gaby learned to focus on her short-term goals and skills instead of focusing on the situations that she could not change (i.e., she was taught to ask herself “is this something I can change?” and to look through her cards to identify a skill that she could use to make the situation better).
In summary, the skills training sessions were adapted to fulfill Gaby’s level of cognitive functioning and needs, while reducing the content of DBT theory associated with each skill, teaching skills relevant to her needs, and increasing the visual prompts, practical activities, repetition, and examples associated with each skill. During the sessions, Gaby was constantly asked to indicate her understanding of the skill and to give examples of the concepts using her own words.
Assessment of Progress
Progress was tracked through frequency of challenging behaviors before and after treatment. Administration of self-report measures was not feasible because Gaby’s reading skills were limited and the administration of self-report measures was time-consuming. Moreover, the frequency of her challenging behaviors was considered a more direct measure of goal progress. Baseline was obtained by counting the frequency of inappropriate behavior reports documented in her records for the target behaviors over the course of 3 months before treatment. During treatment, challenging behaviors were monitored weekly. Figure 1 displays the frequency of challenging behaviors 3 months before starting treatment and during treatment course.
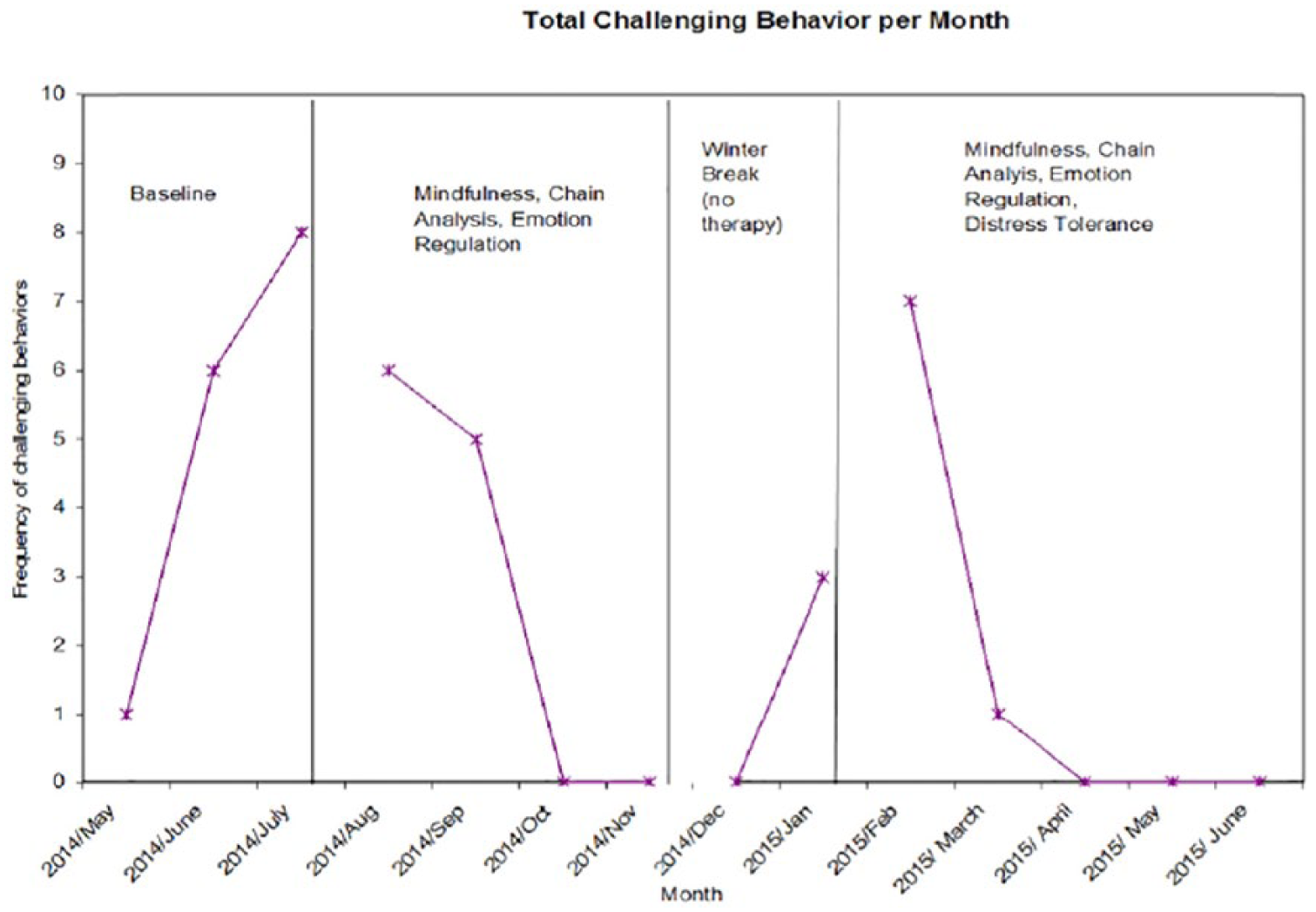
Frequency of challenging behaviors.
As indicated in Figure 1, before treatment, Gaby’s challenging behaviors appeared to be increasing. Assessment was conducted in July and was followed by preagreements and introduction of the mindfulness module. In August, the frequency of all of the challenging behaviors started to decrease. After 1½ months of mindfulness and chain behavioral analyses, the frequency of challenging behaviors reached a zero frequency. During the administration of the emotional regulation module, which lasted 2½ months, Gaby maintained a zero frequency of challenging behavior. During winter break, she did not receive psychotherapy for a month, and she went home to spend approximately 2 weeks with her family for Christmas and New Year’s Eve. Based on previous records and staff report, Gaby always struggled returning to the residential community after the holidays because she had to readjust to the routine, the rules, and she missed her family. After the break from psychotherapy, a couple of days after she returned from home, she reengaged in all of her behaviors (but self-injury) in January. In February, the death of a close friend triggered reappearance of challenging behaviors. When she reengaged in her challenging behaviors in January, mindfulness skills were reintroduced to remind Gaby of the importance of noticing her reactions in the present moment, and chain analysis was conducted to address the contextual factors of her current crises. The module of interpersonal effectiveness was introduced in February (for 3 months) followed by the module of distress tolerance (for 2 months). After the last episode in February, most of her challenging behaviors returned to a frequency of zero. However, she engaged in one uncooperative behavior during March. Gaby maintained a frequency of zero challenging behaviors during the rest of treatment, which ended in June. It is worth noting that during January and February, the intensity and duration of the episodes of challenging behaviors decreased significantly when compared with past episodes.
Progress was also monitored by staff members’ qualitative reports as well as the therapist’s behavioral observations. Staff members indicated improvement of mood and the use of better strategies to deal with problems. Moreover, they reported instances in which Gaby was able to down-regulate emotions using her “tool box” and adequately communicate distress. In addition, because her behavior health specialist recognized the usefulness of treatment, DBT prompting procedures were included in her behavioral program for staff members to intervene when she was signaling escalation of emotions. Some staff members also reported that they used Gaby’s card set of skills to remind her to engage in appropriate behavior when she evidenced escalation of distress. Finally, throughout the course of treatment, the therapist observed improvement in emotional awareness, problem-solving skills, and confidence when dealing with crises. These improvements were also reported by Gaby.
8 Complicating Factors
There were several factors that complicated the implementation of treatment. Some of the limitations were related to Gaby’s significant difficulties recognizing physical symptoms and thoughts associated with distress. Due to these pervasive deficits, it was often difficult for Gaby to practice skills and reflect on her rumination pattern when she was engaging in maladaptive thoughts. These deficits are likely to be accounted for by decreased insights and abstract thinking skills associated with cognitive impairment. Other limitations were related to placement restrictions and difficulties including staff members in treatment. Although the therapist provided instructions for staff on how to adequately prompt Gaby in the presence of cues signaling escalation of distress, the training was not comprehensive due to time and availability restrictions. Along the same lines, environmental contingencies of invalidation and reinforcement of escalation of behavior were difficult to change. Staff members and family members close to Gaby may have exhibited fear when addressing Gaby’s normal emotional expressions and as a result may have avoided dealing with problems when needed. In addition, inconsistency of adequate prompting strategies among staff was an obstacle in the generalization of skills outside of therapy.
9 Access and Barriers to Care
Gaby’s residential placement included access to appropriate care. Gaby received frequent medical and psychiatric checkups. Side effects of medications were monitored by her behavior health specialist, who was also in charge of revising her goals and behavioral plan. Although the behavioral technician did not directly participate in the implementation of the treatment, she was fundamental in communicating to the therapist any update on Gaby’s emotional and behavioral status as well as on motivating Gaby to use her skills. Moreover, her individual support program involved daily exercise and a healthy diet. Psychotherapeutic treatment was supervised by a PhD clinician, and peer-consultations were conducted to guarantee adequate care. In terms of her family, Gaby’s family was a reliable source of support and a significant factor of motivation for Gaby’s change. In terms of barriers to care, given that Gaby’s cognitive functioning was significantly higher than other peers, she had limited opportunities to engage in social interactions with same level of functioning peers.
10 Follow-Up
The therapist’s work contract consisted of a 1-year practicum training, and thus, treatment had the same length of duration. By the end of the therapist’s year of practicum training, treatment was discontinued and Gaby was referred to the next graduate intern. It was suggested for Gaby to continue with DBT treatment of individual therapy, skill training, goal setting, and monitoring of challenging behaviors. Future treatment goals were to maintain change, strengthen coping skills, and prepare Gaby to live in a group home. Presently, Gaby is scheduled to go to a group home in the near future and has maintained an average of less than one challenging behavior per month during the year following termination of treatment by the graduate therapist.
11 Treatment Implications of the Case
This case has important implications for the treatment of mental illness and associated problem behaviors among individuals with IDs. Specifically, the present case strengthens the increased body of findings suggesting DBT as an effective treatment of mental health symptoms in a population that is commonly underrepresented in the literature. As it was mentioned above, in individuals with ID, there are a variety of limitations related to mental health treatment. Thus, it is pivotal to find appropriate interventions suitable to the needs of these individuals. The importance of DBT consists of its inclusion of ABA, skills training, and validation techniques to target a variety of challenging behaviors and mental health symptoms. DBT focuses on basic skill deficits that are likely to be present in individuals with ID and mental health symptoms. Moreover, it promotes an environment of validation and encouragement for these individuals.
This study also demonstrated that DBT is a treatment that can be adapted to a variety of settings and individual characteristics. The manual does a very good job addressing the fundamentals and general guidelines of treatment to train the clinician to react appropriately in a variety of situations. Moreover, in her manual, Marsha Linehan (2014) stated that DBT can be targeted to specific skill deficits, and the modules can be substituted for more appropriate ones, if needed. This flexibility of treatment structure and creativity in treatment implementation appear to be of great benefit in adapting DBT to meet the needs of individuals with ID. In this case, DBT material was effectively adapted to facilitate understanding of material. Furthermore, although the format of treatment had to be altered to individual skills training instead of group skills training, treatment was still possible and effective in reducing challenging behaviors.
Finally, the case study highlights the potential benefits of psychotherapy for individuals with mild to moderate ID. In these individuals, ABA is the standard method of treatment. This method emphasizes modification of contextual contingencies to decrease challenging behaviors. Although ABA is effective, clients might also benefit from individual psychotherapy to provide an environment in which they can voice their concerns and enhance their personal ability to respond to demands. This is particularly important in individuals with comorbid mental illness. In Gaby’s case, individual psychotherapy gave her a sense of control over her challenging behaviors as well as confidence in her capacity to change. The combination of skill training and psychotherapy in these individuals might increase treatment adherence and motivation to change.
12 Recommendations to Clinicians and Students
When working with individuals with ID, a comprehensive assessment of symptoms and challenging behaviors is recommended (Taube-Schiff & Serbin, 2006). To effectively implement treatment, the presence or absence of mental illness and the function of challenging behaviors need to be determined. Because mental health disorders are often misdiagnosed in individuals with ID, it is important to obtain relevant data from different sources, including the client’s report and empirically validated diagnostic tools for this population. Furthermore, a functional assessment and the identification of the client’s strengths and abilities are vital to select treatment. Based on data gathered in the assessment phase, the most parsimonious treatment should be selected. Self-report measures to be answered by caregivers and staff members are important to assess treatment outcome. This enhances the validity of the treatment and better informs the clinician on client progress.
Including people that interact daily with clients is likely to enhance treatment outcome. It is important to incorporate a staff or parent training component on psychoeducation about the skills and appropriate prompting to facilitate implementation of skills. This will potentially enhance generalization of skills across several settings and situations. A multidisciplinary approach to treatment is also recommended. This includes communication with the psychiatrists, behavioral technicians, and other health care providers involved. This was also a limitation of the present case study, and should be addressed in future cases. Last but not least, when initiating treatment with individuals with mild and moderate ID, clinicians should not disregard their clients’ ability to establish and monitor their own goals. When working with individuals with ID, clinicians should focus on their clients’ strengths, and accordingly foster a sense of agency and empowerment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.