
Abstract
Acceptance and Commitment Therapy (ACT) is a third-wave behavioral therapy that is an empirically supported treatment for various mental health concerns. ACT has been found to be efficacious for treating different types of anxiety disorders. This case study presents the conceptualization (functional analysis), treatment (ACT), and treatment outcomes of a client who presented with emetophobia, a phobia of vomiting, complicated by a metabolic disorder. Measures of emetophobia symptoms, mindfulness, cognitive fusion, thought control strategies, and believability of anxious thoughts and feelings, were collected at pretreatment, posttreatment, 6-month follow-up, and 12-month follow-up. The Reliable Change Index was used to evaluate changes across time. Large and clinically significant decreases on all measures were observed at posttreatment. At 12-month follow-up, improvements were maintained on all measures except the Reappraisal subscale of the Thought Control scale. The implications of this study are discussed, and recommendations are made for clinicians using ACT for the treatment of emetophobia.
Keywords
1 Theoretical and Research Basis for Treatment
Emetophobia is the specific phobia of vomiting. This disorder is characterized by an extreme fear of vomiting, seeing others vomit, or being judged by others if vomiting were to occur (Lipsitz, Fyer, Paterniti, & Klein, 2001). Persons with emetophobia frequently avoid situations that may increase their perceived risk of vomiting or being exposed to vomit, such as eating certain foods or interacting with people who are sick (Veale & Lambrou, 2006). Emetophobia has a mean age of onset during early adolescence (Lipsitz et al., 2001). As is the case with most phobias, emetophobia can cause significant social impairment (Veale & Lambrou, 2006).
Emetophobia is estimated to affect between 2% and 7% of the population, with the majority of those diagnosed being women (Philips, 1985). Development of emetophobia is often attributed to a traumatic vomiting event during childhood or early adolescence, and the course of this phobia seems to be chronic if no intervention is provided (Lipsitz et al., 2001). One factor that differentiates emetophobia from other specific phobias is that persons with this disorder have been shown to have a heightened sensitivity to interoceptive cues, meaning that they are more aware of physical feelings from inside their bodies and are more likely to interpret them negatively (Boschen, 2007). Furthermore, emetophobia can at times promote unhealthy weight loss (Veale, Costa, Murphy, & Ellison, 2012).
Phobias are commonly treated with cognitive-behavioral therapy. This study used Acceptance and Commitment Therapy (ACT) as an alternative approach (Hayes, Strosahl, & Wilson, 2016). ACT focuses on six core processes to promote improvement in functioning: acceptance, cognitive defusion, self-as-context, present moment awareness, values, and committed action.
Acceptance is described as a willingness to be in the presence of distressing cognitive and emotional experiences without engaging in avoidance or escape behaviors. This is an important departure from traditional cognitive therapy approaches that encourage attempts at controlling distressing thoughts and feelings via techniques, such as thought stopping, rehearsing positive alternative thoughts, cognitive restructuring, and identifying and disputing distressing thoughts (Dobson & Dobson, 2016).
Cognitive defusion is a strategy used to dispassionately view cognitive and emotional experiences from a third-person perspective sometimes referred to as the “observer self.” Two important ACT processes needed for successful cognitive defusion are present moment awareness and self-as-context. Present moment awareness includes attending to the present moment and immediate experiences without ruminating on the past or worrying about the future. Self-as-context involves recognizing that thoughts and feelings are context-specific and separate from the observer self.
Adding to acceptance and diffusion is values clarification. Here, clients are encouraged to identify important life values that then guide committed action and behavioral pursuit of important aspirational life objectives as opposed to avoidance of distress (Hayes et al., 2016).
A desired outcome in ACT is the acquisition and maintenance of committed actions that are congruent with important life values regardless of variation in unwanted or distressing thoughts and feelings (e.g., Berghoff, Forsyth, Ritzert, & Sheppard, 2014). As such, ACT is aligned with radical behaviorism and functional contextualism (Hayes, Levin, Plumb-Vilardaga, Villatte, & Pistorello, 2013).
As emetophobia is relatively unique in its expression and course, single-subject designs have most often been used to study treatment outcomes (Maack, Deacon, & Zhao, 2013). Previous case studies used combinations of cognitive-behavioral therapy (Graziano, Callueng, & Geffken, 2010), exposure therapy (Hunter & Antony, 2009; Maack et al., 2013; Moran & O’Brien, 2005; Williams, Field, Riegel, & Paul, 2011), and pharmacological intervention (Faye, Gawande, Tadke, Kirpekar, & Bhave, 2013; Fix, Proctor, & Gray, 2016). In addition, most case studies (Faye et al., 2013; Fix et al., 2016; Graziano et al., 2010; Williams et al., 2011) summarized treatments for children or adolescents. These case studies have provided preliminary evidence that traditional cognitive-behavioral therapy can be effective for emetophobia. However, other more recently developed types of behavioral therapy such as ACT have not yet been evaluated.
There is, to date, no manualized treatment of emetophobia, and no randomized-controlled trial studies for the disorder have been published. Although ACT has not previously been used as treatment for emetophobia, ACT has been used successfully for anxiety-related disorders (Bluett, Homan, Morrison, Levin, & Twohig, 2014; Ruiz, 2012). ACT has also been demonstrated to be effective for addressing psychosomatic problems, including health-related anxiety (Eilenberg, Kronstrand, Fink, & Frostholm, 2013). Given that the presentation of emetophobia can include hypervigilance and oversensitivity to interoceptive cues (Boschen, 2007), ACT may be uniquely suited to treat emetophobia. As noted above, two of the core concepts of ACT are acceptance and defusion, which are designed to bring about an awareness that many everyday experiences, including distressing sensory experiences, cannot be volitionally controlled and will vary across contexts and time. Therefore, in emetophobia, an important goal of acceptance and defusion is to help the client discontinue the use of a limited, rigid, and unworkable set of cognitive and behavioral control strategies (i.e., repetitive escape and avoidance behaviors) designed to provide temporary relief from distressing sensory experiences. Instead, clients learn to pursue important longer range values-based life goals using a wide array of behaviors in the presence of distressing sensory experiences. As such, the emphasis is on changing the relationship between distressing sensory experiences and behavior. That is, the client learns that he or she can engage in many important, long-range, values-based behaviors while experiencing distressing sensory experiences. This important skill is referred to as “psychological flexibility” in the ACT literature.
Single-subject and case study designs have important and unique features that allow for the examination of unusual symptoms as well as in-depth examination and analysis of behavior problems and interventions. They also allow for iterative modifications of treatment plans in light of ongoing assessment of client behavior across time. Therefore, it is useful to implement a theoretically supported intervention in a single-subject design to evaluate specific, individualized changes in quality of life and symptomology. Single-subject design studies also allow for in-depth functional analyses of client behavior.
Like case studies, individualized functional analyses also have important and unique features. First, they allow for the collection of individualized data for specific target behaviors in specific contexts (Haynes, O’Brien, & Kaholokula, 2011). For example, a functional analysis of an emetophobia client can include thoughts, feelings, and behaviors surrounding the idea of “eating,” and knowing those thoughts, feelings, and behaviors can help in treatment planning. Second, individualized functional analyses allow for the determination of interrelationships among variables (Haynes et al., 2011). These determinations can then inform treatment and permit an intervention that is specifically tailored to the client and the problems that the client is facing (Haynes et al., 2011).
In this study, we provide an illustration of how functional analysis methods and ACT can be combined to generate an individualized in-case conceptualization. This case conceptualization was used to design an ACT intervention for a client presenting with emetophobia complicated by a metabolic disorder. Finally, we discuss ACT intervention outcomes and processes in highlighting how the intervention differs from conventional cognitive-behavioral therapy for emetophobia.
2 Case Introduction
“David,” a late-adolescent Caucasian male, sought treatment for an extreme fear of vomiting, anxiety, and panic symptoms. (Note: Details of “David’s” identity have been altered to maintain confidentiality and anonymity in this report.) He was previously treated with exposure therapy for similar concerns when he was a preadolescent child. His symptoms had been in remission until February of David’s senior year of high school.
David’s symptoms of emetophobia made life especially difficult, as he was preparing to transition from high school to college and becoming an independent adult. Other important factors present at the time of intake were social anxiety, a limited social network, and a chronic metabolic disorder that required careful dietary management.
3 Presenting Complaints
A functional analysis was conducted to examine the topography of behavioral, physiological/affective, and cognitive variables, and their relationship to each other (Haynes et al., 2011). David’s main concern was intense anxiety resulting from a fear of vomiting. He reported that he would experience ambiguous physical sensations, such as stomach pains or nausea which would then prompt fears that he might vomit. His fear became increasingly intense, and he reported daily worry about vomiting. David reported that he engaged in extensive and frequent (several times per day) self-monitoring of bodily sensations for clues as to whether or not he would vomit. In addition, he would frequently seek reassurance from his parents by explaining his symptoms to them and asking repeatedly for their opinions about whether he was sick and whether he might vomit. This reassurance-seeking was reportedly harming his relationship with his parents because talk about symptoms dominated conversations with them. Furthermore, David sometimes woke his parents in the middle of the night to talk about his symptoms. At other times, he would search online medical websites to determine whether his symptoms were related to various medical conditions. When he was seeking online information, David’s anxiety sometimes increased to the point of panic attacks. These panic attacks were manifested in nausea, racing heart, sweaty palms, shortness of breath, and chest tightness. At the beginning of therapy, these panic attacks were occurring on a daily basis, and he reported they were intensely distressing. David reported that he had been evaluated by physicians who had ruled out gastrointestinal medical conditions. One physician also prescribed an antianxiety medication, but David reported he was hesitant to use them.
A related behavioral variable of interest was significant social anxiety and social isolation. David reported that he tended to avoid social interaction with others. He noted that he did not have close friends and that his anxiety prevented him from talking with others at school. He reported that when he was younger he had more friends, but, when he was older, he found that making friends was more difficult.
4 History
David grew up as the second of four children, with both parents in the home. At the age of 6 years, he was diagnosed with a medical condition that needed careful dietary management and close parental monitoring. He reported that he was homeschooled until about the age of 10 years so that his parents could closely monitor his health. When he was older and able to manage his health more independently, he returned to school.
David arrived to therapy during a time of significant transition. He was anticipating high school graduation which meant leaving a social environment that was familiar to him. He was also being encouraged by his parents to be more independent and to seek work until he began college studies. His parents were closely involved in the management of his health. He was in the process of accepting an offer of admission to college at the beginning of this treatment.
5 Assessment
Multiple methods of assessment were conducted to develop a case conceptualization, including clinical interviews, information gathered from David’s thought log, and measures of emetophobia symptoms, mindfulness, thought control strategies, cognitive fusion, and believability of anxious feelings and thoughts. This information was then integrated into a functional analytic case conceptualization (FACC; Haynes et al., 2011). The FACC included information about the topography of behavior problems, including causal variables that were situational, interpersonal, and intraindividual (i.e., thoughts, emotional states, and physiological states) in nature. The FACC also included variables that reinforced problem behaviors, as well as mediator and moderator variables.
Clinical interviewing was the assessment method used during the first two sessions. David also recorded his experiences using a daily diary in which he recorded the place and time, thoughts, emotions, physical sensations, and triggering events associated with emetophobia anxiety and panic. David was very compliant with this homework, and his diary revealed that he was insightful and attentive to his cognitive experiences. Questionnaires were completed at three time points: at the end of Week 2 as part of the diagnostic assessment (baseline), at 16 weeks (the conclusion of treatment), at 6-month follow-up, and at 12-month follow-up.
Measures
Emetophobia symptoms
The Emetophobia Questionnaire (EmetQ-13; Boschen, Veale, Ellison, & Reddell, 2013) is a 13-item questionnaire in which David rated severity of fear of vomiting over the past week. Among a sample of 95 individuals with emetophobia, the Emet-Q was reported to have high internal consistency (α = .82) and a 1-week test–retest reliability coefficient of .76 (Boschen et al., 2013).
Mindfulness
The Five-Facet Mindfulness Questionnaire–Short Form (FFMQ-SF; Bohlmeijer, ten Klooster, Fledderus, Veehof, & Baer, 2011) is a 24-item questionnaire measuring mindfulness in everyday life (i.e., trait mindfulness) using items that reflected everyday experiences. The FFMQ-SF has five subscales, including Observe, Describe, Nonjudge, Nonreact, and Act With Awareness. Using a sample of 376 adults with mild-to-moderate depressive or anxiety symptoms, Bohlmeijer et al. (2011) reported that the internal reliability for each of the five subscales ranged from .73 to .91 (Bohlmeijer et al., 2011).
Cognitive fusion
The Cognitive Fusion Questionnaire (CFQ; Gillanders et al., 2014) is a seven-item measure that assesses fusion to thoughts, or believing thoughts to be literally true. Gillanders et al. (2014) evaluated the psychometric properties of the CFQ with a sample of 1,040 young-adult college students and community members. They reported that the internal consistency was high (α = .90) and that the 4-week test–retest reliability coefficient was .80.
Thought control
The Thought Control Questionnaire (TCQ; Wells & Davies, 1994) is a 30-item measure that evaluates the degree to which various methods (e.g., Distraction, Social Control) are used to control thoughts. It contains five subscales, including Distraction, Punishment, Reappraisal, Worry, and Social Control. Using data from 229 college students, Wells and Davies (1994) reported that the internal consistency of the subscales ranged from .64 to .79. Furthermore, the test–retest reliability coefficient of the subscales ranged from .68 to .83 across a 6-week interval with the test–retest reliability coefficient for the total score being .83 (Wells & Davies, 1994).
Believability of anxious feelings and thoughts
The Believability of Anxious Feelings and Thoughts Questionnaire (BAFT; Herzberg et al., 2012) is a 16-item measure that assesses how much a person believes his or her anxious feelings and thoughts to be literally true. Among a sample of 503 highly anxious community members, Herzberg et al. (2012) reported that the scale had high internal reliability (α = .91) and a 12-week test–retest reliability coefficient of .77.
6 Case Conceptualization
A Functional Analytic Case Diagram (FACD; Figure 1) was developed after integrating information gathered from the clinical interview, client thought log, and questionnaires. First, it is comprised of three main classes of variables: unmodifiable causal variables, modifiable causal variables, and target behaviors (cognitive, affective, and behavioral responses). Second, it depicts information about target behavior–target behavior relationships and casual variable–target behavior relationships. These relationships can then be organized into sequences of events that can help explain David’s experiences. Finally, an examination of the causal model can point to intervention targets. Specifically, variables that (a) are modifiable and (b) have the most critical links to target behaviors can be prioritized in an intervention design.

Functional analytic conceptualization diagram of a client presenting with emetophobia.
Target behaviors that were identified in the functional analysis were physical symptoms associated with fear (e.g., nausea or restlessness), catastrophic thinking, preoccupation with vomiting, reassurance-seeking, and escape. David reported that the interactions among cognitive and physiological experiences could escalate to the point of panic attacks. Finally, David reported that he was socially isolated and experiencing moderate levels of depressed mood.
Three primary causal variables were identified. One was eating. Specifically, mealtimes triggered gastrointestinal sensations and a fear of choking. Second, being alone at nighttime was a significant causal variable because David reported that he would tend to ruminate about his sensations and the possibility of vomiting during that time. Finally, social reinforcement for reassurance-seeking was identified as an important causal variable.
The FACD suggests the following sequence. Upon sitting down for a meal, David would experience catastrophic thoughts about the possibility of vomiting. These thoughts, in turn, would promote sympathetic activation marked by a number of sensations including gastrointestinal distress. The sympathetic activation, in turn, amplified catastrophic thinking in a reciprocal manner. The combination of catastrophic thinking and sympathetic activation would prompt David to engage in a number of self-scanning and self-checking behaviors, such as hypervigilance to stomach sensations. These checking behaviors provided momentary relief, but this relief was not sustained and had limited impact on catastrophic thoughts and sympathetic activation. Thus, David would tend to proceed to two additional behaviors: escape and/or reassurance-seeking. Reassurance-seeking and escape behaviors provided relief from anxiety and were thus acting as negative reinforcers.
As a result, David’s methods of controlling or avoiding his fear of vomiting resulted in an inability to engage in various activities consistent with his values. His relationship with his parents was impaired, as discussion of his fears and ambiguous physical sensations dominated their conversations. His daily activities were strictly limited to home and school.
7 Course of Treatment and Assessment of Progress
Creative Hopelessness and Willingness
The session topics and therapeutic interventions are summarized in Table 1. The first step of ACT was to instill “creative hopelessness” (Hayes et al., 2016). This process is twofold: First, David and therapists (first and third authors) discussed the effectiveness of escape, avoidance, and reassurance-seeking in “solving the problem.” Based on a critical review of the evidence, David came to the conclusion that these strategies sometimes worked for a short amount of time, but in the long term, they were not successful. The therapists then suggested that these strategies to eliminate unwanted thoughts and emotions were not “workable” based on his own experience. As such, they should be abandoned. Second, if such strategies were not working, it was suggested that an alternative approach would be acceptance and willingness.
Summary of session topics.
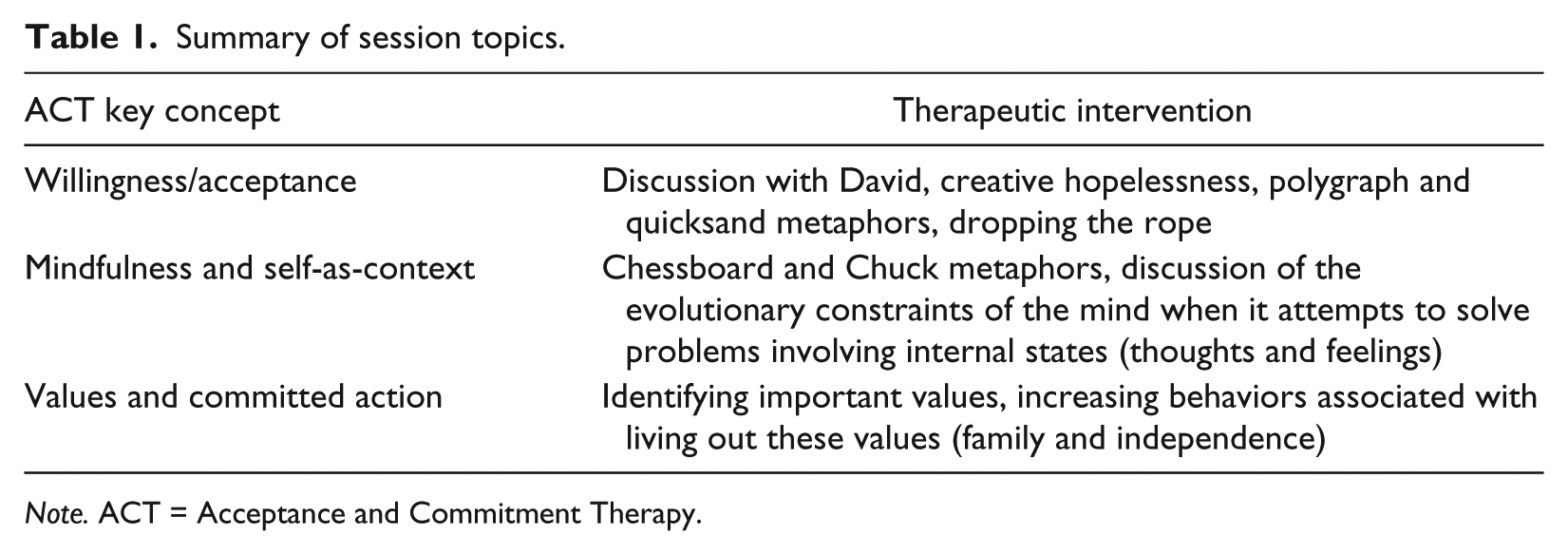
Note. ACT = Acceptance and Commitment Therapy.
In ACT, an important aspect of acceptance is the willingness to discontinue ineffective control strategies (Hayes et al., 2016). Control strategies are methods that clients use to eliminate, control, or avoid unwanted thoughts or feelings. In David’s case, control strategies were avoidance and reassurance-seeking.
To reinforce the concept that control strategies were unworkable, the polygraph metaphor was introduced (Hayes et al., 2016). In this metaphor, David was asked to imagine whether he would be able to prevent himself from having a negative thought or feeling 5 min if he was attached to a polygraph machine that could (a) very accurately detect negative thoughts and feelings, and (b) would shoot him if it detected any negative thought or feeling. In this metaphor, clients generally readily acknowledge that negative thoughts and fears could not be controlled under these conditions. This metaphor was then extended to his personal life. That is, he was asked to contemplate the idea that if negative thoughts and feelings cannot be controlled for 5 min with one’s “life on the line,” how likely is it that they can be controlled in any other life context for a longer period of time? Another metaphor was then presented. Here, David was asked to imagine whether he could immediately and honestly fall in love with a stranger if he was offered 1 million dollars. Again, he noted that this was not possible. In this way, the therapists were encouraging David to consider that thoughts and feelings, whether positive or negative, cannot be effectively controlled even when the stakes are very high.
As an alternative to control, David was asked to consider willingness and acceptance. The “quicksand” metaphor and “dropping the rope” metaphors were used to illustrate this concept. In the quicksand metaphor, David imagined being stuck in quicksand. Even though, his mind generated a solution that involved struggling to get out, which increases “being stuck,” the best way to survive in quicksand is to relax, come into contact with the quicksand, and float. This idea was then extended to the notion of interacting with his emetophobia symptoms. In “dropping the rope” (Hayes et al., 2016), David held one end of a rope and the therapist held the other end, and represented David’s mind. He was asked to move to a different spot in the room, but as he did so, the therapist pulled on the rope and prevented him from moving freely. At the same time, the therapist repeated to him the various self-statements identified in the functional analysis, such as “you’re going to vomit,” “it’s going to be horrible,” and “you won’t be able to stop.” David initially struggled with the “mind.” Then David was asked to drop the rope, and he was able to walk freely without arguing with the mind. This experience was then discussed, and the conclusion was that engaging in a struggle with thoughts and emotions that are inherently uncontrollable consumes energy, limits behavioral activity and freedom, and is ultimately unsuccessful. Alternatively, coming into contact with the negative thoughts and feelings while not attempting to control them is associated with less effort and confers more freedom and behavioral activity even when the negative thoughts and feelings remain present.
For homework and throughout the course of therapy, David was asked to journal his thoughts and feelings between sessions. As therapy progressed, it was evident that journaling was an effective way for David to document his thoughts and feelings. As he became more familiar with ACT principles, he began to recognize moments in which he was engaged in avoidance behaviors and/or engaged in unsuccessful control strategies.
Mindfulness, Defusion, and Self-as-Context
Mindfulness was described to David as paying attention to the present moment without resisting or trying to change it. No formal mindfulness practice was initiated with him. Instead, mindfulness was taught within the context of willingness. The chessboard metaphor (Hayes et al., 2016) was used to assist David with defusion. He was asked to consider his warring thoughts and emotions as pieces on the chessboard. Instead of identifying with and personifying these thoughts, he was asked to imagine that he was the chessboard, the part of the game that holds all of the pieces, but is not affected by them.
One unique method used with David was personification of his worries and fears about vomiting into a single being: “Chuck.” Naming a group of thoughts or even naming one’s mind is an ACT technique arising from relational frame theory that is used to increase awareness of self-as-context and cognitive fusion. By naming his vomit-related fears and worries, David could separate these thoughts from his observer identity. As Chuck is personified, it was easier for David to notice and experience unhelpful thoughts and emotions without using avoidance and escape strategies. Eventually, he began taking on the language of the therapists and talked about emetophobia thoughts as “Chuck,” demonstrating increased defusion and understanding of self-as-context.
David was asked to consider the function of the mind and how it developed.
From an evolutionary framework, the mind is an outcome of selection in which the detection, avoidance, and escape from real-world threats conferred survival advantage. However, another outcome of evolution is that human’s acquired language and symbolic representation of the real world via internal cognitive representations. Thus, a human can encounter external real-world threats and internal imagined threats. Detection, avoidance, and escape from the former are generally effective and adaptive. Detection, avoidance, and escape from the latter are generally ineffective and maladaptive as illustrated by the polygraph metaphor, quicksand metaphor, and cognitive research demonstrating that efforts to suppress specific thoughts and feelings tend to paradoxically increase the frequency and intensity of the unwanted thoughts and feelings (Hayes et al., 2016).
Values and Committed Action
The last few sessions were solely focused on David’s personal goals and pursuing valued life directions despite feeling fragile and fearful. He planned various activities with the therapists to live in accordance with identified values and engaged in these activities between sessions. Some of his values were to maintain good relationships with his family and become more independent.
David valued his relationships with family members and wanted to maintain and improve these relationships. He was asked to consider how his relationship with his parents had been affected by his emetophobia, and he reported that his conversations with them were primarily about his somatic symptoms. In an effort to live in accordance with his values, he decided to talk with his parents about other subjects, choosing instead to tell them about his day or to compliment his mother on dinner. He also shared that he would like to spend time with his siblings. This resulted in improvements in his relationships with his siblings and spending less time alone thinking about emetophobia symptoms.
Another of David’s values was to become more independent. Thoughts that he was vulnerable or could be easily harmed kept him from engaging in independent activities. In an effort to build greater independence, the therapists asked him to practice engaging in behaviors that were perceived as “risky” to David. These activities included being alone, such as riding his bike for longer distances or swimming underwater. Other activities to gain independence were going to the store alone and applying for jobs at local businesses. As the first year of college was approaching, David considered with the therapists whether he would like to live on campus in a dormitory or live at home and commute. He was experiencing some ambivalence about this choice because of financial reasons in addition to his beliefs about vulnerability. He also had concerns about whether his roommate or others would be able to help him if he had a health-related emergency. These were contrasted to the benefits of living on campus and being in greater contact with his peers. Ultimately, David chose to commute and agreed to seek out student organizations or activities to be more connected to campus life.
8 Complicating Factors
As noted earlier, David was diagnosed with a chronic metabolic disorder that required careful diet management. Because of this, there was a greater-than-typical risk of adverse health impact if David skipped meals or restricted food consumption to manage anxiety. In addition, David had been provided with a prescription for Ativan by his physician to be used as needed during episodes of anxiety. He and his father were hesitant for him to use the medication. He did derive some relief from use of Ativan during severe episodes of anxiety, but he used it very rarely.
9 Access and Barriers to Care
David sometimes had difficulty planning and engaging in behaviors that were in accordance with his values, especially the value of being more social. This was conceptualized as experiential avoidance of anxiety resulting from ambiguous social interactions. He tended to choose activities that increased his independence and exceeded his caution threshold, but these activities tended to be those he could complete alone or with close family members. Toward the end of therapy, he gradually began to engage in behaviors that increased social contact outside of family, including searching for jobs. Following therapy, he chose to participate in on-campus student activities and joined student organizations, and was able to interact with people with shared interests.
10 Follow-Up
David returned 6 and 12 months after completion of treatment to complete follow-up measures and check-in with therapists. At 6 months, David reported that he was doing well, especially in school. He indicated that he enjoyed the previous semester of classes and that he had successfully completed his final exams. He also shared that he had become involved in a couple of on-campus organizations. Based on his report, David appeared to be engaged and flourishing in the social and academic domains of his life as a student. He explained that, though thoughts related to vomiting sometimes arose, he was still able to avoid avoidance and engage in his valued behaviors relating to his family and life as a college student. At 12 months post treatment, David reported that he was still doing well in school and had continued his involvement in on-campus activities. He noted that, over the past 6 months, he had experienced only a few instances of significant anxiety.
Reliability of Change Indices (RCIs; Jacobson & Truax, 1991) were used to evaluate the magnitude and reliability of change in outcomes measures relative to baseline. RCI is calculated by dividing the difference between two measure scores by the standard error of difference between the two measure scores. Jacobson and Truax (1991) set the levels of a “clinically significant” RCI at 1.96 and 1.65 which, respectively, correspond to the two-tail and one-tail probability .05 level. The RCIs for David are presented in Table 2.
Summary of Emetophobia Symptoms and Psychological Flexibility.
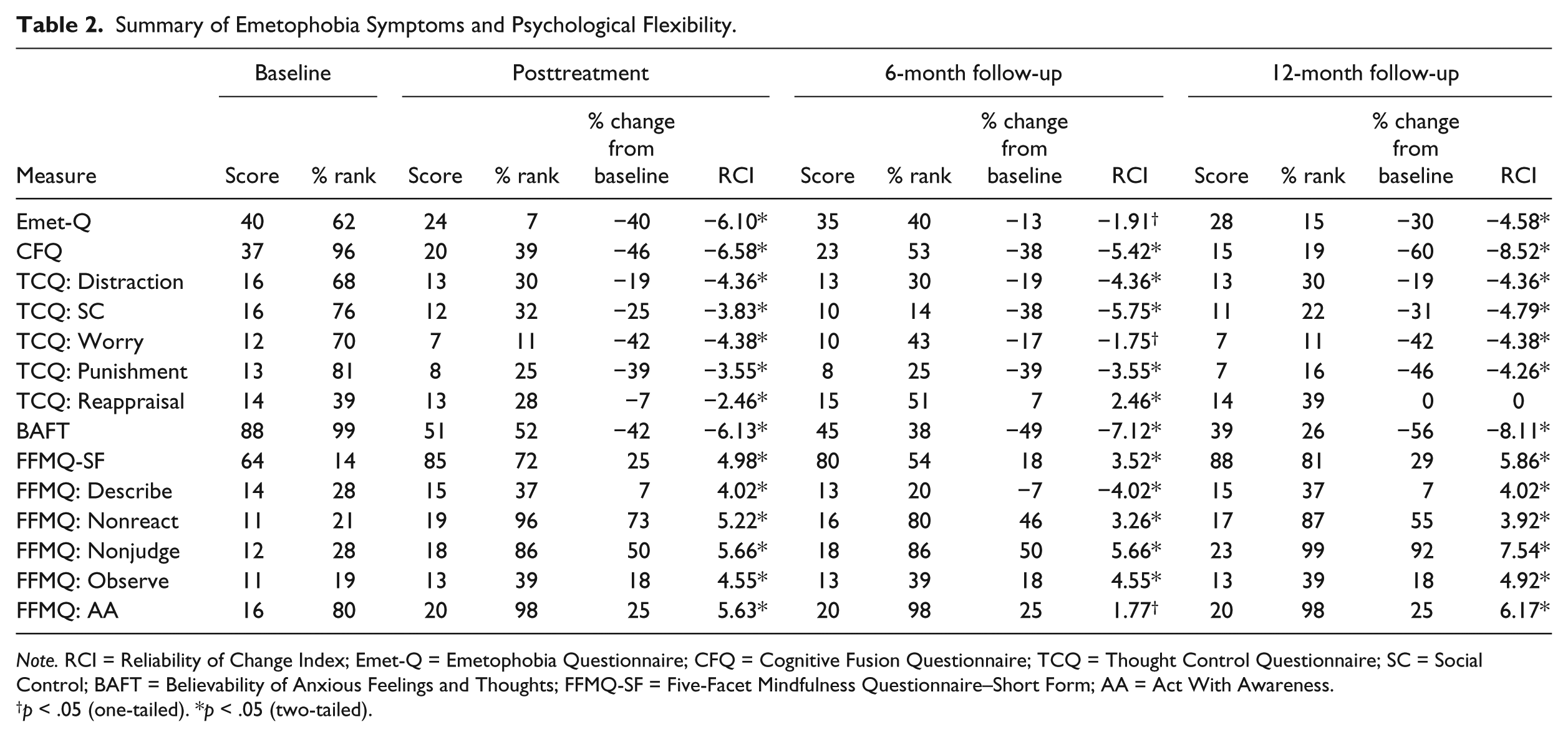
Note. RCI = Reliability of Change Index; Emet-Q = Emetophobia Questionnaire; CFQ = Cognitive Fusion Questionnaire; TCQ = Thought Control Questionnaire; SC = Social Control; BAFT = Believability of Anxious Feelings and Thoughts; FFMQ-SF = Five-Facet Mindfulness Questionnaire–Short Form; AA = Act With Awareness.
p < .05 (one-tailed). *p < .05 (two-tailed).
We examined RCI scores for emetophobia symptoms at baseline, posttreatment, 6-month follow-up, and 12-month follow-up. RCI scores indicated large and clinically significant improvements on all 14 outcome measures between baseline and posttreatment with the largest RCIs being observed for the CFQ, FFMQ Acting with Awareness Scale, the TCQ, and the EmetQ-13. At 6-month follow-up, 13 of the 14 measures remained significantly improved (RCI > 1.96 or 1.65). An examination of the 6-month follow-up means indicated that the EmetQ-13, CFQ, TCQ-Worry, and TCQ Reappraisal increased a small to moderate amount relative to posttreatment. In addition, the TCQ Reappraisal subscale was significantly higher than the baseline mean. However, this increase represented a very small 1-point increase in the subscale total.
At 12-month follow-up, all measures except for the TCQ Reappraisal scale remained significantly improved relative to baseline. The TCQ Reappraisal scale was unchanged relative to baseline. An examination of the 12-month follow-up means indicated that, relative to the 6-month follow-up means, additional gains were made on the Emet-Q, CFQ, TCQ-Worry, TCQ-Punishment, BAFT, FFMQ Total, FFMQ-Describe, FFMQ-Nonreact, and FFMQ-Nonjudge. Symptoms of heightened physiological responses as indicated by panic attacks decreased considerably in frequency and intensity at the end of treatment and at follow-up. Targeted cognitive variables of interest, such as catastrophic thinking, appeared to have decreased, as evidenced through the significant improvements in believability of anxious feelings and thoughts, use of thought control methods, and mindfulness skills. Behavioral areas targeted for improvement, such as reassurance-seeking and checking behaviors, also decreased following therapy. David was more engaged in social behaviors with family and in his community, and reported increased positive mood at follow-up. Of interest, reduction of his emetophobia symptoms was not maintained at 6-month follow-up. Many of the symptoms that had been reduced at posttest had returned to baseline levels, and these tended to be items referring to avoidance of situations that may induce vomiting or people who have vomited or are sick.
11 Treatment Implications of the Case
The functional analysis helped individualize the ACT intervention for David by articulating the topography and function of various problem behaviors along with moderating and mediating variables. As we identified the unique functions of his behaviors, we were able to provide specific interventions early on in treatment. For example, by discovering that anxiety was negatively reinforced through reassurance, we were able to recommend that David instead engage in values-consistent and nonavoidant behaviors, such as engaging his parents in conversation about his day.
Increases in acceptance and mindfulness, as measured through ratings of mindfulness (FFMQ-SF) and methods of controlling thoughts (TCQ), were observed following treatment. These increases were generally maintained to the follow-up measurement point. Similarly, measures of cognitive fusion were significantly reduced as evidenced by ratings on cognitive fusion and believability of anxious feelings and thoughts, and these ratings were maintained at the follow-up measurement point. Although David did not engage in a formal mindfulness meditation practice during or outside of session on his own, many of the therapy sessions were spent increasing acceptance, which is a large component of mindfulness. Mindfulness concepts may have been promoted in therapy through acceptance and self-as-context metaphors, especially the chessboard, polygraph, and quicksand metaphors, and the therapists’ encouragement to “drop the rope” with his thoughts. He also engaged in valued-based actions that promoted increased contact with uncomfortable thoughts and feelings that he had been avoiding. For David, in particular, emetophobia appeared to be maintained through negative reinforcement, so a focus on acceptance, present moment awareness, and committed action in the presence of distressing thoughts and feelings were critical components of ACT.
It is important to note that reductions in David’s emetophobia symptoms fluctuated over time. His EmetQ-13 score was very low at posttreatment. It increased to a marginally higher level at 6 months and then decreased to a lower level at 12 months. This pattern was observed for several other measures, and the emetophobia symptoms did not appear to regress more than these other measures. Based on our interviews with David and an analysis of the timing of follow-ups, the 6-month regressions may be due to two co-occurring factors. First, the 6-month follow-up shortly followed David’s first college-level final exams. It may be that the stress of exams and the end of the semester could have contributed to an increase in sympathetic activation and thereby brought about an intensification of symptoms (see Figure 1) as well as some regression in acceptance, mindfulness, and defusion. At the 12-month follow-up, David may have been more acclimated to college-level work and the associated stress would be diminished. In addition, the 12-month assessment did not closely follow final exams. A second possible factor is that the 6-month follow-up meeting with David, which occurred after he completed the follow-up measures, may have served as an ACT-booster session because the therapists reviewed progress with him and reminded him of key ACT concepts.
12 Recommendations to Clinicians and Students
To our best knowledge, this is the first published account of ACT for emetophobia. Important to the success of this case is the discussion held outside of session between the two co-therapists to determine the most accurate conceptualization of the function of David’s behaviors and thoughts. Creating a FACC was integral to determining the focus of treatment. A third variable for success was the identification and effective use of values-consistent behaviors to replace avoidance behaviors.
Initially, a challenge to this case was cultivating David’s willingness to be in contact with uncomfortable experiences, including his fear of vomiting. Noticing his fears without struggling with his thoughts was particularly difficult for him. He had a long history of using internal experiential avoidance strategies such as analyzing, evaluating, and reassurance-seeking. Convincing David to discontinue these control strategies was challenging because it initially intensified his distress.
As noted above, there are no other published studies exploring the effectiveness of ACT for emetophobia. However, ACT has been successfully used for the treatment of other anxiety disorders (Arch et al., 2012; Avdagic, Morrisey, & Boschen, 2014; Bluett et al., 2014). The single-subject data presented here indicate that ACT was associated with improvements in many psychological constructs, such as mindfulness, defusion, and thought suppression, in a way that is similar in studies of other populations. However, there are limitations in generalizing from this single case. Importantly, the two-phase AB design (where the “A” phase is the baseline and the “B” phase is the treatment phase) of this investigation cannot rule out that other historical and nontreatment-related factors might have also influenced outcomes. Although the evidence in the literature and the present case are promising, more studies should be conducted to further evaluate the efficacy of ACT for specific phobias in general and emetophobia in particular.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.