
Abstract
This single case study examined symptom change in the treatment of a 22-year-old Caucasian female college student presenting with anxious and depressive symptoms and maladaptive coping strategies in the context of an interpersonal dispute. The treatment integrated mindfulness skills training with interpersonal psychotherapy (IPT) to treat symptoms of anxiety, depression, overall total symptoms, and relational problems across the 18-session treatment. We assessed symptoms across treatment and analyzed change in symptom severity over time. Reliable change index analyses indicated significant symptom reduction between baseline levels at the start of treatment and the final sessions in all measured symptoms (anxiety, depression, total symptoms, and interpersonal relations), with decreases in symptom severity occurring gradually over the course of treatment. A 1-month follow-up assessment of symptoms indicated sustained reductions in anxious and depressive symptoms since baseline measurements. We discuss recommendations on the importance of therapeutic flexibility in treating comorbid conditions and therapist willingness to combine multiple treatment approaches for better treatment outcomes.
1 Theoretical and Research Basis for Treatment
A range of studies (de Mello, de Jesus Mari, Bacaltchuk, Verdeli, & Neugebauer, 2005) has empirically supported the efficacy of interpersonal psychotherapy (IPT) for depression. Rooted in theories of attachment and communication, IPT focuses on key relationships, with a time-limited approach to grief and loss, role transitions, interpersonal disputes, and interpersonal skills (Klerman, Weissman, Rounsaville, & Chevron, 1984; Weissman, Markowitz, & Klerman, 2007). Contemporary guidelines encourage the integration of psychodynamic, cognitive, or behavioral interventions to complement primarily interpersonal interventions (Stuart & Robertson, 2012). Clinical case literature has not yet documented the integration of IPT with mindfulness meditation. This integrated approach may be beneficial, especially in clinical settings where effectiveness takes priority over rigorous adherence to research protocols. The current study examined an empirically supported interpersonal treatment for major depression, in conjunction with mindfulness meditation for stress reduction.
Major Depression
The transition to college introduces novel experiences that include subsequent stress related to changes in diet, sleep, financial pressures, and social, academic, and familial factors (Sax, 1997). Also in this developmental period of emerging adulthood is the growing importance of achieving exploration and the establishment of one’s identity and sense of self (Arnett, 2000). Indeed, there is a prevalence rate of 30.6% for major depressive disorder (MDD) among undergraduate university students (Ibrahim, Kelly, Adams, & Glazebrook, 2013).
Women, compared with men, are more vulnerable to depression during the college years, especially in the presence of risk factors including low social support, high self-criticism, lack of self-efficacy, and negative life events (Dixon & Kurpius, 2008). Depressive symptoms commonly occur among women who lack the supportive interpersonal relationships (e.g., familial, social, romantic) regularly needed for assistance during major life transitions (Beeber, 1999). Subsequently, women who lack healthy support and coping strategies are likely to withdraw from social interactions (Kindaichi & Mebane, 2012) and may experience impaired academic performance (Eisenberg, Golberstein, & Hunt, 2009), poor work performance (Harvey et al., 2011), unstable relationships (Whitton & Whisman, 2010), and substance abuse (Weitzman, 2004) during such transitions.
IPT is a short-term treatment based on attachment and interpersonal theories aimed at alleviating a patient’s symptoms by focusing on the improvement of interpersonal relationships and expanding social support systems (Stuart & Robertson, 2012). Extensive research demonstrated that IPT is an effective acute treatment of depression and may be effective in preventing relapse (Cuijpers, Donker, Weissman, Ravitz, & Cristea, 2016; Markowitz & Weissman, 2004). We selected IPT for treatment of the current client over cognitive-behavioral therapy (CBT) due to her presentation of depressive and anxious symptoms in the context of a major interpersonal dispute, or role dispute, as focus on cognitions and behaviors may not have adequately addressed her interpersonal distress. Furthermore, we chose IPT, as a short-term treatment, over psychodynamic psychotherapy due to the client’s financial constraints that would not allow for long-term treatment.
Comorbid Anxiety
Anxious symptoms are commonly comorbid with a diagnosis of MDD but can fall below the threshold of criteria for a comorbid anxiety disorder (American Psychiatric Association, 2013). MDD with subthreshold anxiety, or anxious distress, is also referred to as “anxious depression” (Hirschfeld, 2001; Silverstone & von Studnitz, 2003). Patients with anxious depression are less likely to respond to treatment (Jakubovski & Bloch, 2014; Saveanu et al., 2015) and have higher role impairment and suicidality (McLaughlin, Khandker, Kruzikas, & Tummala, 2006; Roy-Byrne et al., 2000) compared with those with nonanxious depression.
IPT has been adapted to treat a number of mood and nonmood disorders. Evidence supports the successful treatment of social anxiety as well as eating disorders and substance use disorders using IPT (Cuijpers et al., 2016). Furthermore, IPT has been modified and integrated with various approaches, such as the integration of IPT, CBT, and psychodynamic principles used by Wischkaemper and Gordon (2015) in the treatment of depression with relational distress and chronic pain in a middle-aged male. Evidence from case studies suggests that IPT has also been integrated with other treatment modalities in effectively treating comorbid conditions, such as IPT combined with CBT to treat bipolar I disorder and social anxiety disorder (Queen, Donaldson, & Luiselli, 2015), IPT combined with assertiveness skills training to treat avoidant personality disorder with depression (Gilbert & Gordon, 2013), and IPT combined with CBT to treat geriatric depression and bereavement (Wyman-Chick, 2012). Given the lack of empirical evidence supporting the efficacious treatment of generalized anxiety symptoms using IPT and the greater difficulty of successfully treating depression with comorbid anxiety versus depression alone, additional interventions may be helpful alongside IPT, to develop healthy mechanisms to cope with stress and reduce anxious symptoms that may co-occur with depression. Indeed, Stuart and Robertson (2012) suggested that patients likely benefit from a combination of interventions based on clinical judgment, even if this somewhat compromises adherence to the protocol. Thus, in the current study, we propose a trial for an additional modification of IPT to include mindfulness to better address general anxiety that often occurs alongside major depression.
The practice of mindfulness, based in Buddhist meditation, involves awareness of the present moment and one’s thoughts, physical sensations, and emotions with an accepting and nonjudgmental attitude (Kabat-Zinn, Lipworth, & Burney, 1985). Studies have demonstrated the successful treatment of depressive and anxious symptoms using mindfulness-based interventions (Hofmann & Gómez, 2017). Hofmann, Sawyer, Witt, and Oh (2010) conducted a meta-analysis of 39 studies examining the effects of mindfulness-based interventions (i.e., mindfulness-based stress reduction, mindfulness-based cognitive therapy, mindfulness programs paired with acceptance and commitment therapy or dialectic behavior therapy) and found significant effects in the reduction of anxious and depressive symptoms among treating patients with psychiatric and medical conditions.
Specifically, mindfulness-based interventions focus on learning to manage stressful experiences and social interactions with responsiveness, instead of emotional reactivity, and focusing on the present moment, rather than the past or future, reducing rumination and worry present in anxious depression (Ramel, Goldin, Carmona, & McQuaid, 2004). Indeed, Freudenthaler, Turba, and Tran (2017) found mindfulness works to reduce symptoms of anxiety and depression through the improvement of emotion regulation. Furthermore, deep breathing meditation aids in the reduction of physical symptoms of stress and anxiety exhibited in emotional disorders such as depression (Kabat-Zinn, 2003). A single case study by Preddy, McIndoo, and Hopko (2013) showed the reduction in depressive and anxious symptoms in a college student with major depression with mixed anxiety using short-term mindfulness-based treatment. There is also evidence that mindfulness can have interpersonal benefits in improving relational conflicts and relationship success (Davis & Hayes, 2011). Thus, the current treatment integrated mindfulness with IPT to provide methods to cope with anxiety and external stressors and to reduce maladaptive coping strategies (i.e., substance abuse).
2 Case Introduction
B is a 22-year-old Caucasian female and rising undergraduate senior at a public university. At the start of therapy, she was beginning work at a paid internship related to her business-related college major but was at the time not enrolled at the university. Recently, she had become fully financially independent from her mother, which required her to work various jobs and withdraw from the university as well as her university-affiliated social organization. B was self-referred for individual psychotherapy and reported a history of depressed mood and anxiety beginning in late high school, which had been amplified by recent interpersonal and financial stressors, namely that her mother had recently “stole [her] identity” by allegedly taking out a large sum of money in B’s name at a large retail store without informing her.
3 Presenting Complaints
B presented with anxious and depressive symptoms. She endorsed experiencing excessive worry, difficulty relaxing, fear of losing control, and physical tension (including feeling hot, sweaty, shaky, lightheaded, faint, heart racing, difficulty breathing, and abdominal discomfort). In stressful circumstances, she became overwhelmed and unable to independently problem solve. B also indicated irritable mood, frequent crying, apathy, indecisiveness, guilt, self-criticism, social isolation, hypersomnia, fatigue, and occasional passive suicidal ideation, described as a desire “not to exist.” Furthermore, she reported somatic complaints and marijuana use (multiple times per day) to manage nausea, body aches, and anxiety. Her marijuana use caused impairment in occupational, social, and recreational functioning and daily living, and she endorsed frequent annoyance related to others criticizing her use. B initially presented in sessions with poor eye contact, tearfulness, emotional constriction, and slowed speech and thought processes, possibly due to intoxication. The treating clinician diagnosed her with MDD, moderate, recurrent episode with anxious distress (F33.1) and Cannabis Use Disorder, moderate (F12.20).
Interpersonally, B reported frequent concern about family conflicts, loneliness, a lack of feeling loved or wanted, and a lack of fullness and completeness in her relationships. She felt disadvantaged in her problematic financial and familial circumstances in comparison with similar-aged peers. She not only had difficulty trusting others but also a strong desire for a romantic relationship that might provide her with self-assurance and confidence. Furthermore, she felt guilty about not being able to provide the relational and emotional needs she thought her mother expected.
4 History
B grew up with her biological parents and two older sisters in a mid-socioeconomic, suburban area. She grew up participating in gymnastics, which served as an important motivational and social activity. She reported that her mother was supportive but permissive in providing discipline and structure (e.g., B reported that her mother suggested they both stay home and skip school/work if B complained of feeling mildly ill). She described her father as publicly warm, generous, and religious; at home, she portrayed him as self-interested and volatile. B reported that her father was physically abusive toward her mother and sisters. She was afraid and avoidant of her father until adolescence, when she took a more defensive stance against insults directed toward her and her family members and, as a result, experienced emotional abuse in the form of verbal assaults and hostility from her father.
B’s father moved out of the home permanently following a verbal and physical altercation with B during her late adolescence, after which time she ended all communication with him. At the end of high school, B’s father was incarcerated for sexually assaulting a minor. Following the arrest, B became depressed and started antidepressant medication. She received brief therapy from the police department, which she did not find useful.
After her father’s arrest, B and her mother leaned on one another for emotional support and became close. In college, however, they grew more distant as she doubted her mother’s abilities to be financially responsible and to provide emotional support. B became more anxious, wanting and feeling the need to help her mother with bills. B, her mother, and her sisters moved to another state where B attended college a few hours from her family’s residences. She felt that she lacked “normal” family support, as her family visited only once during her 3 years at the university. After discontinuing work in food service and withdrawing from the university, B became socially isolated and financially insecure and experienced depressive and anxious symptoms, which she managed through substance use.
5 Assessment
B provided the presenting complaints and history described above during the first two sessions of treatment. At the first session, B agreed to complete self-report measures of symptom severity at the start of select sessions across treatment to track symptom change over time (see “Complicating Factors” section, for description of barriers to symptom tracking).
We measured symptoms across treatment using three self-report questionnaires. The patient reported symptoms of anxiety using the Beck Anxiety Inventory (BAI; Beck & Steer, 1993), a 21-item self-report measure. She reported depressive symptoms using the Beck Depression Inventory–II (BDI-II; Beck, Steer, & Brown, 1996), a 21-item self-report measure. She reported total symptoms and interpersonal relations using the Outcome Questionnaire (OQ-45; Lambert, Lunnen, Umphress, Hansen, & Burlingame, 1994), a 45-item self-report measure. The Total scale of the OQ-45 includes subscales of Symptom Distress, Interpersonal Relations, and Social Role; the Interpersonal Relations subscale includes assessment of general relationship satisfaction and romantic, familial, and social relational functioning.
6 Case Conceptualization
Using the biopsychosocial/cultural/spiritual model, B was conceptualized as a young woman with a small social support system and poor coping strategies currently experiencing an interpersonal dispute with her mother, contributing to symptoms of anxiety and depression. She had been on antidepressants since late adolescence, reported heavy cannabis use, and had no routine for healthy diet, sleep, or exercise. She reported that her mother struggled with depression, mood instability, and risky financial behavior. She grew up with a volatile and harsh father and an emotionally dependent mother with whom she became enmeshed. Her attachment style, conceptualized as the basis of her relational difficulties and central to IPT, was characterized by a desire for intimacy mixed with fear and worry that others will not or are unable to adequately care for her or meet her needs (i.e., fearful-avoidant attachment; Bartholomew & Horowitz, 1991).
B became emotionally distressed and dysregulated in the face of environmental stressors, which impaired her ability to maintain and pursue academic, occupational, and relational goals. Her inability to manage stress and regulate emotion created dependency on marijuana for stress reduction. She often felt separate from her peers, who were, in comparison, more conservative, religious, family oriented, and financially carefree and dependent. B lacked a solid social support network and had distant family and social relationships due to distrust and withdrawal from others, but maintained an underlying desire for genuine comfort and emotional closeness. Her depression was formulated as associated with her current interpersonal dispute with her mother. With combined anxious and depressive symptoms, B was inhibited in her emotional expression, assertiveness, and ability for open discussion about the conflict. She noted that her anxiety in asserting her needs, identifying her emotions, and confronting her mother was related to guilt about her negative feelings toward her mother, worry about her mother’s well-being, and fearfulness about the emotionality of her mother’s response if distressed by B’s assertions. Thus, she was prone to worry, social isolation and withdrawal, rumination, self-deprecation, and substance use, perpetuating her depression and unsatisfactory social life.
Therapy was designed to provide B both symptom relief and coping strategies using mindfulness skills training. Furthermore, using IPT, treatment focused on identifying B’s interpersonal dispute: Her relationship with her mother at an impasse, as contributing to her depressive symptoms. With the therapist’s encouragement, she explored her values, needs, and emotions related to the dispute; and therapy brought her to a place of informed discernment about moving forward to renegotiating the relationship.
7 Course of Treatment and Assessment of Progress
B’s treatment targeted her anxious and depressive symptoms and interpersonal problems. First, consistent with IPT, the initial sessions involved discussions between B and the therapist about B’s presenting complaints and symptoms, the diagnosis of depression with mixed anxiety, the interpersonal context of the disorder, and the frame and structure of treatment. Next, before beginning the intermediate sessions of IPT, the therapist integrated mindfulness training to help B develop healthy coping strategies (i.e., self-soothing when experiencing stressors) with the goal of providing initial symptom relief and reducing anxiety and maladaptive coping strategies (i.e., marijuana use). Treatment then shifted to the intermediate sessions of IPT and targeted improving the quality of B’s interpersonal style and depressive symptoms, with a specific focus on her interpersonal dispute with her mother. Furthermore, treatment aimed to foster realistic relational expectations, social support, assertiveness skills, and effective communication with the ultimate goal of reducing depressive symptoms. Finally, the termination phase involved reviewing progress, areas for continuing improvement, and maintenance.
Initial Sessions
The initial sessions (Sessions 1-3) included collecting baseline symptom measurements and patient history and determining B’s suitability for IPT by reviewing interpersonal struggles and anxious and depressive symptoms. The therapist reviewed with B how her symptoms indicated a diagnosis of major depression, and normalized the prevalence of the disorder and her feelings of hopelessness in the potential for improvement. The therapist framed depression according to the biopsychosocial/cultural/spiritual model (the five-factor model of distress; Stuart & Robertson, 2012) and explained the disorder to B as a product of attachment, personality, and temperament based on biological and physiological functioning that occurs in the context of social life. This contemporary model of framing depression was chosen over the more traditional disease-based medical model due to its congruency (a) with the theoretical basis of IPT in attachment and (b) with the interventions and techniques related to communication and social interactions, in contrast to medication-based interventions consistent with the medical model. The traditional “sick role” given in IPT was replaced with the approach of therapist in the role of coach, acknowledging various aspects of the disease, including the physiological, with a focus on B’s own responsibility for generating change within her interpersonal life, and building motivation, while still recognizing the difficulty and work that will likely be involved in recovery, as recommended by Stuart and Robertson (2012).
The therapist framed B’s depressive symptoms in the context of her interpersonal life using the interpersonal inventory, involving identification and conceptualization of B’s contemporary relationships, background of interpersonal problems, communication styles relevant to interpersonal problems, and the problem area and focus of treatment (Stuart & Robertson, 2012). To aid this process, B and the therapist developed her interpersonal circle. B placed one sister in the “intimate supports” circle, another sister and an ex-boss/father-figure in the “close supports” circle, and her mother as well as a couple of friends in the “extended supports” circle. B described how the recent interpersonal incident with her mother had changed their relational connection. Using an interpersonal conflict graph, B placed the importance of the relationship with her mother and the severity of the problem above midway on the axes, indicating both her relationship and the problem as highly important. B indicated that her mother’s place on the interpersonal circle as moved from intimate to extended supports over the years since beginning college, and especially given the most recent incident of identity theft. B discussed her expectations of her mother to be financially and emotionally supportive were no longer being met, and B was no longer meeting her mother’s expectations of being emotionally supportive. In this way, the therapist and B identified the focus of treatment as the interpersonal conflict between her mother and her and labeled the problem an interpersonal dispute at the stage of impasse, in which B was inactive in repairing the connection or discussing the problem and feeling resentful and hopeless for improvement.
In continuing to build B’s interpersonal inventory, the therapist brought to focus B’s tendencies to be comparative and critical of her appearance, accomplishments, social standing, and personality and discussed her lack of social support and her tendency to withdraw and isolate herself. B identified tendencies of reticent interactions, poor eye contact, lack of confident speech, and passive decision making. She reported having difficulty attending to personal positive attributes without encouragement and input from others. She also wished for emotional connection with friends and romantic partners but feared that others would not meet her relational needs and could not be trusted. Furthermore, she discovered a desire to improve her self-esteem, as she believed she leaned heavily on others to provide her with a positive sense of self. After the interpersonal inventory was created, the therapist discussed with B the connection between her interpersonal problems and her depressive and anxious symptoms.
Nearing the end of the initial sessions, the therapist discussed the challenges of recovery in B’s case of comorbidity anxiety and the treatment options for anxious depression. B agreed on the structure and frame of treatment to focus first on developing healthy ways to manage anxiety using mindfulness skills training, and then to address interpersonal problems related to her depressive symptoms, specifically her interpersonal dispute with her mother. The therapist and B planned her individual psychotherapy to be short-term (approximately 2 months) and consisting of the three remaining phases: mindfulness skills training, intermediate sessions, and termination. Initially, B and the treating clinician met twice per week for 2 months (with a mid-treatment 1-week absence of the treating clinician). B then met with the treating clinician weekly during the last 2 months of treatment (see “Access and Barriers to Care” section, for description of decisions about session frequency).
Mindfulness Skills Training
Given B’s limited ability to regulate emotions, the therapist implemented mindfulness skills training following the initial sessions of IPT, to provide initial symptom relief in helping B cope with anxiety. During the mindfulness skills training phase (Sessions 4-7), B participated in guided mindfulness exercises (i.e., guided breathing, guided mindfulness relaxation) and psychoeducation about biopsychosocial factors that exacerbate symptoms of anxiety and depression (i.e., excessive marijuana use, unhealthy sleep habits, unhealthy diet, and poor planning and time management). B learned to utilize relaxation techniques in anxiety-inducing situations and worked to develop awareness of physical sensations, thoughts, and emotions. After the main sessions of the mindfulness skills training phase, mindfulness practice was briefly utilized in instances of distress in session during the remainder of treatment, with the recommendation that B listen to guided mindfulness exercises available online at home. Later sessions included discussions on mindfulness practice as an important component of healthy interpersonal communication and assertiveness.
Intermediate Sessions
The intermediate sessions phase (Sessions 8-16) involved the use of IPT techniques to improve interpersonal functioning, specifically to explore B’s options in her interpersonal dispute with her mother, choose a plan of action, modify problematic communication styles and relational expectations, and find a satisfactory resolution to her dispute. Using nondirective exploration, B and the therapist explored her patient–mother relationship, including history, expectations, changes in relating, communication of needs, and attachment style. The recent identity theft by her mother left B struggling with guilt for her inability to help her mother’s financial situation, a desire for relational distance, and conflicting feelings of sympathy and frustration. B learned that she had grown up with a strong sense of responsibility for her mother’s well-being, a role B believed her mother expected of her and that she now found herself unable to fill given her mother’s financial actions, the lack of reciprocal emotional support, and the resulting problem of trust. B acknowledged the nonreciprocal role expectations that had developed in the relationship but was at a loss for how to move forward in their relationship. B perceived her options as (a) going back to her previous way of function, acting as a best friend and therapist for her mother and ignoring risky financial behaviors and intrusions; (b) ending her relationship completely; or (c) continuing her current method of interacting by avoidance and surface-level interactions, discussed as further perpetuating the impasse of the dispute.
Initially, B had difficulty identifying and expressing her emotions and presented as emotionally constricted. The therapist would note B’s tearfulness as she described the factual details of her relationship with her mother and often encouraged B to share her feelings. B reflected on her difficulty expressing herself due to feelings of guilt related to having negative feelings toward her mother. In an integration of mindfulness techniques, the therapist, to normalize and reassure her affective experiences, presented B with a list of universal human needs (Center for Nonviolent Communication, 2005b) to aid her in identifying aspects missing from her relationship form her mother. Furthermore, to foster emotional expression and identification, B was provided with a list of feelings when universal human needs are satisfied and not satisfied (Center for Nonviolent Communication, 2005a).
B and the therapist spent time discussing her overall relational patterns with others. She described herself unable to rely and depend on others, avoided conflict, and did not communicate her relation needs and emotions. The therapist identified the parallels between B’s general interpersonal style and her behavior with her mother and offered therapeutic resources to present another option in approaching her interpersonal dispute, one involving learning to assertively and openly discuss with her mother her disappoints, emotions, values, expectations, needs, and boundaries. B and the therapist completed communication analyses of the few telephone conversations B had with her mother during the period of treatment. Using the techniques of direct elicitation and clarification of material from conversations, the therapist helped B recognize the indirect and avoidant patterns in her conversations and their ineffectiveness in getting her thoughts heard and her needs met. The therapist provided psychoeducation on effective communication techniques (i.e., clarification and expression of emotions and needs) combined with mindfulness-related communication styles (i.e., nonviolent communication; Rosenberg, 2015) and worked with B to problem solve about how she could implement these techniques. B and the therapist also engaged in the IPT technique of role-play in sessions to practice these communication styles, with the roles of the therapist and patient switching between B and her mother. Initially, B was shy and hesitant to role-play as herself in conversation with the therapist as her mother, stating she did not know what to say or how to express herself. Over time, B became more confident and outgoing and was able to role-play as herself and rehearse techniques for asserting and expressing emotions and relational needs.
During Sessions 15 and 16, B prepared for and then reflected on a family meeting created to address her mother’s financial standing with her mother, siblings, and herself. B and the therapist completed a communication analysis of the incident and B’s affective responses. She described the interaction as challenging but found it helpful in practicing learned techniques for emotional self-awareness, assertive communication with others, and stating her needs. At this time, B indicated her readiness for session frequency reduction and termination of therapy.
Termination Phase
The termination phase (Sessions 17-18) involved reviewing progress in meeting treatment goals. Previously lacking emotional awareness, relaxation skills, and skills to effectively communicate her relational needs to her mother and others, B used treatment to reflect on her accomplishments of more open emotional expression and awareness, reduced depressive and anxious symptoms, improved self-esteem and self-confidence, and increased assertiveness in making known her relational needs and values. B entered a new romantic relationship at the time of termination and increased her social interactions and outings with others. The therapist and B discussed her increased self-esteem, independence, confidence, and trust in her ability to discern her own needs, feelings, and boundaries in a relationship, increasing her ability to trust others. Across the course of treatment and the termination phase, B expressed negative emotions more openly and readily with the therapist, spoke more clearly, presented as confident and self-assured, used more consistent eye contact, and presented as more alert. These signs suggested a healthier lifestyle and reduced substance use. She indicated uncertainty in her readiness to engage with and renegotiate her relationship with her mother in a more meaningful manner, but continued a surface-level relationship. The therapist and B noted opportunity for continuing improvement in her awareness of self and others in interactions and continuing to practice and implement learned communication skills, keeping in mind her understanding of her relational patterns and her interpersonal inventory, and continuing to consider available options for dispute resolution and renegotiation. B and the therapist scheduled a maintenance session 1 month after the last session.
Assessment of Progress
The reliable change index (RCI; Jacobson & Truax, 1992) indicates clinically significant change when a patient’s symptom levels are near those of the general population or community sample as opposed to the average symptom levels of a clinical population (Jacobson & Truax, 1992). Statistically, a significant change (p < .05) is made when the RCI is less or greater than the 97th percentile Z score (–1.96 to 1.96). We assessed changes in B’s anxious and depressive symptoms, total symptoms, and interpersonal relations using RCI. We included means and standard deviations of community and clinical populations as well as test–retest reliabilities in RCI analyses for the BAI (Beck, Epstein, Brown, & Steer, 1988; Osman, Kopper, Barrios, Osman, & Wade, 1997), BDI-II (Beck, Steer, Ball, & Ranieri, 1996; Dozois, Dobson, & Ahnberg, 1998; Sprinkle et al., 2002), and OQ-45 (Lambert et al., 1996; see Table 1).
Clinical and General Population Descriptive Statistics Used for RCI Calculations.
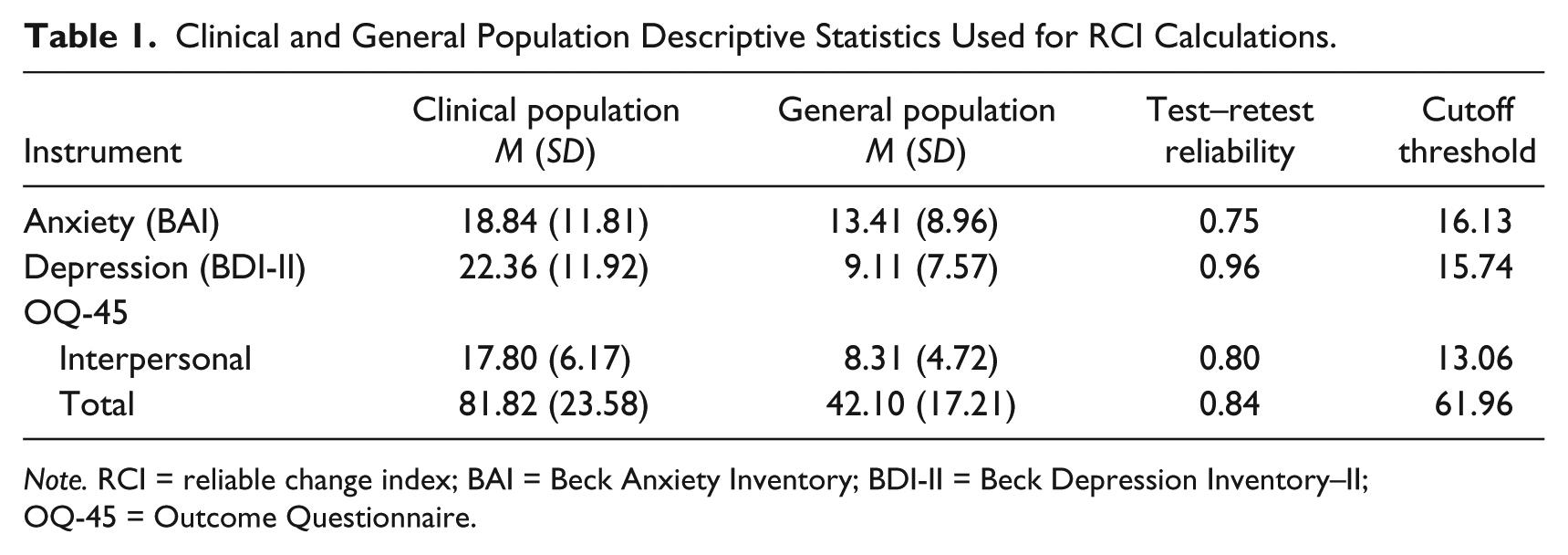
Note. RCI = reliable change index; BAI = Beck Anxiety Inventory; BDI-II = Beck Depression Inventory–II; OQ-45 = Outcome Questionnaire.
B completed self-report measures for anxiety and depression symptoms during the initial sessions phase (the average of two separate ratings from Sessions 1 and 3), twice during the mindfulness skills training phase (Sessions 5 and 7), 4 times during the intermediate sessions phase (Sessions 8, 11, 13, and 15), and once during the termination phase (Session 17). She also completed measures for total symptoms and interpersonal relations once during the initial sessions phase (Session 1), once during the mindfulness skills training phase (Session 6), twice during the intermediate sessions phase (Sessions 10 and 12), and once during the termination phase (Session 18). We calculated RCIs between the baseline average and each time point of data collection following baseline, including Sessions 5, 8 11, 15, and 17 for anxiety and depression, and Sessions 6, 10, 12, and 18 for total symptoms and interpersonal relations.
B experienced no significant change in anxious symptom severity between baseline (collected during the initial sessions) and Sessions 5, 8, and 11. However, anxious symptom improvement was statistically significant for Sessions 15 and 17, with the larger change between baseline and Session 17 (RCI = −3.40, p < .05). She demonstrated statistically significant depressive symptom reductions from baseline measurements during all time points except Session 11 (RCI = −1.17, ns), with the greatest symptom reduction between baseline and Session 17 (RCI = −8.17, p < .05; see Figure 1).
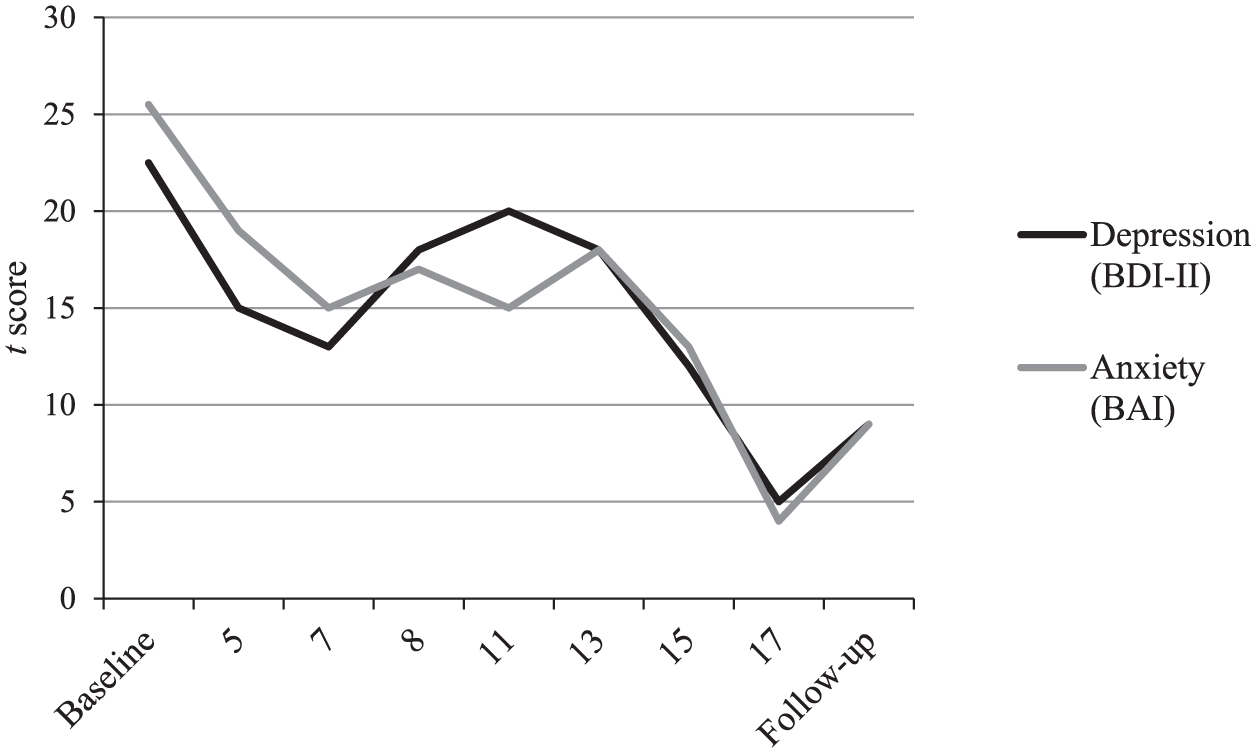
Changes across sessions on the BAI and BDI-II.
B’s interpersonal/relational symptoms showed statistically significant reduction in symptoms only between baseline and Session 18 (RCI = −5.02, p < .05). For total symptoms, she demonstrated significant symptom exacerbation between baseline and Session 10 (RCI = 2.47, p < .05); however, her total symptoms significantly decreased between baseline and Session 18 (RCI = −2.77, p < .05; see Figure 2). Overall, RCI analyses show B experienced depressive, anxious, relational, and total symptom reduction over the course of treatment.
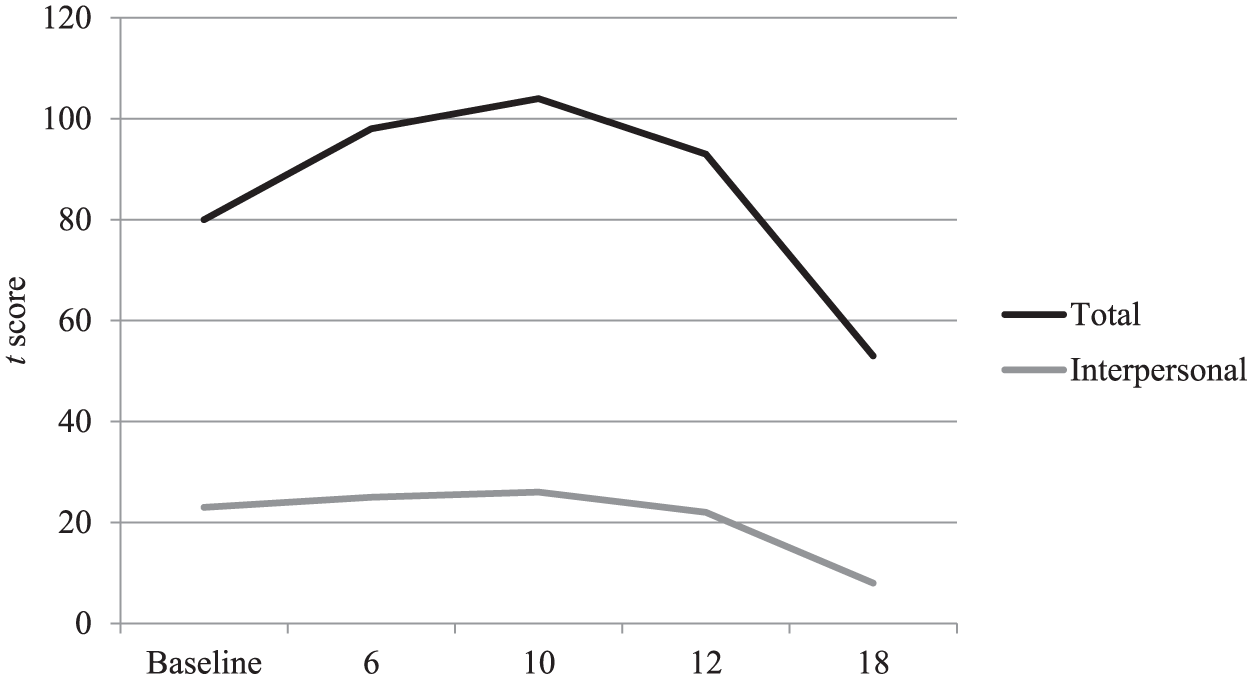
Changes across sessions on Outcome Questionnaire–45 Total scale and Interpersonal Relations subscale.
8 Complicating Factors
At the second session, B agreed to complete daily ratings of her subjective level of worry and depressed mood, both on a Likert-type scale from 1 (none) to 9 (extremely) as well as the number of bowls of marijuana smoked each day. Despite requests to complete these ratings at the third and fourth sessions, B did not adhere to the “homework” assignment. Therefore, the therapist, after a discussion with B about the low likelihood of her completing the ratings, dropped the daily ratings from treatment assessment to avoid disrupting the therapeutic alliance.
The treating clinician planned to assess anxiety and depressive symptoms, total symptoms, and interpersonal relations, alternating the Beck inventories and the OQ-45 every other session. However, B often arrived late to sessions and sometimes did not have time to complete self-report measures before or after sessions. Therefore, there was some inconsistency in the frequency of obtaining self-reported symptom severity across treatment.
At the start of therapy, B was taking an antidepressant medication. Between Sessions 7 and 8, she abruptly stopped taking this medication after she was unable to set up an appointment with her prescriber before her prescription was empty. This immediate discontinuation of medication may explain the increase in depressive symptoms between Sessions 8 and 11. B sought medical services after reporting the issue and started a different antidepressant medication by Session 10, at which time the therapist discussed with her the importance of prescribed medication adherence. The evidence for symptom reduction resulting from medication alone, psychotherapy alone, or combined medication-psychotherapy treatment in the current case is inconclusive; however, a meta-analysis by Cuijpers et al. (2016) indicated that IPT combined with pharmacotherapy was more effective in treating depression than IPT alone.
9 Access and Barriers to Care
The treating clinician received B’s case after she worked for approximately 1 year with a previous clinician who departed from the treatment center. She began treatment with an outstanding bill and no means to pay her balance. To continue treatment, B and the therapist made a fee agreement in which the treatment center did not charge her for the subsequent 2 months of treatment. However, she was required to pay at least 50% of the outstanding balance by the end of the 2 months to continue therapy. Under these circumstances, the treating clinician and B agreed to meet twice weekly rather than once weekly in the case that she may not be able to pay the required amount by the end of the 2 months. Although this barrier to care occurred, the fee agreement enabled B to participate in high-frequency short-term treatment. She was, in fact, able to pay 50% of her bill by the end of the 2 months. After the 2-month no-fee time period ended, B and the therapist agreed to meet weekly to better work with B’s financial abilities and to allow for a more gradual ending to treatment. B indicated reduction in symptom severity and readiness for decreasing session frequency.
10 Follow-Up
After treatment, B participated in a 1-month follow-up session, at which time she completed self-report measures of anxious and depressive symptoms. At the follow-up session, her depression score (T score = 9) and her anxiety score (T score = 9) indicated a slight increase in symptoms since termination. However, symptoms of depression (RCI = −6.31, p < .05) and anxiety (RCI = −2.60, p < .05) remained significantly reduced from baseline levels at follow-up.
11 Treatment Implications of the Case
IPT is an empirically supported treatment for depression (Elkin et al., 1989; Weissman, 1979); in addition, mindfulness is effective for the treatment of anxiety (Hofmann et al., 2010). The current client participated in a combined treatment focused on (a) fostering healthy coping skills for anxiety reduction and stress management through mindfulness and (b) reducing depressive symptoms surrounding an interpersonal conflict through thorough understanding of the conflict and developing effective skills for communicating and relating with others. The present study sheds light on the potential efficacy of a brief intervention combining mindfulness and IPT in the reduction of anxious, depressive, total symptoms, and interpersonal problems. In sum, B’s scores on self-report measures indicated significant reductions in anxious and depressive symptoms as well as total symptoms and problematic interpersonal relations across the course of treatment. Specifically, B’s anxious symptoms decreased gradually across treatment, whereas her depressive, relational, and total symptoms initially decreased, with a brief elevation during B’s sudden break in her antidepressant treatment regime, and gradually decreased to nonclinical (or near nonclinical) levels.
The gradual decrease in anxiety symptoms following mindfulness skills training suggests the learning and implementation of adaptive coping skills prior to the focus on interpersonal skill building and relational and communication analysis may be helpful in addressing treatment-resistant depression with comorbid anxiety, particularly in cases where maladaptive ways of coping (i.e., substance abuse) are evident. In the current treatment, mindfulness may have provided a technique to manage anxiety while also engaging in analyses of communication patterns and interpersonal incidents by improving emotion regulation and awareness of B’s own emotions and interpersonal needs. Furthermore, the focus of mindfulness on nonjudgmental acceptance of one’s emotions and thoughts may have fostered improvements in B’s self-worth and decreased self-criticism. Although B had not resolved her interpersonal dispute with her mother at the end of treatment, she appeared to have a better understanding of her past and present interpersonal patterns and a set of skills for effectively communicating her emotional and relational needs. Furthermore, at the time of follow-up, B reported her new romantic relationship had ended due to infidelity of the partner. The assessment of symptoms at follow-up indicating maintained symptom reduction suggested that mindfulness and IPT may have fostered long-term techniques for managing external stressors and understanding of the client’s own interpersonal patterns, communication styles, and relational needs.
12 Recommendations to Clinicians and Students
The current study utilized IPT and mindfulness in a mixed-method treatment of depression and anxiety in a young adult female college student experiencing a significant interpersonal conflict. To our knowledge, this is the first instance in the existing literature of the integration of mindfulness and IPT in the treatment of anxious depression. There are limitations in the implications for the efficacy of the present treatment methods. Although the study is limited as a single-participant case study, RCI analyses of self-report measures across the course of treatment indicated significant symptom reductions in areas of anxiety, depression, total symptoms, and relational problems. Furthermore, without the reports of daily symptom ratings completed by the client, it is difficult to determine the specific effects of mindfulness, IPT interventions, and the absence and start of antidepressant medication on symptom severity.
Given the demands of daily life among clients who struggle with anxiety, depression, lack of social support, and limited financial resources, ideal circumstances for accurate symptom measurement and tracking are often not possible. In outpatient clinic settings, unpredictable factors can often impede on the therapeutic work; thus, it is important for therapists to be flexible in finding solutions with clients for how to best continue treatment in light of impeding circumstances. In inpatient settings, external factors may be better controlled (e.g., medication management and adherence monitored by hospital staff); in research settings, inclusion for participation in treatment can require completion of daily symptom ratings and regular and consistent session attendance. There is need for further empirical research to generalize these results across settings and populations, as the current study exemplifies a novel approach that warrants ongoing attention.
Clinicians who implement IPT to treat major depression and other related disorders might find that their clients benefit from therapeutic flexibility when cases of comorbid problems occur. Therapist willingness to adapt treatment to client’s presenting complaints and incorporate other forms of treatment (e.g., motivational interviewing for substance abuse; mindfulness or cognitive restructuring for anxiety) may enhance the effectiveness of therapy. In sum, the current findings suggest the potential for the value in combining the treatments of mindfulness and IPT with antidepressant medication to attain rapid symptom reduction in an instance of comorbid anxiety and depression in the context of relational problems.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.