
Abstract
This report details the course of psychotherapy methods and outcomes for a 57-year-old White man who sought services for hoarding disorder (HD) and posttraumatic stress disorder (PTSD). Over 14 months, he completed 54 treatment sessions that spanned two distinct treatment approaches. Given his presentation and the conceptualized relations among his symptoms, therapy was sequenced to address PTSD symptoms prior to undergoing cognitive–behavioral therapy (CBT) for HD. The implications of this decision were key to his treatment progress and outcome, and they are reviewed in detail. Together, treatment consisted of psycho-education, cognitive restructuring, and a combination of in-clinic and home-based exposures. Results were positive, with the client experiencing a decrease in self-reported HD and PTSD symptoms, reduction in home clutter and decreased distress related to discarding, and increased feelings of self-efficacy. In light of limited data addressing treatment for individuals with HD who have a salient trauma history, the major aim of this report is to detail how each step of the client’s treatment was approached, what factors and data were considered for reaching specific decision points, and how the sequencing of treatment is believed to have contributed to the positive outcome achieved.
Keywords
1 Theoretical and Research Basis for Treatment
Hoarding disorder (HD) is a chronic condition characterized by difficulty in discarding possessions, even those with low objective value (American Psychiatric Association [APA], 2013). A perceived need to acquire and save results in clutter and impaired daily living. In fact, 80% to 90% of individuals with HD display excessive acquisition, which may include buying, acquiring free material, or less commonly, stealing. In general, hoarding prevalence rates range from 2.3% to 6% (Frost & Steketee, 2014), with symptom onset often beginning in childhood and worsening with age (Benito & Storch, 2011). Notably, older adults diagnosed with HD tend to hoard more items and normalize their symptoms as their age advances, making detection and intervention more difficult (Ayers, Najmi, Mayes, & Dozier, 2015). Hoarding has been shown to have a negative impact on numerous domains, including health (Frost, Steketee, & Williams, 2000), daily functioning (Frost, Hristova, Steketee, & Tolin, 2013), and relationships with family and friends (Tolin, Frost, Steketee, Gray, & Fitch, 2008). Individuals diagnosed with HD may show low motivation for treatment; one clinical case study suggested low motivation to be a primary reason for poor long-term results in the treatment of HD (Savoie, 2008). Once subsumed under obsessive-compulsive disorder (OCD) per se, HD is classified in Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) as a separate diagnosis within the Obsessive-Compulsive and Related Disorders chapter.
HD may be affected by early life traumatic events. For example, individuals diagnosed with OCD, hoarding subtype, were significantly more likely to have experienced a traumatic life event than those with OCD absent hoarding behaviors, and hoarding severity was greater when traumatic life events had occurred (Cromer, Schmidt, & Murphy, 2007). Furthermore, it appears that individuals with HD have high rates of experiencing traumatic events. In a sample of individuals recruited from local agencies, individuals with HD reported higher rates of being roughly handled and forced sexual activity as compared with individuals without hoarding (Hartl, Duffany, Allen, Steketee, & Frost, 2005). Landau et al. (2011) identified a high incidence of traumatic life events in individuals with HD. Specifically, individuals diagnosed with HD experienced 6.7 traumatic life events on average, as compared with individuals diagnosed with OCD absent HD (M = 3.5) and nonanxious controls (M = 3.9). In addition, severity of hoarding symptoms was significantly correlated with the number of traumatic life events.
Despite a high prevalence of traumatic experiences, rates of comorbid posttraumatic stress disorder (PTSD) and HD appear to be relatively low. Diagnoses of PTSD were no more frequent in hoarding versus nonhoarding groups; in fact, only two participants in an HD group (n = 24) and two in an OCD group (n = 17) met diagnostic criteria for PTSD (Landau et al., 2011). Frost, Steketee, and Tolin (2011) found a comorbidity rate of just under 7% for PTSD and HD (n = 217) in adults, whereas Hartl et al. (2005) reported a 23% comorbidity rate. When examining a sample of older adults (≥ 60 years of age), comorbidity rates ranging from 5-11% were reported (Ayers, Najmi, Mayes, and Dozier, 2015; Ayers, Saxena, Golshan, and Wetherell, 2010). It has been suggested that formal diagnoses of PTSD among hoarders is relatively uncommon (Pertusa & Fonseca, 2014); however, such a finding may be explained in part by HD’s diagnostic status as a subtype of OCD prior to 2013 (see Wu, 2011). In fact, traumatic or stressful events appear to be temporally linked with the onset of HD (Tolin, Meunier, Frost, & Steketee, 2011). Therefore, when conceptualizing an individual who presents with HD, it is important to consider whether inclusion of trauma services as a treatment component is warranted.
The primary treatment goals for HD are to improve the appropriate use of space, reduce clutter, improve decision making, and process beliefs about possessions (Hartl & Frost, 1999). Consistent with these goals, Steketee and Frost (2007) developed a treatment manual based on cognitive–behavioral therapy (CBT). Steketee, Frost, Tolin, Rasmussen, and Brown (2010) found that individuals who completed this treatment showed significantly lower scores on the Savings Inventory-Revised (SI-R; Frost, Steketee, & Grisham, 2004) and Hoarding Rating Scale (Tolin, Frost, & Steketee, 2010; Cohen’s ds = 1.81 and 2.30, respectively). A meta-analysis of 10 studies that followed the Steketee and Frost (2007) treatment found large reductions in hoarding severity (Hedge’s g = .82) and moderate reductions in impairment (Hedge’s g = .52; Tolin, Frost, Steketee, & Muroff, 2015). Of specific relevance to the current report, Steketee and Frost (2007) highlighted that one factor that may influence CBT treatment outcome is unresolved trauma for clients who hoard.
Perhaps because of some low comorbidity estimates, little research has examined treatment outcomes for individuals with comorbid HD and PTSD. In general, case studies may be useful for testing methods for symptom presentations that lack empirical evidence or in advance of larger controlled trials (Gallo, Wilson, & Comer, 2013). Case studies focusing on HD often include trauma as a component of conceptualization (e.g., Cermele, Melendez-Pallitto, & Pandina, 2001; Muroff & Underwood, 2016), but published case studies appear to address the interaction of trauma and hoarding in treatment infrequently. The current report describes the course of treatment for a client with comorbid hoarding and trauma symptoms. Broadly, treatment began with a full course of cognitive processing therapy (CPT; Resick, Monson, & Chard, 2014), was followed by in vivo discarding exposures in a clinic setting, and concluded with home visits that addressed clutter, acquisition, and maladaptive beliefs. The client provided written informed consent for the preparation of this article, including his authorization to use all of the information and images herein.
2 Case Introduction
The client (“Joe”) presented at a university clinic for assessment and treatment of long-standing struggles with HD. In fall 2015, Joe was 57 years of age, a White man married to his wife of 31 years. Although he held a master’s degree and had been successful in a number of fundraising positions, he had been unemployed since early 2013. Joe was self-referred to the clinic, and at the time of intake, reported symptoms associated with what he described as hoarding, OCD, anxiety, and posttraumatic stress; however, he indicated being interested primarily in treating his hoarding symptoms.
3 Presenting Complaints
At intake, Joe reported acquiring many items daily, such as napkins, pens and other “freebies” offered by businesses, “natural” items he intended to use in his artwork (e.g., pine cones, corncobs), as well as items he purchased from stores (e.g., storage tubs). Joe hoarded information from previous jobs and objects from various familial estates for which he was the executor. These items were stored in multiple locations within Joe’s home—an office, a guest room, and a basement were the most cluttered. He tended to respond with marked distress when his wife asked him to discard items; he believed he would need the items to recall positive emotions he experienced when he acquired them or elicit positive memories of deceased family members. Critically, during the intake Joe reported having been sexually assaulted by an adult man when he was 6 years old. As of the start of treatment in fall 2015, he had not disclosed the assault to his wife or to anyone in his family.
Joe displayed limited insight into his hoarding and PTSD symptoms, and reported minimal ability to control acquiring urges or intrusive thoughts related to possessions and discarding. For example, he did not understand how certain etiological factors may have contributed to his hoarding symptoms, including how his traumatic experience may have played a role in his daily functioning or exacerbated his hoarding tendencies.
4 History
Family and Relationship History
Joe reported a “difficult” upbringing, citing poor relationships with his immediate family members and persistent financial difficulties. At the time of intake, Joe reported that a majority of his family members were deceased (e.g., mother, father, uncle, sister) and indicated only communicating with his brother at Christmas. In addition to limited familial relationships, Joe reported having few friends throughout his life, with only one current close friend. Regarding romantic relationships, he reported having one casual relationship in college before meeting his wife, whom he married at the age of 27 years. Although long-standing, Joe described their relationship as “rocky,” noting that his fear of conversation, lack of trust in people, and fear of intimacy all contributed to substantial marital distress. Also contributing to their relationship challenges were his wife’s marked symptoms of depression and anxiety.
Employment History
Joe was unemployed at the time of treatment. His most recent job was a fundraising position that was phased out following the completion of fundraising efforts. Although Joe reported accepting a number of temporary positions in the past, he also indicated struggling to relate to and get along with coworkers and superiors in the workplace. He cited differences of opinion related to how to effectively complete projects as their main source of tension.
Mental Health and Treatment History
As mentioned, Joe reported being sexually assaulted as a child. He reported repressing memories related to this experience until January 2014 when he underwent a hip replacement surgery, after which he was using opiate-based medication for pain. While taking this medication, Joe reported experiencing a muscle spasm in his leg, which caused the memories from his trauma to come “flooding” back to him. At intake, he reported experiencing frequent nightmares, increased startle response, and a dislike of being touched by anyone.
Following the assault, Joe began saving items and having difficulty discarding. He hoarded items that could be concealed easily in his bedroom desk (e.g., newspapers, pencils, food wrappers). His hoarding worsened gradually; he noted declines following several life events, including the deaths of his sister (1996), father (2011), and mother (2012).
At intake, Joe reported having participated in 8 years of therapy he characterized as “supportive.” Joe also reported multiple other therapeutic endeavors, including a 9-week stay on the inpatient unit of a behavioral health hospital. During this treatment history, however, he never engaged in exposure-based CBT.
5 Assessment
The first contact with Joe was a 90-min intake that began with an unstructured interview. Standardized measures (see below) were used to confirm previous diagnoses and assist with the novel diagnosis of PTSD. During treatment, Joe completed a number of tracking measures to assess progress; photos of his home also were taken to monitor discarding progress.
PTSD Checklist for DSM-5 (PCL-5)
At weekly trauma-focused sessions, Joe completed the PCL-5, a 20-item questionnaire that assesses PTSD symptoms on a 0 (not at all) to 4 (extremely) scale with total scores ranging from 0 to 80 (Weathers et al., 2013). A cut-off of 33 has been established for a PTSD diagnosis; a five-point change indicates reliable change and a 10-point change indicates a clinically meaningful response to treatment. Blevins, Weathers, Davis, Witte, and Domino (2015) reported internal consistency (α = .94) in college students.
SI-R
Beginning at Session 19, the SI-R was administered during alternate sessions (Frost et al., 2004). This is a 23-item measure assessing three core components of hoarding (acquisition, difficulty discarding, and clutter) and has displayed strong psychometric properties in adult and older adult samples (Ayers, Dozier, & Mayes, 2017). Symptoms are rated on a 0 (none/not at all/never) to 4 (almost all/extreme/very often) scale and total scores range from 0 to 92. The diagnostic cut-off for the total score is 41; however, individuals with hoarding concerns often score notably higher (M = 62.0, SD = 12.7; Steketee & Frost, 2007). Regarding subscales, the recommended diagnostic cut-offs are as follows: clutter = 17; difficulty discarding = 14; excessive acquisition = 9 (Tolin et al., 2011). Internal consistency has been reported for the total score (α = .92) and subscales (clutter: α = .91; excessive acquisition: α = .87; difficulty discarding: α = .80; Frost et al., 2004).
Activities of Daily Living Scale for Hoarding (ADL-H)
Joe completed the ADL-H during Session 37 (initial home visit) and again at termination (Frost et al., 2013). The ADL-H is a 15-item measure that assesses the degree to which hoarding impairs activities of daily living on a 1 (can do it easily) to 5 (unable to do) scale, with a Not Applicable option for each item. Higher scores indicate more impairment; scores ranging from 2.5 to 5 indicate moderate-to-severe concerns. The ADL-H was internally consistent (α = .92) in a sample of individuals diagnosed with HD. Convergent and discriminant validity were supported by higher correlations with SI-R clutter (r = .63; Frost et al., 2004) as compared with the Beck Depression Inventory (r = .27; Beck, Steer, & Brown, 1996).
6 Case Conceptualization
When he presented for treatment, Joe was experiencing difficulty in multiple areas of functioning and met criteria for several DSM-5 diagnoses. These were HD, OCD, PTSD, generalized anxiety disorder (GAD), and major depressive disorder (MDD). He also reported limited social support and significant marital distress. Joe’s symptoms appeared to be interrelated, sharing maladaptive cognitions and fueled by avoidance. The most notable involved Joe’s PTSD symptoms (resulting from his experience of childhood sexual assault) and hoarding behaviors. For example, Joe reported maladaptive just world beliefs, which included thoughts that he must be a bad person because only people who “deserve” to be assaulted have those experiences. These beliefs led to acquiring and retaining religious items (e.g., hundreds of crucifixes, dozens of bottles of holy water) to offset his “badness.” Similarly, the trauma resulted in feelings of inadequacy, shame, guilt, self-loathing, and the feeling that “surviving means trust no one, including myself.” As a result, he hoarded information and paperwork because he did not trust his judgment, decision making, or memories, especially when they related to discarding. Furthermore, a majority of his items provided him with a sense of validation and comfort, serving as reminders of what he is capable of achieving, his self-worth, and lost relationships.
Individual sessions of weekly therapy targeted Joe’s symptoms. Beginning at intake and spanning the first two sessions, Joe and the clinician completed a functional assessment in which interviews and questionnaires were completed to better understand Joe’s symptom severity and how his symptoms interfered with daily functioning. Whereas Joe initially felt HD was the primary source of his distress, the functional analysis indicated his PTSD symptoms were more impairing at the time, with beliefs surrounding the trauma precipitating his hoarding symptomatology. Given this relationship and subsequent impairment, PTSD symptoms were identified as the first target for treatment. Joe was presented with this rationale and with treatment options; after consideration, he chose CPT to target his maladaptive cognitions.
7 Course of Treatment and Assessment of Progress
In total, Joe completed 53 treatment sessions over 14 months. All sessions were administered by a master’s-level graduate student clinician under the supervision of a PhD clinical psychologist. During all home visits, two clinicians attended each session for safety and liability reasons. Both clinicians had experience in the administration of exposure-based therapies for anxiety and OCD in multiple, supervised settings (e.g., university training clinic, community hospital, private psychotherapy practice). Each session began with a brief check-in and review of the previous week’s homework assignment.
Treatment Phase 1: Sessions 1 to 17
Sessions 1 and 2 were spent completing a functional assessment of Joe’s psychological symptoms. As noted, it was determined that his PTSD symptoms were the most functionally impairing; our prediction was that PTSD symptoms may interfere with HD treatment were it sequenced first. As a result, Sessions 3 through 17 consisted of a full course of CPT. CPT is a trauma-focused treatment based on the social-cognitive theory of PTSD; it has been shown to be effective for a range of traumatic events, including sexual assault (Resick & Schnicke, 1992, 1993). Indeed, clinical case studies demonstrate successful treatment outcomes for survivors of both sexual and nonsexual assault following 12 sessions of CPT (e.g., Waltman, 2015; Wilson & Jones, 2010). The protocol consists of psycho-education, exposure, and skill building. Specifically, clients undergoing CPT are educated about PTSD and differences between thoughts and feelings; complete an impact statement to help identify problems in thinking or “stuck points” related to the event; create a written account of their worst traumatic incident; and challenge relevant distortions. Throughout treatment, the clinician utilizes Socratic questioning to assist with the challenging of distortions and five sessions focus on specific topics likely affected by an individual’s trauma and related distortions. The topics are safety, trust, power/control, esteem, and intimacy.
During this initial phase of treatment, Joe focused on how his traumatic experience affected his life and addressed stuck points related to this experience (e.g., “Unless I reason through everything in depth, I cannot trust my decisions”). He appeared to understand the rationale for treatment and indicated the model described was highly applicable to his life. As a result, Joe consistently was engaged with treatment, asked meaningful questions, and completed assigned homework. Although CPT is designed to be completed in 12 sessions, Joe required 14; two sessions apiece (vs. one) were spent on the trust and power/control topics. Joe evidenced a number of distortions related to both; extending the treatment allowed for more in-depth exploration of these topics and restructuring of related distortions. Through CPT, Joe displayed a marked change in PTSD symptoms as measured by the PCL-5 (Figure 1). His scores began at a 65, increased to a 70 (notably, when completing his trauma narrative during Sessions 6 and 7), and reduced to 33 (the recommended clinical cut-off) during Session 18. Although Joe’s PTSD symptoms remained clinically elevated following treatment, the 32-point (50.8%) decrease exceeded the threshold for clinically significant change (i.e., 10-to-20-point change; Weathers et al., 2013) and positively affected his daily functioning. For example, although Joe reported continuing to struggle with loss of interest in activities, trouble experiencing positive feelings, difficulty concentrating, and hypervigilance; his avoidance behaviors, nightmare frequency, and negative cognitions and feelings about the event and himself decreased, while his sleep quality increased. Notably, a number of the remaining symptoms partially could be attributed to his other diagnoses (e.g., MDD, GAD, OCD). Following what we determined to be successful completion of CPT, and with Joe’s explicit consent, the focus of treatment transitioned to hoarding behaviors.
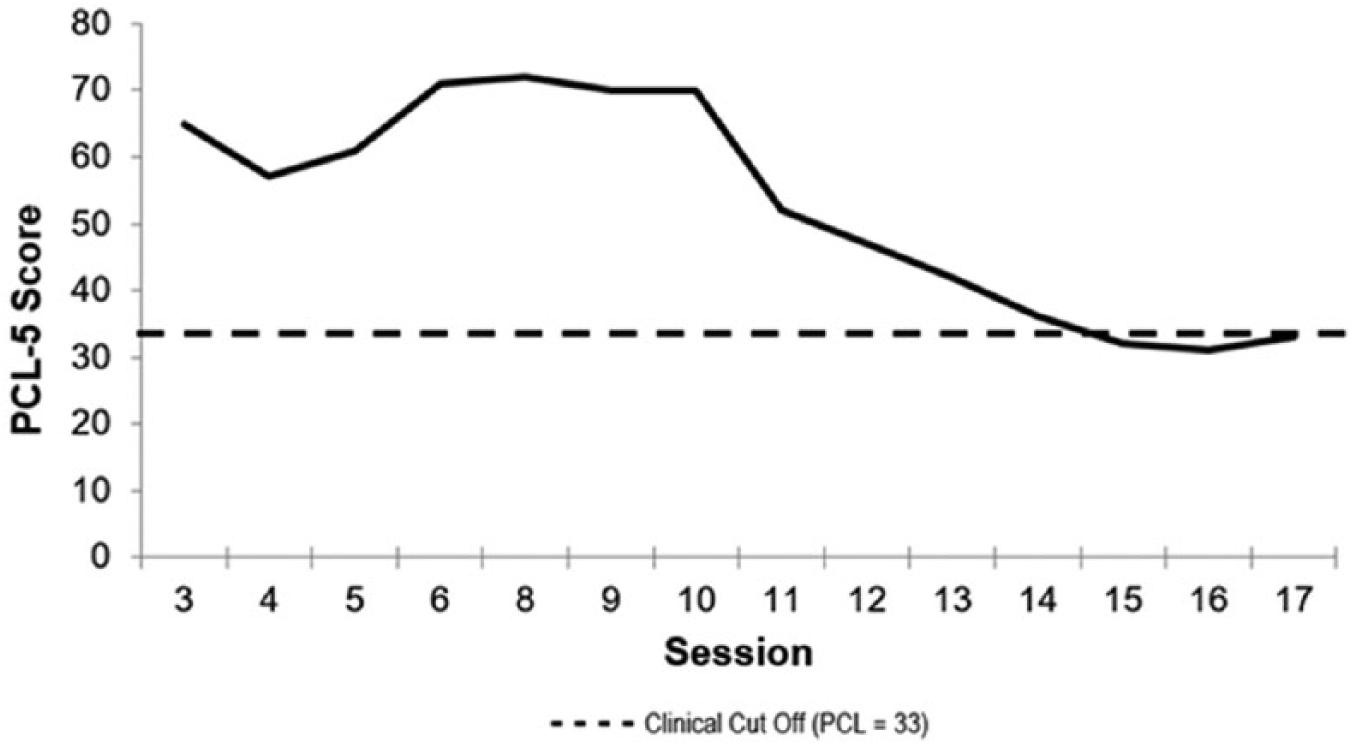
Treatment progress as measured by the PCL-5.
Treatment Phase 2: Sessions 18 to 36
During the second phase of treatment, Joe was provided with psycho-education about exposure and response prevention (ERP; Steketee & Frost, 2007), an empirically supported cognitive–behavioral treatment approach used to treat HD. Not only has this approach been shown to reduce both hoarding severity and related impairment (Tolin et al., 2015), exposure-based treatment strategies also have been shown to be more effective for, and preferred by, older adults with HD (Segal, Qualls, & Smyer, 2018). A foundation for hoarding exposures was completed from Sessions 18 through 26, which lasted approximately 1 hr each. Treatment goals included increasing the use of home space, reducing clutter, improving decision-making and problem-solving skills, and evaluating beliefs about possessions. The formal treatment rationale was discussed with Joe, and an updated functional assessment of his hoarding behaviors (including an exposure hierarchy) was completed.
Initially, Joe struggled to understand the rationale for treatment and had difficulty generating a succinct exposure hierarchy. For example, even after receiving psycho-education specific to hierarchy building, a hierarchy form to complete, and generating multiple examples with the clinician, his drafted hierarchy included 127 items that had been meticulously organized. In addition, Joe reported being overwhelmed with the idea of exposure therapy and feared he would not be able to tolerate it. However, after completing nine foundation sessions focused on psycho-education, cognitive restructuring, and skills-building, he developed an understanding of the benefits of discarding items and resisting the urge to acquire. Furthermore, he and the clinician were able to streamline his hierarchy.
Once Joe better understood and accepted the rationale for treatment, and had begun to restructure maladaptive beliefs related to hoarding behaviors, clinic-based in vivo exposures were targeted from Sessions 27 through 36. To each 90-min session, Joe brought items from his home, including greeting cards, art materials, and items acquired and saved for informational purposes (e.g., newspapers, mailing labels). During sessions, Joe was notably anxious, as evidenced by overt distraction and avoidance behaviors. When an avoidance behavior was identified, Joe stopped the behavior but had difficulty understanding the underlying concept behind avoidance and how it may impair treatment progress. This difficulty prohibited generalization of insight, which tended to result in the replacement of one avoidance-based behavior with another (e.g., switching from verbalizing prayer to making observations about clinic room décor). Joe also exhibited avoidance of homework exposures designed to increase discarding autonomy and decrease acquiring behaviors.
To address this avoidance, psycho-education and treatment rationale were reviewed and the clinician increased emphasis on cognitive restructuring, both when processing exposures and within assigned homework. Through these steps, Joe gained insight about the costs of avoidance behaviors and improved at recognizing when he was engaging in them. He was able to identify his “go-to” avoidance strategies, as well as cognitive distortions he engaged during exposures. This insight allowed Joe to redirect himself, which increased the speed and efficiency with which habituation occurred. Furthermore, it allowed Joe to challenge distortions in real time, which decreased his anxiety, increased habituation, and improved exposure performance overall.
Treatment Phase 3: Sessions 37 to 53
As the nine in-session exposure sessions progressed, Joe habituated more quickly to his in-session anxiety, and his anxiety between sessions was significantly reduced. Thus, following Session 36, it was mutually decided to take the next step in treatment: To begin home-based exposures in an effort to further improve discarding outcomes and symptom reductions per Tolin et al. (2015). Initially, home-based exposures were scheduled weekly for 2.5 hr to 3 hr; after four such home visits, they were stepped down to every other week, with an in-clinic processing session occurring on the off weeks. Processing sessions were held to assist Joe with (a) challenging dysfunctional beliefs, (b) problem solving any homework obstacles, and (c) processing difficulties in other areas of his life that may limit progress (e.g., his relationship with his wife, increased stress as a result of an automobile accident). To reduce avoidance and decrease the chance he would revisit items, Joe donated all designated items to a local thrift store immediately following each session. If he was unable to donate items for any reason—as evidenced by their presence at the following session—they were discarded when the clinician arrived.
In addition to acknowledged dysfunctional beliefs about what home-based exposures would entail, Joe verbalized significant shame regarding the prospect of having the clinicians in his home. For example, he feared that when the clinical supervisor saw the state of his home he would deem Joe “too sick” for treatment and would terminate the therapy relationship. To combat this distress, and reduce potential for avoidance behaviors, Joe completed multiple worst-case scenarios and cognitive restructuring worksheets to modify his thinking about home-based exposures. Further psycho-education also was provided about the process of home visits, with emphasis placed on the fact that all items would need a “home” and that his decisions about whether items would be kept or discarded would be final; that is, no item would be removed from the premises without his permission. Joe also was informed that to keep an item, he would be asked to provide a rationale for why and indicate where the item would be kept.
Preliminary home visit
The first visit allowed the clinician and supervisor to determine the amount and type of clutter present, for Joe to become acclimated having clinicians in his home, and to plan specific sessions. Upon arrival, it became apparent he was invested in keeping up appearances within the neighborhood: The exterior of his home gave no indication that he struggled with excessive acquiring. Conversely, the inside of the home told a different story, with rooms varying in their degree of clutter; the worst area was the basement, but each room presented challenges. Beyond clutter, dust and pet dander permeated the home, and a pronounced odor seemed to result from a lack of cleaning in the kitchen and dining areas. After completing a tour of the home and photographing each room as a baseline, Joe completed the ADL-H. His scores reflected at least moderate difficulty completing nine of 15 items and a total mean score of 2.73 (moderate concerns). As a final activity during this initial home visit, Joe and the clinician developed a plan about the order in which rooms would be targeted for treatment sessions, and which rooms would be reserved for homework. When processing this experience, Joe reported feeling embarrassed, but hopeful about the progress he might make.
Bedroom 1
A bedroom that had been repurposed into an office was the first area of the house Joe identified for discarding exposures. This selection was made for two reasons: (a) this was one of the least cluttered rooms in the house, and, therefore, a reasonable starting point in terms of degree of anticipated difficulty; and (b) Joe was especially motivated to create a functional space for his wife to work. Sessions 38 through 40 were allocated to this space, with Joe identifying which items would be kept, donated, or discarded. If items were to be kept, they were placed either in a designated area in Bedroom 1 or taken to the relevant room in the house where they were stored for later organization. Items identified for discarding were placed in trash bags that were carried to an outside trash receptacle at the end of session. Those identified for donation were placed into boxes; when full, these boxes were moved from the bedroom to the garage, so Joe could access them easily for postsession donation. Despite his initial hesitation, Joe willingly engaged with these exposures and displayed minimal avoidance.
As sessions progressed, Joe became increasingly comfortable having the clinicians in his home. Significant progress was made (Figure 2) and the ease and speed with which Joe was able to make decisions about items improved. During these sessions, Joe indicated he experienced elevated yet manageable anxiety, and was highly encouraged and motivated by the visible progress he made. His success with this area of the home made him more hopeful about future sessions and his ability to progress through his hierarchy.
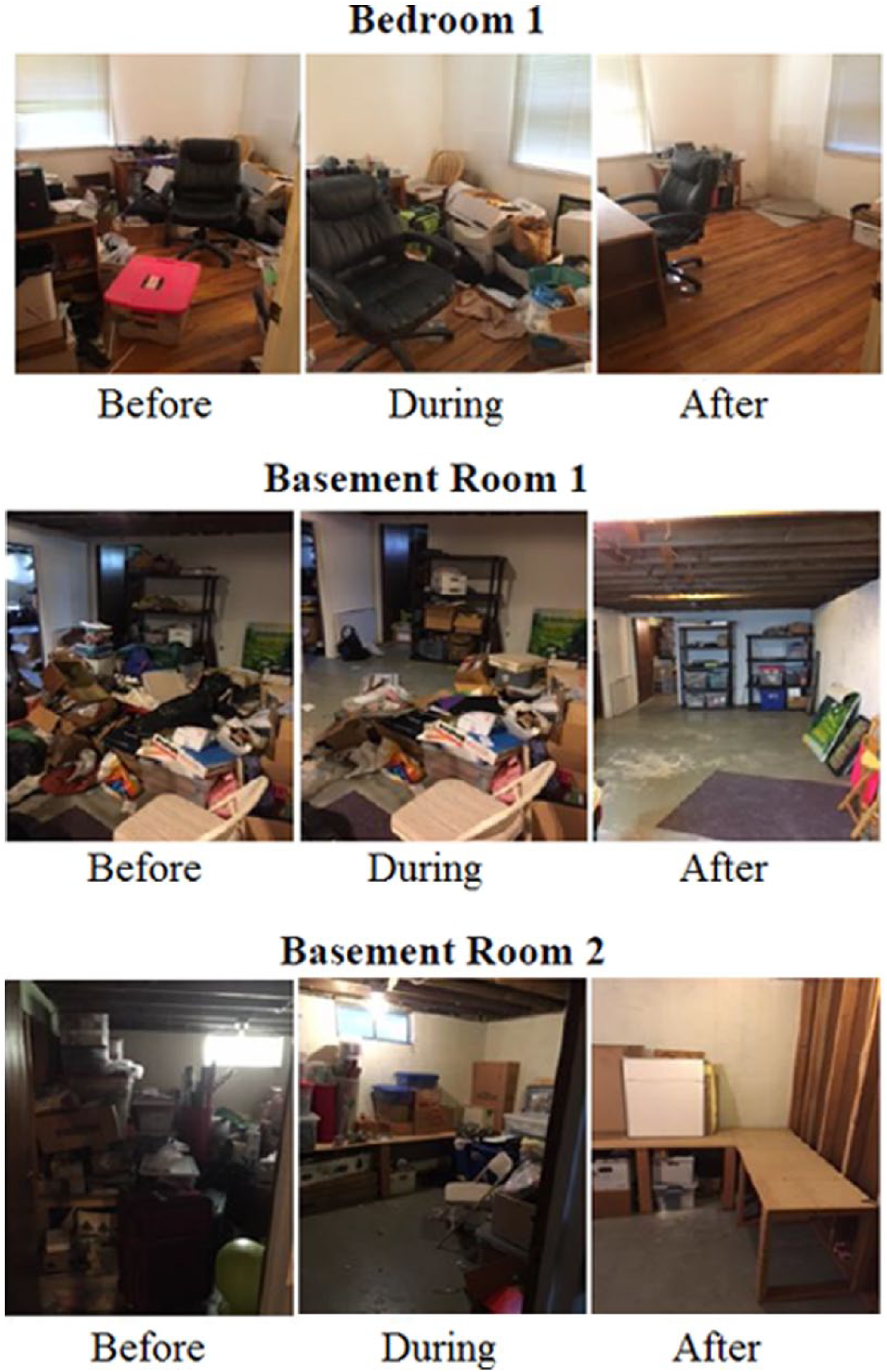
In-session discarding progress.
Basement 1
Joe’s home included a footprint basement with multiple rooms. The main basement room, the largest and most cluttered room in the house, was targeted as the second area for discarding exposures. Sessions 42, 46, and 49 were allocated to this space, with processing sessions interspersed (Sessions 43, 44, 45, 47, and 48). This room represented a clear step up in Joe’s hierarchy, mainly because it included religious items and those from family members’ estates—in other words, strong triggers. In targeting this room, Joe’s reactions to and engagement with treatment were variable and highly dependent on the specific nature of the targeted items. The first session carried the goal of increasing autonomy and confidence in decision making. Although Joe was making progress, avoidance behaviors still were evident. For example, Joe would pick up items, and delay making a decision by holding on to a more difficult item in one hand while discarding other, easier items with his other hand. After pointing out this behavior, Joe and the clinicians collaborated to implement a “one-object-at-time” rule.
Targeted items became increasingly difficult across sessions, culminating in the discarding or donating of religious items in Session 49. Joe experienced extreme difficulty with decision making and discarding when presented with triggering items, especially the bottles of holy water he had acquired through the years, including some from meaningful areas (e.g., the Jordan River). Joe acknowledged that the amount he had was excessive, and indicated it would be most beneficial to discard it (as opposed to keeping or donating); however, when it came time to discard, he was unwilling, fearing he would later need them and would be punished by God for not using them. As a result, he became highly defensive and indicated he had changed his mind: He would keep all of the bottles, despite recognizing the excess.
To address these behaviors, the clinicians reminded Joe that his decisions about items were final. However, they also highlighted that keeping items out of fear or obligation was inconsistent with the treatment rationale. In addition, the clinicians also processed his emotions, and past difficulties and successes to provide him with further motivation and evidence in favor of his ability to succeed in the current moment. In processing his anxiety, Joe revealed that his maladaptive beliefs about being a “bad person” and being punished by God had resurfaced when faced with the decision to discard these items. His beliefs, linked to his assault, increased the anxiety he experienced in relation to discarding, making the task much more difficult for him than he anticipated, especially given initial successes.
Given the level of difficulty, the exposure temporarily was suspended so Joe could spend time with the clinicians restructuring some of his maladaptive cognitions using techniques introduced during earlier phases of treatment, including re-evaluating evidence in favor of discarding versus keeping the holy water. Restructuring his cognitions resulted in increased insight via understanding anxiety was fueling his decision. Joe then was able to make the decision to discard all but one bottle of holy water. Perhaps as a compromise, he chose to discard it on an area of his lawn where it was possible, but not certain, a tree may be planted. After overcoming this obstacle, Joe was able to (a) discard items more easily, (b) reduce the items kept in the basement, and (c) organize those he decided to keep. During the following processing session, Joe reported this was a “defining moment” for him. He felt more in control and better able to manage his anxiety; he viewed challenging situations related to his hoarding as “just a problem I have to face.”
Basement 2
The final area for discarding was a second room in Joe’s basement where he had stored family heirlooms, holiday decorations, and items related to his marriage (e.g., anniversary party decorations). Although this room initially was high on Joe’s hierarchy, it took only Sessions 51 and 53 to complete. During this time, Joe displayed little avoidance, quick decision making, and full engagement with exposures. Even when unexpected heirlooms and family photos emerged, Joe was able to make decisions with minimal guidance. His struggles with triggering items in Basement Room 1 appeared to boost his confidence; he needed little assistance yet reported lower anxiety and increased ease of discarding.
Homework rooms
After each discarding session, Joe was instructed to continue to sort items from the target room identified during session. He agreed to spend 2 to 3 hr per day discarding, decluttering, and cleaning. Once he had finished his weekly work on the target room, he turned his attention to the kitchen and a second bedroom, rooms he would address independently. In addition to discarding assignments, Joe completed cognitive restructuring worksheets to assist with the reduction of maladaptive thoughts he identified while discarding. Joe successfully completed all homework assigned to him with limited avoidance. Following a serious automobile accident between Sessions 40 and 41 (described in more detail in the “Complicating Factors” section), the amount of time Joe was able to spend discarding items decreased. He compensated by increasing the speed with which he made decisions, and by having the clinicians physically assist with object placement. For example, at the end of sessions, the clinicians helped Joe identify specific boxes he needed to sort, and placed them in an accessible location, thereby making it possible for Joe to complete homework prior to the next session. Joe’s independent discarding progress is depicted in Figure 3.

Homework progress.
Termination: Session 54
After completing 53 treatment sessions and making significant gains related to both PTSD and HD symptoms, treatment with Joe concluded. This decision was supported by a functional analysis of Joe’s in-session progress (both observed and reported) and with the benefit of questionnaire data. When Joe first completed the SI-R in Session 19, he surpassed recommended diagnostic cut-offs for total and subscale scores; at termination, all scores were subthreshold (Figure 4). Examining changes on the ADL-H, by termination, Joe no longer reported being unable to complete any of the activities, with a majority of activities rated as a one or two on the scale (mean score = 1.13, indicative of minimal hoarding). During the termination session, the clinicians highlighted Joe’s successes, and provided him with the same before-and-after photographs and quantitative data presented in this report.
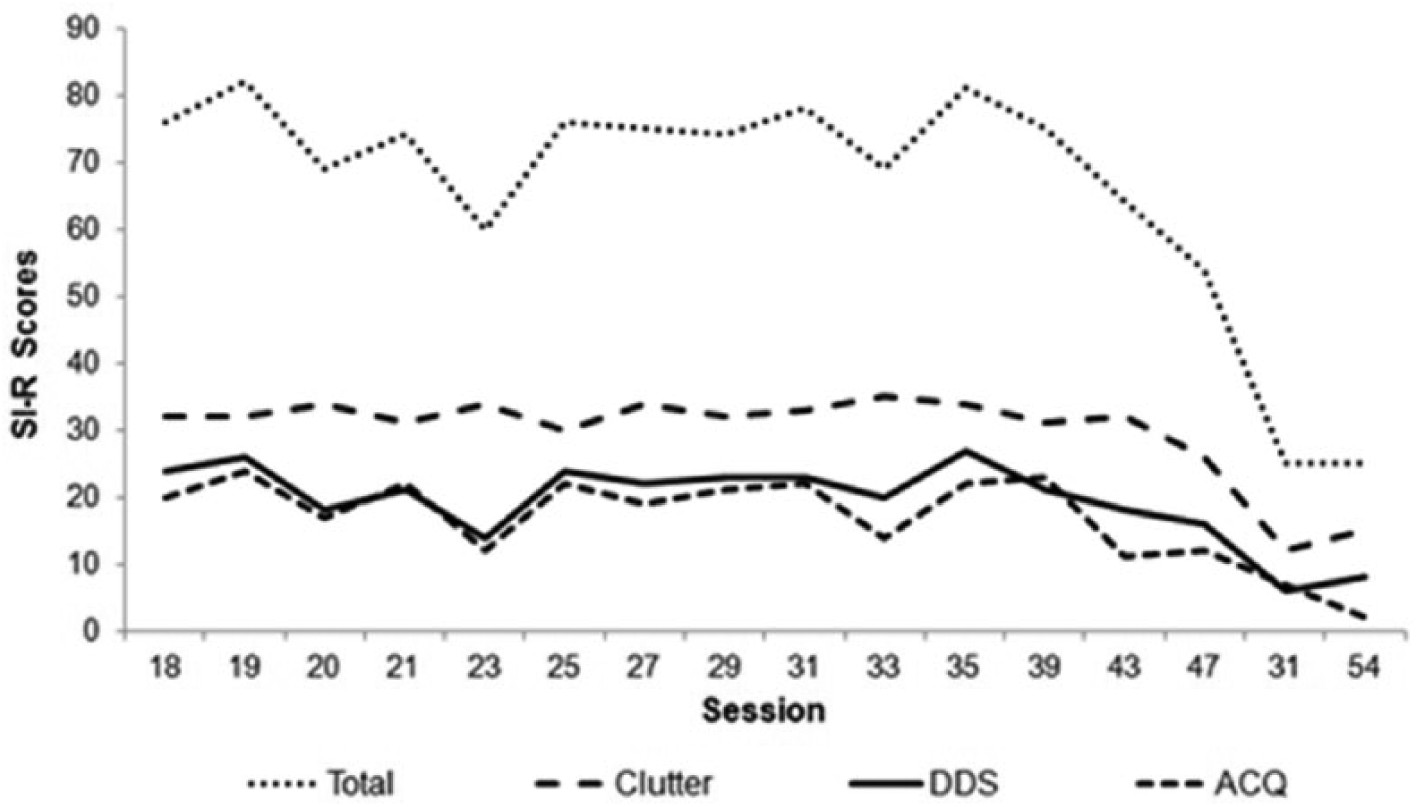
Treatment progress as measured by the SI-R.
Prior to the termination session, Joe had completed a “Relapse Prevention Packet” that asked him to identify skills learned, and how he successfully applied the treatment goals to his unique situation. These skills were reviewed, with emphasis placed on how he could continue to utilize his skills and maintain progress achieved via treatment. At the time of termination, Joe still had two rooms in his basement from which items needed to be discarded, so the clinicians assisted him with creating a timeline and problem-solving anticipated difficulties. At session’s end, both clinicians shared their pride in his efforts and offered their goodbyes.
8 Complicating Factors
Important complicating factors encountered during treatment included Joe’s marital difficulties, a serious automobile accident during the home visit phase, and age. As noted, both Joe and his wife struggle with psychopathology, which appear to have contributed to communication difficulties and a distressed relationship. For example, Joe’s hoarding exacerbated his wife’s depression, which in turn increased his guilt. Joe believed that his wife showed little interest in his discarding and would not participate in his treatment, which reduced his motivation and made homework follow-through more difficult. For 2 weeks during treatment (between Sessions 33 and 35), Joe’s wife was hospitalized for mental health reasons; his subsequent distress resulted in the need to suspend treatment. When treatment resumed, however, Joe was able to utilize learned skills to manage his emotions. In addition, after encouragement from the current clinician, Joe began couples counseling with his wife, which further helped his distress and mitigated his need to process relationship difficulties during hoarding-focused sessions. Ultimately, Joe’s skill development and engagement with couple’s therapy reduced interference with his hoarding treatment.
Joe was involved in a serious automobile accident during the final phase of treatment; injuries to his neck and back impaired his ability to stand or bend over. As a result, he was unable to attend all sessions, fully engage with the material, or complete homework in an efficient manner. Joe attempted a home visit 8 days following the accident, with moderate success. Fortunately, he had developed a strong working alliance with the clinicians and trusted them to move items and assist with disposal; this was considered a key issue that helped in keeping treatment on track. However, following this session, Joe attended a physical therapy appointment and was instructed to limit his activity; the result was the suspension of home visits for 19 days. During this time, treatment focused on cognitive restructuring and using imagery to address feared outcomes associated with discarding highly triggering items (e.g., family heirlooms). As Joe healed, he organized retained papers and shredded boxes of sensitive documents.
Although Joe was not considered an “older adult” at the time of treatment, his age had synergistic effects on his symptoms, which affected treatment. Most notably, Joe had been experiencing symptoms consistent with PTSD and HD since childhood and did not seek treatment for decades. Lack of intervention allowed Joe to normalize his avoidance behaviors and maladaptive coping strategies, thereby maintaining or increasing the severity of his symptoms. As noted, Joe reported hoarding items to remind him of lost relationships; these objects were inherited from deceased family members (i.e., his parents and uncle). Social losses are increasingly common with advanced aging and have been shown to increase the severity of hoarding symptoms (Segal et al., 2018). Furthermore, Joe also experienced a number of physical health concerns (e.g., double hip replacement) that reduced his mobility and made it more difficult to access and dispose of items. As a result, the clinicians offered extra assistance when necessary—for example, by carrying items for him, especially up the stairs—and allowing him to sit instead of stand while sorting items.
9 Access and Barriers to Care
Because Joe’s care was provided within the context of a training clinic, his access to care generally was good. Although the initial per-session fee was modest, it was further reduced due to the family’s financial circumstances. This change allowed him to attend several sessions per week as needed. Given that Joe was unemployed, he also was able to devote far more time to attending sessions and completing out-of-session homework.
A significant barrier to care was Joe’s treatment history. Prior to the current treatment, Joe had been in treatment with another therapist for 8 years. The current clinicians made repeated attempts to coordinate with Joe’s therapist and gather more information about past treatment efforts. However, this proved difficult as the therapist generally was nonresponsive. She did confirm that they had engaged in “sand therapy” and skills-building, with some success. However, without the benefit of requested documentation (e.g., treatment plans), we ultimately relied on Joe’s report. He conveyed a portion of their treatment was dedicated to hoarding; although exposure-based, this treatment was best-described as flooding. Again, by Joe’s report, the first session was a home visit, during which the therapist indicated she would bring “two men and a truck” at the following visit to remove items. Not surprisingly, Joe responded with extreme distress and avoidance of subsequent sessions. Moreover, Joe’s PTSD symptoms and related dysfunctional beliefs were not addressed, which could have contributed to his abandonment of hoarding treatment. Joe attended therapy with both providers concurrently through Session 20.
Unfortunately, communication was not the only difficult experience with regard to the other treatment provider. Despite multiple attempts, we could not reach her after the initial conversation, and thus did not discuss Joe’s efforts at trauma-based treatment. During Session 20, Joe indicated that his other therapist previously had suggested that she was upset about his slow progress related to hoarding behaviors. Per Joe’s report, she was under the impression he was working on skills-building and was unaware that he had been in treatment for trauma. We again offered to reach out to his therapist to coordinate care; however, Joe declined the offer because he was worried the call would “anger her.” Somewhat surprisingly, when the clinician repeated the offer during the following session, Joe indicated that he had terminated treatment with her, after 8 years together. Overall, difficulty coordinating care appears to have had a negative effect on Joe’s treatment progress. For example, it is possible that the other therapist was providing reassurance or treatment that was contraindicated to ERP and CPT; this could account for Joe’s initial difficulty stopping avoidance behaviors and anxiety about treatment.
10 Follow-Up
We were unable to secure quantitative follow-up data. However, Joe exhibited symptom reduction at posttreatment, and appears to have maintained at least some of these gains 1 year later. On two occasions, Joe wrote letters to our clinic to provide an update about his life and treatment progress. In these letters, he indicated that he regularly challenges himself by creating behavioral experiments similar to the exposures conducted in session. Examples include (a) going to stores to exposure himself to items he neither wants nor needs, but would have felt the need to acquire in the past (e.g., candy, containers) and (b) working to continually assess objects with which he can part and discard them without record or rituals. He stated that when he does begin to feel anxious, particularly with regard to hoarding, he is able to challenge his beliefs and confront his concerns instead of acting on them or falling into “tornadic” thinking patterns. Furthermore, Joe indicated that he sought and regularly attends supportive therapy in group and individual formats to help maintain his skills and regulate his distress.
11 Treatment Implications
The results of Joe’s treatment were positive; broader, they may be helpful to clinicians when identifying options for planning and sequencing treatment delivery for clients who report concurrent PTSD and HD symptoms. By addressing trauma symptoms prior to beginning CBT for hoarding, we were able to decrease maladaptive beliefs and increase adaptive functioning. We believe this treatment approach allowed for a smoother delivery of hoarding treatment, as the clinicians were able to refer to Joe’s stuck points and use skills that he had developed in CPT. Treatment resulted in meaningful symptom reduction as measured by the PCL-5 and SI-R; he was also able to increase autonomy and confidence in decision making and discarding. At the end of treatment, Joe reported minimal anxiety about discarding items and increased confidence in his ability to continue independent discarding. In addition, he reported an increase in self-worth (e.g., during one pointed moment, he stated that he was “walking taller”) and was planning to invite friends over to his house, something he and his wife had not done in many years.
Given Joe’s presentation and the interconnected nature of his symptoms, it was important for the clinicians to complete a full functional analysis prior to weighing treatment approaches. Clinical case studies have demonstrated the utility of conducting a functional analysis when an initial diagnosis or treatment path is unclear (e.g., Waltman, 2015). The results of this case suggest that delaying ERP for hoarding so as to allow for completion of trauma treatment may be a beneficial approach for some clients who present with comorbid symptoms. By addressing the primary trigger of Joe’s hoarding behavior before engaging in hoarding treatment, Joe was able to develop trust and rapport with the clinicians and develop insight into the underlying beliefs contributing to his hoarding. Furthermore, by beginning HD treatment with an understanding of the client’s complex presentation and relationship between his childhood trauma and current hoarding behaviors, the clinicians were able to reintroduce therapy elements that the client understood and use them constructively when he struggled. For example, while discarding highly triggering items from his basement, maladaptive beliefs relevant to Joe’s childhood trauma resurfaced, increasing his anxiety and making it difficult for him to follow through with discarding. A brief restructuring exercise was successful in addressing these trauma-based cognitions, which allowed Joe to successfully discard triggering items. If he had not completed PTSD treatment prior to HD treatment, one might hypothesize that he would have experienced heightened anxiety and difficulty discarding more frequently, which could have negatively affected treatment adherence, progress, and efficiency.
12 Recommendations to Clinicians and Students
This case highlights the importance of thorough assessment and broad consideration of a client’s symptomatology. Given the established link between traumatic life events and HD, it may benefit a number of clients to examine for a trauma history prior to beginning treatment for hoarding. Understanding how a client’s trauma influences their belief set can provide a broader perspective of the function of the client’s behavior (Waltman, 2015). For clients with histories similar to Joe, beliefs related to and resulting from a traumatic experience may contribute to irrational, obsessional reasoning that can increase distress and reduce the willingness to discard (or at least its efficiency). Thus, this case highlights how a thorough functional assessment of the interrelated nature of symptoms is helpful for clients with complex histories, especially when stressful or traumatic life events are present. Whereas Joe benefited from a trauma focus before targeting hoarding, clinicians should tailor treatment to meet ideographic needs. For example, in a clinical case study of a Hispanic woman diagnosed with comorbid PTSD and test anxiety, the treating clinician found that once the symptoms of test anxiety were resolved, the client became more receptive to treatment for PTSD, despite initial avoidance and denial of symptoms (Henslee, Schumacher, Holloman, & Coffey, 2009). A functional analysis of a client’s primary symptoms may be of particular benefit, as it can provide insight into the interconnectivity of comorbid diagnoses. Clinicians who are treating older clients, or clients who experienced significant trauma decades ago, may find a functional analysis especially helpful given the potential for limited insight or misattribution of adverse physical and psychological reactions to trauma (e.g., poor sleep) and the previous event (Segal et al., 2018).
The following recommendations may be unique to Joe’s case; however, we feel it is beneficial to provide these recommendations for individuals who are treating clients of similar populations. First, Joe initially sought treatment solely for HD; the clinician identified that the most beneficial approach to treatment would include sequencing PTSD treatment prior to addressing hoarding symptoms. When providing this recommendation to Joe, the clinician generated data from assessment measures to assist with his understanding of how the different disorders were affecting his life, and why it would be beneficial to address trauma-related symptoms first. In addition, the clinician prepared information about multiple treatment approaches for PTSD. When this psycho-education was provided, the clinician included information about why specific aspects of the treatment would be beneficial with regard to reducing PTSD symptoms and providing a scaffolding for later hoarding treatment.
Second, the selected tracking measures were successful and worked well given Joe’s presentation. Specifically, the SI-R was easy for the client to complete and allowed the clinicians to monitor symptoms from multiple domains without spending session time discussing progress in detail, which reduced the potential for Joe to avoid discarding in favor of discussing weekly experiences. Although the tracking data largely were successful, we feel as though it would have been beneficial to continue to administer the PCL-5 throughout hoarding treatment. Doing so would have provided information about symptom fluctuation and the indirect effect of hoarding treatment on PTSD symptoms. Furthermore, if a symptom increase were identified, the clinicians may have better anticipated the resistance that was experienced when discarding from the basement. Whereas ultimately this was resolved successfully, the resolution consumed a fair amount of the session, and if avoided, could have allowed for more discarding time.
Third, Joe’s age and lack of previous intervention targeting HD and PTSD symptoms likely increased the severity of his symptoms as well as the strength of his maladaptive coping strategies (e.g., avoidance behaviors, rituals). If fellow therapists are treating adults in later stages of their life, it is recommended that the therapist consider the impact age may have on symptoms and treatment. Specifically, it may be beneficial to ask targeted questions about health concerns, social losses, and other life stressors that may be related to the client’s age or generation. Furthermore, although Joe did not display impaired cognitive functioning or cognitive decline, a link between neurocognitive disorders and late-life hoarding has been established (Ayers, Najmi, Howard, & Maddox, 2014; Segal et al., 2018). Therefore, if such symptoms are identified when treating an older client, it is recommended therapists research–specific interventions and necessary treatment recommendations before providing treatment. For example, cognitive rehabilitation and exposure-sorting therapy recently has been shown to be an effective intervention for older adults diagnosed with HD and neurocognitive difficulties, and may be more helpful than traditional CBT for these clients (Ayers et al., 2014).
Finally, upon reflection, one decision the clinicians may have handled differently was the treatment of religious scrupulosity that Joe displayed. Throughout treatment, Joe’s scrupulosity only was addressed as it arose in the context of discarding sessions, both in-clinic and at-home. It is possible that addressing his scrupulous beliefs concurrently throughout discarding (e.g., providing additional belief-based homework exercises) could have facilitated HD treatment such that specific objects (most notably, holy water) may not have been as challenging for Joe to discard. Therefore, we recommend fellow therapists actively look to identify symptoms from other disorders that may interfere with treatment. If such symptoms are present, it may be especially fruitful to consider addressing symptoms concurrently with specific HD treatment, particularly, during psycho-education sessions or as homework.
In conclusion, this case highlights the role of trauma as it affected the treatment of hoarding. Given that the rate of comorbid PTSD and HD is lower than that of other anxiety-based disorders (Frost et al., 2011), trauma symptoms may not be routinely addressed in treatment. Furthermore, HD’s new diagnostic status as separate from OCD in DSM-5 means that more research is needed to investigate its stand-alone diagnostic criteria and unique associations with PTSD and other disorders. To clarify the best treatment methods and order of delivery for individuals with HD who have experienced trauma, future research may examine the components of treatment that are most effective for comorbid PTSD and HD. For example, it may be beneficial to examine whether a full course of CPT is necessary prior to HD treatment or whether addressing the most salient themes related to the client’s stuck points is sufficient. This study offered an example of a successful, sequential treatment approach for a client with concurrent PTSD and HD diagnoses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.