
Abstract
Avoidant/restrictive food intake disorder (ARFID) is characterized by restrictive eating in the absence of body image disturbance or drive for thinness, resulting in the persistent failure to meet appropriate nutritional and/or energy needs and/or psychosocial impairment. ARFID is a heterogeneous diagnosis with diverse etiologies. Thus, identification of best practice guidelines and evidence-based treatments for ARFID is challenging and, to our knowledge, randomized treatment studies have not been published. Existing literature promotes a multidisciplinary care approach that integrates behavioral, cognitive behavioral, and family-based interventions. In this report, we present the case of an 8-year-old female with ARFID who began restricting her food and fluid intake following a viral illness. The patient also choked on a lozenge at school and peers laughed in response, resulting in heightened fears of eating, subsequent dehydration, and admission to a gastroenterology unit at a pediatric hospital. While hospitalized, she was diagnosed with ARFID, a nasogastric tube (NGT) was placed, and was referred to outpatient eating disorder specialists. Despite participating in 16-outpatient therapy sessions, progress was limited and the patient was medically admitted to safely remove the NGT in the context of behavioral interventions targeting food refusal. This case report describes the successful use of an intensive inpatient behavioral intervention used for the patient, which resulted in the rapid resumption of food and fluid intake, by mouth. This case study supports the use of such intervention for ARFID when sufficient progress is not achieved in outpatient care.
Keywords
1 Theoretical and Research Basis for Treatment
Avoidant/restrictive food intake disorder (ARFID) is a relatively new eating disorder (ED) diagnosis within the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013), characterized by restrictive eating in the absence of body image disturbance or drive for thinness. Restriction must result in the persistent failure to meet appropriate nutritional and/or energy needs, psychosocial impairment, and cannot be attributed to a medical condition (APA, 2013). ARFID is a heterogeneous diagnosis with diverse etiologies that include generalized anxiety, gastrointestinal symptoms, fear of vomiting or choking, other aversive or traumatic experiences with food, food allergies, lack of interest in feeding, selective eating since early childhood, and/or sensory concerns (Eddy et al., 2015; Fisher et al., 2014).
Limited research exists regarding prevalence and characterization of ARFID. Existing findings document prevalence rates of 3.2% in a Swiss community sample, 5% to 14% among outpatients in pediatric ED programs, and 22.5% in an ED-specific day treatment program (Fisher et al., 2014; Forman et al., 2014; Nicely, Lane-Loney, Masciulli, Hollenbeak, & Ornstein, 2014; Norris et al., 2014; Ornstein et al., 2013). Within a pediatric gastroenterology clinic, 1.5% of patients met criteria for the diagnosis (Eddy et al., 2015). With respect to characterization, early findings suggest that youth with ARFID are younger, more likely to be male, and have greater comorbid anxiety and/or medical symptoms compared to patients with traditional ED (Eddy et al., 2015; Fisher et al., 2014; Norris, Spettigue, & Katzman, 2016). Furthermore, medically hospitalized youth with ARFID are more likely to receive enteral nutrition to reach caloric goals than counterparts with anorexia nervosa (Strandjord, Sieke, Richmond, & Rome, 2015).
Diagnostic heterogeneity inhibits the identification of best practice guidelines and evidence-based treatments for ARFID (Norris et al., 2016; Zimmerman & Fisher, 2017). Existing literature promotes a multidisciplinary care approach with interventions focusing on contingency management, relaxation strategies, systematic desensitization, exposure and response prevention, and family-based interventions (e.g., in vivo parent coaching; Kelly, Shank, Bakalar, & Tanofsky-Kraff, 2014; Mairs & Nicholls, 2016; Norris et al., 2016). Whereas, to our knowledge, randomized treatment studies have not been published, numerous case studies describe successful treatment approaches for ARFID across inpatient and outpatient settings (Bryant-Waugh, 2013; Fischer, Luiselli, & Dove, 2015; Fix, Proctor, & Gray, 2016; Graziano, Callueng, & Geffken, 2010; Kreipe & Palomaki, 2012; Murphy & Zlomke, 2016; Norris et al., 2016; Pitt & Middleman, 2018; Seiverling et al., 2015; Thomas, Brigham, Sally, Hazen, & Eddy, 2017; Williams, Field, Riegel, & Paul, 2011).
Fix and colleagues (2016) and Graziano et al. (2010) described the successful integration of outpatient psychoeducation, cognitive restructuring, exposure therapy, and parent training for individuals with ARFID secondary to fears of vomiting (i.e., emetophobia; Fix et al., 2016; Graziano et al., 2010). Recent studies have also highlighted the use of intensive outpatient treatment for youth with ARFID (i.e., 7-9 days of 6-8.5 hr of treatment per day) in the context of a multidisciplinary feeding team (Seiverling et al., 2015; Williams et al., 2011). In these studies, an intensive treatment format facilitated repeated exposures and behavioral shaping among children with food refusal associated with vomiting and choking fears. Contingency management included rewards for successful completion of exposures, including short breaks from treatment programming, and intentional ignoring of inappropriate behaviors (e.g., food refusal). Successful treatment of increasingly complex ARFID presentations have also been published, including Roth, Williams, and Paul’s (2010) case study describing an adolescent with Autism Spectrum Disorder and comorbid ARFID who presented for treatment with a gastrostomy feeding tube (Roth et al., 2010). The authors removed the feeding tube in hopes of increasing the adolescent’s appetite and subsequent motivation to eat. Outpatient therapy sessions focused on in vivo food exposures, with rewards for exposure completion. A token economy system was initiated in the feeding clinic in which the adolescent earned time in a preferred activity for completing beverages and bites of food, with more bites and drinks rewarded with more activity time and fewer exposures required throughout the day. It is noteworthy that published case studies have illustrated youth with caregivers who closely followed therapist recommendations in the home environment. To our knowledge, existing studies have not described youth with ARFID whose treatment was complicated by parental difficulties with consistent protocol implementation.
In this article, we present a single-case study illustrating the use of cognitive behavioral interventions for a child with ARFID who received outpatient and inpatient care. The purpose of this case report is to (a) describe the clinical presentation of ARFID in a child, (b) present outpatient interventions for ARFID and identify environmental challenges that may warrant a higher level of care, (c) demonstrate the clinical effectiveness of an individualized behavioral intervention for ARFID within the context of a brief medical admission, and (d) discuss the implications for clinical interventions for ARFID, particularly in light of environmental challenges.
2 Case Introduction
This case study describes “Sara,” an 8-year, 7-month-old Caucasian female who was diagnosed with ARFID while medically admitted on a pediatric gastroenterology service. Acute food refusal during the hospitalization resulted in rapid placement of a nasogastric tube (NGT), through which Sara received 100% of her nutritional needs. Following discharge, she attended 16 outpatient psychotherapy sessions for ARFID in the framework of cognitive behavioral therapy (CBT) for children with anxiety (Kendall & Hedtke, 2006) and behavioral parent training (e.g., Zucker, 2001). Minimal outpatient progress prompted a second hospital admission on a specialized ED service. Inpatient interventions targeted food refusal via behavioral interventions in a controlled and highly structured environment. Sara’s parents provided consent for this case study.
3 Presenting Complaints
Sara became ill with upper abdominal pain, nausea, reflux, and vomiting, prompting loss of appetite and gastrointestinal (GI) pain associated with eating. Despite considerable symptom improvement with a course of antibiotics prescribed by her community pediatrician, she reported ongoing chest and throat pain and would not eat food, limiting her consumption to caloric drinks and peppermint candies, which temporarily ameliorated her throat pain. Around 2 weeks following illness onset, Sara was seen by a GI specialist at a Midwestern children’s hospital. She was diagnosed with gastroesophageal reflux disease and ranitidine was prescribed, but her symptoms did not improve. An upper endoscopy was performed approximately 4 weeks after illness presentation, with unremarkable findings. Around this time, Sara choked on a peppermint candy at school. She swallowed the candy but was afraid that she could have died. Per Sara, her peers laughed at her when she choked and she was very embarrassed. Following this incident, her throat pain worsened, she reported the sensation of something stuck in her throat, and she stopped drinking fluids.
Around 5 weeks after symptom onset, Sara had lost 2.5 kg (5.5 lbs), representing a 10.29% body mass reduction from 24.3 kg (53.46 lbs) to 21.8 kg (47.96 lbs; see Figure 1). She had missed 10 days of school due to symptoms. Sara presented to her pediatrician with dehydration and was directly admitted to a GI service at a Midwestern children’s hospital. An NGT was placed on Hospital Day 2 for acute food refusal. A repeat upper endoscopy was normal and a video swallow study revealed functional and developmentally appropriate oral motor skills. A general consultation/liaison psychologist diagnosed Sara with ARFID after medical problems were ruled out. Basic education was provided to Sara and her parents about the illness and anxiety. She was encouraged to approach eating and drinking slowly and to integrate various coping skills, including deep breathing and progressive muscle relaxation. For the duration of the 5-day admission, Sara neither drank fluids nor ate any food. She was discharged home with an NGT at a weight of 22.7 kg (49.94 lbs; see Figure 1). Home health services were arranged to train Sara’s parents on enteral feeds. Outpatient psychotherapy and medical management referrals were also placed within the hospital’s multidisciplinary ED program.

Changes in patient’s weight over course of treatment.
4 History
Sara lived with her biological parents and her 13-year-old sister in a rural, Midwestern community. Her parents endorsed significant financial struggles and qualified for public medical insurance. Neither parent was employed, with Sara’s father receiving disability for a medical condition and her mother historically being a stay-at-home parent. The small community offered limited health care options so Sara was referred for specialist care at a children’s hospital that was 1.5 hr away from their home. Academically, Sara was in the third grade and historically received A’s, B’s, and C’s. She received extra help in reading but had never been diagnosed with a learning disorder or received formalized school accommodations. She enjoyed school and had a few close friends, but had been teased about being “poor” in the past. Sara’s parents described her as bright and strong-willed. Prior to illness onset, she loved to fish, swim, and jump on her trampoline. After becoming ill, she became more anxious and socially withdrawn. She avoided school and was disinterested in previously enjoyed activities. Of note, there was no history of developmental concerns, medical problems, or premorbid mental health diagnoses. Family history of mental health problems was unremarkable, with the exception of maternal anxiety for which a formal diagnosis had never been made.
5 Assessment
At Sara’s first outpatient psychotherapy appointment a diagnostic evaluation was conducted via clinical interview with Sara and her parents. Sara presented as appropriately dressed and neatly groomed. She appeared anxious, was tearful throughout, and made minimal eye contact, particularly when symptoms were discussed. Sara clutched a security blanket and had difficulty separating from her parents. She refused to walk down the hallway without her mother present. Parents reported that these behaviors were not typical for Sara, and began only after symptom onset.
An ARFID diagnosis was confirmed using DSM-5 diagnostic criteria (APA, 2013). At symptom outset, restricted nutritional intake was attributed to an acute illness (i.e., nausea and throat pain). Medical treatment did not resolve reported pain and restricted eating persisted. Furthermore, Sara’s choking incident exacerbated eating difficulties, resulting in fears of choking and complete cessation of food and fluid intake. Consequently, Sara lost a significant amount of weight (ARFID Criterion A). Restricted nutritional intake resulted in significant daily impairment (ARFID Criterion B). Sara became increasingly fearful of separating from her mother. She missed 10 school days in a 5-week period due to physical pain and fears. Her parents spent hours trying to coerce Sara to eat, to no avail. She was no longer included at family meals, as parents feared that watching others eat would make her too upset. Ultimately, Sara became dehydrated and a medical hospitalization was required. Sara’s food refusal was neither due to lack of food availability nor cultural practices. She denied body image disturbances and did not meet criteria for anorexia nervosa or bulimia nervosa (ARFID Criterion C). Finally, the existence of a concurrent medical condition was ruled out during Sara’s admission (Criterion D). Whereas initial symptoms were secondary to a physical illness, restricted intake persisted despite medical treatment and exacerbated due to choking fears.
It is notable that a number of diagnoses were considered and ruled out throughout the evaluation process, including generalized anxiety disorder, separation anxiety disorder, social anxiety disorder, and anorexia nervosa. Anxiety disorders were ruled out because whereas Sara endorsed significant anxiety in multiple domains, her worries were specific to acute events surrounding her illness, GI pain, and choking incident. Furthermore, generalized worries, separation, and social anxiety were reported to be secondary to ARFID symptoms. Finally, criteria for anorexia nervosa were not met given the absence of body image concerns or fear of weight gain.
6 Case Conceptualization
A biopsychosocial model can be applied to the development of ARFID for Sara. From a biological vulnerability standpoint, the family denied premorbid mental health diagnoses, including anxiety disorders. Nevertheless, Sara was highly anxious upon presentation, and interactions over the course of treatment indicated that Sara may have historically had an anxious temperament. Furthermore, family history of maternal anxiety may have made her more vulnerable to experiencing heightened anxiety. Anxiety did not result in significant distress or impairment until Sara was presented with the combined biological and environmental stressors of a viral illness and choking in front of peers, respectively. Specifically, Sara experienced stomach pain and nausea which made eating difficult. Despite medical treatment, trepidation related to eating persisted and Sara remained cautious. The unfortunately timed choking incident, coupled with an adverse reaction from peers (i.e., laughing at Sara) exacerbated Sara’s fears associated with eating and resulted in complete avoidance of food and fluid intake. Sara’s interpretation of these events was in line with probability overestimation, insofar as she was convinced that she would choke and be made fun of again if she tried to eat. Thus, restricted eating was reinforcing to Sara, in that immediate anxiety was reduced and feared outcomes were avoided. Her parents also endorsed fears of Sara choking again, which likely reinforced Sara’s own worries. As Sara was initially admitted and treated by the GI service, where providers had limited experience and comfort treating ARFID, the NGT was quickly placed and, consequently, food avoidance was reinforced because the demand to eat was removed. Furthermore, Sara’s parents were negatively reinforced by the NGT, as it decreased urgency associated with eating by mouth and acted as a safeguard from acute health ramifications. NGT dependence was also positively reinforced through increased attention from peers and parents. Thus, treatment focused on increasing oral intake and reducing dependence on NGT feeds.
7 Course of Treatment and Assessment of Progress
Outpatient Treatment
Sara and her parents participated in 16 outpatient therapy sessions over a 12-week period. Initial therapy goals were established, with resumption of normal eating behaviors and weight restoration prioritized. Outpatient progress was evaluated via weekly weights and the amount and variety of nutritional intake consumed per oral (PO).
Family and individual therapy was provided within a cognitive behavioral framework. Family interventions included the following: (a) psychoeducation about ARFID and anxiety, (b) implementing structured and consistent eating expectations, (c) developing a fear hierarchy of previously enjoyed foods and associated anxiety ratings (i.e., subjective units of distress [SUDS]; for example, Kendall et al., 2005), (d) creating a rewards-based contingency management plan to reinforce consumption, (e) conducting in vivo exposures at therapy appointments, and (f) completing food-related exposures between sessions. Selected Coping Cat (Kendall & Hedtke, 2006) modules were used in individual therapy with Sara, including emotion education and awareness; identifying thoughts and feelings; externalizing anxiety as a “worry bully”; and using adaptive coping strategies. In addition, 5 mg/5 mL of liquid formulation escitalopram was prescribed by Sara’s adolescent medicine physician for long-term management of Sara’s anxiety associated with eating and choking, and 6 mL (12 mg total) of liquid hydroxyzine was prescribed for immediate symptom relief as needed.
At therapy outset, Sara was not included at family meals, as her parents worried that Sara could not handle watching others eat. To reinstitute a consistent eating routine, the therapist immediately recommended the inclusion of Sara at all family meals. She would be presented with previously enjoyed foods and would be given a specific consumption goal (e.g., licking, smelling, or taking tiny bites or sips of items with low SUDS ratings). Upon meeting goals, Sara would receive a reward immediately after the meal, including one-on-one time with parents or inexpensive prizes. NGT bolus feeds were given after each meal to mimic normal hunger and fullness patterns.
The therapist recommended that Sara immediately return to school, but Sara and her parents resisted. Sara worried about separating from her mother, was afraid to ride the school bus, and worried that her peers would tease her. Sara’s mother worried that staff would not appropriately manage her enteral feeds, despite their willingness and competency. Consequently, her family opted for half days at school. Sara’s mother drove her to school every morning, escorted her inside the building, and picked her up before lunch.
Outpatient progress was limited. Although Sara licked and swallowed small bites and sips during in vivo therapy exposures, including pudding, chocolates, and animal crackers, progress did not generalize to home. Her parents struggled to consistently implement the contingency management plan. They did not want to upset Sara, particularly given her current struggles, and feared that she could choke again. An additional barrier involved Sara receiving secondary gain for ARFID symptoms, as food refusal resulted in negative reinforcement via shortened school days, car rides to school (as opposed to taking the bus), and eating lunch at home (instead of eating in the cafeteria). Symptoms also fostered one-on-one attention, including alone time with parents during car rides to school and medical appointments, special attention from her mother during times that she would traditionally be at school, and care and concern during enteral feeds (during which Sara clung to her mother). At one therapy visit, Sara expressed worries that health restoration would result in less attention from parents and more teasing from peers. The therapist shared concerns for secondary gain with Sara’s parents and recommended that they minimize attention given to Sara during NGT feeds, reinstate full school days, and remove privileges upon failure to meet consumption goals. Her parents recognized their role in symptom maintenance, yet struggled to implement recommendations.
Totally, 3 months after hospital discharge Sara continued to rely on six bolus enteral feeds per day for 100% of her nutritional needs. A second inpatient admission, this time to the hospital’s Adolescent Medicine service with specialized ED treatment, was recommended to implement a behavioral protocol in the context of a controlled environment. Inpatient medical monitoring could facilitate the safe removal of Sara’s NGT, with monitoring for dehydration and refeeding syndrome. Sara’s parents were in agreement with this recommendation.
Inpatient Admission
Sara weighed 24.9 kg (54.78 lbs) upon admission to the hospital, representing a weight appropriate for her premorbid growth pattern and a 3.1 kg (6.82 lbs) increase since hospital discharge 3 months prior (see Figure 1). At admission, a behavioral protocol was presented to the family, with rewards and consequences to shape the amount and variety of items consumed by Sara. Her parents were encouraged to be present throughout the admission to reinforce the behavior plan and to maximize behavioral generalizability to the home environment. Because the family lived over an hour away from the hospital, they slept in Sara’s hospital room and made accommodations for her older sister to stay with extended family during the admission.
A specialized ED dietitian established a daily caloric goal of 1400 calories (kcals) that would be distributed evenly over three scheduled meals and three snacks per day. Initially, enteral feeds would be administered immediately after meals and snacks to supplement PO intake. As Sara’s PO intake increased via shaping, enteral feeds would be decreased and ultimately discontinued. Sara was given specific consumption goals at each meal and snack, which were to be met within a given time period. Initially, Sara received 5 minutes to meet goals and as quantities increased, the time allotment also increased. Calories from any unmet PO goals would be added to scheduled enteral feeds.
If Sara met PO goals at meals and snacks, positive reinforcement was given. She received immediate praise from parents and milieu staff, selected a toy from a prize basket, and received one-on-one attention from parents during the enteral feed, which was administered by the nurse. Bonus points were rewarded for any bites or sips taken beyond identified goals and could be exchanged for pleasurable activities (e.g., walk to the gift shop with parents, time in the activity room).
If Sara did not meet meal and snack goals, her parents were coached to respond neutrally to minimize secondary gain. They were instructed to verbally externalize Sara’s anxiety (e.g., “The worry bully must be really strong. You can try again at the next meal”) and to leave Sara’s room while the nurse administered the NGT feed (e.g., “We are going for a walk and will be back after you’ve gotten your nutrition”). Her parents returned when the feed was complete and told Sara to rest until the next scheduled meal. Rest was framed as a means of conserving energy. The lights were dimmed, activities and technology were discontinued, and attention was minimized. Sara’s parents were encouraged to remain in her room while she was resting, but were asked to engage in quiet activities and to minimize engagement with their daughter. They were instructed to redirect Sara upon her attempts to engage (e.g., “You need to rest right now. We can talk after your next meal”).
To foster ownership of the plan and to increase parental self-efficacy related to caring for Sara, her parents were coached by the psychologist to (a) determine and record specific consumption goals for each meal, using Sara’s food hierarchy as a guide; (b) order Sara’s meals from room service 30 minutes before scheduled meal times (as opposed to the traditional milieu approach in which staff orders patient meals); (c) present Sara with her tray and review specific goals prior to each meal; (d) prompt Sara to begin eating; and (e) end the meal after the allotted time.
On Hospital Day 1, Sara’s goals included eating small bites of popsicles and pudding, which had low SUDS ratings on her food hierarchy. At the first meal, she ate three bites of a popsicle. Praise was given to positively reinforce her efforts. Sara was visibly excited about the accomplishment. At bedtime snack, Sara’s goal was to take a full bite of pudding. She licked the pudding but disliked the texture and refused to eat more. In line with the behavior protocol, her parents ended the meal after 5 minutes and left Sara’s room while the nurse administered the NGT feed. Her parents returned after the feed, turned off the TV, and told Sara to rest. Sara began to cry, yet her parents remained calm and firm. Sara complied and her parents exhibited newfound confidence. They remained in Sara’s room and reinforced the plan by turning out the lights and going to sleep early. On Hospital Day 1, 19.07 % (267 kcals) of Sara’s nutritional intake was met PO (see Figure 2).
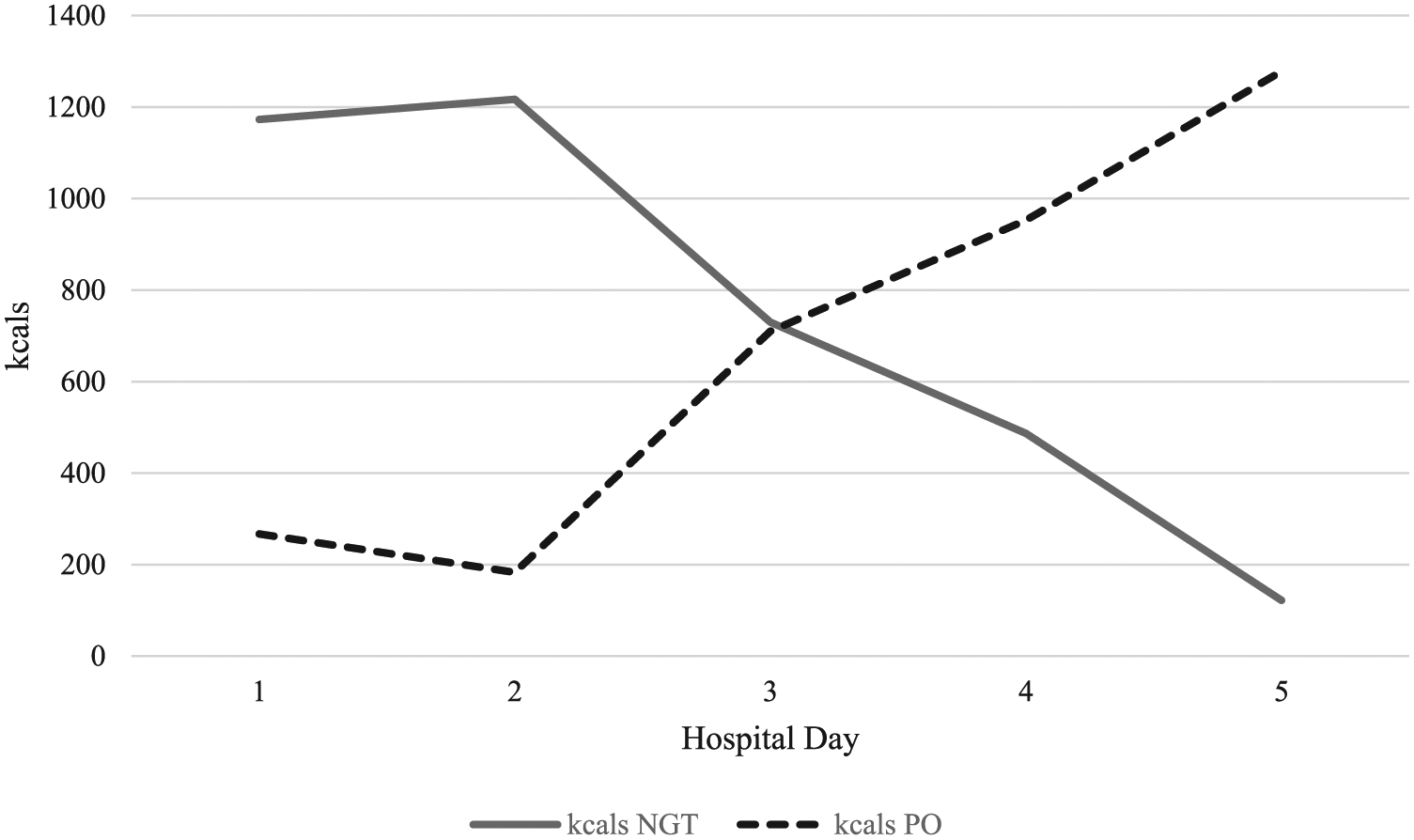
Total calories (kcals) consumed enterally (NGT) and PO.
Sara successfully completed all goals on Hospital Day 2, eating increasingly more bites of popsicles and swallowing a spoonful of pudding, despite associated discomfort. On Hospital Day 3, crackers and Boost supplement were introduced. Sara expressed fears of choking and disliked the texture of the items. Rest was instituted twice but by the end of the day, Sara had drunk sips of Boost, licked crackers, eaten bites of pudding, and consumed entire popsicles. She significantly increased her PO intake, with 50.71% (710 kcals) of total nutrition consumed by mouth on Hospital Day 3. Her parents were increasingly enthusiastic about the protocol and were proud of Sara’s progress.
On Hospital Day 4, goals included bites of mashed potatoes and larger quantities of Boost. Despite her trepidation, Sara successfully met all demands and consumed 68.07% (953 kcals) of total intake by mouth. Sara’s ongoing progress prompted removal of the NGT on Hospital Day 5. Although Sara worried that she would not be able to maintain her success, her parents and the medical team expressed support and certainty that she could continue standing up to the “worry bully.” Upon NGT removal, Sara was expected to drink four ounces of Boost and take bites of specific foods at each meal and snack. By the end of the day, Sara had eaten 100% of her nutritional requirements PO without requiring any rest. She consumed 91.29% (1278 kcals) of her meal plan and consumed a number of new foods, including bites of macaroni and cheese, Fruit Roll-Ups, chocolate ice cream, and a cheese stick.
Sara was discharged on Hospital Day 6. A behavior plan was created by Sara’s family and the psychologist prior to her discharge, including expectations that Sara complete 100% of PO goals at each meal and snack. Sara would only be allowed to meet 50% of daily caloric needs through liquids. Rewards would be earned for meeting nutritional expectations and integrating feared foods. Noncompliance would result in bed rest, characterized by no engagement in activities and minimal attention to limit secondary gain. Rest was framed as a natural consequence of restriction insofar as energy conservation would be prioritized if Sara did not complete meals and snacks. She would return to school full-time and would eat lunch in the cafeteria. If she did not complete her lunch at school, she would rest after school until dinner time. Sara’s parents expressed confidence in implementing this plan, given their ability to successfully reinforce a similar plan during the admission. Sara was excited to try foods that she enjoyed in the past and even asked parents if they could stop for French fries on the drive home from the hospital. Although she expressed worries about eating challenging foods and attending school, Sara expressed confidence in her ability to face her fears and use coping skills. At discharge, Sara’s weight was 24.9 kg (54.78 lbs), consistent with her admitting weight (see Figure 1).
8 Complicating Factors
In Sara’s case, initial outpatient treatment was complicated by the NGT placement during her first hospitalization. Use of enteral feeds facilitated ongoing nutritional avoidance with minimal consequences. Specifically, Sara received secondary gain when she did not eat, as evidenced through increased positive attention from parents and avoidance of feared situations, like riding the bus and eating in the cafeteria. Parental struggles with limit setting also interfered with the successful implementation of outpatient interventions. It is notable that Sara’s parents recognized these challenges and were motivated to address them. They were onboard with a second admission and welcomed additional support in a nondefensive manner.
9 Access and Barriers to Care
For many youth with EDs, access to evidence-based treatment is limited given the highly specialized nature of care for EDs and ARFID, in particular. In this case, Sara and her family were fortunate to have access to a medical team consisting of physicians, nurses, and dietitians with experience in EDs; a highly specialized ED psychologist with behavioral expertise; and providers comfortable with treating ARFID. It is noteworthy that even within an institution with a comprehensive pediatric ED program, Sara’s initial care and hospitalization was managed by GI. The institution’s ED program was not consulted until medical problems had been ruled out. By that time, Sara was not consuming anything PO, was dehydrated and medically hospitalized, and an NGT was placed. In our experience, lack of education about and experience in treating ARFID among medical providers can result in delayed diagnosis. Furthermore, in Sara’s case, rapid placement of an NGT without the initiation of behavioral interventions to target food avoidance inadvertently reinforced her illness symptoms. Rather than requiring Sara to face her fears by eating and drinking with use of a contingency management plan, the NGT facilitated her avoidance of feared outcomes (i.e., choking and pain) and reduced parental urgency to set firm limits around eating.
An important consideration for implementing the described intervention is the need for a controlled, inpatient environment staffed with a milieu experienced with EDs and family-based behavioral interventions. In Sara’s case, the inpatient environment provided Sara’s parents with repeated opportunities to implement and reinforce the intervention. Milieu staff provided her parents with an abundance of praise, support, and modeling of effective limit setting. Thus, parental self-efficacy was improved and likely maximized behavioral generalizability to the home environment.
Potential barriers also include a myriad of direct and indirect costs associated with mental health interventions. For Sara, indirect barriers included a round-trip travel time of 3 hr to our institution, missed school, transportation barriers and costs, and child care needs for Sara’s sister. Direct barriers included financial costs associated with multidisciplinary care. At symptom onset, extensive, costly medical testing ruled out medical conditions. Diagnosis of ARFID and provision of specialized ED care was delayed, resulting in more health care utilization. Fortunately, Sara’s family had extensive community support, received help with child care, and were provided with meal and gas cards from our institution. Her parents were encouraged to stay overnight in her hospital room, which minimized lodging costs, while concurrently integrating them into the intervention.
10 Follow-Up
Sara and her parents completed six additional outpatient therapy sessions after her discharge. In the first week home, she willingly tried pizza, ravioli, baked chicken, green beans, and cornbread. Although she was initially anxious, she used coping skills and remained motivated. Sara returned to full school days, rode the school bus, and played with peers, with minimal resistance. Therapy was terminated after 2 months, given full remission of ARFID symptoms and ongoing maintenance of a healthy weight. Around 4 months after discharge, Sara had grown 2.9 cm since her initial hospitalization, 7 months prior. Her weight had increased to 26.5 kg (58.3 lbs), placing her body mass index (BMI) in the 52nd percentile (see Figure 1).
11 Treatment Implications of the Case
This case study describes a child who developed ARFID after a GI illness and subsequent choking incident. Initially, medical providers focused solely on evaluation of potential organic causes of her symptoms, consulting mental health professionals only after medical causes of restricted intake were ruled out. That approach, coupled with rather quick placement of an NGT, contributed to prolonged dependence on the NGT by inadvertently decreasing the family’s sense of urgency associated with eating orally and facilitating avoidance of Sara’s emotional distress.
Implementation of a consistent behavioral protocol prompted rapid results. Sara’s symptoms dramatically improved within 5 days, from complete reliance on enteral feeds at admission to 100% PO intake at discharge. Inclusion of Sara’s parents was crucial, as intensive parent coaching greatly bolstered their confidence. Furthermore, providing unwavering expectations and implementing consequences acted as an exposure for Sara’s parents. They learned that Sara could eat feared foods, would eventually calm down if she became upset, and could eat a variety of foods without choking. With repeated protocol implementation, their own fears extinguished and Sara’s successes were reflected in her newfound confidence.
It’s noteworthy that upon “getting over the hump” of eating feared foods without choking or pain, Sara’s anxiety dramatically reduced and her willingness to try more diverse foods increased. This was apparent following discharge, when Sara willingly and rapidly increased the variety of foods she consumed. As such, in the treatment of ARFID, it may be the case that successful completion of initial eating-related exposures prompts rapid generalization to other avoided foods.
12 Recommendations to Clinicians and Students
This case supports the use of a behavioral intervention in an inpatient medical setting to decrease NGT dependence and improve oral intake in patients with an anxiety-based, avoidant type of ARFID. While outpatient treatment may be sufficient for some youth with ARFID, this case supports the use of a more intensive intervention when sufficient progress is not achieved in an outpatient setting. In this regard, a number of recommendations for clinicians and students can be generated from this case.
This case demonstrates the need for interdisciplinary evaluation and application of the biopsychosocial model to children and adolescents who present with decreased oral intake. Although it is critical that youth are thoroughly assessed by a medical team to rule out organic causes for presenting complaints, for youth with acute food refusal, mild malnutrition, or dehydration manageable via IV fluids, it is plausible that rapid mental health intervention, coupled with the delay of NGT placement, could promote improved parental and youth engagement in behavioral treatments. As with Sara, NGT placement could prolong illness symptoms and consequences, inadvertently reinforce avoidance of unpleasant demands for patients and families, and promote unnecessary health care utilization and costs. Thus, early intervention by mental health providers is strongly recommended. Finally, admission to a higher level of care treatment, offering specialized care within a controlled environment, is worth considering if patients are not making progress in outpatient care.
Footnotes
Acknowledgements
The authors acknowledge the cooperation of Sara and her parents.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.