
Abstract
The fear of vomiting (i.e., Emetophobia) causes substantial distress for affected individuals, and is associated with hypervigilance to somatic sensations, panic attacks, and behavioral avoidance. Interventions for Emetophobia have traditionally relied heavily on exposure to vomit, vomiting, and vomit-related cues, providing some challenges in identifying appropriate graded exposures for Emetophobia due to medical and hygiene concerns. Recent efforts have been made to treat psychopathology transdiagnostically; however, very few efforts have been made to reduce Emetophobia symptoms in such a fashion, without the explicit use of vomit-related exposures. The current case study describes the cognitive-behavioral, transdiagnostic treatment approach utilized to treat a young woman with Emetophobia. We report significant symptom reduction at the end of therapy, as well as at a 7-month follow-up. The current study provides further evidence that emetophobia can be effectively resolved utilizing transdiagnostic strategies and without direct exposure to vomit or vomit-like stimuli.
1 Theoretical and Research Basis for Treatment
The fear of vomiting (i.e., Emetophobia) has been defined and recognized as a clinical construct for a number of years, and has an estimated prevalence rate of approximately 2% in men and 7% in women (Van Hout & Bouman, 2006). Emetophobia causes substantial distress for affected individuals, and is associated with hypervigilance to somatic sensations, panic attacks, and behavioral avoidance. In addition to immediate symptoms and discomfort, there is evidence that this fear may have lasting impact on affected individuals’ larger life decisions. Recent work suggests a substantial proportion of women experiencing Emetophobia choose to postpone having children or avoid having children all together due to anxiety associated with the anticipation of morning sickness (Veale & Lambrou, 2006).
Although a number of case studies have documented successful symptom reduction with few instances of relapse using exposure-based, and cognitive-behavioral, treatment strategies (e.g., Ahlen, Edberg, Di, Schiena, & Bergström, 2015; de Jongh, 2012; Graziano, Callueng, & Geffken, 2010; Hunter & Antony, 2009; Maack, Deacon, & Zhao, 2013; Paulus & Norton, 2016; see also Riddle-Walker et al., 2016, for a cognitive behavioral randomized control study), Emetophobia remains a difficult disorder to treat. Fix, Proctor, and Gray (2016) utilized cognitive strategies, such as challenging distorted thoughts about vomiting, and graded exposure to vomit-related stimuli (e.g., videos of other people vomiting) to successfully reduce emetephobic symptoms in an adolescent girl. Similarly, Maack et al. (2013) utilized a predominately exposure-based treatment to target Emetophobia in an adult woman. The authors reported that the client showed significant symptom reduction after engaging in exposure exercises that included viewing two of her therapists vomit, inducing her own gag response, and causing herself to vomit. Similar treatment strategies, all relying on significant exposure to actual vomit, vomiting, and vomiting cues, have been reported in a number of other published case studies (Graziano et al., 2010; Hunter & Antony, 2009).
Previous successful interventions have relied heavily on exposure to vomit, vomiting, and vomit-related cues; thus, it can be challenging to identify appropriate graded exposures for Emetophobia due to medical and hygiene concerns. While an individual with a fear of snakes may eventually work up to safely interacting with a snake, it has been argued that inducing vomiting or even a gag response in a psychotherapy client is potentially unethical for a therapist without medical training, and could lead to unintended health consequences for the client (e.g., Wolitzky-Taylor, Viar-Paxton, & Olatunji, 2012). Although therapists have successfully utilized creative strategies for simulating vomit and vomiting (e.g., Hunter & Antony, 2009), it would be beneficial to both the client and the clinician if the reduction of vomit-related anxiety could be accomplished without inducing or simulating vomit or vomiting. This point seems particularly important, as prior studies suggest that, across treatments for phobias in general, clients with Emetophobia have much higher dropout rates, in part because of the clients’ strong reaction toward the prospect of vomiting as part of treatment (Boschen, 2007).
A potential work-around for these difficulties is to desensitize an individual by exposing them to other, co-occurring cues. The expectation is that learned tolerance and coping skills would then generalize to real life exposure to actual vomit and vomiting. Relatedly, clinical psychology has recently begun to place much greater emphasis on utilizing transdiagnostic treatment strategies to address psychopathology. Such therapeutic approaches aim to treat the underlying physiological and psychological processes that cut across diagnostic categories (Kring & Sloan, 2009) rather than creating disorder specific treatments because evidence suggests such shared processes likely account for the substantial comorbidity of diagnosis in many psychiatric patients (Watson, 2005). For these reasons, the National Institute of Mental Health has suggested an alternative framework for the clinical conceptualization and research of psychopathology (i.e., RDoC, Insel et al., 2010) and is encouraging the use of this approach when developing treatments and making decisions about patient care. The RDoC framework promotes the study of correlates of symptomology transdiagnostically (e.g., recklessness, regardless of clinical diagnosis), instead of researching specific diagnoses (e.g., attention deficit hyperactivity disorder [ADHD] vs. antisocial personality disorder). In the context of anxiety, it has been suggested that “defensive reactivity” (e.g., startle response) underlies all fear-based disorders, regardless of specific diagnostic category (Lang, McTeague, & Bradley, 2016). In other words, while the feared stimulus may differ across patients (e.g., social anxiety related to social stimuli; Emetophobia related to vomit stimuli), the basic underlying process of heightened startle responsivity is likely a key physiological factor contributing to anxiety, more generally.
Furthermore, it has been suggested that diagnosis-specific treatment protocols do not easily accommodate the diagnostic co-morbidities that frequently present in clinical settings (Farchione et al., 2012). For instance, if a client presents with clinically significant symptoms of depression and generalized anxiety, it can be difficult to ascertain which disorder to treat first. Similarly, attempts to combine components of independent treatments to address comorbid conditions may influence their effectiveness. In the case of Emetophobia, a low incidence diagnosis, it is likely not practical for clinicians to be trained on a specific individual treatment protocol. Extant evidence suggests Emetophobia is highly comorbid with other anxiety disorders particularly panic disorder and generalized anxiety disorder (Sykes, Boschen, & Conlon, 2016), and that specific characteristics such as acute awareness and negative interpretation of internal physiological cues may account for this relationship. Paulus and Norton (2016) have demonstrated that addressing anxious symptoms more generally while still including vomit-related exposure items is helpful to ameliorating Emetophobia. More recently, Bogusch, Moeller, and O’Brien (2018) also reported an effective course of therapy for Emetophobia without the use of explicit vomit cues. Thus, treatment of Emetophobia may benefit from a more transdiagnostic approach.
However, the application of transdiagnostic treatments in clinical practice has gotten off to a slow start, particularly with regard to treating lower prevalence disorders such as Emetophobia. For this disorder, very little outcomes research is available using a transdiagnostic approach. Paulus and Norton (2016) described the successful treatment of a young women suffering from vomit-related anxiety using a transdiagnostic cognitive-behavioral approach for anxiety. The authors successfully utilized basic cognitive-behavioral strategies (e.g., cognitive restructuring, exposure to feared stimuli) to challenge maladaptive thoughts and improve coping even though only limited vomit-specific stimuli were used during exposure exercises. In addition, although the authors demonstrated significant symptom reduction in a short period of time, longer term follow-up data was not reported, so it remains unclear if such a transdiagnostic approach produces similar long-term results comparable with treatments utilizing vomit specific exposures.
Because of the unique barriers to treating vomit phobia (e.g., concerns about potential injury, low incidence diagnosis leading to lack of clinician familiarity with treatment, high disgust factor for treating clinician), it seems important to explore the effectiveness of a general transdiagnostic treatment approach with little to no actual exposure to vomit and vomiting. Such a treatment approach would be expected to effectively reduce not only the specific symptoms of Emetophobia but also the symptoms of any co-occurring anxiety disorder(s). Such a treatment would benefit both the patient, in that less distressing stimuli could be used during exposure sessions, and also the average clinician, who does not have medical training and likely does not have extensive experience treating individuals with this condition.
Accordingly, the current case study describes a young-adult woman who presented with Emetophobia and whose case was conceptualized and treated using a broad, transdiagnositic, cognitive-behavioral approach toward anxiety, without the addition of any explicit vomit-specific stimuli.
2 Case Introduction
The following de-identified case example presents a patient treated by the first author (an advanced graduate student in a clinical psychology program) and supervised by the second author (a licensed clinical psychologist) at a university-based outpatient training clinic. Modifications of specific case details were made to protect patient confidentiality.
At treatment initiation, Mary was a 19-year-old Caucasian female enrolled full-time in a bachelor’s degree program. She held a part-time job, lived with several female roommates, and had a long-term boyfriend who she described as supportive.
3 Presenting Complaints
At intake, Mary described her primary concerns of frequent panic attacks and generalized anxious symptoms. Upon interview, a strong fear of vomiting was also revealed. The incident precipitating her seeking treatment was a severe panic attack that caused her to seek medical attention while on a recent family vacation. Mary described feeling nauseous after eating lunch, which caused her to worry that the nausea would worsen, that she would become seriously ill and would vomit. She spent a number of hours in a public restroom until emergency medical services arrived and determined that she was not seriously ill. Mary had experienced strong fears of vomiting since middle childhood, but had never sought psychological or medical treatment to manage these symptoms. In addition, since enrolling in college, Mary had experienced an increase in anxiety related to her academic performance. She noted that general increases in stress tended to exacerbate her Emetophobia symptoms. She maintained a very high grade point average (GPA), and frequently worried about her grades. At the time treatment began, she had recently withdrawn from a course due to poor performance. The course was required for her degree program, and she worried about her ability to successfully complete the course in the next semester. In addition, Mary had concerns about her ability to manage the stress associated with a very difficult class.
4 History
She reported a close relationship with her family, but noted that she grew up in a very small town and was happy to be more independent while attending college. Reportedly, her father had a long-standing history of anxiety, including ongoing health-related anxiety (e.g., concern about using public restrooms) that often interfered with his ability to leave his home. She reported that her family was generally accommodating of her father’s limitations in an effort to prevent the escalation of his anxious symptoms. Mary indicated that observing how her father’s health-related anxiety negatively impacted his life motivated her to seek treatment for her own concerns.
5 Assessment
Psychopathology and Personality
Personality Assessment Inventory (PAI)
The PAI is a self-report tool designed to assess broad-range psychopathology (e.g., anxiety, depression, trauma, and borderline traits) and provides information regarding treatment planning (Morey, 1991). Raw scores are converted to T scores with an average of 50. Scores at or above 70 are considered clinically elevated. The PAI has established high levels of reliability, internal consistency, and stability (for the full scales, generally in the .80s, and subscales in the .70s; Morey, 2007). The PAI was administered during the initial intake session only to establish baseline personality and psychopathology. This clinic does not have clients re-take the PAI upon completion of treatment, and therefore, follow-up data for the PAI are not available.
Diagnostic Interview
SCID-5
The SCID-5 is a semi-structured interview that assesses major psychopathology classifications and enables clinicians to make diagnoses (First, Williams, Karg, & Spitzer, 2015). The SCID-5 has demonstrated high internal consistency (above .80), test–retest reliability, and predictive validity (Shankman et al., 2018). The SCID-5 was administered as part of the intake interview.
Overall Symptoms
OQ®45.2
The OQ®45.2 is a 45-item self-report outcome/tracking instrument designed for repeated measurement of client progress through the course of therapy and following termination (Lambert et al., 1996). The OQ®45.2 was designed to assess three domains of patient functioning: symptoms of psychological disturbance (e.g., depression, worry, and physiological anxiety symptoms), interpersonal problems, and social role functioning. Total scores, reflecting general distress, range from 0 to 180. The OQ®45.2 total score has established excellent internal consistency (.93; Lambert, Gregersen, & Burlingame, 2004). This measure was administered at intake and prior to each session. Consistent with her self-report during the intake session, Mary endorsed a significant number of anxiety symptoms (e.g., worry, physiological arousal/discomfort) on the OQ®45.2.
Vomiting Anxiety
Specific Phobia of Vomiting Inventory (SPOVI)
The SPOVI is a 14-item self-report measure of vomit phobia (Veale et al., 2013). Each item is rated on a Likert-type scale from 0 (not at all) to 4 (all the time). The SPOVI consists of two subscales, one assessing Avoidance to vomit-related stimuli, and the other assessing Threat Monitoring of vomit-related stimuli. The SPOVI has demonstrated good internal consistency (.89), as well as convergent and divergent validity (Maack, Ebesutani, & Smitherman, 2018). The SPOVI was administered prior to the first therapy session, and approximately every other week thereafter to assess change in symptoms related to vomit phobia.
6 Case Conceptualization
Although Mary’s initial presenting concern was the frequent occurrence of panic attacks, further discussion revealed that feelings of nausea and/or other stomach disturbances were the primary trigger of these panic-like episodes. Interestingly, this client interpreted almost any physical sensation experienced “between the nose and the knees” as an indication that she was becoming ill and would vomit. Mary reported that her daily activities were frequently and significantly impacted by her worry about vomiting and experiencing panic attacks. For example, Mary indicated she always sat on aisle seats in lectures to enable her to easily exit in case she felt nauseous. She also made sure she could immediately identify the nearest restroom in all classroom buildings so she could access them quickly if necessary. Mary reported significant concern about vomiting in a public place which would lead to embarrassment. Eating at restaurants, eating unfamiliar foods, and eating foods she had not prepared herself triggered repetitive thoughts of becoming ill. In general, Mary attempted to avoid such situations which severely restricted her social interactions and interfered with her relationships. When unable to avoid restaurants or eating in public, she typically became quite anxious, did not eat, and often fled from the situation.
In addition, Mary ate a bland and very limited diet, avoided broad categories of food she felt would make her ill (e.g., sushi, Mexican food), and did not drink alcohol because of fear of becoming nauseous and/or vomiting. Although at the time of treatment Mary was below the legal drinking age, she indicated that her aversion to alcohol made socializing difficult during her freshman year of college. Mary often skipped meals or ate very little due to concern about upsetting her stomach. She also evinced repetitive behaviors such as scrupulously checking the expiration dates on food items to avoid eating spoiled food. Mary acknowledged that many of the foods she discarded were unlikely to elicit illness (e.g., “a day old muffin”) but she threw them away, nonetheless. Resultantly, she noted that she spent more time and money on grocery shopping each week than other people she knew who did not have such stringent guidelines about food expiration.
A significant portion of her day was spent attending to bodily sensations to monitor the possibility of vomiting. She suggested that nearly all bodily sensations (e.g., hunger pang, headache, and muscle tension) caused anxiety because they indicated she might vomit. Similarly, Mary interpreted symptoms of physiological anxiety (e.g., “butterflies in her stomach” before a final exam) as a sign of vomiting, and would become even more anxious. She also avoided foods that she believed would produce uncomfortable somatic sensations such as carbonated beverages, spicy foods, and eating a larger volume of food. In addition to food avoidance, Mary avoided all moderate to strenuous exercise out of fear that it would result in vomiting and felt strongly that she would never have children because of the potential for nausea and vomiting during pregnancy. Finally, although Mary endorsed a strong interest in a medical career, she doubted her ability to achieve this goal because of her vomit-related anxiety. At the time of intake, she volunteered at a local hospital and was frequently uneasy and anxious about encountering a nauseous or vomiting person during the course of her duties.
Mary became anxious about vomiting during childhood after a stomach virus spread rapidly through the other children at her summer sleep-away camp. Although Mary herself did not become ill and was kept apart from the other campers, she spent the time until her parents could retrieve her in a heightened state of anticipatory anxiety, attending to bodily sensations that might indicate vomiting was unavoidable. After this experience, Mary frequently slept on the bathroom floor in her home in case she became sick and needed to vomit. Although at the time she presented for treatment, Mary had not vomited in many years, she continued to sleep in the bathroom as an adult when she detected certain bodily sensations or had eaten certain foods. In addition, she reported her belief that particular food items would cause her to vomit was related to an experience of vomiting several hours after eating chocolate cookies as a young adolescent. Since then she avoided eating chocolate cookies and became convinced that certain food items invariably caused nausea and vomiting.
In addition to Emetophobia, Mary endorsed significant symptoms of generalized anxiety disorder, with particularly strong fears surrounding her academic performance and ability to manage her time, despite good grades, good work performance, and positive feedback from others. Mary had several physiological symptoms of generalized anxiety, as well (e.g., headaches, muscle tension). She also met diagnostic criteria for social anxiety disorder, was generally concerned about how others’ evaluated her, and tried to avoid feeling embarrassed whenever possible. These fears were prevalent in several areas of her life and included a marked difficulty expressing opinions and asserting herself in personal relationships, avoiding relationships to avoid rejection/criticism, and difficulty answering questions and participating in class discussions. Although Mary’s presenting concern related to symptoms of panic, these experiences were secondary to her symptoms of Emetophobia, and therefore did not warrant a diagnosis of panic disorder. She did have acute periods of intense distress related to vomiting, but these did not meet diagnostic criteria for panic attacks.
Mary endorsed a variety of anxiety symptoms, including symptoms consistent with social anxiety, generalized anxiety, specific phobia, and panic. Mary’s primary concern and reason for seeking treatment directly related to a specific fear of vomiting (Emetophobia) and the significant, panic-like distress that ensued as a result. For this reason, Emetophobia was Mary’s primary diagnosis.
7 Course of Treatment and Assessment of Progress
Mary’s primary goals for treatment included reducing overall anxiety levels, managing school-related stressors, and reducing specific anxiety and panic-like symptoms related to vomiting. She also expressed an interest in addressing anxiety related to social interactions. Given Mary’s interest in addressing anxiety broadly, with a specific emphasis on Emetophobia, a transdiagnositic cognitive-behavioral approach was taken in her treatment planning. The specific topics addressed throughout treatment are detailed below, and presented as four “phases” based on the content covered across these session clusters. The total course of treatment for anxiety symptoms and stress management was comprised of 46 sessions. The first 10 sessions focused on the physiological sensations related to Mary’s panic-like symptoms. Sessions 11 to 46 addressed symptoms more specifically related to Emetophobia, social anxiety, and assertiveness. At the end of 46 sessions, termination was discussed as no significantly impairing anxious symptoms remained. At this time, Mary indicated that she had additional treatment goals related to interpersonal functioning within her relationships and chose to create a new treatment plan and continue in therapy. This new treatment plan did not address Emetophobia or other specific anxious symptoms. Symptoms of and associated with Mary’s experience of Emetophobia were the primary focus of treatment for the first 46 sessions. The client had ongoing interpersonal difficulties with a romantic relationship, and with academic performance, which occasionally took precedence over Emetophobia symptoms. For instance, Mary had ongoing conflicts in her relationship, and would occasionally choose to prioritize these concerns in session, while continuing to do exposure activities outside of session. These “stressor sessions” contributed to the overall number of sessions. Administration of outcome measures was conducted in the last 5 min of each session.
Phase 1: Psychoeducation, Treatment Planning, and Behavioral Activation
Sessions 1 to 10
The primary focus of Phase 1 was to provide psychoeducation about anxiety from a transdiagnostic perspective, develop treatment goals, and initiate behavioral activation strategies to reduce Mary’s overall level of distress. Using a biopsychosocial perspective, it was explained that genetic makeup, environment, and social context all influence experiences of anxiety. Mary’s various, specific experiences of anxiety (e.g., vomit related, social, academic) were explored in the context of an anxious temperament, likely influenced by family predispositions to anxiety. In addition, discussions centered on her family context explored how anxious thoughts were likely supported and reinforced by her father’s modeling of health-related anxiety and safety behaviors, and other family members’ supporting/enabling behaviors. Phase 1 also introduced a cognitive model of anxiety emphasizing that the thoughts and subsequent emotional responses related to certain events may or may not be accurate and could be reinterpreted or modified in response to other information. This model was specifically applied to thoughts and expectations about vomiting, although discussion of the cognitive model was also applied to Mary’s ongoing worry about academic performance, social anxiety, and generalized anxiety.
Because Mary reported academic concerns, difficulty with time management, and that she had stopped engaging in certain activities because of anxiety, these initial sessions also emphasized behavioral activation and effective time management. With assistance from the therapist, Mary created weekly schedules to ensure progress on her school work. Mary recognized that she had a tendency to “overload” certain days of her week (e.g., leave a lot of work to get done over the weekends), but would rarely get it done due to other scheduling conflicts (e.g., volunteer positions). She and the therapist worked to schedule realistic goals for each day. This scheduling improved Mary’s overall productivity, and subsequently reduced her general academic anxiety. Behavioral activation was also utilized to ensure she was engaging in enjoyable activities. Mary had substantially reduced her enjoyable activities because she felt very anxious engaging in them when she had school work to do. By maintaining a school schedule, and scheduling in relaxation/recreation, Mary felt less anxious about her academic responsibilities and performance overall.
Basic relaxation strategies (e.g., breathing exercises) were also taught to manage general symptoms of over-arousal. Mary noted that as her baseline level of anxiety decreased, she began to focus less on internal physiological states, and subsequently spent less time ruminating about vomiting. At this point, the thought of vomiting was still quite distressing, but she reported experiencing such thoughts less frequently.
Phase 2: Exposure-Based Exercises
Sessions 11 to 22
Phase 2 focused more specifically on psychoeducation related to Emetophobia, including an overview of the interoceptive components of vomit and health-related anxiety. Mary’s tendency to misinterpret common somatic experiences as likely dangerous or indicative of nausea and vomiting was discussed. In an effort to learn that somatic symptoms do not necessarily lead to vomiting, Mary was asked to complete interoceptive exposure exercises in session and for homework. Examples of these exposures included spinning in circles, jumping jacks, breath holding, running in place, and push-ups. While couched in the context of vomit-related fears, interoceptive exposure exercises also aimed to reduce Mary’s experience of panic-like symptoms.
Mary was also asked to generate a list of gastrointestinal somatic experiences (e.g., hunger pang, fullness, “nerves”) and describe in detail what those experiences felt like, and how they felt different from nausea. Mary was challenged to label these somatic experiences, as she felt them, as homework to better discriminate her internal states and reduce generalization of physiological symptoms to nausea.
After interoceptive exposures were introduced, a fear hierarchy was created that was more specifically related to Emetophobia and emetephobic cues (see Table 2 for an example of fear hierarchy). A traditional systematic desensitization format was utilized for this component of treatment. Mary was asked to complete an activity on her fear hierarchy at least 3 times a week, in between therapy sessions. She began with the least anxiety-provoking situations, and eventually worked up to the most anxiety-provoking. She selected specific activities to engage in over the week in session. Mary completed and brought to session a weekly log of exposure-activities and anxiety-ratings related to each exposure activity.
While vomiting was listed as the most anxiety provoking experience on the fear hierarchy, Mary was explicitly told that she would not be required to actually vomit or simulate vomiting. Rather, in vivo exposure exercises on the fear hierarchy related to other activities and sensations Mary avoided because of emetephobic concerns.
Several notable events occurred during Phase 2. First, Mary showed a slight increase in SPOVI score during Week 18 (from a 4 to an 8) after eating dinner at a restaurant. Eating at an unfamiliar restaurant was part of Mary’s exposure homework for the week. This was used as an opportunity to discuss the fact that, despite feeling anxious, Mary did not become sick after eating dinner. Similarly, it was highlighted that eating an unfamiliar food did not produce nausea. Mary reported feeling angry that her anxiety interfered with her ability to enjoy her dinner out, and felt discouraged by her continued tendency to spend time in the bathroom “just in case” she became sick. Mary’s frustrations were validated and re-framed to maintain motivation for treatment, and she was commended for completing in-vivo exercises despite heightened anxiety.
Second, Mary completed an assigned in vivo exposure of eating left-over food during Week 20. Her family was visiting during this week, observed her eating left-over food, and expressed great concern that she might become sick and vomit because of this. Mary reported that her family’s anxiety about her eating left-overs sounded “ridiculous” when she heard it expressed out loud, and she ate the food anyway. She did not become ill or experience any negative consequences of eating the left-over food. This experience seemed to be particularly impactful for Mary. Not only was she able to experience eating a left-over food without becoming ill, but she also experienced a fairly dramatic shift in her beliefs about the potential dangers of eating left-over food.
Third, during Week 22, Mary had a chance encounter with an individual who reported feeling nauseous. Mary was interested in the medical field, and began engaging more with a hospital volunteer experience as therapy progressed. Although she reported an increase in anxiety throughout the situation, this provided an opportunity to discuss the fact that Mary did not become sick just from being around this individual. This also allowed for a conversation regarding the difference between Mary’s anticipated anxiety and experienced anxiety, while interacting with a nauseous person. While she previously estimated that this experience would be almost unbearable, she was able to remain in the situation without overwhelming distress.
Because Mary also endorsed social anxiety during the intake interview, Mary was encouraged to engage in exposure-based exercises to address specific social concerns. She generated a separate fear-hierarchy related to social anxiety on her own, and would periodically provide updates to the therapist on how well this strategy was working to reduce her anxiety.
Phase 3: Challenging Cognitive Distortions
Sessions 23 to 30
Mary continued to complete in vivo exposures from her Emetophobia hierarchy throughout Phase 3. In addition, the cognitive model of anxiety was re-visited to address thoughts specifically related to Emetophobia. This discussion revealed Mary held various distorted beliefs about vomiting, such as “if my stomach hurts, it means I will vomit” and “exercising leads to vomiting.” She engaged in thought-challenge exercises (including the completion of thought records) identifying the likelihood of vomiting in various situations, and generating evidence for and against her thoughts. Mary also identified “worse case scenarios” associated with vomiting and evaluated her ability to handle these scenarios. She acknowledged that although vomiting would be very unpleasant, the likelihood of her vomiting on a daily basis was very low, and the likelihood of something bad happening as a result (e.g., choking, humiliation) was also very low. Mary was able to generalize and apply these cognitive strategies to other areas of her life as well. For instance, she acknowledged that the thought, “If I don’t get a 4.0 GPA I will never get into medical school” was likely exaggerated, and was able to modify this thought to incorporate a more balanced perspective. She reported considerably less worry about her academic performance during this phase of treatment.
During Phase 3 (Session 30), Mary had another chance encounter with an individual who was actively vomiting (at her medical volunteer position). As a part of her volunteer service, she was required to interact with this person. Mary reported during the session after this experience that, although quite unpleasant, her anxiety level was only at a 5 or 6 out of 10. In the past, when asked to rate a hypothetical situation of being around someone who was vomiting or seeing actual vomit, Mary reported that her anxiety would likely be a 9 out of 10.
Phase 4: Applying Cognitive and Exposure-Based Strategies to Socially Relevant Fears
Sessions 31 to 46
During Phase 4, Mary reported that she was experiencing “significantly less worry about vomiting” and felt that this anxiety was no longer disrupting her life. As an example, she reported that she was around an ill family member and did not notice an increase in anxiety at all. In addition, she reported during a final session that she overate “greasy” food and actually felt nauseous, but did not feel any anxiety. At this point, it was mutually agreed to shift the focus of treatment away from emetephobic concerns. The final treatment sessions incorporated the learned, transdiagnostic strategies (e.g., exposure, challenging cognitive distortions, behavioral activation) to address concerns about social evaluation anxiety and general interpersonal functioning.
Pre- and posttreatment symptom inventory scores are presented in Table 1, and an example of the fear hierarchy generated is presented in Table 2. Mary scored a 72 on the OQ assessment during the intake session, indicative of elevated distress levels (e.g., low mood, high anxiety, impaired social functioning). Similarly, she endorsed elevated levels of anxiety on the PAI, particularly noting concerns with anxious rumination (Cognitive Anxiety scale) and feeling distressed by symptoms of anxiety (Emotional Anxiety scale). By the end of treatment, Mary’s OQ score dropped down to 26, which falls below the range of the average individual in outpatient treatment. This reflects a substantial decrease in overall psychological distress, including generalized anxiety.
Pre and Posttreatment Scores.
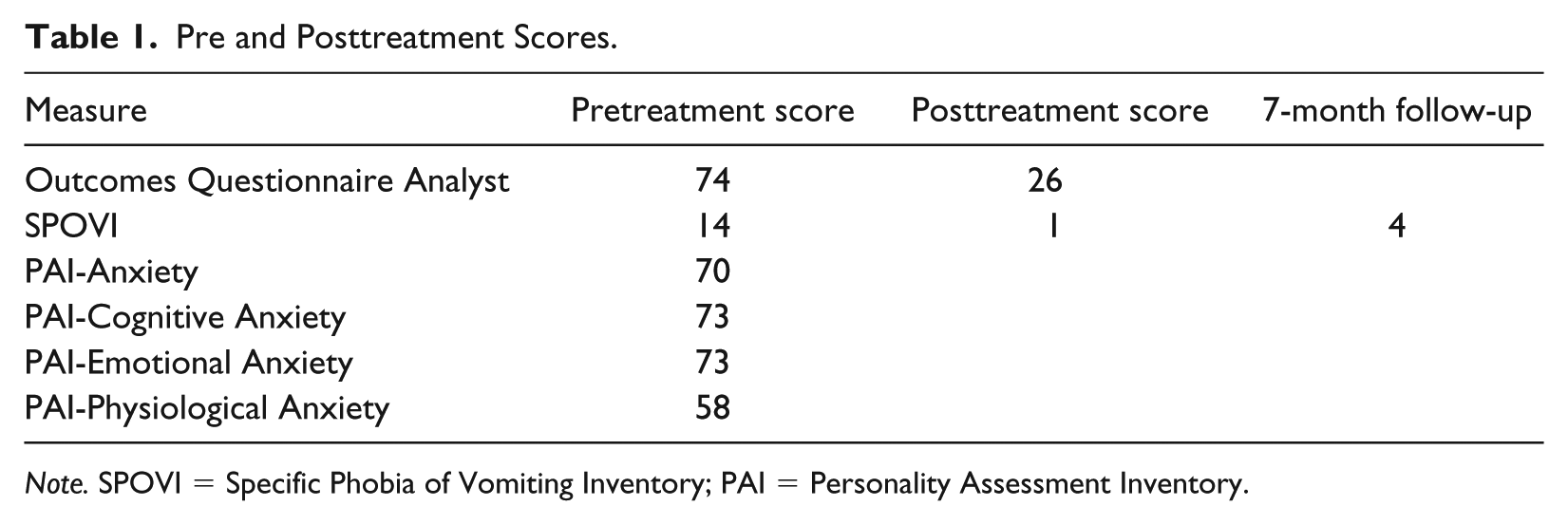
Note. SPOVI = Specific Phobia of Vomiting Inventory; PAI = Personality Assessment Inventory.
Example Fear Hierarchy.
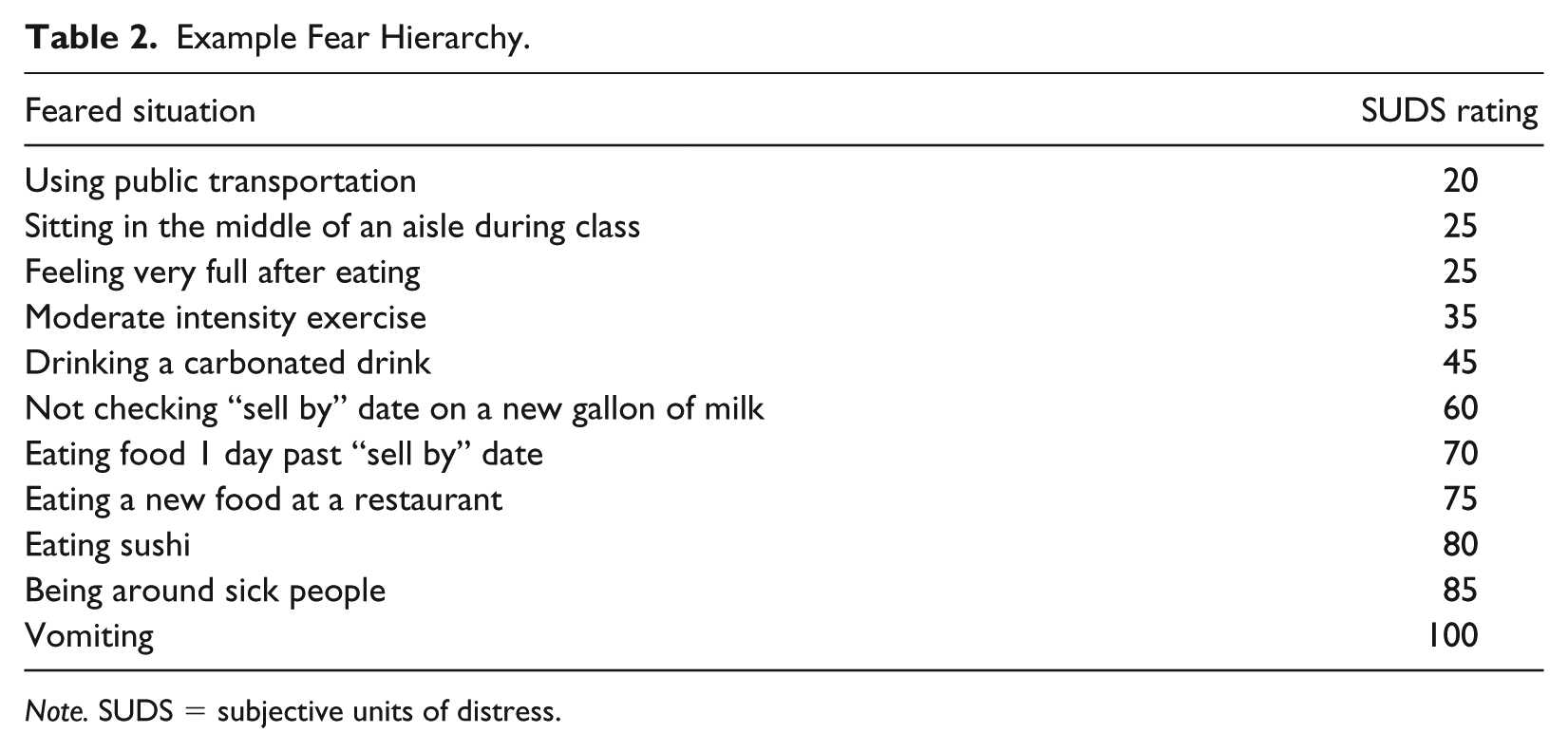
Note. SUDS = subjective units of distress.
Importantly, her SPOVI score decreased from 14 to 1 by the end of treatment (see Figure 1). Mary ultimately reported that she experienced almost no thoughts or worries about vomiting during the last week of treatment. Specifically, during the initial session, Mary scored a 10 on the Avoidance subscale of the SPOVI, and a 4 on the Threat Monitoring subscale. After treatment, she scored a 0 on the Avoidance scale and a 1 on the Threat Monitoring scale. Thus, by the end of treatment, Mary reported marked improvements in overall anxiety levels and social functioning (OQ scores) as well as specific fears of vomiting (SPOVI scores).

SPOVI scores during treatment.
8 Complicating Factors
Mary was very motivated and focused to address vomit-related anxiety throughout therapy. Nonetheless, acute stressors arose periodically (e.g., final exams, relationship distress), and she chose to prioritize these concerns in session. This did not detract from the overall effectiveness of the Emetophobia treatment, but likely extended the total number of sessions necessary to treat her vomit-related anxiety.
9 Access and Barriers to Care
There were no significant barriers to care during this treatment intervention. Treatment was conducted once per week, outside of schedule conflicts (e.g., holidays, exam schedule).
10 Follow-Up
Mary was contacted approximately 7 months after completing treatment and agreed to complete a follow-up SPOVI assessment. At a 7-month follow-up, her SPOVI total score was a 4, suggesting that her symptoms have maintained in a low level since ending therapy services.
11 Treatment Implications of the Case
This case study provides additional evidence that the use of a transdiagnostic approach for Emetophobia is effective in reducing specific fears of vomiting, as well as comorbid generalized and social anxiety. As only the second case study to show efficacy in utilizing a transdiagnostic approach in the treatment of Emetophobia, it will be important to develop a more well-defined evidenced-based practice protocol for vomit-related anxiety.
Importantly, this study shows that long-term maintenance of emetephobic symptoms occurred at a 7-month follow-up. This represents a strength of both the current study and the treatment protocol. Only one prior study utilized a transdiagnostic approach to the treatment of Emetophobia (Paulus & Norton, 2016) and this study did not include a follow-up of symptom severity post-treatment.
While two previous studies have shown reductions in anxiety after only five to 10 sessions, the current case describes a more long-term treatment. This opportunity was afforded not only due to the nature of a training clinic (e.g., very inexpensive for the client; convenient campus location; graduate clinician availability) but also because the client was quite motivated to overcome long-term symptoms of anxiety. Given evidence of high attrition due to concerns about the use of explicit, vomit-related stimuli (Boschen, 2007), the fact that Mary remained in treatment for a long period of time provides further evidence for the utility of not incorporating such specific exposure exercises in the treatment of Emetophobia.
Although the lack of time-constraint was a unique feature of this case, it also represents a limitation, as it is unlikely that many outpatient clinic providers treating emetephobic concerns can meet with clients for over 40 sessions. Future studies should consider the length of treatment needed to treat Emetophobia from a transdiagnostic approach. While it may be possible to target emetephobic concerns in just a few sessions, longer term treatment that addresses the client’s other comorbid anxious symptoms as well is likely beneficial.
12 Recommendations to Clinicians and Students
The current study provides further evidence that Emetophobia can be effectively resolved utilizing transdiagnostic strategies and without direct exposure to vomit or vomit-like stimuli. Clinicians should consider utilizing such an approach, as the treatment described here resulted not only in reduced anxiety about vomiting but improvements in more generalized anxious symptoms and daily functioning. Along these lines, recent efforts have been taken to provide empirical support for the use of a transdiagnostic treatment protocol for emotional disorders (Farchione et al., 2012; Wilamowska et al., 2010). Results from these studies have largely been positive, suggesting that such approaches can effectively reduce symptoms of anxiety and depression (e.g., Farchione et al., 2012). As research on shared vulnerability between diagnostic categories increases, it will be critical that researchers continue to study, and clinicians continue to utilize, transdiagnostic approaches to psychopathology. Such approaches offer flexibility in treating psychopathology regardless of diagnostic category, and may facilitate the use of evidence-based practices among clinicians.
In sum, although it will be important for future studies to examine more well-controlled treatment efforts, the present evidence suggests that Emetophobia can be largely resolved from a transdiagnostic approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.