
Abstract
Though anger is a common human emotion, the unfettered behavioral expression of anger is often costly, contributing to a range of functional impairments, poor quality of life, and both physical and mental health problems. The current case illustrates how a third-generation cognitive behavioral therapy, Acceptance and Commitment Therapy (ACT), may be effective in reducing suffering linked with problematic anger. The client (“Robert”), a treatment-naïve man of low socioeconomic status, presented to a university training clinic reporting problematic anger outbursts that interfered with his relationships at work and with his girlfriend. The therapist conceptualized Robert’s problematic anger through the ACT psychological flexibility model, wherein Robert’s anger appeared to function as experiential avoidance to distance him from underlying emotional hurt. The therapist used ACT over 27 sessions to reduce Robert’s psychological inflexibility while promoting more psychological flexibility. Early sessions highlighted the unworkability of Robert’s anger, whereas subsequent sessions focused on clarifying values, loosening cognitive fusion, facilitating present moment awareness, and cultivating mindful acceptance in the service of living a meaningful life. The therapist monitored treatment progress using quantitative measures and qualitative reports. Collectively, the client showed notable gains. The case study adds to the growing body of literature supporting ACT for problematic anger.
1 Treating Problematic Anger With Acceptance and Commitment Therapy: A Case Study
Theoretical and Research Basis for Treatment
Anger is not inherently problematic but can be harmful when expressed or suppressed (Eifert & Forsyth, 2011; McKay et al., 2003). Anger is defined as a negative emotion triggered by perceived threat provocation and, when mishandled, is associated with aggression, interpersonal problems, and physiological disorders (Berkout et al., 2019). Anger rarely occurs in isolation and is often comorbid with numerous psychological conditions including depression, anxiety disorders, posttraumatic stress disorder, and substance use disorders (Cassiello-Robbins & Barlow, 2016; Coccaro et al., 2016). Moreover, inappropriate responses to anger can lead to more anger, distress, and functional impairments (Eifert & Forsyth, 2011). As such, it is often anger behaviors that create problems, thus prompting need for psychological intervention.
Cognitive Behavioral Therapy (CBT) is widely regarded as a moderately effective intervention approach for problem anger (Lee & DiGiuseppe, 2018). However, CBT for problematic anger has been met with some criticisms including high dropout rates (Berta & Zarling, 2019) and lack of data on efficacy in heterogeneous populations (Chesworth, 2018; Donahue et al., 2017; Toohey, 2021), especially among low-income and minority individuals (Saavedra, 2007). Though discussions of CBT for anger highlight the need for more work addressing mechanisms of change (Toohey, 2021), other research suggests that reductions in anger symptoms are mediated by increases in calming skills, but not cognitive or behavioral skills, after a course of group CBT (Mackintosh et al., 2014). Further, CBT for problematic anger conceptualizes anger itself as the problem and does not address transdiagnostic processes maintaining anger or other comorbid conditions (e.g., depression). For example, veterans showed reductions in anger symptoms after a course of CBT for anger management but evidenced no change in symptoms of posttraumatic stress disorder (Kalkstein et al., 2018). As it stands, CBT for anger attempts to reduce anger-related thoughts, emotion, and arousal (e.g., thought stopping; Reilly & Shopshire, 2019), which, if taken in the context of the emotion control and suppression literature (e.g., Gross, 2015; Wang et al., 2020), may lead to paradoxical increases in anger (Novaco, 2016; Quartana et al., 2007; 2010; Roberton et al., 2012). Thus, alternative conceptualizations and treatment methods, especially those targeting transdiagnostic processes, are indicated.
One such conceptualization views anger and anger behavior as serving the function of avoiding other emotional pain (Eifert & Forsyth, 2011). That is, by getting angry and engaging in anger behaviors, individuals avoid experiencing primary emotional experiences such as hurt, betrayal, fear, loss, or being loved or cared for (Eifert & Forsyth, 2011; Eifert et al., 2006). This conceptualization, in turn, can be understood through the lens of a transdiagnostic process known as psychological flexibility.
Psychological flexibility is the ability to remain in contact with the present moment and to behave consistently with freely chosen values even when unwanted thoughts, emotions, or bodily sensations are present (Hayes et al., 2012). Psychological flexibility, in turn, involves six interrelated processes: acceptance (i.e., willingness to experience unwanted private events), contact with the present moment (i.e., awareness of current experience as it is), defusion (i.e., ability to see thoughts as thoughts, without attaching to the literal meaning), self-as-context (i.e., an observer or transcendent self-perspective), values clarity (i.e., connection with what is important in life), and committed action (i.e., engaging in behaviors that are consistent with values) and is largely associated with quality of life and wellbeing (Hayes et al., 2012; 2013).
Psychological inflexibility, on the other hand, is the narrowing of behavioral repertoires away from valued ends when psychological pain shows up (Hayes et al., 2012; 2013). Psychological inflexibility involves experiential avoidance (i.e., unwillingness to experience private events and subsequent efforts to eliminate them), fusion (i.e., attachment to unhelpful thoughts, including judgment, as literal truth), self-as-content (i.e., attachment to unhelpful narratives and stories linked with the self, such as “I am an angry person”), disconnection from the present moment, unclear values, and inaction regarding values (Hayes et al., 2012). Psychological inflexibility is a transdiagnostic process, meaning it is associated with numerous psychological problems and dysfunctional behaviors including anxiety and mood disorders, disordered eating, substance and alcohol use (Grom et al., 2021; Levin et al., 2014), problematic anger, and aggression (Berkout et al., 2019).
Acceptance and Commitment Therapy (ACT) aims to increase psychological flexibility and decrease psychological inflexibility by targeting each of the aforementioned processes (Hayes et al., 2012). Several experiential exercises and metaphors are used to contact client’s unworkable anger management strategies in favor of more workable behaviors (e.g., Eifert et al., 2006). Research on ACT for the treatment of anger and aggression suggests that it is effective for reducing physical and verbal aggression, stress, and experiential avoidance while also increasing acceptance, psychological flexibility, and values-driven behaviors (Cohen’s d = .36–4.73; Berkout et al., 2019). Notably, decreases in intimate partner violence have been found to be mediated by increases in psychological flexibility (Zarling et al., 2015).
Despite studies with small samples and few randomized control trials, initial research in this area is promising. Because problematic anger is often comorbid with other psychological disorders, a transdiagnostic treatment approach, such as ACT, seems warranted. Moreover, a majority of intervention studies examining ACT for anger focus on veterans and military personnel, or incarcerated adults (Berkout et al., 2019). Thus, more work is needed to examine ACT for the treatment of anger in civilian populations. Further, we are not aware of any protocols for clinicians regarding the treatment of anger using an ACT framework. This case study explored the utility of ACT for problem anger in a low-income, non-incarcerated civilian client with problematic anger. We hope that this case study provides clinicians with a guide to treating problematic anger using ACT interventions.
2. Case Introduction
“Robert” (a pseudonym) was a 33-year-old heterosexual, cisgender, White male. He self-referred to a community mental health clinic affiliated with a large northeastern university for problematic anger related with work and intimate relationships. The therapist was a clinical psychology graduate student in his second year of doctoral training under the supervision of licensed psychologists. Identifying information was changed to protect client confidentiality.
3. Presenting Complaints
Robert presented with complaints of problematic anger. He reported frequent outbursts at work which resulted in verbal altercations with coworkers and supervisors, including throwing tools or punching trees in anger. He also complained of recurring arguments with his girlfriend, and her concern that Robert was teaching her son poor anger management skills.
4. History
Robert was an only child born and raised in a medium-sized metropolitan city in the northeast. His parents were married, and he lived with both growing up. Robert stated that his mother had an alcohol problem and was verbally abusive and neglectful. He denied a history of physical abuse. Robert’s anger problems reportedly began around the age of eight. He stated he was bullied throughout his school years and that he occasionally bullied others. Robert noted that his father taught him to cope with his anger by hitting a tree with a crowbar. Robert stated he and his father maintained a good relationship from childhood through his adult years and noted that his father supported his efforts to seek treatment for his anger. Robert received a high school diploma and did not pursue college. At the time Robert sought treatment, he was gainfully employed in the construction industry earning an annual income of approximately $26,000. He denied previous psychological treatment, though he indicated sporadic meetings with school guidance counselors in middle and high school for anger management.
At intake, Robert noted being in a yearlong romantic relationship with a woman who lived in a neighboring state. Robert, in turn, lived in a local boarding house and traveled to visit his girlfriend and her 10-year-old son on weekends. Robert described his relationship with her son as good, noting that he assumed a role as a father figure for him. He stated his girlfriend was pursuing her nursing degree and experienced considerable stress and anxiety. Robert reported he and his girlfriend got in frequent arguments, though believed they had a good relationship, noting they shared a friend group and enjoyed many activities together. He vehemently denied physical acts of anger toward his girlfriend or her son.
5. Assessment and Diagnosis
Intake
Robert’s psychosocial history was evaluated over three, one-hour intake sessions and included the Mini-International Neuropsychiatric Interview Version 7.0 (MINI; Sheehan et al., 2014). Because Robert’s presenting problem included anger outbursts, questions probing for Intermittent Explosive Disorder (IED) were included. The intake sessions also included orienting Robert to the policies and procedures of the clinic, gathering psychosocial history not covered by the MINI (e.g., educational history), providing a case conceptualization, and building rapport. The final intake session also included several symptom and process-based self-report assessments (see Progress and Treatment Monitoring section below). Robert was pleasant, cooperative, and engaged in treatment. He was fully oriented to person, place, and time, made appropriate eye contact, and his affect was appropriate. Throughout, his mood was generally euthymic, his memory and judgment were intact, and his thought processes remained coherent and clear. Robert denied experiencing hallucinations, delusions, suicidal or homicidal ideation.
Robert reported that his girlfriend encouraged him to seek psychological treatment for problematic anger outbursts. He stated his girlfriend was concerned because her 10-year-old son was having behavioral issues, such as acting out and not following directions, and she worried that Robert’s anger outbursts may be influencing her son in negative ways. Robert acknowledged that his anger outbursts were interfering with his relationship with his girlfriend and perhaps her son, though he did not believe his anger interfered with his work performance. Yet, he endorsed frequent problems with coworkers and managers.
He stated that his anger outbursts at work manifested as verbal altercations with coworkers and managers several times a week. Robert indicated that his anger was often triggered when managers and coworkers referred to him using derogatory names or when instructions appeared unrealistic to him. Robert also reported anger when he perceived coworkers being lazy and when managers and coworkers criticized him. He stated that, about once a month, his anger led him to throw tools (e.g., a screwdriver). Approximately once a year Robert noted becoming so enraged that he would punch a tree; an action that often resulted in sprained wrists. However, Robert denied physical aggression towards other people or animals, including property damage resulting from his anger.
Robert stated that he and his girlfriend got into verbal arguments multiple times a week, which escalated quickly. He reported unintentionally provoking his girlfriend which, in turn, would often lead her to respond to him with anger and criticism. Robert stated that critical comments from his girlfriend made him think he was “not good enough,” sparking his own anger. As a result, Robert would frequently “storm off,” slam doors, or make passive aggressive and critical comments during arguments. He indicated that after they both cooled down, they would apologize to each other and work to repair the relationship. Robert reported that such verbal altercations with his girlfriend were more likely to occur when they were drinking alcohol. The therapist assessed for domestic violence and child abuse. Robert adamantly denied any history of physical assault of his girlfriend or her son.
Robert reported a seasonal pattern of low mood for the past several years that coincided exclusively with the winter months. While he denied any symptoms of depression in the weeks prior to intake (which occurred in early Fall), he noted that almost every winter he experienced depressed mood, lack of interest in activities, fatigue, feelings of worthlessness, and difficulties concentrating. Robert denied current and past history of suicidal ideation. He reported these mood symptoms occurred together over the same two-week period and usually lasted one to 2 months. He indicated that depressive symptoms emerged during the winter months due to the construction off season, leaving him with more downtime and fewer financial resources. His last depressive episode occurred approximately 1 year prior to intake following a breakup of a previous relationship. He also indicated having bouts of anxiety and worry regarding his finances and living situation, occurring 1–3 days a week for approximately 2 h. Robert reported being bothered by these worries but denied that they interfered with his life.
Robert also reported episodes of problematic alcohol use. He stated that in the past year, he drank 1–6 beers daily for several weeks in a row. He indicated he often drank more than he intended, especially on weekends. He noted engaging in risky behaviors, such as driving, after consuming alcohol. He stated his stressful work environment led him to crave alcohol as a coping strategy. Though Robert reported that his drinking did not interfere with work performance, he did believe that it was contributing to his problematic anger and arguments with his girlfriend. Robert indicated making efforts to reduce his alcohol intake over the previous 6 months to intake, leading to reduced intake of 1–3 beers a night on weekend nights.
Diagnosis and Differential Diagnoses
Information gathered using the MINI was used to inform diagnoses. Robert failed to meet full diagnostic criteria for IED. Though Robert endorsed verbal aggression, more than twice weekly, for a period of at least 3 months, these events occurred in the context of a high stress work environment where coworkers and managers also got argumentative and critical. Thus, these outbursts did not appear “grossly out of proportion to the provocation or to any precipitating psychosocial stressors,” thus failing to meet Criteria B for IED. Further, his outbursts seemed to follow the escalation of arguments over time, rather than occurring suddenly with minimal provocation.
Robert met diagnostic criteria for past history of major depressive disorder (MDD), recurrent, and because he did not endorse any depressive symptoms for the past year, his MDD appeared to be in full remission. Robert also met criteria for mild alcohol use disorder, in early remission. Robert’s bouts of anxiety were infrequent, limited to specific domains (e.g., finances), and he reported no difficulty controlling his worries. Thus, he failed to meet criteria for generalized anxiety disorder. Robert also denied symptoms of social anxiety disorder, panic disorder, agoraphobia, and specific phobia.
6. Case Conceptualization
Robert’s case was conceptualized by mapping his experience and history onto each of the six interrelated processes of psychological inflexibility (e.g., Hayes et al., 2012). From an early age, anger expressions were reinforced by his father (e.g., hitting a tree with a crowbar) and by his peers. For Robert, anger expression functioned as a socially acceptable substitute for expression of other emotions, such as fear and sadness. For example, Robert’s feelings of sadness and inadequacy in response to his mother’s neglectfulness or by bullies’ verbal abuse were punished (e.g., being told to “man up”), whereas expressions of anger were temporarily reinforced by overshadowing feelings of pain/hurt or reducing bullies’ harassments. The avoidance of negative emotions was further reinforced by Robert’s use of cathartic aggression, in which hitting a tree with a crowbar and bullying peers resulting in temporary relief from his emotional discomfort. As a result, Robert learned to express anger, either verbally or by hitting objects, when he experienced any emotional pain or discomfort. Although this anger expression may have been adaptive at times during his childhood, it was no longer workable in adulthood as it interfered in relationships with his girlfriend and colleagues.
At the time Robert sought treatment, his anger expression appeared to function as experiential avoidance from the pain and hurt he felt with his girlfriend or at work. Robert reported that when his girlfriend criticized him, he thought of himself as inadequate. Rather than addressing the fear and hurt linked with feelings of inadequacy, Robert focused his attention outwardly by reminding his girlfriend of times she also behaved poorly. Similarly, Robert reported an anger response when he perceived criticism from managers, or when he felt slighted by colleagues at work. In these situations, Robert’s anger (e.g., thinking, “they’re idiots”) and anger behavior (e.g., verbal altercations), served as avoidance from feeling other forms of emotional pain. Robert’s overt anger behaviors (e.g., yelling at coworkers, throwing screwdrivers, etc.) served as attempts to escape the experience of anger itself. Robert reported experiencing short-term relief from anger and discomfort after engaging in overt anger behaviors, thus reinforcing overt behaviors in the context of anger. Over time, such behaviors may have become automatic, impulsive reactions to anger, rather than deliberate attempts to escape anger. During times of heavy drinking, Robert also used alcohol to reduce unwanted emotions.
In addition to experiential avoidance, Robert appeared to be fused with thoughts, judgments, and rigid rules about life and how things “should” be. When he felt emotional pain due to perceived criticism, Robert would often fuse with evaluative judgments (e.g., “my girlfriend has her own anger issues,” “idiot” coworkers). Robert also fused with judgments that text messages from his girlfriend, which he thought of as “passive aggressive,” leading him to search for hidden meanings and motives. Robert also fused with verbal rules of how things “should be” (e.g., equipment should be returned in a particular way after use). Fusion with rules about how to deal with anger also influenced his behavior (e.g., “anger needs to be controlled,” “I have to do something to release anger”), leading him to storm out of conversations or throw objects.
Robert also evidenced fusion with his self-story (i.e., self-as-content). Thoughts such as “I am inadequate” or “I’m not good enough” appeared when he was criticized by his girlfriend or managers and coworkers. When criticized, he bought into self-referential thoughts and viewed them as literal truths. Activation of the self-referential pain elicited anxiety and other difficult emotions and thoughts fueled his downstream, avoidant anger cycle. Moreover, Robert described himself as someone who “has a short fuse” and “can’t handle stress.”
Robert’s difficulties with fusion and experiential avoidance made it difficult for him to remain in the present moment when angered or otherwise emotionally hurt. For instance, he commonly responded to criticism from his girlfriend by engaging in ruminative thinking about past moments when his girlfriend made mistakes. At work, Robert also got lost in imaginary arguments with coworkers who slighted him. After arguments with his girlfriend, Robert would often get pulled into thoughts about the past (e.g., by reviewing an argument he just had) or the future (e.g., contemplating how to break free from anger and manage it better).
Although Robert was stuck in processes of experiential avoidance, fusion with thoughts and his self-story, and difficulties with present moment awareness, he did demonstrate clarity about his chosen values (i.e., being a loving partner and a dependable coworker). It was such values that led him to therapy. Nonetheless, Robert struggled living in accordance with his values when faced with pain, discomfort, and anger. When pain and discomfort showed up, Robert’s behavioral repertoires narrowed in an effort to eliminate or avoid difficult emotions at the cost of living a meaningful and fulfilling life. Rather than noticing and responding flexibly in the presence of his fears, judgments, and anger toward his girlfriend, he responded with defensiveness and harsh words. These behaviors consequently interfered with his desire to be a loving partner. Holding on to rigid rules and high expectations also interfered with being a dependable coworker.
This case conceptualization identified processes that are difficult for Robert and served as a road map for his treatment. The ACT intervention described below targeted the six interrelated inflexibility processes with the aim being to expand Robert’s behavioral repertoires to include values-consistent behaviors in the face of difficult thoughts and emotions. In short, therapy aimed to help Robert act on his values with whatever thoughts and feelings that may arise vs. acting on his anger experience by lashing out or throwing tools.
7. Course of Treatment and Assessment of Progress
The ACT therapeutic relationship (Hayes et al., 2012) flows from a stance that is in line with discussions of the importance of common factors of therapy (Norcross & Lambert, 2011), including empathy, agreement on goals, and genuineness (Hovarth et al., 2011). These common factors were upheld as much as possible in working with Robert, wherein the therapist made efforts to maintain a strong therapeutic alliance while modeling and upholding an open, accepting, and non-judgmental stance.
The purpose of an ACT approach to Robert’s anger was not to reduce anger or to teach relaxation strategies to help him be calmer. As stated above, such strategies may have prolonged his struggle with anger or paradoxically increased difficult emotions (Eifert & Forsyth, 2011; Quartana et al., 2010). Instead, the focus was on helping Robert cultivate psychological flexibility by 1) recognizing unworkability, suffering, and costs linked with efforts to control his anger, 2) identifying and holding difficult thoughts, feelings, and other sensations in gentle awareness, and 3) behaving in values-consistent ways even when difficult private events (e.g., difficult thoughts, feelings, and bodily sensations) show up. Therapy did not progress in a stepwise linear fashion. Instead, the therapist fluidly attended to ACT processes as they arose in the moment (Eifert & Forsyth, 2011). Metaphors and experiential exercises were introduced and revisited throughout treatment to help Robert shift focus from avoiding and reducing anger to engaging in behaviors that led to a meaningful life. Specific metaphors and experiential exercises were modeled after those found in ACT therapeutic texts (Hayes et al., 2012), an ACT self-help book for problematic anger (Eifert et al., 2006), and other ACT intervention resources (e.g., Harris, 2019).
Creating the Context for Change
Plotting the New Course
Robert’s self-referral for treatment indicated there was something about the relationship with his girlfriend, her son, and his coworkers he cared about. To further clarify values, Robert was led through an exercise where he watched a metaphorical movie of his life as he grew older. He was prompted with questions such as, “what do you want your life to look like? Who would be up on that screen with you? What would you be doing?” Afterward, Robert shared what saw on his movie screen and some of his core values: being a supportive and loving partner and being a caring, supportive, and fun father figure. These values he summed up as being a “family man.” Robert also stated that he enjoyed creativity and artistic beauty, community in his music production pursuits, fun and friendship with his peers, and lastly being a dependable employee.
The passengers on the bus metaphor (Hayes et al., 2012) were used to help Robert determine who was in control of his life: his emotions or himself. Here, Robert was invited to imagine unwanted thoughts and emotions as obnoxious passengers on his bus, telling him where to go and what to do. Robert stated that throwing tools at work was almost like trying to kick the anger off the bus. He noted that while he was doing this, his bus was not moving and was stuck in one place. The therapist encouraged him to consider driving his bus without being controlled by the unruly passengers. That is, perhaps he could allow the passengers to make a ruckus without doing as they say, and without getting out of the driver’s seat to chastise, fight, or kick them off the bus. Instead, he could drive his bus wherever he wanted to go in life and with the passengers. The therapist often reminded Robert of the metaphor throughout treatment by asking “who is driving your bus?” The metaphor also overlapped with mindful acceptance processes as Robert was asked to identify thoughts or emotions that were trying to drive his bus and then practicing allow them to be as they are without struggle or resistance.
Cultivating Mindful Awareness and Acceptance
Robert was introduced to mind watching (Eifert et al., 2006) to develop perspective taking with his thoughts. After closing his eyes and taking several deep breaths, Robert was invited to simply notice thoughts as they arise and to label them (e.g., “there’s judging”). After a few min, Robert was asked to expand his awareness to bodily sensations, such as the feeling of the chair on the back of his legs, and then do the same with emotions. Robert continued noticing and labeling for several min. This intervention was intended to promote mindful attention to the present moment, to facilitate an observer perspective to reduce entanglement with thoughts, and to begin cultivating acceptance of thoughts and emotions. Robert was encouraged to practice this exercise twice a day and then apply it to moments when he felt anger.
Robert was invited to notice specific emotions, thoughts, and bodily sensations in response to anger cues (e.g., girlfriend criticizing him). When a situation prompted anger, Robert was encouraged to stop and “watch for flags” of anger (Eifert et al., 2006) by pausing and noticing (a) what his thoughts were doing and (b) what sensations he felt in his body and where he felt them. During these moments, Robert was invited to maintain focus on his inner experience and allow it to unfold without trying to control, suppress, or alter it. Through this exercise, Robert gained awareness of his “flags” of anger so that he could then practice mindful awareness with his thoughts and feelings. The therapist encouraged Robert to say to himself “I am noticing” before a thought to facilitate defusion, self-as-context, and mindful acceptance of experience (e.g., “I am noticing the thought that my girlfriend is criticizing me.” vs. “my girlfriend is criticizing me.”)
Robert was also introduced to the inner and outer shuttle exercise (Eifert et al., 2006) to further facilitate mindful awareness of experience, cultivate the observer perspective, and practice acceptance of thoughts, emotions, or bodily sensations. Robert was invited to close his eyes for a few moments, notice a thought, emotion, or sensation, sit with it, and notice who is noticing it. Then, he was asked to open his eyes and notice an object in the room, sit with it, and then notice who is noticing that object. At first, he reported getting hooked on judgmental thoughts and found the exercise challenging. Yet, he also expressed an increased ability to accept his internal experience and notice his own noticing.
Undermining Believability of Thoughts and Feelings
Robert found the chess board metaphor (Hayes et al., 2012) particularly helpful, in which unwanted emotions and subsequent actions were likened to a game of chess. Robert’s imaginary arguments with coworkers were compared to movement of the black and white pieces during a chess game; the move of one piece was to combat the move of the opposing side. Unlike a game of chess, though, no side could win as both occurred within Robert’s mind. He was encouraged to explore what it would be like to be the chess board, which had no stake in the outcome. Just as the board provides the space for the game to occur so could Robert’s provide the space for thoughts to arise without pushing for one side to win. This metaphor helped reduce Robert’s entanglement with imaginary arguments and self-referential thoughts.
Robert was also guided through the leaves on the stream exercise (Harris, 2019) where he was invited to imagine sitting on the edge of the stream watching leaves float by, and then gently placing a thought on each leaf and watching it come and go. As with the chess board exercise, Robert was encouraged to take the perspective of the stream, while noticing that the stream does not care what thought is on each leaf, but rather simply provides a place for the leaf to land and drift along. Robert and the therapist discussed how this exercise could be used when he found himself hooked by judgments, evaluations, or other thoughts that lead to anger.
Robert reported that metaphors and experiential exercises were helpful in shifting his relationship with his thoughts and in helping him recognize how his inner dialog acted as gasoline on a burning fire, leading him to react with more anger with each provocation. To undermine the literality of his internal arguments, the therapist suggested Robert sing the arguments to himself (one of several ACT defusion strategies; American Psychiatric Association, 2013). Robert stated that he occasionally got caught up in the imaginary arguments. However, once he gained mindful awareness of what his mind was doing, he shifted to singing the rest of the argument. Robert reported that this strategy was effective and made him laugh, and thus appeared to create space for something new.
Forgiveness and Compassion
Because anger is suggested to be an emotion that masks other forms of emotional pain (Eifert & Forsyth, 2011), the therapist and Robert discussed extending compassion towards himself and others. The therapist led Robert through a perspective taking exercise similar to one found in Eifert and colleagues’ (2006) ACT for anger workbook. The therapist invited Robert to get in touch with others’ suffering and imagine being the recipient of his expressed anger. The therapist then led Robert through an exercise in which he was encouraged to practice giving loving-kindness to himself first, then extending it to someone he cared for, and lastly offering it to someone he had difficulties with. After, the therapist and Robert discussed how others, like him, also experienced emotional pain and hurt and how he could extend patience and compassion to others when they appeared upset with him or criticized him.
Forgiveness of others was targeted using the fishhook metaphor. Here, Robert was encouraged to imagine himself on a fishhook of anger with all the “wrongdoers” added to the hook after him. Robert was challenged to get off the hook. Here, he recognized that this was impossible because he was the first on the hook, and if he was to get off, the others would have to be let off the hook first. More importantly, Robert noticed that he had the power to let others off the hook (e.g., of being idiots) and that this was something he could do for himself.
If Not Anger, Then What?
Within the ACT framework, practicing mindful awareness of thoughts and feelings is pointless without a purpose. Robert brainstormed and practiced different behaviors, in line with his values, he could engage in when his anger showed up. He recognized that practicing mindful awareness was one committed action he could take. For example, rather than making passive aggressive comments to his girlfriend, he paused to notice his thoughts and emotions. Then he practiced patience and communicated understanding and asked if she needed space. Robert committed to giving her the space she needed, by slowly going to a different room, rather than abruptly packing up his belongings or storming out. Robert expressed willingness to resist the urge to yell at his girlfriend’s son when he was misbehaving, opting instead to teach him new skills he learned in therapy. At work, Robert committed to thanking his coworkers and managers for suggestions, even when he disagreed with them. He also took several min to check in with his breathing while noticing his judgmental thoughts before shifting his attention back to other tasks.
Progress and Outcome Monitoring
Robert’s progress was monitored through quantitative and qualitative assessments.
Treatment Progression and Outcomes
Pre- and Post-treatment response across transdiagnostic process and symptom measures.
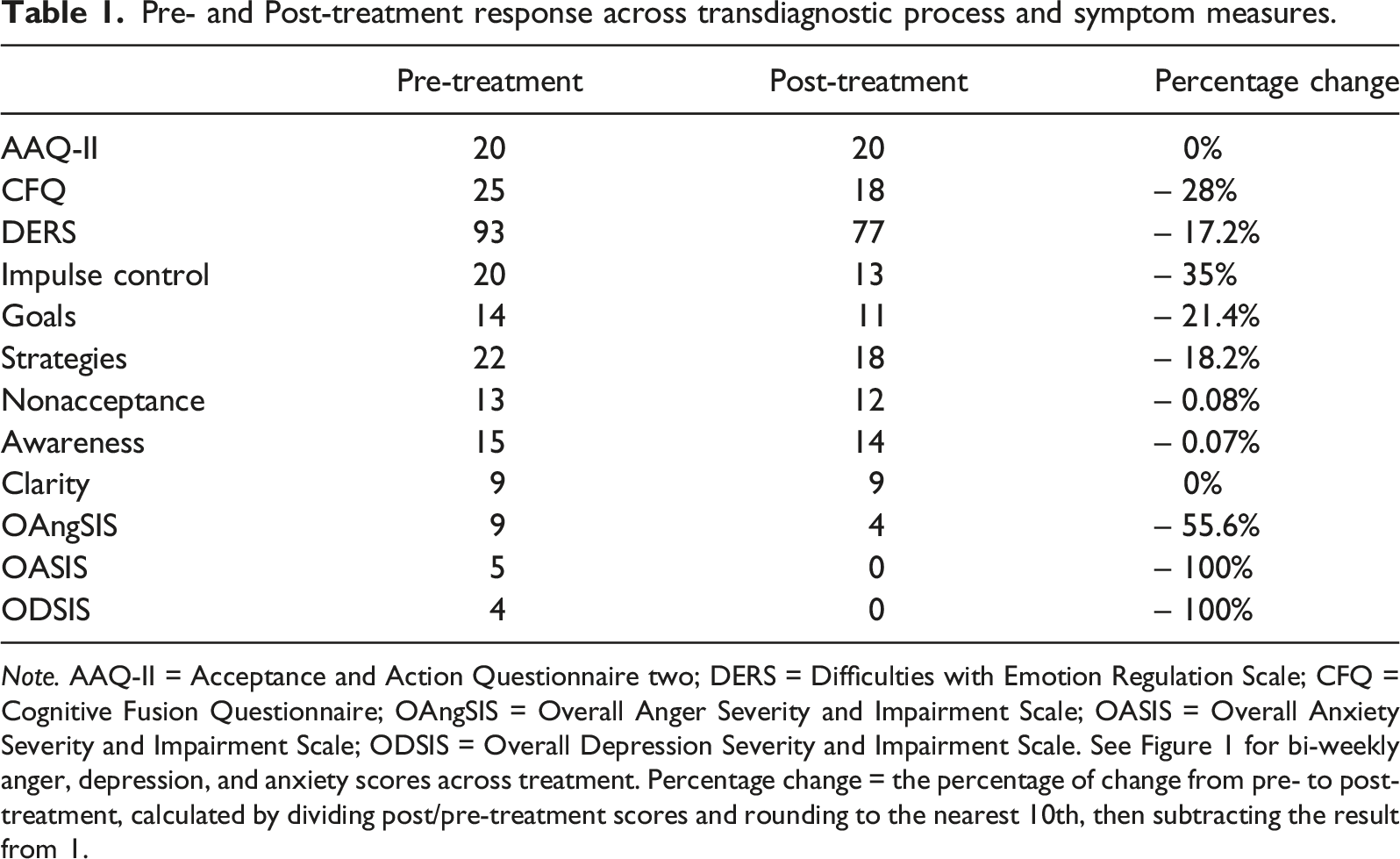
Note. AAQ-II = Acceptance and Action Questionnaire two; DERS = Difficulties with Emotion Regulation Scale; CFQ = Cognitive Fusion Questionnaire; OAngSIS = Overall Anger Severity and Impairment Scale; OASIS = Overall Anxiety Severity and Impairment Scale; ODSIS = Overall Depression Severity and Impairment Scale. See Figure 1 for bi-weekly anger, depression, and anxiety scores across treatment. Percentage change = the percentage of change from pre- to post-treatment, calculated by dividing post/pre-treatment scores and rounding to the nearest 10th, then subtracting the result from 1.
Overall, quantitative measures suggest a successful treatment response. As seen in Figure 1, treatment appeared to decrease both the experience of anger and the functional impairments attributed to Robert’s anger from 9 on the OAngSIS at the beginning of treatment to 4 at termination. Although a small spike in anger occurred at Session 21 (OAngSIS = 6) and toward the end of treatment, he consistently endorsed benefits in response to treatment. Robert’s treatment progress on anger, depression, and anxiety.Note. OAngSIS = Overall Anger Severity and Impairment Scale. OASIS = Overall Anxiety Severity and Impairment Scale. ODSIS = Overall Depression Severity and Impairment Scale. Bi-weekly measurement began during the last intake appointment (i.e., Session 3).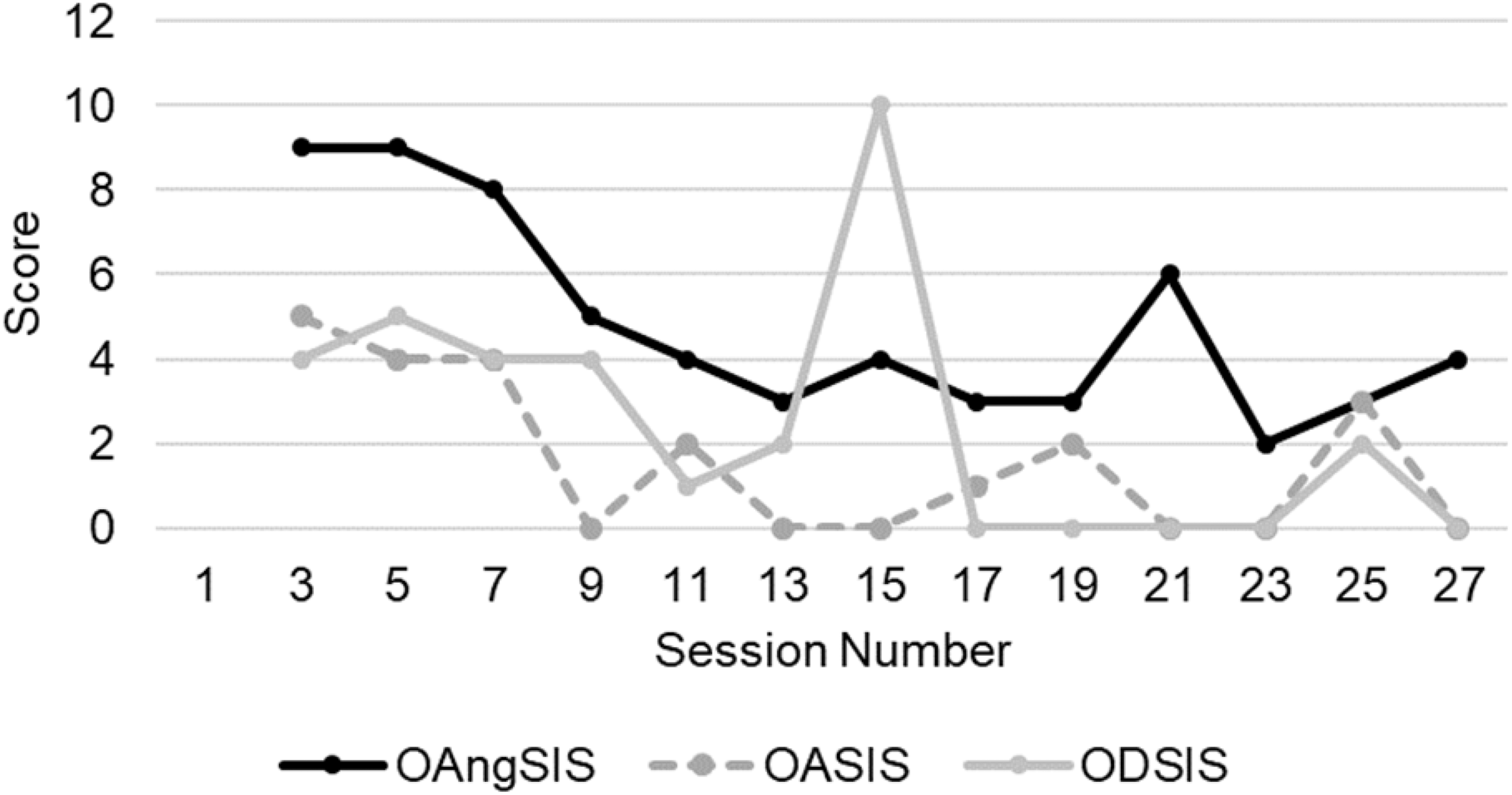
The AAQ-II did not change from pre- to post-treatment (AAQ-II = 20). The lack of change may reflect issues with limiting assessments to two data points pre- and post-treatment, which does not allow for a clear evaluation of trend and variability. As such, had the AAQ-II been measured more frequently throughout treatment, a clearer evaluation of trend would have been possible.
Cognitive fusion, measured by the CFQ, decreased from a pre-treatment level of 25 to 18 at post-treatment (i.e., Session 25). This change suggests Robert became less entangled in his thoughts and emotions across treatment sessions. Though clinical guidelines for the CFQ do not exist, Robert’s pre-treatment CFQ score was similar to individuals reporting high work stress (M = 25.84) and dropped below average scores observed in community samples (M = 22.28; Gillanders et al., 2014).
Robert’s anxiety and depression (measured by the OASIS and ODSIS) were low at the beginning of treatment and appeared to decrease across treatment (see Figure 1). However, Robert’s depressive symptoms spiked in a clinically elevated range at Session 15 (ODSIS = 10). At this time, Robert was laid off from his job and reported experiencing anhedonia. Here, the clinical focus shifted from anger to his experience of depression, with the aim being to help Robert generalize his skills to other difficult thoughts and emotions. By termination, Robert’s ODSIS scores were well below clinical cutoffs.
Changes in the DERS from intake (score = 93) to Session 25 (score = 77) indicated improvements in Robert’s difficulties with emotion regulation. To provide context to these scores, males engaged in psychological or physical aggression reported mean DERS scores of 86.18 (SD = 19.37) and 87.20 (SD = 18.01), respectively; mean scores for males who do not engage in aggressive behaviors are 76.96 (SD = 21.73) in one sample and 82.55 (SD = 21.10) in another (Shorey et al., 2011). The largest pre- to post-treatment improvements were in Robert’s impulse control (pre = 20 to post = 13), his ability to reengage in goal-directed activities (pre = 14 to post = 11), and emotion regulation strategies (pre = 22 to post = 18). Robert’s one point decrease in nonacceptance (pre = 13 to post = 12) was consistent with lack of noticeable change on the AAQ-II. Awareness decreased modestly from 15 to 14, and Emotional Clarity remained stable (pre = 9 to post = 9). Overall, Robert’s emotion regulation skills appeared to improve over the course of treatment as did his engagement in meaningful goal-directed activities; two outcomes that are consistent with the aims of ACT.
Regarding the therapeutic alliance, scores on the WAI-S after Session 10 suggest that Robert and the therapist had a strong therapeutic alliance. High scores indicated agreement on goals, appropriateness of interventions, and a strong bond. The strong therapeutic alliance in the current case may account for some Robert’s treatment gains (Hovarth et al., 2011).
Robert also verbally reported therapeutic gains in addition to improvements evidenced on the quantitative assessments. Robert frequently stated that he noticed improvements in his anger and anger behaviors (e.g., “this stuff works”). Robert clarified that he was able to reduce anger outbursts and connect with others. Robert reported that he did not throw any tools at work during treatment; a behavior that occurred once a month prior to treatment.
Per Robert’s report, therapy appeared to have the most significant impact on his performance at work. He indicated he was less caught up in judgmental thoughts and anger when coworkers or managers behaved in ways that previously triggered his anger. Robert stated that when he noticed judgmental thoughts or anger, he could step back and recognize the thoughts and breathe with the anger. He indicated that these new behaviors gave him space to hold the anger while he was able to redirect his attention back to whatever task he was working on. Robert also reported that his colleagues noticed changes in his anger and anger behaviors, including his calmer disposition.
Robert reported greater difficulties implementing the skills when he was with his girlfriend. However, he did note improvements in his relationship with his girlfriend. Though Robert indicated that he and his girlfriend would argue from time to time, he also stated that he no longer would not make sarcastic comments or aggressively pack up his belongings and leave. Rather, he asked that they go to different rooms when discussions became unhelpful. Robert reported that stepping out of the room was helpful and consistent with his values because he was left to experience his anger and emotional pain, rather than make hurtful comments to his girlfriend to avoid his anger. He reported that his communication with his girlfriend improved and his perspective taking skills had increased. He was able to see situations from his girlfriend’s perspective which allowed him to respond in more compassionate ways. Robert reported a reduction in his tendency to “read between the lines” when his girlfriend texted him and found the leaves on the stream exercise helpful during times when he noticed old “read between the lines” thoughts emerging.
Robert also reported benefits in his relationship with his girlfriend’s son. Robert indicated that by practicing mindful awareness when he was frustrated with his girlfriend’s son, he was able to gain enough space to speak appropriately with him. Robert stated that he found joy in teaching his girlfriend’s son some of the metaphors and mindfulness skills he had learned in therapy. This led to them engaging in new activities together, such as gardening.
Additionally, Robert reported that he was able to maintain his alcohol intake at a level that did not interfere with functioning or lead to clinical distress. Although Robert’s alcohol use disorder was in early remission upon entering therapy, he reported that he no longer consumed alcohol to relieve stress or anxiety.
Overall, the treatment gains observed in quantitative assessments and qualitative reports suggest that Robert benefited from an ACT approach for his problem anger and treatment also improved his quality of life. We cannot rule out that Robert’s reduced alcohol use significantly contributed to his reductions anger outbursts. In fact, it probably did to a certain degree. However, we are confident that treatment was largely responsible for reductions in anger outbursts given that he was still experiencing such outbursts after he reduced drinking prior to beginning treatment. Though Robert reported a brief increase in sub-clinical depression during treatment, the rapid remittance of depression and the maintenance of remission of his alcohol use disorder suggest that a transdiagnostic approach, coupled with a strong therapeutic alliance, was effective.
8. Complicating Factors
During Robert’s treatment, one complicating factor emerged. Between Sessions 14 and 15, Robert was laid off from his construction job, with the layoff being associated with symptoms of anhedonia (see also elevated score on the ODSIS). Robert stated that he had lost motivation to complete chores around his apartment and engage in hobbies. Robert also endorsed fatigue. The therapist shifted away from active, experientially based interventions in favor of validation and reflective listening to communicate empathy. Because empathy is a common factor with strong empirical support (Elliot et al., 2011), the therapist made efforts to provide supportive listening regarding Robert’s concerns. Robert was without work for a couple weeks and his symptoms of depression improved with new employment at another construction job site. In the interim, however, he experienced depressed mood. This experience, in turn, may have been beneficial in the long run by helping Robert learn to generalize therapeutic skills, from anger to depression and other painful emotional events.
9. Access and Barriers to Care
Robert’s financial situation may have been a barrier to his treatment, which may have impacted treatment response. Indeed, research suggests psychological disorders are highly prevalent in low-income populations due to high levels of stress related to economic hardship (Santiago et al., 2013). Further, the stress associated with low income may lead to higher levels of anger and substance abuse (Saavedra, 2007). Robert initiated treatment at a time when his income was decreasing for the winter season. The summer months brought more hours of work per week due to longer workdays and warmer weather. In winter months, the cold and snow interfered with projects. As a result, Robert made significantly more money in the summer than in the winter. The added stress associated with reduced income may have interfered with Robert’s treatment, including his tendency to experience depressed mood.
The therapist and Robert discussed his ability to purchase food and other necessities. Robert reported his financial situation did not interfere with access to adequate nutrition or other basic needs. Because the clinic operated on a sliding scale based on yearly average income, Robert’s reported yearly income was inflated compared to what he made during the winter months. The therapist offered to reduce Robert’s fee to reflect what he was currently making. Nonetheless, Robert stated that he would pay based on his yearly income. Though Robert never mentioned financial burdens due to treatment, he did report general financial difficulties. Mid-treatment, Robert mentioned that he was laid off from one project, resulting in a significant reduction in work. The therapist checked in again about lowering the fee so that treatment would remain accessible. Robert again declined stating that he was no longer going to local bars to drink alcohol as frequently as he once did which allowed him to allocate money towards his treatment.
10. Follow-Up
Upon treatment termination, Robert indicated that he did not want to be transferred to another therapist at the clinic because he was in the process of moving closer to his girlfriend who was living in a neighboring state. Robert further stated he had learned useful skills in responding to his anger and would be pursuing couple’s counseling with his girlfriend after he moved. The therapist highlighted the changes Robert had made in therapy and encouraged him to acquire a copy of ACT on Life Not on Anger (Eifert et al., 2006) to reinforce and strengthen his skills going forward. Due to clinic policies precluding contact with clients after termination, we were unable to collect follow-up data to evaluate maintenance of treatment gains.
11. Treatment Implications of the Case
The current case study highlights the utility of ACT as a transdiagnostic process-oriented intervention for problematic anger in a treatment-naïve man of low socioeconomic status who also presented with a history of substance abuse and depression. Notably, this approach did not target anger reduction directly, but rather a set of evidence-based processes that appear linked to problematic expressions of anger and other forms of human suffering (i.e., psychological inflexibility; Berkout et al., 2019). As such, treatment focused on undermining inflexible patterns of responding with difficult thought and emotions in favor of behaviors consistent with the Robert’s freely chosen values. Across 27 sessions, improvements were observed in both qualitative and quantitative assessments. Robert consistently reported therapeutic gains throughout sessions, suggesting treatment improved his overall functioning and quality of life. As a client-centered approach, ACT appeared effective based on assessment of the therapeutic alliance, suggesting that both the treatment modality and therapist were a good fit for Robert.
12. Recommendations to Clinicians and Students
In hindsight, there are several suggestions that follow from the present case. First, when working with client’s presenting with problem anger, it is important to explore the struggle and efforts to control emotional experiences early (i.e., creative hopelessness), with particular attention to the long-term workability and costs of anger behaviors. This important work, in turn, is something a clinician will often need to return to throughout the course of therapy. Unless the client contacts the costs of anger and its management, they may readily take any intervention you offer and use it as another clever way to manage and control anger. This work may also include exploration of client beliefs about anger along with the myths of anger (Eifert et al., 2006).
Second, helping our clients act in ways that are consistent with what matters is the point of ACT and, in a way, the purpose of the work. As such, we encourage values work to be introduced early and to be brought into the therapeutic interaction often. In the process, the costs of problematic anger often damage, or get in the way of, what clients care about. However, not all clients may be ready for values work early on in treatment. Clients, especially those who are self-critical, may view values as an area of insufficiency and express challenges surrounding values work. In such cases, we encourage attention to other processes (e.g., acceptance and defusion) as it relates to barriers to one’s chosen values (e.g., noticing and opening to judgmental thoughts regarding values).
Third, the other intervention processes can be introduced in a values context to help clients change their relationship with what they think and feel so as to create space to do what they really care about. Thus, a client may continue to experience judgmental or critical thoughts, but now they can see them as they are and can choose not to feed them and instead move with them in the service of what they care about. Of course, this approach makes a distinction between anger the feeling and anger the action, with the action often leading to enormous suffering and costs. Additionally, measuring relevant ACT processes throughout treatment, rather than pre- and post-treatment, could elucidate key processes where clients are improving, remaining unchanged, or deteriorating. Such information could provide useful insights on where to focus treatment interventions.
Lastly, though the interventions described herein appear linear, it is recommended that therapists apply ACT flexibly, targeting the processes linked with psychological inflexibility and suffering as they arise in session. This is where our own work, particularly in identifying ACT processes in our own lives and as they emerge within us in the therapeutic interaction, can be helpful.
Footnotes
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article. John P. Forsyth is a co-author of ACT on Life, Not on Anger, but played no direct role in supervision or treatment of this case.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.