
Abstract
Subclinical symptoms of anxiety and/or depression may negatively impact individuals’ lives, as they impair daily functioning and increase the risk of developing emotional disorders (e.g., depressive and anxiety disorders, and others related). Accordingly, preventive interventions targeting individuals with subclinical symptoms are essential. Among these, transdiagnostic approaches have proven to be particularly suitable, especially the Unified Protocol for Transdiagnostic Treatment of Emotional Disorders (UP). The UP has recently been adapted for preventive contexts and has shown encouraging results, including significant reductions in negative affect. Despite these promising findings, existing adaptations are not specifically tailored to adults who present with subclinical symptoms of anxiety and/or depression. Thus, this study describes the implementation of a brief preventive version of the UP (UP-Prevent), which was delivered in a face-to-face group format across six two-hour sessions to three women with subclinical symptoms of anxiety and/or depression. Assessments were conducted at three time points (preprogram, postprogram, and three-month follow-up) and included measures of depressive and anxiety symptom severity, symptom-related impairment, emotion regulation difficulties, perceived functional impairment across domains (e.g., work, social activities, private leisure activities, interpersonal relationships), quality of life, positive emotions, and positive mental health. To evaluate changes, the reliable change index (RCI) was computed. Significant improvements were observed across participants in several variables, including anxiety symptoms and anxiety-related impairment, emotion regulation difficulties, and positive mental health. Participants reported high levels of satisfaction with the program, underscoring its acceptability and feasibility and highlighting the UP-Prevent as a promising intervention for individuals with subclinical symptoms.
Theoretical and Research Basis for Treatment
The experience of intense, unpleasant emotions, such as sadness and anxiety, has become increasingly prevalent in people’s daily lives, as reflected in the high prevalence of depressive and anxiety disorders and related conditions, which are commonly referred to as emotional disorders (EDs; Bullis et al., 2019). In Portugal, recent data indicate that anxiety and depressive disorders were the most prevalent mental health conditions in 2019, with prevalence rates of 9% and 6%, respectively (OECD & European Observatory on Health Systems and Policies, 2023). These symptoms negatively affect individuals’ lives, highlighting the importance of intervening not only when a diagnosis of ED is present but also at a preventive level to reduce the risk of symptom progression (Zhong et al., 2024) and the likelihood of developing a diagnosable disorder in the future. Subclinical symptoms are also relevant, as they have been shown to adversely affect individuals’ quality of life (Rodríguez et al., 2012) and daily functioning in social, familial, and occupational domains (Ketz et al., 2011). Additionally, individuals who experience these symptoms frequently seek help in primary health care settings, contributing to increased demand for mental health services and longer waiting times for an initial appointment (Ebert et al., 2018; Lee et al., 2019). In Portugal, this increasing demand is reflected in the steady annual increase in psychological consultations within the Portuguese National Health Service, with an average growth rate of approximately 12% (Entidade Reguladora de Saúde [ERS], 2023).
Transdiagnostic treatments have emerged as valuable options for intervention in preventive contexts, as they provide a relatively comprehensive understanding of mental health difficulties and accurately reflect the complexity of clinical settings (Ornelas & Moreira, 2024). These approaches focus on the shared underlying mechanisms of ED (e.g., neuroticism) that contribute to the development and maintenance of these mental conditions (Sauer-Zavala et al., 2017). Transdiagnostic interventions, such as the Unified Protocol for Transdiagnostic Treatment of Emotional Disorders (UP; Barlow et al., 2018), offer several advantages, including the possibility of implementation in a group format, which allows clinicians to work simultaneously with multiple individuals with a range of symptoms and comorbid conditions (Ornelas & Moreira, 2024). According to these authors, they also reduce the training burden for mental health professionals and facilitate broader dissemination, as they allow clinicians to be trained in a single-protocol design to address a broad range of emotional disorders.
The UP is a manualized intervention based on cognitive behavioral therapy (CBT) principles and comprises eight modules (Barlow et al., 2018; Sauer-Zavala et al., 2017). It aims to enhance tolerance of frequent and intense emotions while promoting the development of more adaptive strategies to regulate emotions (Barlow et al., 2018). The UP has been delivered across multiple formats, including face-to-face and online, as well as in individual and group settings (Pedro et al., 2025; Schaeuffele et al., 2024). Evidence supports its efficacy across a range of mental conditions, particularly depressive and anxiety disorders (Cassiello-Robins et al., 2020; Schaeuffele et al., 2024), and across diverse populations (e.g., children, adolescents, and adults; Carlucci et al., 2021). In addition to reducing psychological symptoms (e.g., anxiety and depression), the UP has been associated with significant improvements in emotion regulation, mindfulness, and quality of life (Pedro et al., 2025).
Recently, the UP has been adapted for preventive contexts (Castro-Camacho et al., 2022; Martinez- Borba et al., 2022; Socias-Soler et al., 2024), with existing adaptations implemented in a variety of formats. Some authors have developed brief workshops and online courses (2 hr; Bentley et al., 2017; Sauer-Zavala et al., 2021), whereas others have tested multisession versions delivered face-to-face (six sessions; Castro-Camacho et al., 2022), online (five sessions; Socias-Soler et al., 2024), and in a hybrid format (Martínez-Borba et al., 2022). The results of these studies have been encouraging, as they demonstrated reductions in symptoms of anxiety, depression, and stress (Castro-Camacho et al., 2022), difficulties in emotion regulation (Socias-Soler et al., 2024), and neuroticism, as well as improvements in quality of life (Bentley et al., 2017), suggesting that the UP can be applied in preventive contexts. However, the literature has also highlighted several limitations, namely, the need for more diverse and representative samples (Castro-Camacho et al., 2022) and the development of longer duration formats (i.e., longer than 2 hr), which could generate more significant effects (Sauer-Zavala et al., 2017, 2021). On the basis of these findings, our research team developed a brief preventive version of the UP (UP-Prevent), which comprises six face-to-face group sessions, each lasting 2 hr, for adults presenting subclinical symptoms of anxiety and/or depression.
To the best of our knowledge, no preventive versions of the UP have been adapted for adults with subclinical symptoms, a population in which early intervention is crucial to prevent the exacerbation of difficulties and the onset of a mental disorder. The aim of this study was to assess the acceptability and feasibility of the preventive version through a case study with three participants presenting subclinical symptoms of anxiety and/or depression. Therefore, a detailed description of each session of the group-based UP-Prevent program is presented, along with an analysis of changes in symptom severity and impairment, emotion regulation difficulties, quality of life, and positive mental health, which were assessed at three time points (preprogram, postprogram, and three-month follow-up). Participants’ acceptability and satisfaction were also evaluated through individual interviews with the participants regarding their experiences in the program.
Case Introduction
This case study involved a group of three Portuguese women, aged between 22 and 37 (M = 30.33, SD = 7.64), who participated in the program over a six-week period. The participants enrolled voluntarily and participated in the program in person. With respect to marital status, one participant was married, one was single, and one was in a de facto union. To ensure their anonymity, the following pseudonyms are used: Maria, Joana, and Teresa.
All the participants presented subclinical symptoms of anxiety, whereas Joana and Teresa also exhibited subclinical symptoms of depression, as reflected in their scores on the Patient Health Questionnaire (PHQ-9; Ferreira et al., 2018; Kroenke et al., 2001) and the Generalized Anxiety Disorder-7 (GAD–7; Sousa et al., 2015; Sptizer et al., 2006) and confirmed during individual clinical interviews. Maria scored 3 on the PHQ-9 and 6 on the GAD-7; Joana scored 8 on the PHQ-9 and 9 on the GAD-7; and Teresa scored 7 and 10, respectively.
Presenting Complaints
The UP-Prevent study was disseminated through posts specifically created for the project on social media platforms (e.g., Facebook and Instagram), as well as through mental health professionals from the clinical psychology unit at the host institution.
Participants predominantly exhibited subclinical symptoms of anxiety, with Joana and Teresa also presenting subclinical symptoms of depression. All participants reported emotional difficulties, including experiences of guilt and shame at certain moments in their lives, which were associated with significant discomfort. Difficulties in emotional regulation were also evident, particularly in relation to uncertainty and unpredictability, as illustrated by Joana’s statement (“I like to know what is going to happen, so I can prepare myself and know what to do”), as well as tendencies toward worry and rumination about past events, as described by Teresa (“I keep thinking about situations that happen and about what I said, almost every day”). These difficulties were further reflected in Maria’s and Teresa’s reduced capacity to fully experience or appreciate their daily activities, with Teresa also reporting decreased engagement in activities she would typically enjoy.
At the individual level, participants reported additional difficulties across different domains. Maria described difficulties in delegating and refusing tasks at work, in saying no when asked for help, and in expressing her opinions calmly and clearly when others held differing views. Joana, in turn, reported struggling to manage her anxiety in social situations, particularly with unfamiliar people. She acknowledged avoiding social events (e.g., invitations from her friends) where she did not know others well, either by making excuses not to attend or by limiting her interactions with familiar friends. She also found situations involving public speaking (e.g., oral presentations) especially challenging, as these often triggered fears of being criticized, not being perceived as interesting, or not knowing what to say (“I want others to like me”). In such contexts, she reported experiencing physical symptoms of anxiety, including dry mouth, sweating, a racing heartbeat, chest tightness, and trembling hands.
Similarly, Teresa reported difficulties with public speaking and expressing her opinions in front of others. Additionally, she described difficulties managing negative automatic thoughts, as these negatively affected her well-being and often led her to focus on adverse aspects of situations. In line with Joana’s experience, Teresa reported physical symptoms such as strong palpitations, feelings of heat, and a sense of loss of control.
Overall, both Joana and Teresa tended to avoid public speaking whenever possible; however, when avoidance was not feasible, they experienced significant discomfort in these situations.
History
Among the three participants, Joana and Teresa had previously received individual psychological counseling (CBT) at another stage in their lives. However, for all three participants, this was their first experience with group psychotherapy, namely, a transdiagnostic approach, and none of the participants were on medication or receiving psychiatric treatment at the time. With respect to family history, Maria and Teresa reported a history of anxiety and obsessive‒compulsive disorder, respectively.
Assessment
To enroll in the UP-Prevent program, participants completed a registration protocol that included sociodemographic and clinical questions, as well as the Portuguese versions of the PHQ-9 (Ferreira et al., 2019) and the GAD-7 (Sousa et al., 2015), to assess the presence and severity of depressive and anxiety symptoms. Participants who scored between 5 and 9 on both the PHQ-9 and the GAD-7 were then required to proceed to a clinical interview. These criteria were determined on the basis of prior research involving subclinical populations using these instruments (e.g., Sousa et al., 2015; Wong et al., 2018). Notably, Teresa obtained a score above the established cutoff on the GAD-7 (10 points). Nevertheless, the research team decided to proceed with a clinical interview to assess the presence of subclinical symptomatology. After providing informed consent, the three participants were assessed for subclinical symptoms of anxiety and/or depression by a clinical psychologist (first author) through a synchronous online interview using the Structured Clinical Interview for DSM-5 (SCID-5; First et al., 2017). During the interviews, particular attention was given to the onset and severity of the difficulties, as well as to the degree of interference and distress in participants’ daily lives (Grenier et al., 2011; Rodríguez et al., 2012). The interview confirmed that Teresa met the criteria for inclusion in the study.
Maria, Joana, and Teresa completed a web-based assessment protocol (through LimeSurvey) at three time points (preprogram, postprogram, and three-month follow-up), using the questionnaires described below.
Patient Health Questionnaire-9 (Ferreira et al., 2018; Kroenke et al., 2001). The PHQ-9 consists of nine items (e.g., “Feeling down, depressed, or hopeless”) designed to assess the severity of depressive symptoms. Each item is rated on a 4-point response scale from 0 (not at all) to 3 (nearly every day). Total scores vary between 0 and 25 points, with scores above nine suggesting the presence of major depressive symptoms. This measure has shown acceptable psychometric properties in the Portuguese population, with a Cronbach’s alpha of .75 (Ferreira et al., 2018).
Generalized Anxiety Disorder-7 (Sousa et al., 2015; Sptizer et al., 2006). The GAD-7 is a self-report questionnaire consisting of seven items (e.g., “Not being able to stop or control worrying”) scored on a 4-point response scale ranging from 0 (not at all) to 3 (nearly every day). It is used as a screening instrument to assess the severity of generalized anxiety disorder and has been used to assess anxiety symptoms more broadly (Crockett et al., 2020; Socias-Soler et al., 2022). The total scores range from 0 to 21, with higher scores indicating greater severity of anxiety symptoms. The GAD-7 has demonstrated good psychometric properties in the Portuguese population, with a Cronbach’s alpha of .88 (Sousa et al., 2015).
Overall Anxiety Severity and Impairment Scale (OASIS; Norman et al., 2006; Pereira et al., 2023). The OASIS is a five-item self-report measure (e.g., “When you felt anxious, how intense or severe was your anxiety?”) that evaluates anxiety severity and associated functional impairment. Each item is rated on a 4-point response scale, with response options varying according to the item. Total scores range from 0 to 20 points, with higher scores indicating greater severity and functional impairment of anxiety symptoms. The OASIS has demonstrated good psychometric properties in the Portuguese population, with a Cronbach’s alpha of .89 (Pereira et al., 2023).
Overall Depression Severity and Impairment Scale (ODSIS; Bentley et al., 2014; Pereira et al., 2023). The ODSIS comprises five items (e.g., “During the past week, when you felt depressed, how intense or severe was your depression?”) and is designed to assess the severity and impairment of depressive symptoms. Items are rated on a 4-point response scale, with response options varying depending on the item. Total scores range from 0 to 20 points, with higher scores corresponding to greater depressive severity and functional impairment. In a Portuguese sample, the scale showed excellent psychometric properties, with a Cronbach’s alpha of. 95 (Pereira et al., 2023).
Work and Social Adjustment Scale (WSAS; Caetano et al., 2024; Marks, 1986). The WSAS is a self-report instrument that assesses patients’ perceived functional impairment. It consists of five items (e.g., “Because of my problems/symptoms, my ability to work/study is impaired”) covering five domains: work, home management, social leisure activities, private leisure activities, and relationships with others. Items are rated on an 8-point scale from 0 (not at all) to 8 (very severely). Total scores range from 0 to 40, with higher scores indicating greater functional impairment. The Portuguese validation demonstrated good psychometric properties, with a Cronbach’s alpha of .80 (Caetano et al., 2024).
Difficulties in Emotion Regulation Scale–Short Form (DERS-SF; Kaufman et al., 2015; Moreira et al., 2022). The DERS-SF is an 18-item self-report measure (e.g., “I pay attention to how I feel”) comprising six subscales: nonacceptance of emotional response, difficulties engaging in goal-directed behavior, impulse control difficulties, limited access to emotion regulation strategies, lack of emotional awareness, and lack of emotional clarity. Items are rated on a 5-point response scale ranging from 1 (almost never) to 5 (almost always). The total score ranges from 15 to 75 and is computed by summing 15 items, excluding the lack of emotional awareness subscale, in line with recommendations from the original Portuguese version (Moreira et al., 2022). Higher scores indicate greater difficulties in emotion regulation. The Portuguese version has shown excellent reliability, with Cronbach’s alpha values ranging from .92 (Clarity) to .98 (Nonacceptance and total score).
EUROHIS-QOL-8 (Pereira et al., 2011; Power, 2003). The EUROHIS-QOL-8 is a measure designed to assess overall quality of life. It consists of eight items (e.g., “How would you rate your quality of life?”) rated on a 5-point scale, with response options varying depending on the item. Total scores range from 0 to 100, with higher scores indicating a better perceived quality of life. A Portuguese validation study revealed excellent reliability (Cronbach’s alpha = .90; Pereira et al., 2011).
Positive Emotions Scale (Barlow et al., 2018). This measure was used to monitor the presence of positive emotions in individuals’ lives. This scale is part of the UP intervention and comprises five items (e.g., “I did not experience any positive emotions during the past week”) rated on a 4-point response scale, where response options vary depending on the item. The total score ranges between 0 and 20 points. Higher scores indicate greater levels of positive emotions. This scale has not yet been validated for the Portuguese population.
Mental Health Continuum-Short Form (MHC-SF; Keyes, 2009; Monteiro et al., 2020). The MHC-SF consists of 14 items (e.g., “During the past month, how often did you feel happy?”) assessing positive mental health across three dimensions: emotional, social, and psychological well-being. It uses a 6-point response scale ranging from 0 (never) to 5 (every day), yielding total scores from 0 to 70. Higher scores indicate better positive mental health. The Portuguese version has demonstrated good psychometric properties, with a Cronbach’s alpha of .89 (Monteiro et al., 2020).
Moreover, at the end of the program, individual interviews were conducted by psychologists with training and experience in implementing the UP to assess the program’s acceptability and satisfaction. For this purpose, the research team developed an interview guide consisting of a set of questions about the program’s structure (e.g., “What is your opinion regarding the total number of sessions?”) and content (e.g., “What is your opinion regarding the content covered in the program?”), as well as participants’ experiences and engagement in the program. Participants provided informed consent for audio and video recording. The interviews were transcribed verbatim, anonymized, and used for qualitative analysis.
Case Conceptualization
Considering the difficulties and characteristics presented by the participants, the case conceptualization was developed in accordance with the UP (Barlow et al., 2018), identifying (a) the problems/difficulties presented, (b) intense and uncomfortable emotions, (c) aversive reactions, and (d) each participant’s efforts to avoid or escape these emotions. With regard to the main difficulties, all three participants identified anxiety as the most frequently experienced emotion, as well as the emotion causing the greatest discomfort and interference in their lives. Additionally, they recognized the presence of other intense and uncomfortable emotions, such as sadness, guilt, and shame. Maria, Teresa, and Joana reported adverse reactions to these emotions or to specific components of them (e.g., thoughts, physical sensations, behaviors). For instance, Maria stated, “When I’m more anxious, I experience episodes of intense crying, and I feel foolish,” and Teresa reported, “I don’t want to feel this (anxiety). I feel I can’t enjoy the good things”. Finally, regarding efforts to avoid or suppress anxiety, the three participants engaged in avoidance behaviors. For example, Maria tried not to discuss certain topics to avoid creating conflict with others. Joana, whenever possible, avoided giving presentations or speaking in public; when invited to social events with unfamiliar people, she sometimes made excuses not to attend, or if she did attend, she limited her interactions to close friends. Teresa tended to avoid talking about herself or expressing her opinions in groups, and when she did, she consistently emphasized that these reflected only her personal perspective. She also avoided volunteering to deliver training sessions to other team members at her workplace. All three participants exhibited cognitive avoidance behaviors, such as rumination about past events. Joana also displayed some procrastination behaviors (e.g., initiating academic written assignments), and when visiting new places, she sometimes preferred to be accompanied so that the other person could take the lead in potential social interactions (i.e., safety behaviors).
Course of Treatment and Assessment of Progress
Therapists
The UP-Prevent was implemented by two psychologists (therapist and cotherapist), both of whom held a master’s degree in clinical and health psychology and had received training in implementing the UP. Moreover, both professionals had clinical experience in implementing the UP in individual and group formats.
Course of the Treatment
Structure, Objectives, Exercises, and Weekly Challenges of UP-Prevent Sessions
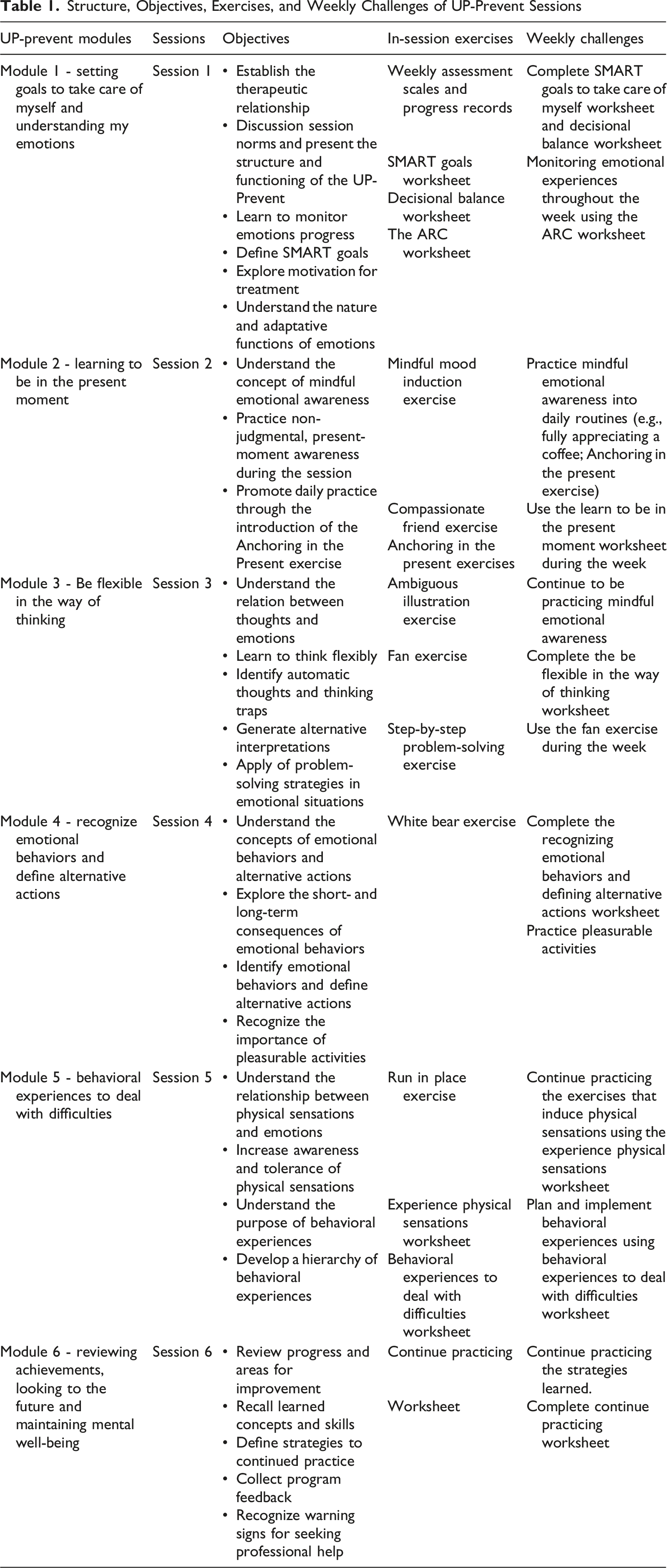
Although this was a brief version of the UP, the patient workbook from the original version was provided to the participants (Barlow et al., 2018/2023), who were informed that the session content represented a simplified and adapted version of the workbook that reflected the preventive focus and reduced symptom severity. In addition, the Weekly Challenge Booklet was developed, containing key information about the program, including objectives, participation norms, characteristics of emotional disorders, and worksheets for weekly challenges. Moreover, at the end of the sessions, digital materials and resources were emailed to the participants, allowing them to access the content as needed and practice the exercises between sessions.
Module 1 - Setting Goals to Take Care of Myself and Understanding My Emotions
The session began with introductions, during which participants acknowledged slight discomfort with the group setting. In the first part of the session, the therapists presented the session norms, as well as the UP-Prevent modules and objectives, emphasizing the importance of weekly emotion monitoring throughout the program. In the second part of the session, the SMART goals (S: specific; M: measurable; A: achievable; R: relevant; T: time-limited) were introduced, and participants identified areas of difficulty, formulated concrete goals, and broke the goals into small steps. Some of these goals and small steps were shared within the group (e.g., Joana’s goal was “Spend less time on screens (e.g., phone)”). Motivation was also discussed, and decisional balance exercise was carried out collectively. Psychoeducation on emotions (e.g., fear, joy, anxiety) and their adaptive function was provided, and the ARC model (A: antecedent; R: response: thoughts, physical sensations, behaviors; C: consequences) was introduced to help participants identify what occurred before, during, and after each intense emotion. Participants’ examples were used to illustrate the completion of the worksheet. By the end of the session, participants reported that their initial discomfort and fears related to being in a group and interacting with people they did not know had dissipated.
Module 2 - Learning to Be in the Present Moment
At the beginning of the second session, the SMART goals and the ARC form were reviewed. Teresa and Maria reported difficulties setting boundaries and saying no in certain situations (e.g., in response to requests for help or invitations) and set a goal of becoming more assertive and developing the ability to refuse requests. Teresa provided an example: “At times, I’m tired and in need of rest; however, when my family invites me to an activity, I still attend, as I fear disappointing them”. All the participants found the ARC form useful and completed it. Teresa shared an example of a personal situation: (a) situation: a colleague called and said the hospital service was chaotic and she thought she would be the team leader next day; (b) emotion: anxiety; (c) thoughts: “everything is going to go wrong and I won’t be able to handle it”; (d) physical sensations: chest tightness, tachycardia (e) behaviors: speaking harshly to others and avoiding her supervisor; (f) consequences: short-term relief, long-term continued lack of confidence in taking on the team leader role. To develop mindful emotional awareness, a brief mood-induction exercise using a video was provided to evoke emotions. The video portrayed the story of an older adult who spent Christmas alone and staged his death in order to reunite the entire family. Participants and therapists reflected together on the emotions (Joana stated, “In the beginning, I felt sadness and then happiness when the family was together”), thoughts (Teresa reported, “I thought this was a reality these days… In my previous job, I often encountered older people who were alone and lacked family support”, and behaviors that arose and discussed any tendencies to judge or suppress these emotions. The participants reported that the video reminded them of past experiences or prompted them to imagine similar future situations. Maria had a strong emotional response (i.e., crying) and expressed self-judgment (“I wish I didn’t have this reaction”). The concept of emotional awareness was introduced, followed by the “compassionate friend” exercise.
Module 3 – Be Flexible in the Way of Thinking
The session began with Teresa reporting having had a very good week, noting that she was able to fully enjoy several moments. Joana stated that she had become more aware of when she was not in the present (“I realized I would spend a lot of time living in the future”). The second part of the session focused on the role of thoughts in emotional experiences, highlighting how our interpretations influence emotions and behaviors. To illustrate this, the ambiguous illustration exercise was conducted, where participants first shared their initial interpretation of an image (e.g., “the woman passed away”) and then generated multiple alternative interpretations (e.g., “she might be fine; perhaps she just had a baby”). A subsequent group reflection emphasized the role of negative automatic thoughts, the importance of questioning their accuracy, and the need to adopt more flexible thinking to promote adaptive responses to situations. The concept of problem-solving was then introduced. Since Maria was absent, she was advised to read the corresponding manual chapter on cognitive flexibility.
Module 4 - Recognize Emotional Behaviors and Define Alternative Actions
In session 4, Maria reported practicing emotional awareness and reading the recommended chapters. Joana reported that she started a postponed report during the week and was close to finishing it (“I had been putting it off because I thought I wasn’t motivated enough”). Teresa mentioned that she had started structuring a project she planned to present to her supervisor. In the second part of the session, the concept of emotional behaviors was introduced, emphasizing the importance of recognizing when such behaviors maintain existing difficulties. To illustrate this, the short- and long-term consequences of emotional behaviors were discussed, and the white bear exercise (thinking about a white bear for 1 min, followed by 1 min of instructed not thinking about it) was conducted to demonstrate the effects of avoidance. Moreover, the participants reflected on their own emotional behaviors. Joana acknowledged that when feeling sad, “I try to distract myself,” while Teresa shared that she tends to avoid giving presentations or engaging in certain conversations. All the participants also acknowledged that they tended to respond more harshly to others when they felt angry/anxious. The concept of alternative actions was then introduced, and Joana shared an example to illustrate how to complete the Recognizing Emotional Behaviors and Defining Alternative Actions worksheet. The importance of incorporating pleasant activities into daily routines was emphasized.
Module 5 - Behavioral Experiences to Deal With Difficulties
Session 5 began with Joana reporting difficulties in defining alternative actions; she illustrated this with a situation from that week recorded in the Recognizing Emotional Behaviors and Defining Alternative Actions worksheet. She shared the following example: (a) situation: speaking with someone she did not know well; (b) emotion: anxiety; (c) emotional behavior: avoiding the conversation and subsequent ruminating; (d) alternative actions: using breathing techniques and practicing self-kindness; (e) consequences: discomfort but a sense of progress toward her goals. In the second part of the session, the group discussed the role of physical sensations and how their interpretations influence emotional experience, as well as the long-term consequences of avoiding these sensations. Participants identified the physical sensations they found most uncomfortable during intense emotions (Joana: rapid breathing; Maria: rapid breathing and sensations of heat and sweating; Teresa: racing heartbeat). Teresa added, “When my heart begins to race, I feel as though it is in my throat. It’s awful.” To build tolerance, participants completed an in-session exercise eliciting typically avoided physical sensations (e.g., running in place for 1 minute across three trials with short breaks and then rating discomfort and similarity after each trial). The importance of planning behavioral experiences (e.g., situations, activities) to face intense emotions was introduced. Participants were encouraged to apply the skills learned and to respond to emotions more adaptively by identifying situations or activities to practice in daily life.
Module 6 - Reviewing Achievements, Looking to the Future and Maintaining Mental Well-Being
Participants began the last session by discussing that they had completed exercises designed to elicit physical sensations, as well as behavioral experiences to address their difficulties. Joana performed the straw-breathing exercise, Maria practiced running and climbing stairs, and Teresa used a stationary bike and attended a social event involving uncomfortable interactions. The participants subsequently reflected on their progress (Teresa stated, “I notice that I am calmer and less impulsive”). The weekly scores from self-report measures were also reviewed, and the participants were invited to share their feedback about the UP-Prevent. Joana mentioned, “I found the program very useful, including challenges and many helpful strategies.” Maria reported, “I frequently use cognitive flexibility and discuss this skill with those around me.” Although this was the final session, the importance of continuing to practice learned skills was emphasized, and it was highlighted that there was still room for improvement. A summary of all program skills was presented, and participants were encouraged to use the Continue Practicing worksheet to plan for ongoing application. Finally, strategies for preparing for future difficulties, such as setting new goals and monitoring emotions, were discussed, along with warning signs indicating a potential increase in difficulties and the need to seek professional help.
Assessment of Progress
To monitor the participants’ emotions throughout the program, some measures were administered via LimeSurvey at the beginning of each weekly session to assess symptoms of anxiety (OASIS) and depression (ODSIS), positive emotions (Positive Emotions Scale), and positive mental health (MHC-SF).
During the program, the therapists observed notable improvements among the participants, particularly in their emotional and behavioral awareness, ability to identify negative automatic thoughts, and increased use of cognitive flexibility as a strategy, as evidenced by the participants’ examples, self-reports, and in-session behavior. Maria, Joana, and Teresa also showed an improved ability to recognize the consequences of emotional behaviors and to engage in more adaptive alternative actions. To analyze changes in self-report measures between the pre- and postprogram assessment, the reliable change index (RCI; Jacobson & Truax, 1991; Tingey et al., 1996) was computed using the following formula:
Normative data for each measure were used in the calculation of the RCI: PHQ-9 (
Outcome Scores and Reliable Change Index (RCI) at Pre and Post-Program, and 3-Month Follow-Up
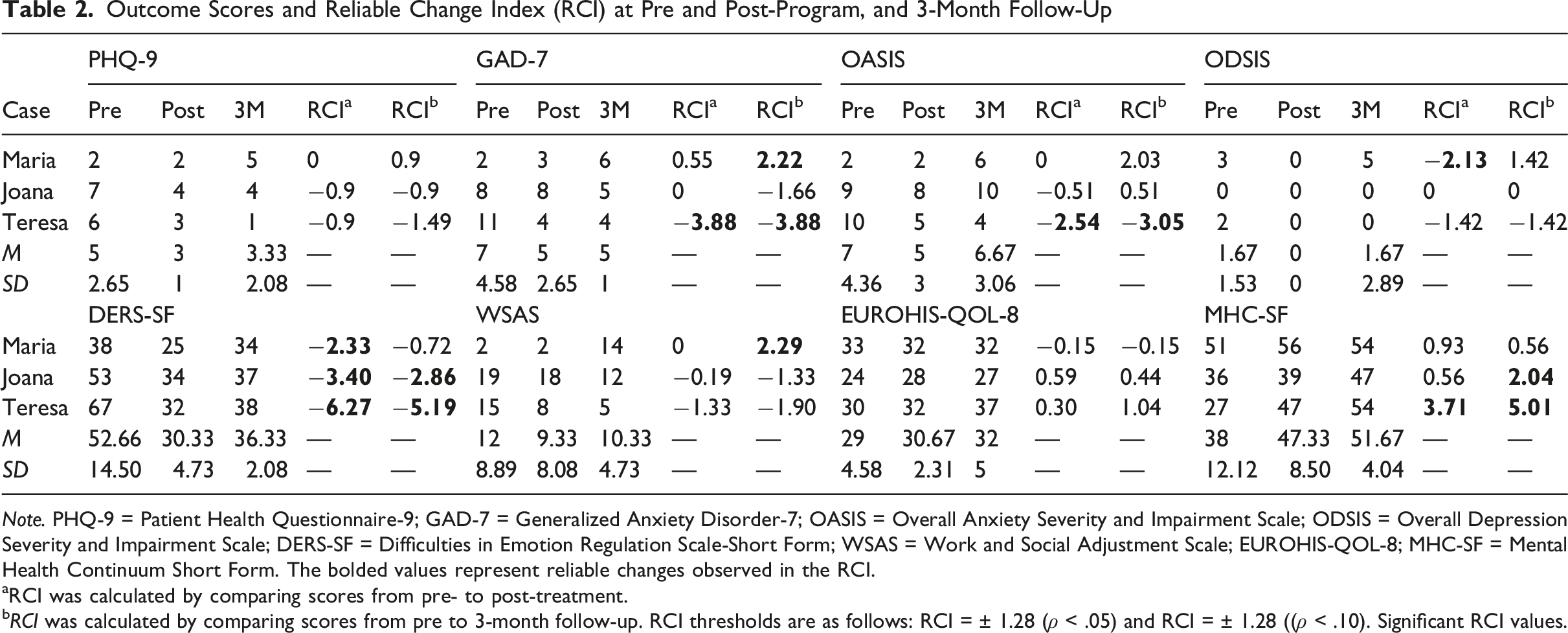
Note. PHQ-9 = Patient Health Questionnaire-9; GAD-7 = Generalized Anxiety Disorder-7; OASIS = Overall Anxiety Severity and Impairment Scale; ODSIS = Overall Depression Severity and Impairment Scale; DERS-SF = Difficulties in Emotion Regulation Scale-Short Form; WSAS = Work and Social Adjustment Scale; EUROHIS-QOL-8; MHC-SF = Mental Health Continuum Short Form. The bolded values represent reliable changes observed in the RCI.
aRCI was calculated by comparing scores from pre- to post-treatment.
bRCI was calculated by comparing scores from pre to 3-month follow-up. RCI thresholds are as follows: RCI = ± 1.28 (ρ < .05) and RCI = ± 1.28 ((ρ < .10). Significant RCI values.
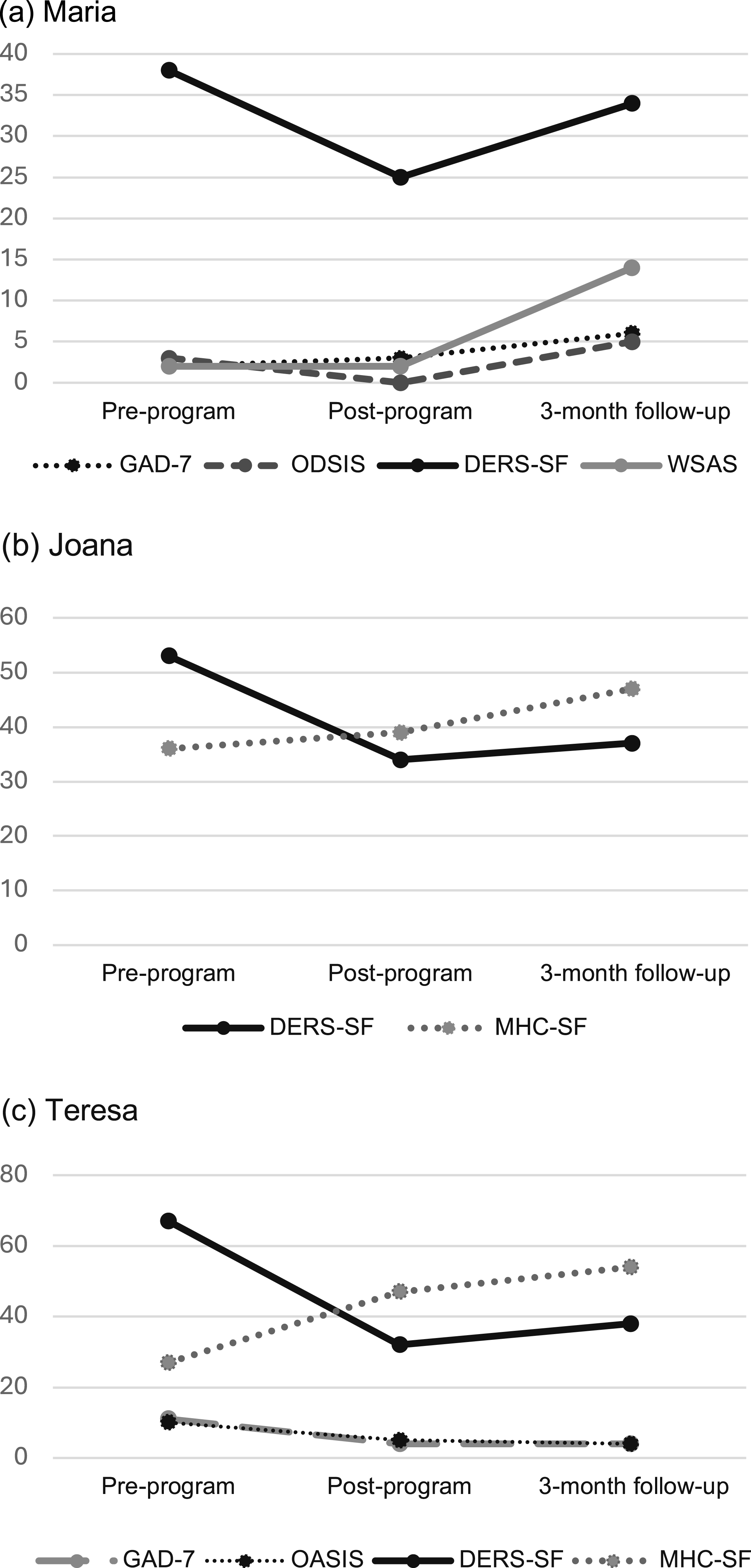
Observed improvements across assessment time points for three participants.
Acceptability and Satisfaction
Participants reported high levels of satisfaction and attendance throughout the program. All acknowledged the benefits of the group format. For example, Joana stated, “We end up identifying with and connecting to the people in the group, giving us the feeling that we are not alone”. The participants also agreed that they would recommend this format to others seeking psychological support. This finding is particularly relevant given that some of the participants’ difficulties were explicitly related to expressing their opinions and speaking in public or with people they did not know well. Such situations are inherent to a group setting and could hinder group dynamics. Nevertheless, throughout the sessions, a safe environment characterized by identification, mutual support, and cooperation became evident. With respect to the program, they reported that the number of sessions, their frequency, their duration (2 hours), and the face-to-face format were appropriate. The participants also described the UP-Prevent as well structured and organized. They all emphasized the program’s practical nature, highlighting that the skills and strategies learned were useful and could be easily applied in daily life, particularly emotional awareness and cognitive flexibility, and reported that the number of weekly challenges did not constitute an overload. Maria further noted the importance of the ARC. Overall, they felt that the UP-Prevent helped them manage their difficulties, with Teresa affirming, “These weeks helped me a lot; it was fantastic.”
Complicating Factors
All the participants demonstrated high levels of engagement with the program. However, they did not always complete all the written records for the weekly challenges. Nevertheless, during the review of these challenges, it became clear that they had all applied the strategies and exercises learned to their daily lives. To facilitate the practice of these challenges, the therapists suggested that participants could use alternative ways of recording information, such as taking notes on their mobile phones or recording audio reflections on the application of the exercises in their everyday routines. Furthermore, whenever necessary, and following the group guidelines proposed by Bullis et al. (2015), additional time was devoted to reviewing the weekly challenges to ensure that the questions were clarified and that the skills were consolidated. Between sessions 4 and 5, it was necessary to extend the interval between sessions so that Maria would not miss session 5, as she was unable to attend it for professional reasons. This longer interval allowed the participants to practice and consolidate the newly learned skill.
Access and Barriers to Care
There were no major barriers to the implementation of the UP-Prevent, as participation involved no financial costs, and the manuals were provided to participants free of charge. The only expenses incurred were related to transportation to the clinical psychology unit. However, an important potential barrier is that the delivery of the UP program requires two therapists per session, which may pose logistical challenges. Session schedules were adjusted to accommodate participants’ needs and commitments, facilitating attendance for all three participants. When Maria was unable to attend a session, she was advised to read the corresponding module chapters, and time was allocated in the subsequent session to address any questions that might arise.
Follow-Up
A face-to-face follow-up session was conducted three months after the program was completed to (1) assess continued skill use, (2) evaluate ongoing exposure to difficult emotions, and (3) examine the maintenance of therapeutic gains. First, qualitative feedback was collected from each participant. Joana reported experiencing a challenging period since starting her master’s program, as she did not yet know her classmates and was attempting to integrate, which contributed to anxiety and discomfort. Despite this, she continued attending classes and applying the strategies in her daily life. She also described using alternative actions during class breaks. For instance, although her initial impulse was to remain alone in the classroom, she went into the corridor without her phone (a previously identified safety behavior) and approached someone she knew.
Maria reported a major life change after applying for a job abroad, which she was subsequently offered. Although she was initially excited, she later experienced increased anxiety and stress related to the upcoming transition and related preparations. During this period, she attempted to apply the strategies learned in the program, such as cognitive flexibility and mindful emotional awareness. She also reported feeling calmer and regaining excitement about the change at follow-up. Teresa mentioned feeling very well and explained that she had continued to practice the strategies, with a particular emphasis on cognitive flexibility.
After the follow-up session, the participants completed the same assessment measures administered before and after the program (see Table 2 and Figure 1). Joana maintained significant improvements in emotional regulation difficulties (DERS-SF) and showed a reliable increase in positive mental health (MHC-SF). Teresa maintained gains across all the assessed domains, including anxiety symptoms (GAD-7), anxiety severity and related impairment (OASIS), emotional regulation difficulties (DERS-SF), and positive mental health (MHC-SF). In contrast, Maria presented a significant worsening in anxiety symptoms (GAD-7) and perceived functional impairment (WSAS).
Treatment Implications
The present study aimed to evaluate the acceptability and feasibility of delivering the UP-Prevent in a face-to-face format to a group of three participants. The findings suggest that the UP-Prevent may be a promising, brief, preventive program for adults with subclinical symptoms of anxiety and/or depression, as significant changes were observed in some participants. The UP-Prevent appears to have had a positive effect on anxiety symptoms and related impairment, while also having a positive impact on participants’ emotion regulation difficulties and positive mental health, which is coherent with past studies (Castro-Camacho et al., 2022; Socias-Soler et al., 2024). These results are consistent with participants’ reports identifying anxiety as the emotion associated with the greatest distress and interference in their daily lives, which may explain the therapeutic gains observed. The observed improvements in emotion regulation difficulties are particularly important, as difficulties in emotion regulation are present across a wide range of psychological conditions, including emotional disorders. Accordingly, the literature emphasizes the need for interventions that directly address emotion dysregulation (Barlow et al., 2016). Moreover, the improvements observed in positive mental health support the concept that the UP-Prevent also promotes improved emotional well-being. In this sense, these results are consistent with the main objectives of the UP-Prevent, which include not only reducing subclinical symptoms but also promoting more adaptive emotion regulation strategies and enhancing positive emotions and overall mental well-being. Notably, Maria presented a different symptom trajectory than the other participants, with an increase in symptom severity observed at the 3-month follow-up. A possible explanation for this pattern is that during this period, the participant experienced a major life transition (i.e., preparing to move abroad to work), which, according to her report, was associated with elevated levels of anxiety. This account is consistent with her higher and more clinically significant scores on the GAD-7 and WSAS, which assess anxiety severity and patients’ perceived functional impairment, as well as with elevated—although not clinically significant—scores on the OASIS. Nevertheless, despite this increase in anxiety symptoms, Maria did not show significant reductions in variables such as quality of life or positive mental health. This pattern may suggest that although she experienced intense negative emotions (e.g., anxiety), positive emotions were also present and may have contributed to the maintenance of her perceived quality of life and positive mental health. This balance may also be understood in light of the skills and content acquired through the UP-Prevent, which also aims to promote better mental well-being. During the postprogram period and up to the 3-month follow-up session, none of the participants received additional psychological support.
With respect to the satisfaction and acceptability of the UP-Prevent, the participants reported high levels of satisfaction with the program’s format and content, perceived the intervention as highly useful, and emphasized the advantages of the group format. These findings are consistent with existing studies on the adaptations implemented to date and reinforce the acceptability of the UP as a brief, preventive group-based intervention (Castro-Camacho et al., 2022; Martínez-Borba et al., 2022; Socias-Soler et al., 2024).
Despite the valuable insights provided by this case study, some limitations should be acknowledged, and these findings should be interpreted with caution. The fact that the target population consisted of adults with subclinical symptomatology may have limited the potential for observable change, thereby reducing the magnitude of the intervention effects. This has been observed in previous research involving similar populations, where small effects are commonly reported because of the limited severity of baseline symptoms (Cuijpers et al., 2014). Moreover, in two sessions, the second therapist was unavailable, leaving the first therapist to conduct the sessions alone. Although this was manageable in the small group, such situations may be more challenging in larger groups. The exclusively female composition of the sample also limits the generalizability of the findings. However, this feature is consistent with evidence indicating that women are more frequently diagnosed with EDs (OEDC, 2025) and are more receptive to transdiagnostic, group-based interventions (Pedro et al., 2024). Finally, the reliance on self-report measures constitutes a further limitation, as these depend on subjective perceptions and may be influenced by response biases.
Recommendations to Clinicians and Students
From a clinical implementation perspective, the delivery of the UP requires therapists to have certified training in the protocol, as well as experience in group-based interventions. The findings of the present study are promising and contribute to the growing body of literature on the UP, particularly regarding its application in preventive contexts. Given that the UP-Prevent is a brief, transdiagnostic, group-based preventive program, further research is needed to establish its efficacy. Nevertheless, it may represent a valuable approach to addressing the current challenges in Portuguese mental health services, especially in primary care settings, where subclinical symptomatology is highly prevalent and frequently managed. As a short program, the UP-Prevent may be particularly suited to contexts characterized by high service demand and limited resources, which often restrict access to longer-term psychological interventions. As a preventive program, it aims not only to reduce subclinical anxiety and/or depressive symptoms but also to mitigate the risk of progression to full-threshold mental disorders while promoting overall mental well-being. Furthermore, its transdiagnostic framework and group format enable the targeting of shared underlying mechanisms across diverse symptom presentations while simultaneously increasing reach. This is especially relevant considering the high levels of comorbidity observed in clinical and community settings, as well as the long waiting lists commonly reported in these contexts.
Future studies should therefore examine the efficacy of the UP-Prevent in larger samples using randomized controlled trials, compare its effectiveness with control conditions, and assess the long-term maintenance of treatment gains. Additionally, incorporating therapist-rated observational measures alongside self-reported data would allow a more comprehensive assessment of change. As a next step, the research team intends to conduct a feasibility study to systematically assess implementation outcomes, including engagement, adherence and acceptability, in preparation for a larger-scale efficacy trial.
Footnotes
Acknowledgments
The authors would like to thank all the participants who enrolled in and took part in the program, the Clinical Psychology Unit at the host institution for providing the facilities in which the sessions were conducted.
Ethical Considerations
This project was approved by the Ethics Committee for Research of the host institution.
Consent to Participate
Informed consent was obtained from all participants included in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Center for Research in Neuropsychology and Cognitive and Behavioral Intervention (CINEICC) of the University of Coimbra (https://doi.org/10.54499/UIDP/00730/2020) and by a PhD grant (reference: 2022.13971.BD; ![]() ) from the Portuguese Foundation for Science and Technology (FCT).
) from the Portuguese Foundation for Science and Technology (FCT).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.