
Abstract
Purpose:
There is a lack of large-scale evidence regarding the prognostic impact of Chinese herbal medicine (CHM) on patients with lung cancer. This paper aimed to conduct a nationwide population-based study to investigate the role of CHM for patients with lung cancer with standard treatment.
Methods:
Patients diagnosed with lung cancer and treated with standard therapy between 2013 and 2015 were retrospectively identified from National Health Insurance Research Database and Taiwan Cancer Registry. Patients were classified into a CHM group and a non-CHM group based on prior medical records. Kaplan-Meier analysis was performed to estimate overall survival (OS) between each group.
Results:
A total of 7351 matched patients were included in the outcome analysis and comparison, with 3677 patients in the CHM cohort and 3674 patients in the non-CHM cohort. The mean age of our patients was 60.68 ± 11.26 years, and 56% of our patients were female. Our results demonstrates that patients who received CHM had significantly longer OS compared to those who did not receive CHM (HR: 0.59, 95% CI: 0.556-0.625, P < .0001). In subgroup analysis, survival differences were not significant for stage I-II disease, whereas OS was significantly better in the CHM group among patients with stage III-IV disease. Multivariable analysis showed CHM usage was found to significantly influence OS. The most commonly used single CHM was Hedyotis diffusa Willd and compound CHM was San-Zhong-Kui-Jian-Tang.
Conclusion:
Our nationwide population-based study suggested that CHM in conjugation with standard treatment was associated with improved survival in patients with advanced lung cancer. Integrating cancer treatment with CHM could be adopted in the treatment of lung cancer to improve prognosis.
Introduction
Lung cancer is one of the most prevalent and lethal forms of cancer globally. Characterized by uncontrolled cell growth in lung tissues, it is a significant public health concern that devastates millions of lives each year. According to the World Health Organization, lung cancer accounts for approximately 18% of all cancer deaths, making it the leading cause of cancer-related mortality worldwide. 1 Lung cancer incidence varies significantly across different geographical regions, with the highest rates observed in developed countries. 2 According to Global Cancer Observatory 2020 data, there were approximately 2.2 million new cases of lung cancer diagnosed worldwide. 3 Men have a higher incidence rate compared to women, largely due to historical smoking patterns and genetic predisposition. 4 Surgery is the standard treatment for early stage lung cancer, while chemoradiotherapy will be considered in patients with locally advanced lung cancer.5,6 Recently, several novel agents including targeted therapy and immune checkpoints inhibitors were demonstrated to prolong survival in metastatic non-small cell lung cancer (NSCLC)7,8 or extensive stage small cell lung cancer (SCLC). 9 Despite advances in treatment, the 5-year survival rate for lung cancer is approximately 19%, reflecting the challenges associated with early detection and treatment. 10 Furthermore, treatment-related toxicities remains a major concern during the treatment of lung cancer. Some patients experience severe adverse events leading to treatment discontinuation and poor prognosis. 11 Hence, the management of side effects becomes an important issue for patients with lung cancer.
In recent years, the integration of complementary and alternative medicine practices, particularly traditional Chinese medicine (TCM), has gained popularity among cancer patients. 12 TCM emphasizes a holistic approach to health by restoring balance within the body through herbs, acupuncture, dietary therapy, and lifestyle changes. Among the various components of TCM, Chinese herbal medicine (CHM) is prominently used, boasting centuries of empirical knowledge and a growing body of scientific research supporting its efficacy. 13 Several clinical studies have explored the effects of CHM on cancer patients, often focusing on its use as an adjunct to conventional treatments such as chemotherapy and radiotherapy. 14 Although several nationwide population-based studies using Taiwan’s National Health Insurance Research Database (NHIRD) have investigated the association between Chinese herbal medicine (CHM) and survival outcomes in lung cancer, important gaps remain regarding stage-specific effects, integration with validated cancer registry data, and contemporary treatment contexts. The present study aimed to conduct a nationwide, population-based propensity score–matched analysis integrating data from the National Health Insurance Research Database and the Taiwan Cancer Registry to evaluate the prognostic impact of CHM in patients with lung cancer receiving standard oncologic treatment. By incorporating validated AJCC staging information, performing rigorous 1:1 propensity score matching, and conducting stage-stratified survival analyses, we sought to clarify the real-world survival benefits of CHM, particularly in advanced-stage disease, and to characterize commonly prescribed herbal formulations in contemporary integrative lung cancer care.
Method
Data Sources
The data utilized in the present study were obtained from the National Health Insurance Research Database (NHIRD), which covers over 99% of the Taiwanese population. In addition, the Taiwan Cancer Registry (TCR) has comprehensive coverage, capturing more than 98% of potential cancer cases in Taiwan. Cancer diagnoses within the TCR are validated through histological or cytological examinations. This retrospective, nationwide, population-based study integrates data from both the NHIRD and TCR, which contain detailed information regarding cancer diagnosis, staging, and treatment modalities. The TNM staging in this study was based on the 7th edition of the American Joint Committee on Cancer (AJCC) staging system. All diagnoses recorded in the NHIRD and TCR are coded according to the International Classification of Diseases (ICD), 9th Revision, Clinical Modification and 10th Revision. To ensure patient privacy, all identification numbers are encrypted prior to database release. This study was approved by the Institutional Review Board of Fu Jen Catholic University (IRB No. C110199), and the requirement for individual written informed consent was waived because this was a retrospective analysis of NHIRD.
Study Population
In this population-based study, patients diagnosed with lung cancer (ICD-O-3 codes C33, C34) and treated with standard therapy between 2013 and 2015 were retrospectively identified from the TCR. Standard treatment was defined to include conventional lung cancer therapies reimbursed by the National Health Insurance system, including surgery, chemotherapy, radiotherapy, targeted therapy, and immunotherapy, as applicable to disease stage and clinical practice during the study period. Lung cancer patients who received only palliative hospice care without any active treatment were excluded from our study. The index date was defined as the date of the first recorded lung cancer diagnosis for each patient. The follow-up period extended from the index date until the date of death or the last available date in the NHIRD, which was December 31, 2021. Patients who received CHM, excluding acupuncture or traumatology therapies, in conjunction with standard treatment for more than 14 days were classified as CHM users. Patients without any records of CHM nor less than 14 days of CHM usage were classified as non-CHM users. The 14-day cutoff was selected based on conventions used in prior studies utilizing the National Health Insurance Research Database (NHIRD),15,16 where short-term CHM exposure is considered insufficient to reflect therapeutic intent or sustained use. Figure 1 provides a flow diagram illustrating the enrollment process for this study.

Flow chart of patients’ collection.
Covariates
Demographic characteristics evaluated in this study included gender, age, initial cancer stage, treatment status, and comorbidities. Comorbidities were assessed using the Charlson Comorbidity Index (CCI), as well as specific conditions such as hypertension (ICD-9 codes 401-405), chronic kidney disease (ICD-9 codes 585-586), and chronic hepatitis (ICD-9 codes 571-573). Comorbidities were included if they appeared in outpatient records at least twice or in inpatient records at least once within 1 year prior to the lung cancer diagnosis. A higher CCI score indicates a greater risk of mortality, suggesting the presence of multiple comorbidities, which can adversely impact the prognosis of lung cancer and related conditions.
Matching
To minimize selection bias between the 2 groups, we employed 1:1 propensity score matching. The propensity scores were calculated using logistic regression analysis, incorporating variables such as gender, age, CCI score, and clinical cancer stage. Patients with incomplete stage data were categorized as “other”.
Statistical Analysis
Between-group differences for continuous variables were assessed using the Student’s t-test, while categorical variables were analyzed using the Chi-square test. Kaplan-Meier analysis was performed to estimate overall survival (OS) between the matched study groups, and survival curves were plotted accordingly. OS was calculated from the date of initial diagnosis of lung cancer to the date of death or last follow-up. Mortality risks between the 2 cohorts were evaluated using hazard ratios (HR) with 95% confidence intervals (CIs). Multivariable Cox proportional hazards models were employed to assess lung cancer patient survival, adjusting for covariates such as age at diagnosis, pathology, treatment, comorbidities, and CHM use. All statistical analyses were conducted using SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA) and R software (version 4.4.1). A 2-sided P-value of less than .05 was considered statistically significant.
Results
Patients Characteristics
We identified patients diagnosed with lung cancer between 2013 and 2015 using data from the NHIRD and TCR (Figure 1). Among the 47 751 eligible patients, 3930 received CHM treatment, while 33 477 did not receive CHM. Following propensity score matching (PSM) using nearest neighbor matching, a total of 7351 matched patients were included in the outcome analysis and comparison, with 3677 patients in the CHM cohort and 3674 patients in the non-CHM cohort, ensuring balanced baseline characteristics for subsequent outcome comparisons. The distribution of patient characteristics between the CHM and non-CHM groups is summarized in Table 1. The average age in both groups was approximately 60 years, and the majority of patients were female. Additionally, the average age of patients in the non-CHM group was higher compared to that of the CHM group. Regarding pathological type, non-small cell lung cancer was the predominant category in both groups. No significant differences were observed between the 2 groups in terms of gender, age, CCI score, and cancer stage.
Baseline Characteristics of the Patients with All Stage Lung Cancer.

Abbreviations: CHM, Chinese herbal medicine; SD, standard deviation; CKD, chronic kidney disease; CCI, Charlson comorbidity index.
Overall Survival
The Kaplan-Meier survival curve for overall mortality across all cancer stages is presented in Figure 2. The figure demonstrates that patients who received CHM had significantly longer OS compared to those who did not receive CHM, accounting for 3.6 versus 2.4 years (HR: 0.59, 95% CI: 0.556-0.625, P < .0001).

Overall survival of all stage of lung cancer.
Subgroup Analysis With Clinical Stage
Our patients were then stratified according to their stage. Table 2 summarizes the characteristics of patients across cancer stages I to IV. The Kaplan-Meier survival curves for mortality in each cancer stage are presented in Figure 3. The results indicate that for stage I (P = .9) and stage II (P = .67) patients, those who received CHM had longer OS compared to those who did not receive CHM, although the differences were not statistically significant. In contrast, for stage III (P < .0001) and stage IV (P < .0001) patients, CHM users demonstrated significantly better OS compared to non-CHM users.
Basic Characteristics of Stage I-IV Lung Cancer After PSM.
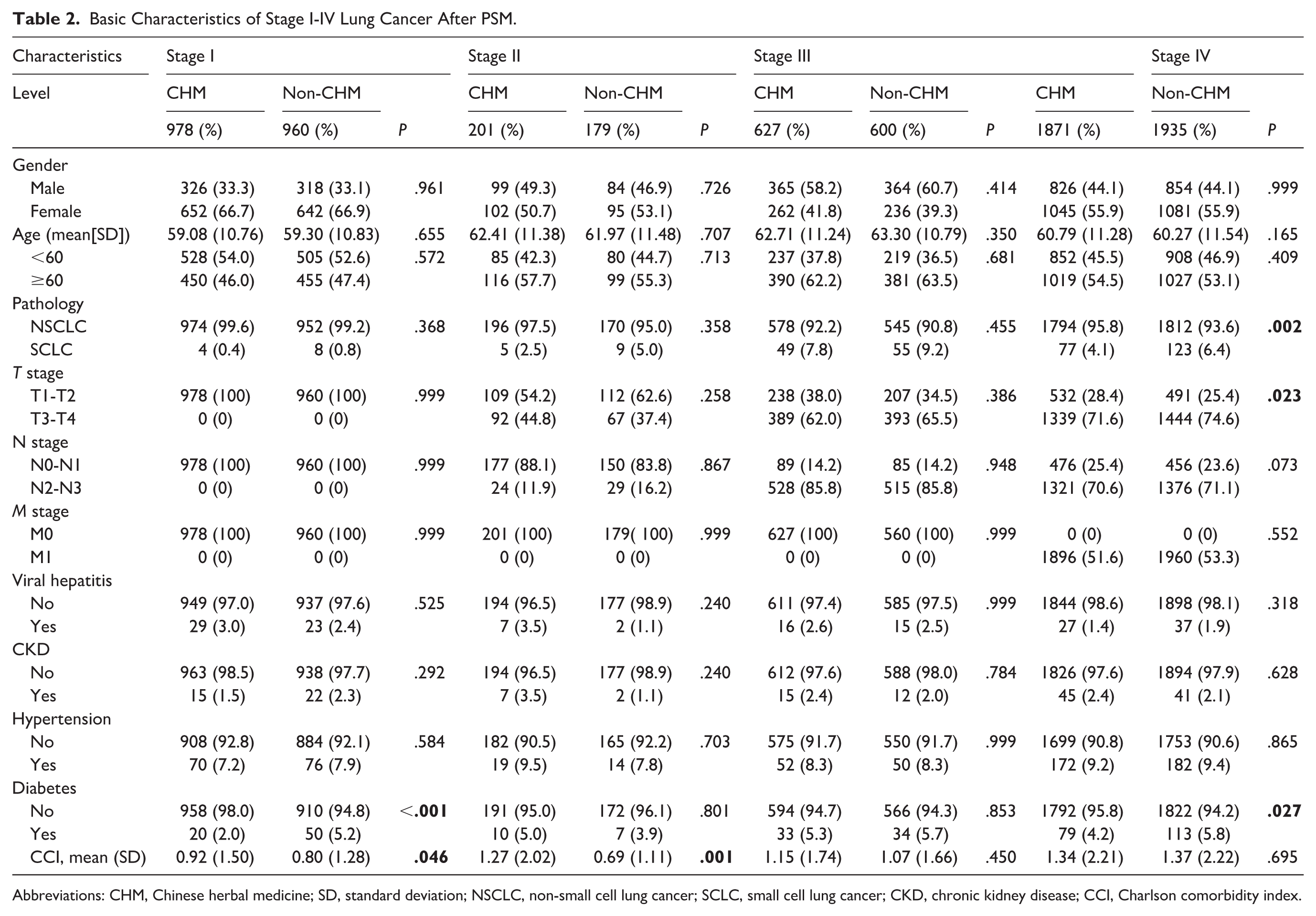
Abbreviations: CHM, Chinese herbal medicine; SD, standard deviation; NSCLC, non-small cell lung cancer; SCLC, small cell lung cancer; CKD, chronic kidney disease; CCI, Charlson comorbidity index.
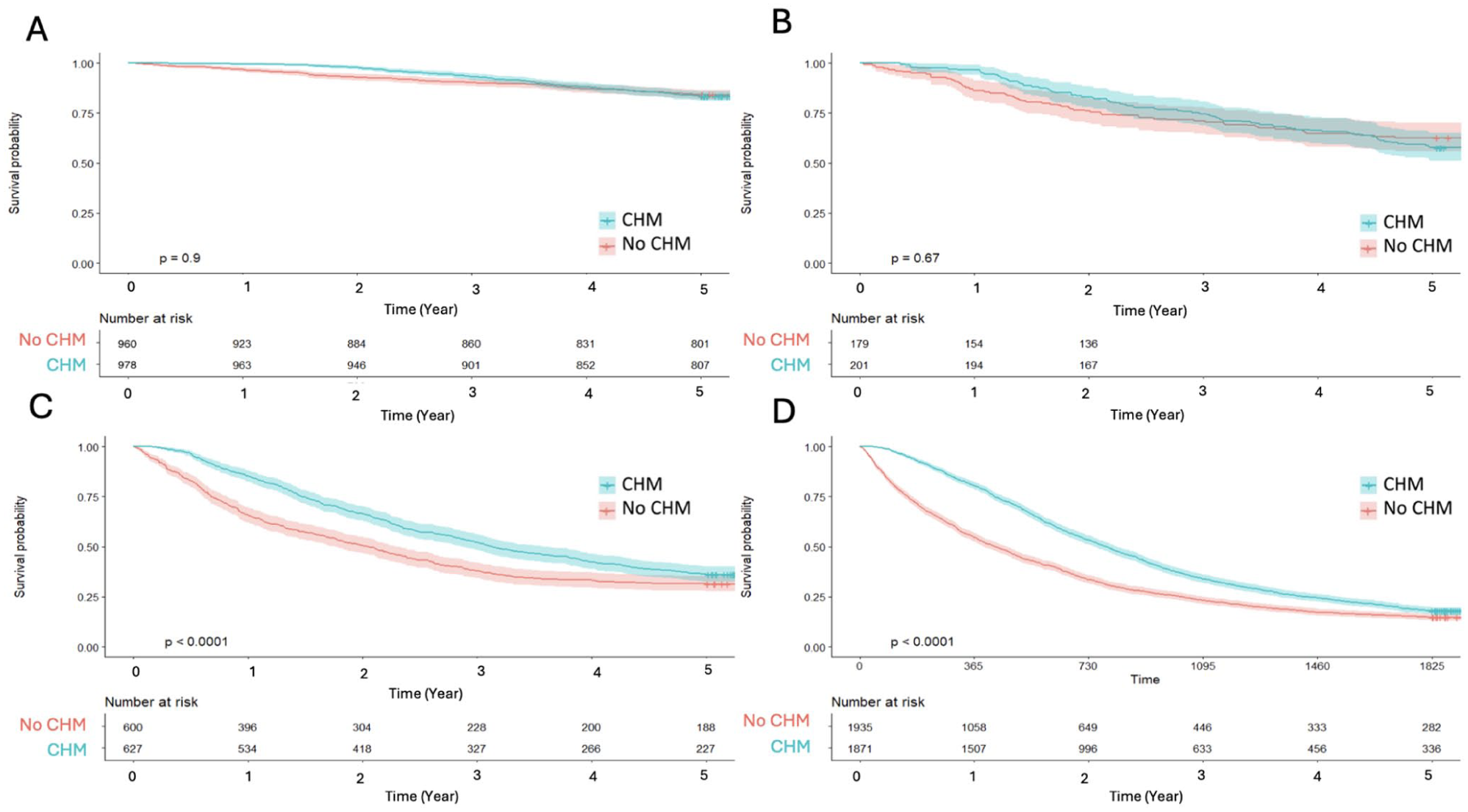
Overall survival of lung cancer patients, stratified by stage: (A) stage I, (B) stage II, (C) stage III, and (D) stage IV.
Univariate and Multivariate Analysis
Table 3 presents the results of Cox regression analysis for mortality, expressed as HR with 95% confidence intervals. In the univariate analysis, age group, hypertension, and chronic hepatitis were not found to have significant effects on mortality outcomes in lung cancer patients. In the multivariable analysis, after adjusting for potential confounding factors, variables including CHM usage, gender, age group, pathology type and cancer stage were found to significantly influence 5-year mortality.
Cox Regression Analysis of OS in Patients with All Stage Lung Cancer.

Abbreviations: HR, hazard ratio; CHM, Chinese herbal medicine; NSCLC, non-small cell lung cancer; SCLC, small cell lung cancer.
Commonly Used CHM in Lung Cancer
Table 4 displays the 10 most commonly used CHM among patients with stage III and stage IV lung cancer, categorizing these herbal medicines into single and compound formulations. For patients with stage III-IV lung cancer, the most commonly used single CHM was Hedyotis diffusa Willd and most commonly used compound CHM was San-Zhong-Kui-Jian-Tang.
Top 10 Most Commonly Used Chinese Herbal Medicine in Stage III and Stage IV Lung Cancer Patients.

Discussion
To the best of our knowledge, this is one of the largest nationwide population-based propensity score–matched analyses integrating NHIRD and TCR data to evaluate the stage-specific prognostic impact of CHM in lung cancer. Our study included the largest cohort and provided a real-world evidence for physicians who treated patients with lung cancer. Our result showed that lung cancer patients treated with standard care and CHM concomitantly had longer survival than those who received standard care alone without CHM. After subgroup analysis, the survival benefits were robust in patients with stage III-IV lung cancer. Multivariate analysis also demonstrated the superior prognosis of CHM in patients with lung cancer. Our conclusion highlighted again the importance of supportive treatment like CHM. Under CHM support, lung cancer patients continued the standard of care and prolonged longest survival. Interestingly, our study also disclosed that patients with advanced lung cancer benefited from CHM support the most, while patients with early-stage lung cancer derived modest benefit from CHM support. The reasons were unclear. One possible explanation might be advanced-stage patients may derive greater benefit from symptom control, immune modulation, or treatment tolerance enhancement provided by CHM, whereas early-stage patients already have favorable prognoses with standard curative therapies, limiting the observable incremental benefit.
Several prior nationwide studies based on the National Health Insurance Research Database have examined the survival impact of CHM in lung cancer. Our study further supported a positive association between integrative Chinese and Western medicine and improved prognosis. However, several methodological and contextual distinctions differentiate the present study from prior investigations. First, many earlier NHIRD-based analyses relied primarily on administrative claims data, which may lack granular and validated staging information.17 -19 Our study integrates NHIRD claims with data from the Taiwan Cancer Registry, which captures over 98% of cancer cases in Taiwan and includes histologically confirmed diagnoses and AJCC TNM staging. This integration enhances staging accuracy and strengthens internal validity. Second, while some previous studies adjusted for confounders using regression models, not all employed rigorous 1:1 propensity score matching incorporating age, gender, comorbidity burden (CCI), and clinical stage. 20 In our study, 7351 patients were matched to ensure balanced baseline characteristics, thereby reducing selection bias and improving comparability between CHM and non-CHM cohorts. Finally, unlike several prior survival-focused analyses, 21 our study also characterizes commonly prescribed single herbs and compound formulas among stage III-IV patients. The most frequently used single herb was Hedyotis diffusa Willd (Baihuasheshecao), and the most commonly used formula was San-Zhong-Kui-Jian-Tang. This prescription-level analysis provides additional clinical insight into real-world integrative practice patterns. Few prior NHIRD studies reported detailed prescription-level frequency data. Taken together, while previous NHIRD-based studies have demonstrated an association between CHM use and improved survival in lung cancer, our study contributes additional value through registry-validated staging, rigorous propensity score matching, stage-stratified survival analysis, detailed prescription pattern evaluation, and extended follow-up within a contemporary treatment era.
CHM has been explored for its potential benefits in various types of cancer, both as a complementary therapy and as part of integrative cancer treatment approaches. Recently, Liu et al published a systemic review and demonstrated CHM contains numerous flavonoids, alkaloids, terpenoids, polyphenols, and other active compounds that are effective against lung cancer. 22 However, overall methodological quality of these publications were poor, and the level of evidence required improvement. It is necessary to carry out large-scale, standardized, and higher-quality research in the superior and weak areas of CHM treatment of lung cancer. Our study is a nationwide population-based study with a largest cohort to suggest the positive role of CHM in the treatment of lung cancer. CHM functions through various mechanisms that might influence cancer progression and patient survival. First, certain CHM are believed to enhance immune function, promoting the activity of natural killer cells and lymphocytes, which are crucial for targeting cancer cells. 23 A trial indicated that patients treated with a combination of herbs, including Astragalus membranaceus and Ganoderma lucidum, showed increased levels of CD4+ T cells and NK cell activity, correlating with better clinical outcomes. 24 These findings underscore the potential of herbal medicine to bolster the body’s immune response, which is particularly important in cancer management. Second, many CHM are rich in antioxidants, which can help counteract oxidative stress that contributes to cancer progression. 25 Moreover, some CHM exhibit cytotoxic properties against cancer cells, inhibit their growth and promote apoptosis leading to extend survival. 26 A systematic review of randomized controlled trials indicated that cancer patients receiving CHM alongside conventional treatment had improved overall survival rates compared to those who did not. 27 One notable study found that patients given a specific herbal formula, Shenqi Fuzheng Injection, showed a significant increase in median survival time. 28 This formula was synthesized from a combination of herbs traditionally used to invigorate Qi and nourish the body. Last, CHM may increase the efficacy of conventional treatments by reducing side effects, alleviating symptoms, and improving overall quality of life. 29 In a study involving patients with advanced lung cancer undergoing chemotherapy, adjunct treatment with specific Chinese herbal formulas was found to significantly improve quality of life and reduce chemotherapy-related side effects, such as nausea, fatigue, and neuropathic pain. 30 Improved quality of life can lead to better treatment adherence and potentially improve survival outcomes.
Limitations
This study has some limitations. Our study is a nationwide population based retrospective study and has several inevitable limitations. First, patients with CHM were treated with different herbal medicine. This might be the major bias in this study. Due to the nature of NHIRD data, granular information on dosage, duration, and specific herbal combinations is not consistently available. Therefore, our study could not make a conclusion that which CHM had best benefits for patients with lung cancer. Furthermore, the immortal time bias arising from the interval between lung cancer diagnosis and initiation of CHM might also be a potential limitation. Due to database limitations, CHM exposure was treated as a fixed covariate, and a time-dependent Cox model could not be fully implemented. Second, although every patient received standard therapy, the treatments were variable. Chemotherapy drug, targeted therapy, immune checkpoint inhibitors and radiotherapy course were divergent between each other. Third, the associations between annual accumulation dosage and response were not clear. It would be better to perform such a subgroup analysis to answer this question. However, due to restrictions in the period of database access and licensing limitations, we were unable to reconstruct year-by-year CHM usage data for this cohort. These limitations should be acknowledged as inherent to retrospective studies. Lastly, different durations of CHM treatment, different dosage of CHM, and differences in follow-up duration also limit the strength of the findings of our study. Nonetheless, detailed information, including dosage, duration, combination regimens and adverse events, could not be systematically assessed using the NHIRD, as laboratory data and toxicity grading are not captured in the database. Thus, propensity score matching was used to diminish selection bias. Although propensity score matching was performed, unmeasured confounders such as performance status, treatment adherence, and socioeconomic factors may still influence outcomes. Given these inherent limitations, our study was a nationwide population-based study with largest cohort to investigate the role of CHM in the treatment of lung cancer. To date, there are no prospective randomized controlled trials focusing on the impact of CHM for patients with lung cancer. In spite of a retrospective study with selection bias inherent to any retrospective studies, our study remains clinically valuable and provides clinical implication for physicians who treat patients with lung cancer.
Conclusion
The concept of integrative oncology emphasizes the combination of complementary therapies with conventional cancer treatments. The prognostic impact and benefits of Chinese herbal medicine in improving survival outcomes for lung cancer patients are gaining recognition in the medical community. Our nationwide population-based study suggested that CHM was associated with better survival benefits of standard treatment in patients with lung cancer, especially stage III-IV lung cancer. However, further rigorous clinical trials and studies are crucial for understanding their efficacy, safety, and mechanisms of action in cancer treatment. Healthcare providers should consider adopting an integrative approach, where patients can receive personalized plans that incorporate both CHM and standard oncological treatments. This model not only respects the patient’s cultural beliefs and preferences but can also provide comprehensive care addressing physical, emotional, and psychological aspects of cancer treatment.
Footnotes
Acknowledgements
This work was supported by grants from E-Da Cancer Hospital (Grant no. EDCHP112016). The authors would like to express their sincere appreciation to the Taiwan Association of Cancer Research (TACR) for providing support in project coordination and research administration throughout the study (TACR No. 24A07).
Ethical Considerations
This study was approved by the Institutional Review Board of Fu Jen Catholic University (IRB No. C110199), and was conducted in accordance with the Declaration of Helsinki.
Consent to Participate
The requirement for individual written informed consent was waived because this was a retrospective analysis of National Health Insurance Registry Database.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.*