
Abstract
Consolidated Standards of Reporting Trials (CONSORT) 2025 Statement was issued in April 2025, however, no dedicated CONSORT extension currently exists for integrative oncology. It is therefore essential to provide practical recommendations, grounded in the CONSORT 2025 Statement and in an analysis of randomized controlled trials (RCT) reporting quality against CONSORT 2010, to guide future RCTs. This study presents a literature-based analysis of RCTs published in Integrative Cancer Therapies between 2010 and 2025, describing study characteristics and overall weighted adherence to CONSORT 2010 of 72 included RCTs. The annual number of publications exhibited an overall upward trend over the past 15 years; overall weighted adherence to CONSORT 2010 across the 72 studies was 67.9%, and the mean per-manuscript adherence was 67.2%. Drawing on this analysis and the CONSORT 2025 update, several specific measures are proposed to improve the reporting quality of RCTs in integrative oncology.
Introduction
According to Cancer Statistics, 2025, 2,041,910 new cancer cases and 618,120 cancer deaths are projected to occur in the United States. The national cancer mortality rate continued to decline through 2022. 1 The near future will present new challenges associated with a growing population of cancer survivors, an aging survivor cohort, and the unknown adverse effects of novel treatments. 2 Addressing these issues requires a holistic approach, such as integrative cancer, defined as patient-centered, evidence-based cancer care that uses mind and body practices, natural products, and lifestyle modifications from different traditions alongside conventional cancer treatments.3,4
On April 14, 2025, The BMJ, JAMA, The Lancet, Nature Medicine, and PLOS Medicine simultaneously published the updated CONSORT (Consolidated Standards of Reporting Trials) 2025 statement,5-9 accompanied by an explanatory and elaboration article in BMJ. 10 The update comprises a 30-item checklist of essential reporting items and a participant flow diagram, reflects recent methodological advancements and user feedback, and aims to improve the use, understanding, and dissemination of CONSORT by providing authors with guidance to enhance the completeness and transparency of randomized trial reports. 11 Following the CONSORT 2010 Statement—the previous version—approximately 20 CONSORT extensions were developed. 12 However, the interval for developing or updating CONSORT extensions is uncertain and can be prolonged; for example, the CONSORT 2010 Extension for Chinese Herbal Medicine Formulas was published in 2017, seven years after the issue of CONSORT 2010. 13 Moreover, apart from the CONSORT Extension for Chinese Herbal Medicine Formulas, no dedicated CONSORT extension currently exists for integrative oncology.
Given the rapid development of integrative oncology trials, it is essential to offer practical recommendations grounded in the CONSORT 2025 Statement and in an analysis of the reporting quality of randomized controlled trials (RCTs) conducted between 2010 and 2025 against CONSORT 2010, to guide future RCTs.
Methods
Search Strategy
The article search was conducted in the PubMed database to obtain clinical trial reports published in Integrative Cancer Therapies, and followed by manual searching. The following inclusion filters were applied in the search: Adaptive Clinical Trial, Clinical Study, Clinical Trial, Clinical Trial, Phase I, Clinical Trial, Phase II, Clinical Trial, Phase III, Clinical Trial, Phase IV, Controlled Clinical Trial, Randomized Controlled Trial. Two authors (Yang GL and Guo ST) systematically reviewed the search results using EndNote 2025 software. Inclusion criteria were as follows: (1) the study was an interventional clinical trial involving human participants, including randomized controlled trials and phase I-IV clinical trials; (2) the full-text article was published in Integrative Cancer Therapies; and (3) the publication date was between June 1, 2010, and April 14, 2025. Exclusion criteria included the following: non-randomized studies (e.g., single-arm studies), review, meta-analysis, literature analysis, commentary, letter, retrospective studies, pilot studies, secondary analysis of completed studies, follow-up studies, protocol studies, and articles with insufficient data.
Data Extraction
For each publication, two authors (Yang GL and Guo ST) independently extracted the following information: first author’s geographic origin, category of complementary and alternative medicine (classified according to the National Center for Complementary and Integrative Health system into: alternative medical systems [e.g., acupuncture, homeopathic treatment, etc], biologically based therapies [e.g., chelation therapy, folk medicine, etc], manipulative and body-based therapies [e.g., massage, movement therapies, etc], mind-body therapies [e.g., yoga, tai chi], and energy healing therapies [Reiki, etc]),14,15 an “other” category was also included for interventions not fitting these groups), sample size, type of control group (conventional treatment, placebo, best supportive care, blank control, or other), study design (single-center or multicenter), and blinding method (open-label, single-blind, double-blind, or other).
Two authors (Yang GL and Guo ST) independently assessed the reporting quality of the included articles using the 25-item CONSORT 2010 checklist. 16 Each checklist item was scored dichotomously as “Yes” or “No,” based on whether the required information was reported. For each item, adherence was calculated as the percentage of included articles scoring “Yes.” Discrepancies between the two primary reviewers were resolved by consensus, with arbitration by a third author (Zhang HQ) when necessary.
Calculation of Adherence
Overall weighted adherence to CONSORT 2010 was calculated by aggregating item-level reporting across all included studies. Items judged as entirely not applicable (NA) were excluded from the calculation. For items with limited applicability, a normalized weight factor was applied to standardize their contribution across the full sample. For items with full applicability, the weight factor was 1. Overall weighted adherence was then calculated as the sum of weighted compliant counts divided by the sum of applicable study-item instances across all included items.
Mean per-manuscript adherence was calculated at the study level. For each manuscript, the adherence rate was defined as the number of CONSORT items adequately reported divided by the number of applicable items after excluding NA items. The mean per-manuscript adherence was then obtained by averaging the adherence rates across all included manuscripts.
Study Aim
The primary objective of the study is to evaluate overall adherence to the CONSORT 2010 Statement among randomized trials published in Integrative Cancer Therapies between 2010 and 2025, and the secondary objective is to offer practical recommendations aligned with CONSORT 2025 to guide future RCTs.
Statistical Analysis
Data were extracted from the included RCTs to capture study characteristics and adherence to each CONSORT 2010 checklist item. Categorical variables (e.g., study characteristics and checklist adherence) were summarized using frequencies and percentages. Continuous variables, including sample size, were described using medians. For each CONSORT 2010 item, the number and percentage of studies meeting the reporting requirement were calculated to quantify reporting quality. All analyses were performed using SPSS 26.0 software (Chicago, IL, USA).
Results
A total of 234 records were initially identified from Integrative Cancer Therapies. After screening titles and abstracts, with full-text review as needed, 162 records were excluded for not meeting the inclusion criteria. Reasons for exclusion were: 59 pilot studies, 26 nonrandomized trials, 23 prospective observational studies, 21 feasibility studies, and 33 studies deemed not evaluable, included 15 secondary analysis or follow-up studies, 9 protocol studies, 4 qualitative studies, 3 retrospective studies, and 2 studies classified as other (Figure 1). Flow diagram showing the selection process for this study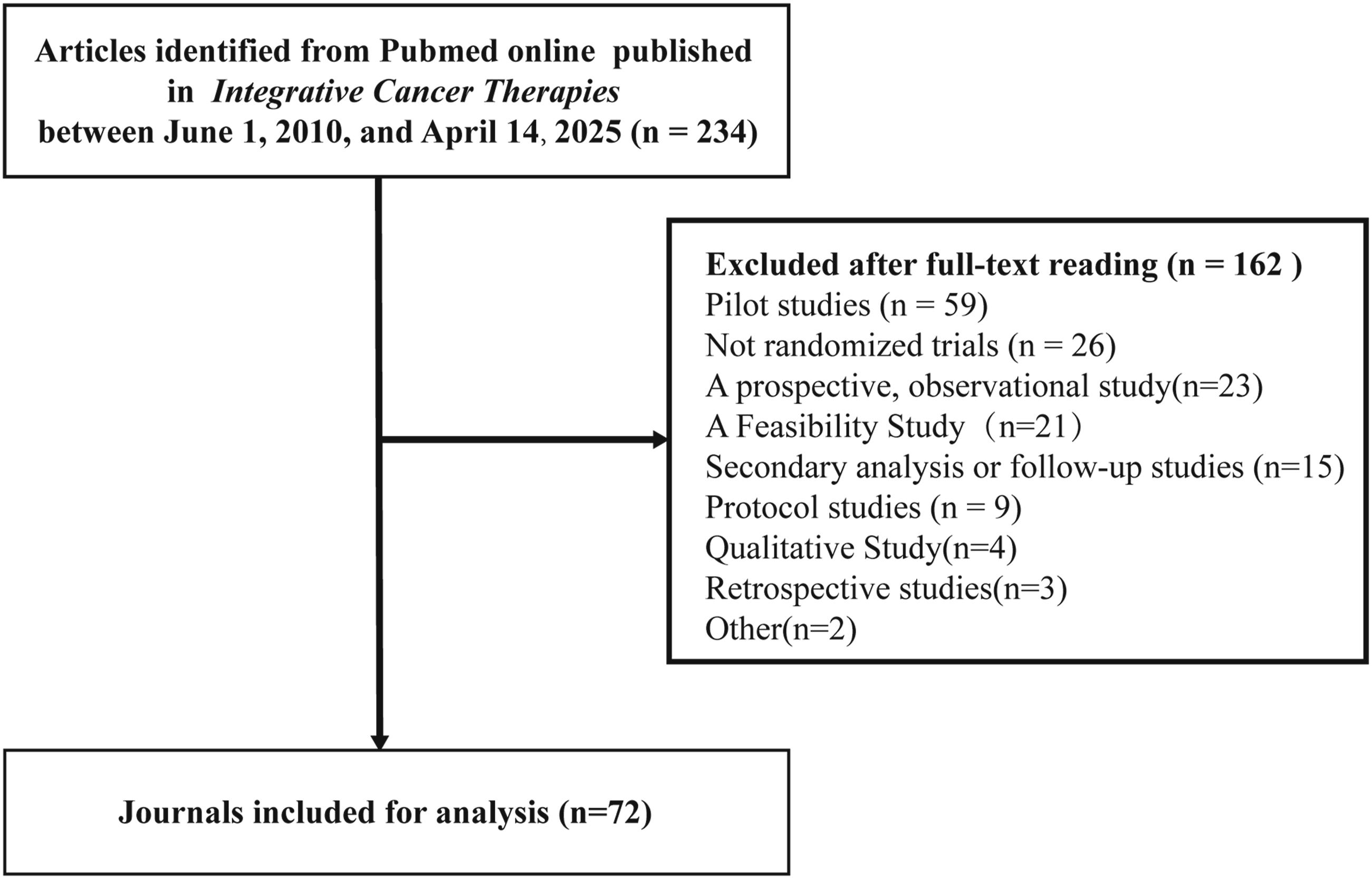
Across the 72 included articles, key study characteristics were as follows. The annual number of publications increased overall from 2010 to 2025, peaking in 2023 (Figure 2). Most studies were conducted in Asia (47/72, 65.3%). Regarding intervention category, “alternative medical systems” were most prevalent (27/72, 37.5%), followed by “biologically based therapies” (14/72, 19.4%) and “manipulative and body-based therapies” (14/72, 19.4%). The mean sample size per trial was 87.3 participants. The most common control conditions were conventional treatment (24/72, 33.3%) and placebo (21/72, 29.2%). The majority of trials were single-center (57/72, 79.2%). With respect to blinding, more than half of the studies were open-label (37/72, 51.4%), whereas 19/72 (26.4%) employed double-blind designs (Table 1). Publication year distribution of included studies Characteristics of the Included Studies (n=72) α“Other” primarily encompasses comparisons between different complementary and alternative medicine therapies. βThe “Other” category refers to triple-blind studies.

CONSORT 2010 Assessment of Included Randomized Controlled Trials (n=72)

αOmission of the personnel responsible for randomization generation, enrollment, and/or intervention assignment.
βOmission of a baseline characteristics table.
γOmission of a precision measure (e.g., 95% CI) for the effect size.
Discussion
To our knowledge, this is the first study to evaluate overall adherence to the CONSORT 2010 Statement among randomized trials published in Integrative Cancer Therapies between 2010 and 2025. Using a PubMed search, we identified 72 eligible studies. Overall weighted adherence to CONSORT 2010 was 67.9%, and the mean per-manuscript adherence was 67.2%.
Overall, adherence to CONSORT 2010 among studies published in Integrative Cancer Therapies was suboptimal, with approximately one-third of checklist items not reported on average. These findings are consistent with reports from other medical journals, which likewise document modest adherence to CONSORT and related reporting guidelines.17-20 Such modest adherence may reflect the absence of a dedicated CONSORT extension for integrative oncology and limited awareness or implementation of CONSORT guidance by authors. Underreporting was most pronounced for critical methodological details, as well as elements of the Results and Discussion sections.
The rising overall weighted adherence and the mean per-manuscript adherence suggest that reporting in integrative oncology trials has improved over the past 15 years. In addition, the annual number of publications increased over time. Compared with prior literature analyses of complementary and alternative medicine RCTs in oncology, we observed obvious improvements in sample size, reporting of sample size calculations, and use of blinding.21,22
Update of CONSORT 2025
Building on CONSORT 2010, CONSORT 2025 Statement introduces seven new checklist items, revises three items, deletes one item, and integrates several elements from key CONSORT extensions. 11 The main changes can be summarized as follows: (1) enhanced transparency regarding statistical analysis plans, funding, and conflicts of interest; (2) explicit requirements for data and material accessibility and sharing; (3) detailed descriptions of patient and public involvement across all stages of the trial; (4) clearer definitions and assessments of harms, including both systematically collected and non-systematic reports; and (5) requirements to report protocol and methodological changes and to clearly present group assignments and participant numbers to ensure transparent randomized trials. 12
With the publication of CONSORT 2025, the design and reporting of randomized trials in integrative oncology should adhere to the latest version, with particular attention to the new and revised items.
Besides, on April 28, 2025,JAMA, BMJ, Nature Medicine and PLOS Medicine simultaneously published the updated guideline for protocols of randomized trials of SPIRIT 2025 statement, with an evidence-based checklist of 34 minimum items and a diagram.23-26 As living guidelines for improving clinical trial quality, CONSORT and SPIRIT have different emphases. CONSORT requires transparent reporting of completed randomized trials regarding design, methods and results, whereas SPIRIT informs the development of ethically appropriate and scientifically rigorous trial protocols prior to study initiation.27-30 Investigators are recommended to apply the updated CONSORT and conventional SPIRIT guidelines simultaneously. 11
Adoption of CONSORT 2025 in Integrative Oncology: Perspectives and Recommendations
Undoubtedly, all CONSORT 2010 items retained in CONSORT 2025 warrant rigorous adherence, particularly those historically underreported.31,32
Among the seven newly added checklist items, Items 4, 33 5b, 34 12b, 35 and 21 36 primarily address data sharing; financial and other conflicts of interest; eligibility criteria for sites and investigators; and the definition of grouping and analysis of missing data. These requirements are not specific to integrative oncology and should therefore be straightforward for investigators and clinicians to adhere to. Item 8 emphasizes patient and public involvement in the design, conduct, and reporting of trials, which may pose challenges for investigators given global disparities in health literacy. Given that 51.4% of integrative oncology RCTs in our analysis were open-label, patient involvement may be more feasible than in blinded interventional trials. Item 15 clarifies approaches to assessing harms and other unintended effects. 37 In cancer-related randomized trials, including integrative oncology, the Common Terminology Criteria for Adverse Events (CTCAE) are widely used to grade adverse events and their severity. 38 As of January 1, 2026, CTCAE version 6.0 is scheduled to replace version 5.0. Item 24 adds requirements to report how the intervention and comparator were actually administered, as well as details of concomitant care received during the trial. 39 Because integrative oncology interventions are diverse and often combined with conventional therapies, investigators should specify interventions clearly. Reporting of concomitant care remains uncommon; investigators should incorporate plans for capturing concomitant care into trial design.
The three fully revised checklist items—Items 3, 40 10, 41 and 26 42 —Primarily address the statistical analysis plan, reporting of important trial changes, and specification of each primary and secondary outcome. None of these items are specific to integrative oncology.
Furthermore, Items 17a and 17b are consistent with those in the CONSORT 2010 statement. Given the generally low reporting rates regarding the type of randomization and details of any randomization restrictions, we encourage the involvement of design and biostatistics experts in clinical trials at the design stage.
Limitation
This study has several limitations. First, the RCTs of integrative oncology included in the analysis were drawn exclusively only from Integrative Cancer Therapies, which may limit generalizability to the broader literature. Second, although some checklist items—particularly in the Methods and Randomization domains—are more consequential than others, our analysis weighted all CONSORT items equally. All biostatistical analyses were descriptive only, no statistical tests, subgroup analyses, or regression modeling were performed to explore predictors of improved reporting. Third, our recommendations regarding the seven newly added and three revised CONSORT 2025 items only reflect expert opinion, which should be supported by empirical evidence or official guidance.
Conclusion
Drawing on our analysis of randomized trials published in Integrative Cancer Therapies against the CONSORT 2010 Statement, and informed by the CONSORT 2025 update, we propose several specific measures to improve the reporting quality of RCTs of integrative oncology. We also encourage the CONSORT Group to develop a dedicated extension to support the design, conduct, and reporting of randomized trials in integrative oncology.
Footnotes
Ethical Considerations
This study does not involve any human participants, human tissue samples, or animal experiments. Therefore, no ethical approval was required for this study.
Author Contributions
YGL, GST, and ZHQ contributed to the study’s conception, design, conduct, and interpretation of the data. WF and HX prepared the tables and data for analysis. YGL and GST performed the statistical analysis. YGL and GST drafted the initial version of the manuscript, while HX and ZHQ provided feedback on all revisions. All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Generative AI Usage Statement
The authors declare that no generative AI or AI-assisted technologies were used in the preparation, drafting, editing, or visualization of this manuscript.