
Abstract
Impacts of traumatic stress on psychological and physical outcomes were investigated in a moderated mediation model. Two groups of firefighters participated. The trauma group participated in the World Trade Center search and rescue operations in New York City, and the control group, from the same organization, worked at their regular jobs. A mediation analysis indicated that both psychological and physical indicators showed significantly higher negative reactions in the trauma group, above and beyond what might be expected from reported levels of stress exposure. A moderated mediation analysis indicated that personal resources that provided a buffer to damaging outcomes for the control group might not function effectively or may even make individuals more vulnerable under traumatic stress conditions. Implications for protective actions are discussed.
High-risk occupations such as combat, firefighting, or trauma care in hospital settings may expose individuals to traumatic conditions that affect their psychological and physical well-being. Increasingly, those studying the impact of working in high-risk occupations have attended to the concept of traumatic stress as an occupational hazard (Jermier, Gaines, & McIntosh, 1989; McFarlane & Bryant, 2007). The vast majority of firefighters, paramedics, and other emergency personnel experience both acute and chronic symptoms during their careers including disturbed sleep, demoralization, anger, physiological reactivity, alienation, isolation, guilt, feelings of insanity (Beaton, Murphy, Pike, & Jarret, 1995; McFarlane, 1988; Murphy & Beaton, 1991). In addition, estimates of work stress-related costs to businesses and organizations amount to nearly 10% of annual earnings. Despite the fact that physical danger in the workplace has been a growing concern for decades, research rarely addresses the physical and psychological impact of traumatic events (Jermier et al., 1989; see Bacharach & Bamberger, 2007 for an exception).
The general research interest in traumatic stress (Dougall, Hyman, Hayward, McFeeley, & Baum, 2001; Green, 1996) also contains more specifically focused research on the traumatic reactions of firefighters (Bacharach & Bamberger, 2007; Williams & Baker, 2001). The current study attempts to contribute to the literature in three ways: First, it addresses the call for research on traumatic stress during catastrophic events. Intense, acute, traumatic stressors such as terrorist attacks or natural disasters are shorter in duration yet can be psychologically devastating and may have long-term consequences (Tedeschi, Park, & Calhoun, 1998). From a theoretical point of view, the characteristics of the stressful situation should affect the individual’s reaction to it (Gottlieb, 1997). Further clarification of this relationship is one aim of this study. Second, the current study examines the boundary conditions of the relationship between perceived stress and psychological and physical outcomes. Examining individual moderators such as hope and other personality variables enhances theory by identifying the conditions under which perceived stress is related to outcomes (Costa & McCrae, 1994; Snyder, Cheavens, & Sympson, 1997). Assessing such variables under traumatic conditions can help to understand if individual differences act in a similar/different fashion compared with day-to-day, normal stress situations. Third, this study addresses the call for research in traumatic stress that involves not only psychological but also objective physical outcomes (Smith, Manning, & Petruzzello, 2001).
This study examines psychological and physical consequences in firefighters exposed to traumatic search and rescue activities after the World Trade Center attack. A moderated mediation model (Baron & Kenny, 1986) is proposed in which type of stress (traumatic vs. regular job stress) mediates between perceived stress (reported stressors) and physical and psychological symptoms (strain). Mediation does not imply causality between predictor and mediator variables, but rather describes a particular relationship in which the mediator accounts for variance between the predictor and the outcome variables. Beyond mediation, hope and other personality variables may moderate the mediated relationship, as described by Wofford, Goodwin, and Daly (1999).
We begin with a review of the literature on firefighters’ reactions to stress at both physiological and psychological level. Next, we turn to a discussion on personality factors such as hope and Big Five personality factors as related to stress, and we propose specific hypotheses.
Traumatic Stress and Physiological and Psychological Stressors Among Firefighters
Traumatic stress is characterized by traumatic events or significant catastrophes that have a sudden onset, are temporary in nature and tend to challenge people’s sense of meaning, their sense of mastery, and their self esteem (Carayon, 1995; Updegraff & Taylor, 2000). Traumatic events involve “actual or threatened death or serious injury, or threat to physical integrity of self and others” (American Psychiatric Association, 1994, p. 424). These events are extraordinary not because they occur rarely but rather because they may overwhelm the ordinary human adaptations to life and produce profound and lasting changes in physiological arousal, emotion, cognition, and memory (Herman, 1992). Studies have shown that individuals who have been exposed to traumatic stressors have reported adverse physical health outcomes, including poor self-reported health status, a greater number of self-reported medical problems, and increased morbidity and mortality (Bacharach & Bamberger, 2007; Schnurr & Green, 2004).
From a theoretical viewpoint, a distinction in the type of stress has been seen as important in understanding the stressor–personal well-being connection (Gottlieb, 1997). In this conception, it is not merely the objective stressors but the characteristics of the stress process (chronic, acute, and traumatic) that should be accounted for. Indeed, some scholars have advanced the theory that traumatic stress may be different in kind, not only degree, from other stress types (Gottlieb, 1997). Traumatic stress often includes actual physical and psychological harm and loss, above and beyond the mere threat of such harm. Therefore, traumatic stress will be incorporated into the model as a mediator, and we posit the following:
Hypothesis 1: Exposure to traumatic conditions will mediate the relationship between perceived stress and both psychological and physical outcomes.
Traumatic stress has long been recognized as an occupational hazard in public safety professions (Paton, Violanti, Dunning, & Smith, 2004). Emergency workers may face mass causalities (McFarlane, 1988); airplane crashes (Brooks & McKinlay, 1992); or terrorist attacks (Bacharach & Bamberger, 2007; Galea et al., 2002; Pfefferbaum et al., 2002). Traumatic events can generate stress for several reasons. First, given the nature of mass-causality incidents, handling dead bodies or body parts is highly traumatic in itself (McCarrol, Fullerton, Ursano, & Hermsen, 1996). Second, an element of exposure to danger of accidents with the risk of personal injury is increasingly present in such catastrophic events. Third, time pressure while working in these traumatic situations is very high. Fourth, the aftermath of traumatic events is very uncertain; firefighters must react immediately and move rapidly especially as the role of firefighting has increasingly changed from fire suppression to emergency medical response (Gist & Lubin, 1999). Lastly, when people are unprepared, not only do they suffer from the losses associated with the event but also their worldview may be shattered and forever altered (North & Pfefferbaum, 2002). These symptoms are experienced not only from those who are victims but also by those individuals who witness horrifying incidents that leave them feeling helpless.
Previous research on exposure to traumatic stress indicates that there are many variables that may effect psychological and physical adjustment to intense, acute stress situations (McCammon, 1996; Schaubroeck, Ganster, & Fox, 1992). Using some measures of physiological responses, but mainly relying on questionnaires and self-reported surveys, several studies have been conducted concerning the risk to the psychological and physical well-being of firefighters caused by exposure to traumatic events (McCall & Salama, 1999). Regehr and Bober (2005) studied cardiac responses such as elevated heart rate in emergency service workers following a stressful event on the job. Williams and Baker (2001) assessed the relationship between social problem-solving appraisals, work stress, and psychological distress suggesting that fire service personnel reporting higher levels of stress and psychological distress have less effective problem-solving appraisals; in particular, they report more helplessness and less problem-solving control. The previous studies emphasize the importance of examining both psychological and physical reactions to stress in firefighters (Bacharach & Bamberger, 2007).
The current study compares the reactions of firefighters who participated in the “ground zero” World Trade Center search and rescue activities with firefighters who did not, following September 11, 2001. One component of the cognitive appraisal theory would suggest that the more severe exposure to stress one encounters, the higher probability of negative symptoms he or she will develop. Individuals other than the primary victims may also be affected psychologically and physically after major disasters such as those of September 11. This is not to say that some of the stay-at-home firefighters may not have encountered traumatic stressors, but rather that the intensity and duration of the ground zero stressors reached a different level entirely for virtually all of the ground zero volunteers. Consequently, we posit the following:
Hypothesis 2: Exposure to traumatic stress conditions will result in significantly higher psychological and physical symptoms than in regular job stress conditions.
Moderating Role of Individual Differences
Cognitive appraisal theory suggests that characteristics of the traumatic stressors, the rescue operation, and the rescuer himself or herself may all affect the degree of the stress experienced (Bowman, 1997; Raphael & Meldrum, 1991). Several personality variables have been related to the perception of stress. Hope may be one of these. As recognized in positive psychology, hope is defined as “a positive motivational state that is based on an interactively derived sense of successful (1) agency (goal-directed energy) and (2) pathways (planning to meet goals)” (Snyder, Irving, & Anderson, 1991, p. 287; also see Snyder, Rand, & Sigmon, 2002). Snyder and his associates indicate “extensive convergent and discriminant validational support” for this concept (Snyder et al., 2002). Hope as conceptualized by Snyder et al. (1991) is similar to optimism in that there is a generalized expectancy regarding positive outcomes that is a dispositional component of personality. Furthermore, Snyder et al. (2002) review the discriminations between hope and related constructs such as optimism, self-efficacy, self-esteem, and problem solving. They conclude that, although there is overlap between the constructs, hope taps psychologically unique features not addressed by the other constructs. Hope specifically includes a pathway to the desired outcome in addition to the belief that a positive outcome will occur. A sense of hopelessness is expected to correlate with maladjustment to traumatic stressors. Individuals demonstrating higher levels of hope are expected to adapt more effectively to trauma (Tennen & Affleck, 1998).
The theoretical approach to personality embodied in the Big Five conceptualization (Costa & McCrae, 1994) posits five orthogonal factors that account for the range of human personality characteristics. The Big Five factors of neuroticism and conscientiousness have accounted for variance in outcomes following traumatic events (Grant & Langan-Fox, 2006; McFarlane, 1988; Soane & Chmiel, 2005). Neuroticism describes the tendency to attend to negative affect. Individuals scoring high on neuroticism are characterized by worry, anxiety, depression, inadequacy, and insecurity. Neuroticism has been a consistent predictor of negative posttraumatic outcome and is strongly associated with passive and ineffective forms of coping (Costa & McCrae, 1994). Therefore, those individuals displaying high levels of neuroticism have been found to be more susceptible to the negative effects of traumatic events (Creamer, Burgess, & Pattison, 1990; Chung, Easthope, Chung, & Clark-Carter, 2000; McFarlane, 1989).
Conscientiousness also has been found to account for variance in scores when investigating positive or negative outcomes following a traumatic event (Moran & Shakespeare-Finch, 2003). The conscientious individual is reliable, organized, and persistent in pursuit of goals, as opposed to being careless, unreliable, and hedonic. Conscientiousness, which has emerged as the construct most consistently related to performance across jobs (Judge, Higgins, Thoresen, & Barrick, 1999; Salgado, 1997), is very important trait for the emergency workers who participate in high-demand and low-control situations. Conscientiousness has been demonstrated to relate significantly to positive changes in the wake of a traumatic event (Tedeschi & Calhoun, 1996).
The cognitive appraisal model of stress (Lazarus, 1999) indicates that it is not the stressors alone, but stressors in combination with personal characteristics that may affect physical and psychological well-being. Thus, we predict that personal characteristics will moderate the joint stress perception-stress type relationship.
Hypothesis 3: Hope, neuroticism, and conscientiousness will moderate the relationship between exposure to traumatic stress and psychological and physical outcomes; that is, hope and conscientiousness will relate to lower symptoms given the level of stress, whereas neuroticism will relate to higher symptoms given the level of stress.
Method
Participants
Participants were firefighters from a major Western city (n = 102). One group of 50 firefighters participated in the search and rescue operation at the World Trade Center in New York City in the aftermath of the Twin Tower destruction in September 2001 (trauma group). They arrived in New York City the same day. They spent approximately 2 weeks working in that venue. The second group of 52 from the same organization stayed at home during the World Trade Center search and rescue activities and worked at their regular jobs such as attending emergency incidents: fires; road accidents; floods; bomb incidents; spillages of dangerous substances; and rail and air crashes, providing emergency care for sick and injured persons, routine maintenance of fire apparatus, as well as drilling and training in new fire fighting techniques and practices (control). All participants were male. The trauma group was significantly older (43.4 vs. 36.6) and had been in the firefighting profession longer (19.2 vs. 14.1), but showed no differences with the control group in education level, average hours of week per week worked, or thyroid problems.
Measures
Level of perceived stress
Perceived Rescue Stress was constructed by evaluating and reviewing firefighters’ job analyses resulting on a 6-item scale measuring the frequency of search and rescue activities. Participants were asked to rate the previous 2 weeks with regard to days and hours per day involved in rescue activities, percentage of time saving lives and treating injuries, and intensity of damage to property and injury to persons. Frequency was elicited using a 9-point Likert-type scale; intensity was elicited via a 7-point scale. The total was the sum of the adjusted scale values. Alpha equaled .92.
Type of stress
Type of stress was a categorical variable. The trauma category indicated that the individual firefighter had participated in the World Trade Center operation. The control category indicated that the individual firefighter had remained in their regular job. Follow-up focus groups with firefighters from the trauma group (40% of participants) provided verification of the traumatic nature of the stressors they faced. Firefighters reported first that the scale of the rescue site was overwhelming and the largest with which they ever have been involved. Their acquired knowledge and experience still did not fully prepare the firefighters for an event of such massive collapse and devastation. One firefighter described the scene:
It was a 16 acre site 80 feet deep full of all kinds of debris and we were on a mission to rescue people. It was a total scene of chaos. I still remember the particular smell on the site meanwhile we were digging.
Another firefighter recalls, “The situation was overwhelming and we were not prepared to intervene in the same organized manner that we did normally at home.” This information suggests that the trauma group had difficulty performing their job in a systematic way. Such comments parallel the characteristics of traumatic stress described earlier in the literature review (Gist & Lubin, 1999).
Psychological symptoms
The level of psychological symptoms was measured using the Brief Symptom Checklist (BSI; Derogatis & Melisaratos, 1983). This 53-item measure has nine symptom cluster scales and a summary Global Severity Index (GSI). The GSI, a combination of number of symptoms checked and their perceived severity, can be seen as an indicator of overall adjustment. The GSI was used as the dependent variable for psychological symptoms. Alphas for the nine cluster scales for the current sample ranged from .80 to .90
Physical symptoms
Physical adjustment was measured by an index of a number of objective methods: reported blood pressure, diastolic and systolic levels, as well as total cholesterol levels. Although these measures were not taken directly by the investigators, the units in which participants worked monitored and provided these variables as a part of their routine job duties. In addition, upper respiratory illness symptoms were elicited using a 12-item measure of recent, and chronic symptoms of upper respiratory infections adapted from a variety of existing inventories (α = .83; e.g., Schaubroeck, Jones, & Xie, 2001; Ware, Johnston, Davies-Avery, & Brook, 1979).
Hope
Three components of hope were measured using scales developed by Snyder and his colleagues (Lopez, Ciarlelli, Coffman, Stone, & Wyatt, 2000; Snyder, Cheavens, & Sympson, 1997). At the dispositional level, two components of overall hope were measured: hope agency, the degree to which the individual felt that they might be able to act to achieve a positive outcome and hope path, the degree to which an individual could see a way or path toward a positive outcome. All hope items were rated using an 8-point Likert-type scale ranging from 1 = definitely false to 8 = definitely true. Alphas for the current sample were hope agency = .73 and hope path = .66. In addition, hope work (eight items) was a domain specific scale measuring hope in the work setting. Alpha for the current sample was .77.
Personality dimensions
Personality was measured using two scales of a short version of the Big Five personality factor approach (Fossum, Weyant, Etter, & Feldman-Barrett, 1998). For this scale, each subscale had 7 items. The scales and key defining traits used in this research include: neuroticism: anxious, hostile, self-conscious; and conscientiousness: diligent, disciplined, well-organized, and dependable. Alphas for this sample are .76 and .85, respectively.
Procedures
Within the week following the return of the trauma group, questionnaires containing measures of psychological adjustment, hope, personality, and self-reported physiological measurements were distributed to both trauma and control groups. During a debriefing session by the captain of the major unit of search and rescue workers who had returned from New York City, questionnaires were distributed in stamped, return envelopes. The same questionnaires were distributed in stamped, return envelopes to the control search and rescue workers during a companywide meeting that took place on the same day. Altogether, 130 questionnaires were distributed, and 106 questionnaires were returned with 102 completely filled questionnaires within 4 weeks of the trauma group’s return from New York, representing 78% response rate. The questionnaires were mailed directly back to the researchers from each respondent over a period of 1 month following the rescue mission.
Results and Discussion
The trauma group (M = 48.54) reported significantly more perceived Rescue Stress than did the control group, M = 15.86, F(1, 100) = 175.14, p < .001. In comparison with the control group, trauma group firefighters worked more days involving search and rescue activities with longer hours per day and a greater probability of saving lives and treating injuries. Likewise, they reported more extreme intensity of damage to property and injury to persons as well as a greater probability of injury to themselves and their colleagues. Although the rescue stress measure may not tap all of the stressors to which the trauma firefighters may have been exposed, it does indicate that exposure to the concentrated search and rescue activities following the September 11th attacks at the World Trade Center created a substantially more intense set of stressors than did the usual events for firefighters in their regular jobs.
Hypothesis 1: Exposure to Trauma as a Mediator
Above and beyond the perceived level of stress, exposure to traumatic conditions mediated the relationship of perceived stress to both psychological and physical symptoms. Demonstrating mediation is a three step process (Baron & Kenny, 1986). First, the predictor and mediator variables must show significant relationship. In this case level, perceived stress (Rescue Stress) was significantly related to type of stress (trauma or control group membership), (R2 = .77, p < .001; see Table 1 for all first-order correlations). Second, the predictor and the dependent variables must show significant relationship; the level of perceived stress (Rescue Stress) significantly predicted the psychological and physical outcome variables at p < .001. Finally, when the mediator variable is added to the regression of the predictor on the dependent variable, the regression must be statistically significant, and the contribution of the predictor variable must decrease because the mediator variable accounts for some or all of the variance of the predictor variable. To control for possible confounding from demographic variables, age, length in profession, and education level were held constant in this analysis.
Means, Standard Deviations and First-Order Correlations of All Research Variables

p < .05. **p < .01. ***p < .001.
For psychological measures (see Table 2) the mediation was virtually total; the relationship of perceived stress to psychological measures was almost completely accounted for by exposure to traumatic stress. For physical measures the mediation was partial; the relation of perceived stress to physical measures was only partly accounted for by exposure to traumatic stress. Above and beyond the perceived stress level of the situation, the type of stress was a significant mediator. The type of stress extended the explanation of contributors to the outcomes.
Mediation of Relationship of Perceived Stress and Outcomes by Type of Stress With Demographics Controlled
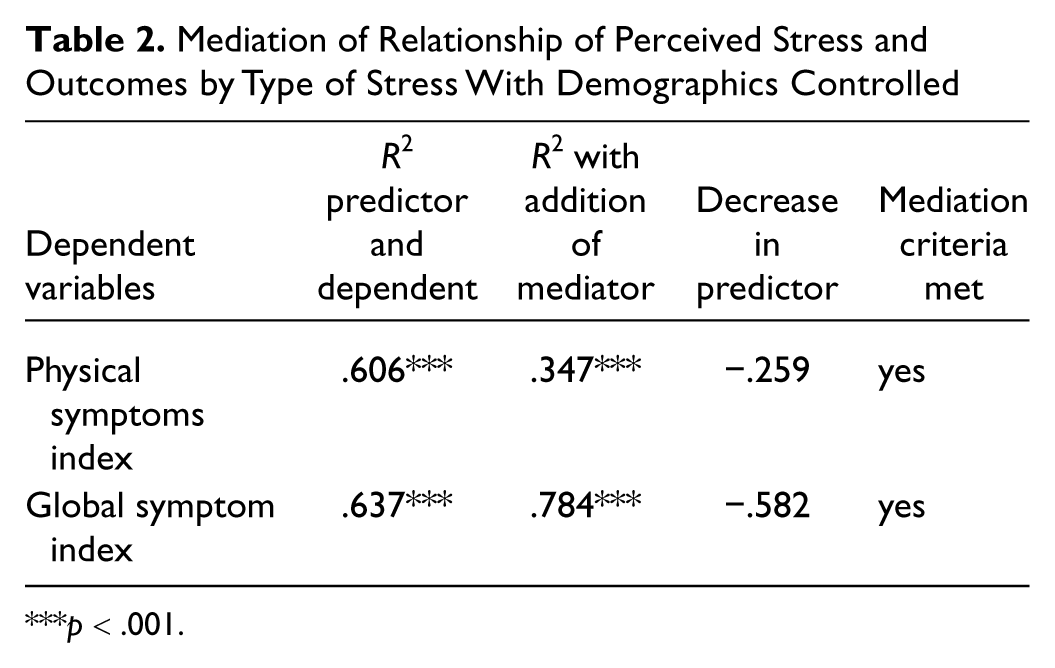
p < .001.
Hypothesis 2: Psychological and Physical Adjustment
To control for possible confounding of self-selection into the two experimental groups, a multiple analysis of covariance was completed to assess differences between the groups on psychological and physical symptoms controlling for demographic and personality variables. In this analysis, the groups were significantly different on both psychological and physical symptom indexes (see Table 3).
Means and Standard Deviations of the Trauma and Control Groups for Psychological and Physical Measures of Adjustment With Fs From Covariance Analysis
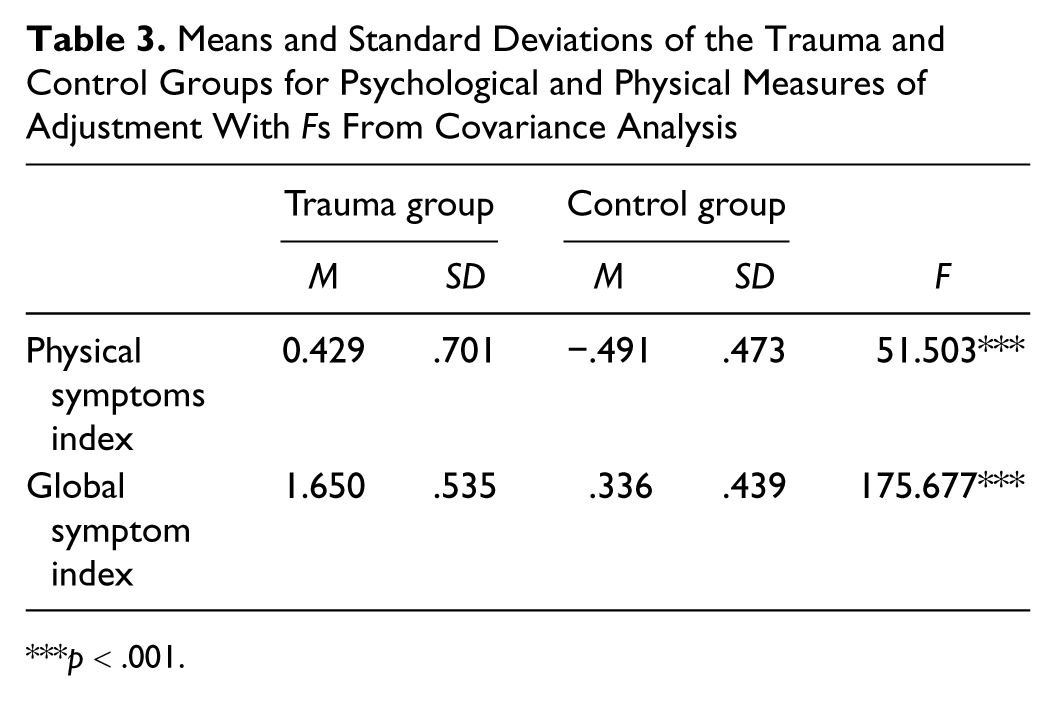
p < .001.
Hypothesis 3: Moderation of Psychological and Physical Adjustment
An analysis of covariance between groups on individual difference variables controlling for demographics indicated no significant differences between the trauma and control groups on hope or personality variables. In addition, simple addition of individual difference variables enhanced the multiple regressions between type of stress and psychological and physical outcomes in only 38% of analyses. A further examination of the contributions hope and personality variables to the relationships between perceived stress, type of stress, and outcome variables was conducted using moderation analysis as described in Baron and Kenny (1986). Using a moderated mediation model, the level of perceived stress was first controlled, then moderation analysis was done between the categorical variable of type of stress (traumatic or control) and outcome variables with hope and personality variables as the moderators. Moderation is demonstrated by the significance of the cross-product term (statistical interaction) between the moderator variable and the predictor variable. In other words, the relationship between the mediation of type of stress and psychological and physical outcomes is predicted to vary based on the level of hope and personality moderator variables of individual firefighters. The trauma and control groups are predicted to react differently depending on the impact of hope and personality variables.
For all mediation analyses, age, length in profession, and education were controlled. For psychological symptoms, all personality variables moderated the relationship between type of stress and outcome with level of perceived stress controlled. The moderator of hope agency (interaction β = .298, p < .001) functioned as expected in the control stress situation. In the control context psychological symptoms decreased as hope agency increased. This inverse relationship between hope and maladjustment is consistent with hope theory, and has been reported frequently in the literature (Snyder et al., 2002). Paradoxically, however, in the trauma stress situation, psychological symptoms increased slightly as hope agency increased. Although individuals with higher hope actually reported more psychological symptoms than those with lower hope in the trauma situation, the slope of the trauma regression line was not significantly different from zero, but the slope of the control regression line was (p < .001; Aiken & West, 1991). Thus, it seems that hope agency did not provide the buffer against stressors in the trauma situation that it did in the control situation. This general pattern was repeated for hope work (interaction β = .222, p < .01) and conscientiousness (interaction β = .300, p < .001). The pattern was reversed for neuroticism with individuals in the control stress situation displaying a positive relationship between neuroticism and GSI (interaction β = –.285, p < .01). For hope path, individuals in the trauma condition actually increased their reports of psychological symptoms significantly (interaction β = .223, p < .01), whereas individuals in the control condition decreased, though not significantly. In general, patterns of moderation of personality variables on the relationship of type of stress and psychological symptoms indicated that personality variables exert different effects depending on the type of stress to which the individual was exposed.
For physical symptoms, a smaller number of personality variables playing a moderating role: conscientiousness, neuroticism (marginal), and hope work. Physical symptoms decreased significantly with increased conscientiousness in the control stress situation (interaction β = .234, p < .05), but reports of physical symptoms increased with higher conscientiousness (although not significantly) in the trauma situation. For neuroticism, the pattern for physical symptoms repeated that shown for psychological symptoms with individuals in the control stress displaying a positive relationship between neuroticism and physical symptoms (interaction β = −225, p < .08). For hope work, individuals in the trauma condition actually increased their reports of physical symptoms significantly as hope work increased (interaction β = .252, p < .02), whereas individuals in the control condition decreased, though not significantly. In general, patterns of moderation of personality variables on the relationship of type of stress and physical symptoms also indicate that personality variables exert different effects depending on the type of stress to which the individual is exposed.
In summary, the traumatic stress situation seemed to block or even reverse the efficacy of various personality variables in helping firefighters in the traumatic situation deal with stressors. It may be that the extreme range of environmental stressors overwhelmed personal resources that would protect individuals from psychological and physical reactions under conditions of more modest stress. Likewise, specific characteristics of the traumatic condition may degrade specific personal resources.
Conclusions
The results taken as a whole suggest that exposure to higher levels of stress was related to both higher levels of perceived stress and higher levels of both psychological and physical maladjustment. In addition, exposure to the specific type of stress, traumatic stress, mediated the relationship of perceived stress to both psychological and physical symptoms. It was not level of exposure alone that accounted for the outcomes. All personality variables moderated the relationship between type of stress and psychological symptoms. There was an inverse relationship between hope and maladjustment in the control context. Paradoxically, however, in the trauma stress situation, psychological symptoms increased slightly as hope agency and hope work increased.
Because perceived level of stress and type of stress both predicted psychological and physical outcomes, it might be justifiable to use only one or the other of these variables in a research study. However, mediation analysis indicates that it may be more useful to use both variables, as their intercorrelation was not perfect, and the addition of type of stress accounted for qualitatively different aspects of the stress situation. As Gottlieb (1997) points out in his extension of stress theory, different types of stress (e.g., chronic, acute, and traumatic) may influence appraisal and coping strategies of individuals in different ways.
Building on the notion that individuals may respond differently to stressful situations of different types, the moderated mediation analysis indicated that personal resources that provide a buffer to damaging outcomes under one type of stress might not function effectively or may even make the individual more vulnerable under other circumstances. Moderation was significant in 8 of the 10 analyses done in this research. Three general patterns emerged. First, as with hope agency, a personal resource associated with lower levels of symptoms in the control setting was ineffective in the trauma setting. Second, as with hope path, higher levels of the moderator were related to higher levels of symptoms in the trauma setting. Third, as with neuroticism, a characteristic related to higher maladjustment in the control setting was not so related in the trauma setting. The relationships between moderators and outcomes were different under different types of stress.
One interpretation concerning the ineffectiveness of ordinarily protective personal resources under conditions of traumatic stress comes from the notion of shattered assumptions (Janoff-Bulman & Berg, 1998). Beyond the harm and loss inherent in a traumatic stress situation, there is also a harsh confrontation between the reality the individual faces and the protective illusion that they possess the personal resources to cope with just about anything. As one firefighter explained, “As we were debriefed on the plane to New York, we were shocked and troubled by the feeling that this event took away the innocence and our society’s internal safety.” Disillusionment over shattered assumptions may add to the overall stress experienced. Individuals with higher levels of hope and conscientiousness may be more vulnerable to such disillusionment given their stronger reliance on such resources.
The findings from our study have applications within work environments with critical events, and other “first-responder” professions such as paramedics, military, and police. One potential limitation of this study concerns the potential generalizability of the findings. Similar research examining such occupations as police officers, and military personnel is needed.
Implications for buffering the effects of traumatic stress and ameliorating the symptoms fall into two categories. First, prior knowledge of the possible outcomes of exposure to traumatic stress may normalize some of the more troubling features, and may provide a framework within which the intensity of response can be seen as temporary and a possible avenue to future growth (Janoff-Bulman & Berg, 1998). Second, immediate and long-term support should be available, even mandatory, as some workers may withdraw from constructive contact. One-time debriefing may not be enough depending on the intensity of the traumatic stress, and the personal resources the individual worker can mobilize. Emphasis can be focused on constructing a world view and set of assumptions that include not only the traumatic stress experience but also a reformulation of the limitations of personal resources and an appreciation of the worker’s life and personal history independent of the traumatic stress (Janoff-Bulman & Berg, 1998; Tedeschi & Calhoun, 2004).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.