
Abstract
Spiritual changes, or “soul wounds,” have long been described as expectable consequences of combat, useful in understanding the profound changes in many surviving warriors. However, moral injury as a research construct has only recently been introduced into the combat trauma literature (Drescher et al., 2011), and it is in the early stages of construct validation. To extend validation efforts, the current study examined National Vietnam Veterans’ Readjustment Study (NVVRS) veterans’ narrative responses to questions about the lingering effects of their combat participation for themes consistent with moral injury as reported by combat trauma experts in the Drescher et al., (2011) study. Findings confirmed key experiences involving civilian deaths and betrayal as themes among NVVRS participants’ responses about their troublesome combat experiences.
Keywords
Trauma research has long focused on military veterans, but has generally emphasized the physical and psychological toll of war. However, war experiences are broader than combat and include the various ethical and moral challenges faced during deployment (Drescher et al., 2011; Litz et al., 2009). Such experiences can impact veterans’ spiritual and moral values and identity.
Although traditional treatment has focused on the bio-psycho-social model of mental and physical illness, research in clinical practice has suggested that there is benefit to including the spiritual dimension in the treatment of end-of-life issues (Sulmasy, 2002), cancer (Ben-Arye, Bar-Sela, Frenkel, Kuten & Hermoni, 2006), and substance use (Leukefeld & Leukefeld, 1999). In fact, these studies showed that the patients were interested in the incorporation of spiritual struggles into their treatment, even when providers were reluctant to focus on those spiritual needs. In an effort to capture the complex psychological, social, and spiritual effects of ethical and moral challenges, the term moral injury (MI) has been coined (Drescher et al., 2011; Litz et al., 2009). An MI can occur when an individual experiences internal conflict stemming from involvement in acts that violate deeply held moral and ethical standards (Drescher et al., 2011). In a recent study of MI, trauma experts were surveyed about the scientific usefulness of the concept. These experts agreed that the posttraumatic stress disorder (PTSD) construct does not capture the full impact of war-related events, and that the concept of MI is helpful in explaining a broader range of combat reactions (Drescher et al., 2011). These experts also suggested that MI would most likely occur following events that involved betrayal, inappropriate or disproportionate violence, incidents involving civilians, and within-ranks violence (Drescher et al.). Furthermore, these experts suggested that signs and symptoms of MI would likely include social problems, loss of trust or a sense of betrayal, spiritual/existential issues, psychological symptoms, and self-deprecation (Drescher et al.).
The potential for MI may be increased in nontraditional, guerilla warfare where combatants have difficulty separating civilians from enemies, such as in the Vietnam war and current operations in Iraq and Afghanistan (Litz et al., 2009). Additionally, engaging in disproportionate violence may increase the risk of exposure to an MI, and is more likely to occur when combatants deviate from rules of engagement due to life threatening circumstances, loss, or orders from superior officers (Drescher et al., 2011). Finally, combatants may be at increased risk of MI when they are deployed for longer periods of time, which is correlated with a reduction in ethical behavior (MHAT-V, 2006).
Although the MI concept is currently largely theoretical, literature on the exposure to and perpetration of disproportionate violence may be applicable because these acts may be morally injurious (Litz et al., 2009). For example, committing atrocities and even sanctioned war zone killings result in symptoms beyond the criteria for PTSD (c.f. Maguen et al., 2009), and may include changes in spiritual and ethical attitudes and behaviors (Drescher et al., 2011).
Because MI is a new concept, existing research on the topic is either theoretical (e.g., Litz et al., 2009) or qualitative (e.g., Drescher et al., 2011). Thus, the goal of the present study was to extend research on MI, by applying qualitative methods to confirm and extend the MI concept using free narrative responses from the National Vietnam Veterans’ Readjustment Study (NVVRS; Kulka et al., 1990). The NVVRS was a congressionally mandated epidemiological study conducted between 1986 and 1988 using a randomly selected, stratified, nationally representative sample of U.S. Vietnam Era veterans (Kulka et al., 1990). The total sample consisted of 3,016 male and female veterans who served in the U.S. military between August 5, 1964, and May 7, 1975, including 1,200 men who served within the Vietnam Theater (i.e., Vietnam and the surrounding area; “Theater” veterans) and 412 men who served outside the Vietnam Theater (“Era” veterans). The main findings of the NVVRS included a lifetime PTSD rate for male Theater veterans of approximately 31%, whereas the current (at the time of the interview) PTSD rate was 15% (Kulka et al., 1990). Since the initial publication of these results, the NVVRS data archive has been used by other trauma researchers to examine other combat-related research questions. For example, the dataset has been examined for additional correlates of PTSD, including exposure to atrocities, combat exposure, perceived threat, perception of a harsh environment, minority status and having killed during the war (Beckham, Feldman, & Kirby, 1998; Dohrenwend, Turner, Turse, Lewis-Fernandez, & Yager, 2008; King, King, Gudanowski & Vreven, 1995; Kulka et al., 1990; Laufer, Gallops, & Frey-Wouters, 1984; Lewis-Fernandez et al., 2008; MacNair, 2002; Maguen et al., 2009). Additionally, studies have examined disability and psychosocial adaptation (Martz, Bodner, & Livneh, 2009); loss of meaning and combat exposure (Fontana & Rosenheck, 2005), and spousal perceptions of veterans with PTSD (Renshaw, Rodebaugh, & Rodrigues, 2010).
Although there has been extensive research on the NVVRS, to date the focus has been on quantifying traumatic experiences, or the presence or absence of specific psychiatric disorders based on quantitative data (Martz et al., 2008). The current study qualitatively analyzes traumatic experiences and psychosocial outcomes based on open-ended questions from the NVVRS database, with particular attention paid to events and symptoms associated with MI. More specifically, the study aimed to address the following research questions:
What themes of MI are present in the descriptions of traumatic events from male Vietnam Theater and Vietnam Era veteran participants in the NVVRS? How do these themes relate to themes of MI described by experts in the trauma field (Drescher et al., 2011)?
What types of MI signs and symptoms are present in the descriptions of the long-term impact of the Vietnam war on male Vietnam Theater veterans? How do these themes relate to the signs and symptoms identified by the experts from the Drescher et al. (2011) study?
Is there a relationship between the signs and symptoms identified as being consistent with MI and potential MI events reported by male Vietnam Theater veterans?
Method
Participants
This study utilized archival data from veterans who participated in the NVVRS, which comprehensively assessed for premilitary, military, and postmilitary characteristics and functioning. This study received an exemption from Pepperdine University Gradue and Professional schools IRB. The full sample (N = 3,016) was a nationally representative, stratified random sample of men and women drawn from the 8.2 million veterans who served in the military between August 1964 and May 1975. This included those who served in Vietnam and the surrounding areas (Theater veterans) and active duty veterans who served in other regions (Era veterans), as well as civilian controls. There were 1,200 male Theater veterans and 412 male Era veterans included in the overall sample. For the purposes of this study, an initial 100 Theater and 200 Era men were randomly selected. The Era veterans were initially oversampled because it was presumed that MI would be less frequent in that population. Subsequently, an additional 100 male Theater veterans were randomly selected to assess for saturation of MI themes.
Measures/Dataset
Events
All participants in the NVVRS were assessed for exposure to traumatic events through the following script:
Now we’d like to talk about unusual events that are extraordinarily stressful or disturbing—things that do not happen to most people but when they do they can be frightening, upsetting, or distressing to almost everyone. By that I mean things like being in a war or heavy combat, being physically assaulted or raped, being in a major earthquake or flood, or a very serious accident or fire, seeing other people killed or dead, or some other type of disastrous event (Kulka et al., 1990).
The emphasis on the words extraordinary, unusual and disastrous was to suggest the nature of the desired responses. Participants provided an open-ended account of each event, and no limitations were placed on the number or types of events reported.
Signs and symptoms
All Theater veterans were extensively questioned on the lasting impact of the Vietnam war. First, participants were asked: “How much would you say the Vietnam war has affected your everyday life? A great deal, a fair amount, hardly at all, or not at all?” Unless the participant responded with “not at all,” they were asked “In what ways has the Vietnam war affected your everyday life?” All Theater veterans were later asked:
Now, please tell me briefly, in your own words, how your experiences in or around Vietnam have affected your life? First, what were some of the positive things you gained from your Vietnam experience? And what were some of the negative things?
For the purposes of this study, responses to the two open-ended questions: (a) “In what ways has the Vietnam war affected your everyday life?” (Neutral Question) and (b) “And what were some of the negative things?” (Negative Question) were examined, and particularly assessed for signs and symptoms of MI.
Data Analysis
Initially, the responses to the open-ended questions listed above were gathered from randomly selected subsamples of 200 male Era veterans (events only) and 100 male Theater veterans (events and signs and symptoms). The research team reviewed all responses in the raw data for consistency with MI. These responses were then coded for MI themes, including the creation of new themes if applicable. If a given response fit into more than one theme, it was given the code deemed best fit by consensus of the research team. Next, the frequency (F) and extensiveness (E) were calculated for all codes (Krueger, 1998). F was determined based on the total number of times a theme was reported. E was also calculated to represent the total number of participants who had at least one response within a code.
After this analysis was complete, an additional 100 Theater veterans were randomly selected to assess for saturation of MI themes. The first subsample would be considered “saturated” if no new themes were found in the second subsample. Then, the research lab reviewed all responses from the events and signs and symptoms variables and identified responses consistent with MI. Finally, the data from the 200 Theater veterans was subject to further review. Specifically, the individuals who had responses coded as MI for events and at least one of the two signs and symptoms questions were identified and the responses were compared.
Results
Demographics
Demographic information is outlined in Table 1. Several participants served in more than one branch of the military, thus the total number of responses for that question is greater than 400.
Demographics.

Moral Injury
Events
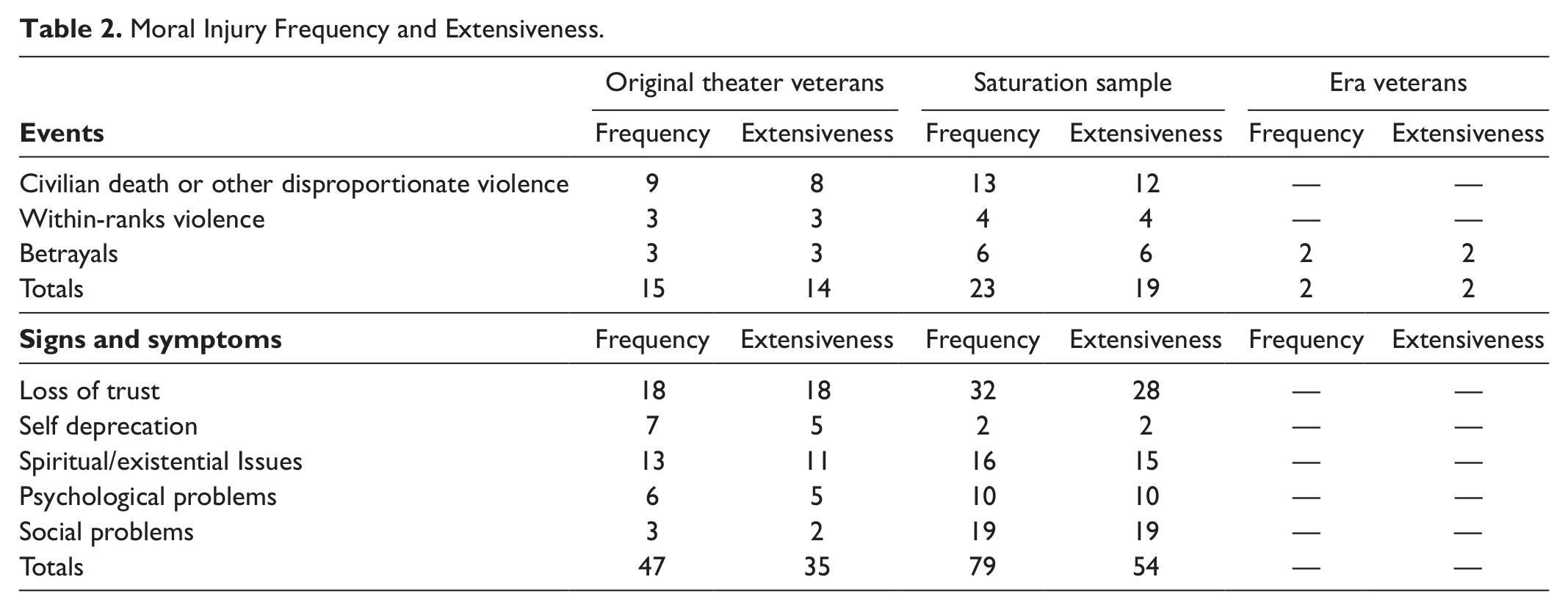
For the initial 100 Theater veterans, 15 responses from 14 individuals were identified as possible MI events. These were coded as Civilian Deaths (F = 9, E = 8) Within-Ranks Violence (F = 3, E = 3), and Betrayals (F = 3, E = 3). Examples from the Civilian Deaths category include “killing civilians,” and “Mama san and Papa san killed on bridge.” Within-Ranks Violence included “Being shelled—by either side,” “Mortar fire came from my own company,” and “Walking in rice paddies and received friendly fire.” Finally, Betrayals included responses such as “kid trying to steal hand grenade” and “laughing at people being killed.”
For the Era veterans, two responses from two individuals were coded as potential MI events. Specifically, these responses were “Car on fire couldn’t get girls out,” and “House fire tried to save the children and couldn’t.” Although both responses involved the death of children, these events did not take place in a war zone and therefore were not coded as Civilian Deaths. Instead, both were seen as a failure to live up to one’s own standards and were coded as Betrayal events (e.g., betrayal of their own standards for themselves).
Signs and symptoms
In terms of the Neutral Question, “In what ways has the Vietnam war affected your everyday life?” 12 veterans responded with 13 statements deemed consistent with signs and symptoms of MI. Specifically, Loss of Trust was identified in six responses from six veterans (e.g., “As far as the government goes, I feel like you can’t really trust the government to tell you what’s going on”); Self-Deprecation was coded for five statements from four veterans (e.g., “I’m a loser now I wanted us to win the war and we didn’t”); one response was indicative of Spiritual/Existential Issues (“Made me question my values”) and one statement indicated Psychological Symptoms (“It made me aware of human rights that were being misused over there in Vietnam”).
With regard to the Negative Question, “And, what were some of the negative things?” 34 responses from 28 veterans revealed signs and symptoms of MI. Specifically, Loss of Trust was identified in 12 statements from 12 veterans (e.g., “Feeling that the government didn’t really care about us over there” and “the feeling of lack of caring for us from the American people”); Spiritual/Existential problems were reported in 12 statements from 10 veterans (e.g., “The biggest thing was being forced to do something I was opposed to” and “How senseless a lot of the dying was”); Psychological Symptoms were indicated in five responses from five veterans (e.g., “Somewhat bitter about not finishing the job we started to do we weren’t allowed to win”); Social Problems were identified in three responses from two veterans (e.g., “The reverse of appreciation of life” and “Rejection by family and friends”) and Self-Deprecation was coded in two statements from one veteran ( “By not being able to be a combat soldier it gave me a guilt feeling”).
Theater veteran saturation sample
An additional 100 Theater veterans were randomly selected to assess for saturation of MI themes. All responses from the events and signs and symptoms variables were reviewed and responses consistent with MI were identified and coded. Overall, 23 events were identified as being MI (E = 19). Specifically, six responses from six veterans were identified as Betrayals (e.g., “Backing out of fire fight—Leaving American wounded”), 13 events from 12 individuals were coded as Civilian Deaths or Other Disproportionate Violence (e.g., “A child died when hit by a can of tuna fish” and “Downed chopper we came on everyone was mutilated”), and four exemplars from four participants were indicative of Within-Ranks Violence (e.g., “Friendly fire” and “Being bombed by our own air force”).
On the Neutral Question, 36 responses were coded as possible signs and symptoms of MI (E = 28). These included 10 responses coded as Loss of Trust (E = 10), nine which were coded as Spiritual/Existential Problems (E = 8), four Psychological Symptoms (E = 4), and 13 Social Problems (E = 13). Loss of Trust included responses such as “I find myself suspicious of most politicians” and “they, the people here, have never really let us come home.” Spiritual/Existential Problems included “My whole life is changed” and “I’ve never been satisfied since I came back, never.” Psychological Symptoms included “I have emotional problems, symptoms of anxiety” and “A lack of confidence I have trouble with that.” Finally, Social Problems included “I never felt like I was accepted back again” and “My mother thought I’d been killing kids.”
For Negative Question, 84 of the 100 Theater veterans provided responses, including 43 coded as possible signs and symptoms of MI (E = 34). These were coded as: Loss of Trust (F and E = 22), Spiritual/Existential Problems (F and E = 7), Psychological Symptoms (F and E = 6), Social Problems (F and E = 6), and Self-Deprecation (F and E =2). For this group, Loss of Trust included responses such as “Learned to distrust people, our government” and “A lot of people won’t employ a Vietnam veteran.” Spiritual/Existential problems included “Religion doesn’t mean as much to me as it did when I went in” and “Life means nothing, life is cheap.” Psychological Problems consisted of responses like “The total overload, just burned out” and “Thinking about all the death and dying, I still have nightmares. I was hurt and can’t get help.” Social Problems included “Dealing with people” and “People don’t care,” and finally, Self-Deprecation included responses such as “I learned to hate myself.”
For both events and signs and symptoms, the additional 100 Theater veterans provided responses that were consistent with the initial random sample. No new themes of MI were identified, suggesting that the initial 100 Theater veterans were sufficient to reach saturation for MI themes. See Table 2 for summary of the MI events and signs and symptoms reported by each group.
Moral Injury Frequency and Extensiveness.
MI signs and symptoms for MI events
Further analysis was conducted on the 200 Theater veterans regarding the responses coded as MI. To explore the relationship between the identified MI events and signs and symptoms, these responses were directly compared. That is, for the 33 individuals who had at least one response coded as an MI event, the signs and symptoms were examined to identify any MI coding. Overall, 19 participants reported both at least one event and at least one sign and symptom coded as consistent with MI. These 19 individuals provided 22 events and 31 signs and symptoms, for a total of 33 overlaps between events and signs and symptoms. Figure 1 shows the overlaps between events and signs and symptoms broken down by event codes.

Comparison of MI events and symptoms.
Discussion
In an attempt to enhance the validity of the MI construct, this exploratory study utilized a randomly selected subsample from a nationally representative sample of veterans to determine if the current understanding of MI could be corroborated by primary source material. The goal of this study was to ascertain if the traumatic experiences and functional impairments reported by Vietnam veterans included thematic events and signs and symptoms of MI indicated in Drescher et al. (2011). In addition, signs and symptoms of MI were further assessed for combat veterans who endorsed exposure to an MI event.
The themes of traumatic events associated with MI proposed by Drescher et al. (2011) include betrayal, disproportionate violence, incidents involving civilians, and within-ranks violence. Qualitative analyses of traumatic experiences reported by Theater veterans identified possible MI events consistent with Drescher et al. (2011) including Civilian Deaths or Other Disproportionate Violence, Within-Ranks Violence (specifically, Friendly Fire), and Betrayals. Thus, the data from the Theater veterans sample was consistent with the experiences of experts in the field.
To serve as a comparison group, traumatic events reported by Era veterans were also examined. Qualitative analyses of the data reported by the Era veteran subsample identified two responses from separate participants involving the inability to prevent the pain and suffering of children as consistent with Betrayal as defined by Drescher et al. (2011), specifically involving the failure to live up to one’s own values. Hence, these findings suggest that exposure to an MI related event is either particular to combat veterans or that it may be experienced by noncombat veterans in response to a sense of failure in living up to their own moral standards (i.e., personal betrayal). The questions assessing signs and symptoms of MI were related to the long-term impact of the Vietnam war, and as such, the Era veterans were not asked these questions. Thus, information on the signs and symptoms of MI is not available for this group.
To examine psychological complaints potentially associated with an MI event, thematic symptoms of MI were also examined utilizing the same Theater veterans. Analysis by the principle investigator and research lab members revealed that all themes from the Drescher et al. (2011) coding scheme were present within the examined NVVRS data. Specifically, Loss of Trust was the most frequently observed theme, followed by Spiritual/Existential Issues, Social Problems, Psychological Symptoms, and Self-Deprecation.
The findings of this study support the concept that moral and ethical violations which do not fit into traditional models of trauma can still be injurious to war veterans. Although trauma research and treatment has traditionally focused on the consequences of being the victim of, or witness to, violence, during the course of their military service these men were required to perform acts which go against their own deeply ingrained sense of right and wrong, for example, perpetration of violence. In fact, many of the traumatic events which were not coded as MI included traditional combat experiences (e.g., being involved in a firefight), supporting the research that sanctioned killings have a significant impact on the perpetrators.
Because the NVVRS data was collected after the end of the Vietnam war, 11 to 24 years after the men served, it is important to note that the presence of MI responses points to the enduring nature of signs and symptoms associated with MI. Some participants may have resolved their MI symptomatology prior to NVVRS data collection, thus additional signs or symptoms of MI may have been observed in these veterans’ responses if interviews had been conducted closer to their wartime military service.
Findings of the present study indicate that the Vietnam war clearly influenced the types of MI signs and symptoms that were ingrained within its veterans. For instance, the F and E of the two themes Loss of Trust and Spiritual/Existential Problems exceeded that of the other MI themes. The sociopolitical context surrounding the United States’ involvement in Vietnam, and the unique style of guerrilla warfare associated with this war likely contributed to these findings. Comparing the present study findings to those of Drescher et al. (2011), the heightened prevalence found of the Loss of Trust theme was particularly significant, as it was the theme least mentioned by experts. The predominance of this theme also suggests that there may be fundamental differences between veterans’ experiences in earlier or later wars and the unique experience of Vietnam.
It is interesting to note that guilt and shame were readily observable among MI responses in the form of the theme Self-Deprecation. Although they are not the most frequently identified theme, these findings still suggest that guilt and shame are important psychological symptoms associated with the MI construct.
Although this study did not include mental health outcome measures, comparisons of the identified MI events and signs and symptoms revealed several overlaps. In particular, Civilian Deaths or Other Disproportionate Violence were the most likely MI events to have associated signs and symptoms reported. Specifically, Civilian Deaths or Other Disproportionate Violence was associated with eight Spiritual/Existential Problems, six codes of Loss of Trust, six Psychological Problems, four Social Problems, and one Self-Deprecation. In contrast, Betrayal events and Within-Ranks Violence were associated with each signs and symptoms code between zero and two times. These findings suggest that civilian deaths (or disproportionate violence) may have a unique impact on an individual’s Spiritual/Existential functioning, and that this type of MI should be emphasized when considering appropriate interventions.
Overall, the findings appear to be largely consistent with those of Drescher et al. (2011), and add to the validity of MI as a construct. Themes put forth by Drescher et al. were found within the NVVRS narrative reports given by Vietnam combat veterans themselves. Moreover, the analysis of overlapping MI events and signs and symptoms appear to extend the validation of the MI construct. If the concept of MI is robust, then the same individuals who report MI events should also report MI signs and symptoms, and this occurred with 19 of the 33 individuals who reported MI events. While no new traumatic events or symptom parameters associated with MI were identified, the results do enhance the validity of the themes currently in use in that they were shown to be useful descriptors of MI in additional contexts.
Lastly, these findings advocate for the idea that it is necessary to expand the current conceptualization of combat trauma to include MI. Many of the themes fall outside the purview of the diagnostic criteria for PTSD, thus indicating that unique sets of reactions to traumatic experiences exist, including those that occur when a person’s moral framework has been violated. In this way, this study serves as further evidence of the construct validity of MI, and highlights the need for a bio-psycho-social-spiritual model to address injuries related to moral and ethical dilemmas faced by combat veterans.
Limitations
One limitation of the current study was that it relied upon NVVRS archival data that was not intended to be used in the examination of the current construct under investigation. As a result, questions may not have been asked in a manner that facilitated identification of all associated thematic constructs, and the questions themselves were targeted at other information (e.g., identifying Criterion A events for PTSD, in the case of the events question). Another limitation of the current study was that it relied upon self-report data, which includes the possibility of self-report bias in the results. For example, due to associated stigma, participants in the NVVRS may not have reported all their symptoms to interviewers, or may have avoided reporting wartime events of which they were ashamed (possibly including MI events).
There may have been limitations associated with the deductive aspects of this particular qualitative approach. The research lab members were not blind to the thematic events or signs and symptoms of MI from the Drescher et al. (2011) study, and approached the data with informed thought when assigning themes. As a result of this approach, inherent bias may have occurred. In other words, researchers may have been more apt to find evidence that was supportive rather than nonsupportive of the previous theory, possibly blinding them to other contextual aspects of the phenomenon.
A final limitation exists in that the study specifically examined the responses of male Vietnam veterans who served within the war zone and experienced traumatic combat events there. Thus, the results cannot be directly extended to women or survivors of other types of trauma that may involve MI.
Future Research
While this study represents a significant step forward in the validation of the MI construct, future studies should investigate MI in other types of trauma. For example, narrative accounts of law enforcement personnel should be qualitatively examined for unique signs and symptoms of MI. Additionally, psychometrically sound measures should be developed that assess exposure to MI events and related signs and symptoms. Perhaps even more important is the emphasis upon identifying appropriate interventions to alleviate MI related distress. New interventions have to be developed, or existing interventions adapted, and then tested for efficacy.
Clinical Implications
In the meantime, when MI is observed in clinical cases, giving attention to MI events and symptomatology an important part of the treatment process. When veterans describe their combat-related MI reactions, such as spiritual/existential issues, it is important that clinicians be familiar with a bio-psycho-social-spiritual model of combat trauma that also addresses spiritual aspects of mental health functioning.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.