
Abstract
Delays in wound healing often result in infection, chronic ulceration, and possible amputation of extremities. Impaired wound healing is a major complication of the 23 million people in the USA with diabetes, and financial and medical burdens are demanding new treatments for wound healing. Previous studies have demonstrated that topical application of the opioid antagonist naltrexone (NTX) dissolved in moisturizing cream reverses delays in wound closure in rats with streptozotocin-induced type 1 diabetes. A target of NTX’s action is DNA synthesis and cell proliferation. In this study, granulation tissue was evaluated to ascertain the specific cellular targets that were impaired in diabetic wounds, as well as those that were enhanced following NTX application. Mast cell number as well as the number of new blood vessels immunoreactive to fibroblast growth factor-2 (FGF-2), vascular endothelial growth factor (VEGF), and alpha smooth muscle actin (α-SMA) antibodies were recorded at 3, 5, 8, 10, 15, and 20 days following creation of full-thickness dorsal cutaneous wounds in normal and type 1 diabetic rats. Diabetic rats displayed delays in wound closure as well as a reduction in the number of mast cells responding to the injury, and delays in the spatial and temporal expression of FGF-2, VEGF, and α-SMA in capillaries. Topical NTX accelerated the rate of wound closure and stimulated expression of angiogenic factors within granulation tissue of diabetic rats relative to control animals receiving saline in moisturizing cream. These data support observations that a novel biological pathway is impaired under diabetic conditions and can be modulated by topical NTX to enhance proliferative events in wound healing.
Keywords
Introduction
Impaired wound healing is a major complication of diabetes that can result in chronic debilitating ulcers and lead to amputation. Given the rapid rise in diagnosis of diabetic persons in the United States, along with the escalating costs for treatment of diabetic wounds, there is a challenge to identify treatments that target the underlying pathophysiology of wound healing. There is currently no fully effective prevention or treatment for these complications. Initial studies from our laboratory have shown that blockade of endogenous opioids and their receptors enhance wound closure. Using an opioid antagonist naltrexone (NTX), at a dosage that blocks endogenous opioids which inhibit cell proliferation, it has been reported that re-epithelialization is stimulated in cutaneous diabetic wounds. 1
Endogenous opioids are present in neural and non-neural tissues, and mediate cell proliferation, angiogenesis, and tissue migration, as well as immunity and neuromodulation.2–5 Studies measuring circulating levels of native opioids in diabetes have reported that both type 1 and type 2 diabetic animals including the genetically obese (db/db) mouse, 6 and type 1 diabetic (T1D) humans,7,8 have elevated levels of the opioid peptide [Met 5 ]-enkephalin. Behaviourally, an associated complication of diabetes has been diminished nociception which may be related to the elevated opioids. 9
Previous studies have shown that endogenous opioids, as well as classical and non-classical opioid receptors, are present in skin.2,10–12 One endogenous opioid, opioid growth factor (OGF), chemically called [Met 5 ]-enkephalin, regulates DNA synthesis and proliferation of corneal epithelium13–15 and skin. 2 Exogenous OGF inhibits DNA synthesis, with the mechanism being a receptor-mediated, reversible action that targets upregulation of the cyclin-dependent inhibitory kinases p16 and/or p21. 16 Topical or systemic application of NTX blocks the interaction of OGF with its receptor, OGFr, and enhances cell proliferation.
The efficacy of NTX as a topical treatment of cutaneous wounds in streptozotocin (STZ)-induced hyperglycaemic, T1D (DB) rats was demonstrated by administration of NTX (10−5 mol/L) dissolved in moisturizing cream3,15 and recording accelerated wound closure in T1D rats. The current study examines granulation tissue within the cutaneous wounds over 20 days and evaluates the effects of NTX on proliferation of cells related to inflammatory processes and angiogenesis. Cutaneous tissues within the full-thickness wounds surgically created in normal and T1D rats, and treated with either NTX or saline (control, vehicle) dissolved in moisturizing cream, were examined for the number of neutrophils and mast cell infiltration as markers of inflammation. In addition, the number of new blood vessels identified by the presence of fibroblast growth factor-2 (FGF-2), vascular endothelial growth factor (VEGF), and alpha smooth muscle actin (α-SMA) were recorded as markers for angiogenesis.
Material and methods
Animals and induction of diabetes
Adult male Sprague-Dawley rats (∼150 g; Charles River Laboratories, Wilmington, MA) were housed in an environmentally controlled animal room, and provided with water and food (2018 Global Rodent Diet, Teklad®, Indianapolis, IN) ad libitum. Investigations conformed to an approved protocol and the guidelines of The Pennsylvania State University College of Medicine Institutional Animal Care and Use Committee.
At six weeks of age, T1D was induced by intraperitoneal (i.p.) injection of 40 mg/kg STZ (Sigma, St. Louis, MO) on two consecutive days. 15 This regimen produced insulin-dependent diabetes in 100% of the animals within 72–96 h and with minimal death. Blood glucose was monitored from the tail vein using a True Track Smart System glucometer (Home Diagnostics, Ft. Lauderdale, FL). Measurements were taken prior to receiving STZ, as well as at 1, 4, and 8 weeks after induction of hyperglycaemia. Blood glucose levels that measured >350 mg/dL indicated a hyperglycaemic state. Control animals received injections of citrate and were considered normal (N). All rats were weighed weekly and utilized for experimentation eight weeks following the induction of T1D when the rats were 14 weeks of age. If an animal’s blood glucose levels remained >600 mg/dL and the animal appeared lethargic and unresponsive to food and water, it was not included in the study.
Cutaneous wounds and NTX application
One day prior to wounding, a 6 × 10 cm area was shaved on the dorsal surface using electric clippers. Cutaneous wounds were created following methodology described previously. 1 Animals were anaesthetized by i.p. injection (0.25 mL) of a cocktail of ketamine (60 mg/kg), xylazine (10 mg/kg), and acepromazine (1 mg/kg). Under sterile conditions, four 6 mm full-thickness circular excisional skin wounds were positioned 1 cm off the midline, with two wounds in the pelvic and two wounds in the pectoral regions. Tissue was removed down to the level of the panniculus muscle using an Acupunch (Acuderm Inc., Fort Lauderdale, FL). Following surgery, the wound sites were treated with an antiseptic, but left uncovered. All surgeries were conducted between 08:00 and 09:00 h in order to alleviate diurnal rhythm effects.
Topical administration of ∼0.1 mL NTX cream (1:1, v/v of 10−5 mol/L NTX thoroughly mixed into Neutrogena moisturizing cream) or vehicle cream (0.5 mL of saline mixed into Neutrogena moisturizing cream) was initiated immediately following surgery, and given at 08:00, 12:00, and 17:00 h thereafter.
Photography
Areas of residual wound were monitored by capturing images with a digital camera mounted on a tripod located ∼15 cm from the surface. Changes in magnification were corrected by photographing a ruler with each wound. For photography, rats were manually sedated by isoflurane regulated with a mixture of oxygen. Photographs were taken immediately after surgery and every other day for 20 days. Areal analyses of the images were performed using Image ProPlus 6.2 (Media Cybernetics, Inc., Bethesda, MD), and the percent residual wound was calculated at each time point for every rat.
Histopathology
Full-thickness wounds were harvested for histopathology at 3, 5, 8, 10, 15, and 20 days following surgery. At each time point, three to six rats in each treatment group were euthanized for wound analysis, providing at least 12 wounds for each time point from at least three different animals. Rats were euthanized with a 0.5 mL i.p. injection of Euthasol® (Virbac AH, Inc, Fort Worth, TX). Following euthanasia, a dissection (3 cm2) was performed around each wound, tissue bisected with a scalpel, and removed, fixed, and processed for paraffin embedding. Sections (6 µm) with the greatest diameter of residual wound were collected for immunohistochemical analyses. In addition, two unwounded normal and diabetic rats were euthanized and tissue collected in order to establish baseline levels of angiogenesis markers and mast cell number.
Granulation tissue within the wound site was assessed for mast cell number, neutrophil infiltration, and new blood vessel formation. Angiogenesis was analysed in granulation tissue using standard immunohistochemistry protocols17–20 and primary antibodies specific for cell types associated with blood vessel formation. An early marker for new blood vessel formation is the appearance of FGF-2 which is an initiator of angiogenesis. Endothelial cells within new blood vessels were identified by basic FGF using FGF-2 primary antibody (1:150; Abcam®, Cambridge, MA). VEGF detected endothelial cells in vessels, and α-SMA was used to mark smooth muscle cells in new blood vessels. Endothelial cell development was analysed based on modified methods 20 with anti-VEGF A-20 polyclonal antibody (1:200; Santa Cruz Biotechnology®, Santa Cruz, CA). Newly developing capillaries were defined as tubular structures with approximately 90% of the endothelial cells expressing FGF-2 or VEGF. Analysis of smooth muscle development was accomplished by counting blood vessels that expressed α-SMA (1:200; Dako®, Carpinteria, CA) in the smooth muscle wall of the capillary. Sections were examined with an Olympus BH2-RFCA microscope at × 25 magnification. Positively stained blood vessels were quantified from an area of 3.1 mm 2 within the granulation tissue. Capillary cross-sections less than the area of a single grid square were not included for evaluation.
Data analysis
Body weights and glucose measurements were analysed using analysis of variance (ANOVA) with condition (normal or diabetic) and time as a repeated measure. Areal measurements of defects (e.g. percent residual wound, contraction) were analysed using a multifactorial ANOVA with condition (normal or diabetic) and treatment (NTX or saline) and time. All wounds were not measured on all days as some animals were euthanized for histopathology. Tissues for histopathology were collected from different experiments, thus the numbers of antibody-positive cells were evaluated using a two-factor ANOVA with condition and treatment. All subsequent planned comparisons were made with the Newman–Keuls tests.
Results
Induction of hyperglycaemia
Adult, male Sprague-Dawley rats weighed approximately 230 g at six weeks of age. Within two weeks of STZ injection, these rats weighed 10% less than normal males receiving citrate injections, and by week 8 weighed 340 ± 7 g, a 29% reduction in body weight relative to that of normal animals (Figure 1a). Rats receiving STZ were rendered hyperglycaemic with blood glucose levels reaching >450 mg/dL within 48–72 h of STZ injection; three rats died from high glucose levels over the course of eight weeks, whereas no normal rats died (Figure 1b). A total of 34 normal rats yielding 67 wounds treated with NTX (44 wounds) or saline in moisturizing cream (23 wounds) were assessed, and 23 T1D animals providing 26 wounds treated with NTX and 16 wounds treated with saline in moisturizing cream (i.e. vehicle) were evaluated.
The body weights and glucose levels of STZ-induced type 1 diabetic (DB) and normal adult male rats over an 8-week period. (a) Body weights were recorded prior to STZ injection (week 0), and weekly thereafter. (b) Blood glucose levels were assessed before (week 0) and at 1, 4, and 8 weeks after STZ administration. Values represent means ± SEM for 10–22 animals/group at each time point. Significantly different from normal values at **P < 0.01 and ***P < 0.001. STZ: streptozotocin. (A color version of this figure is available in the online journal)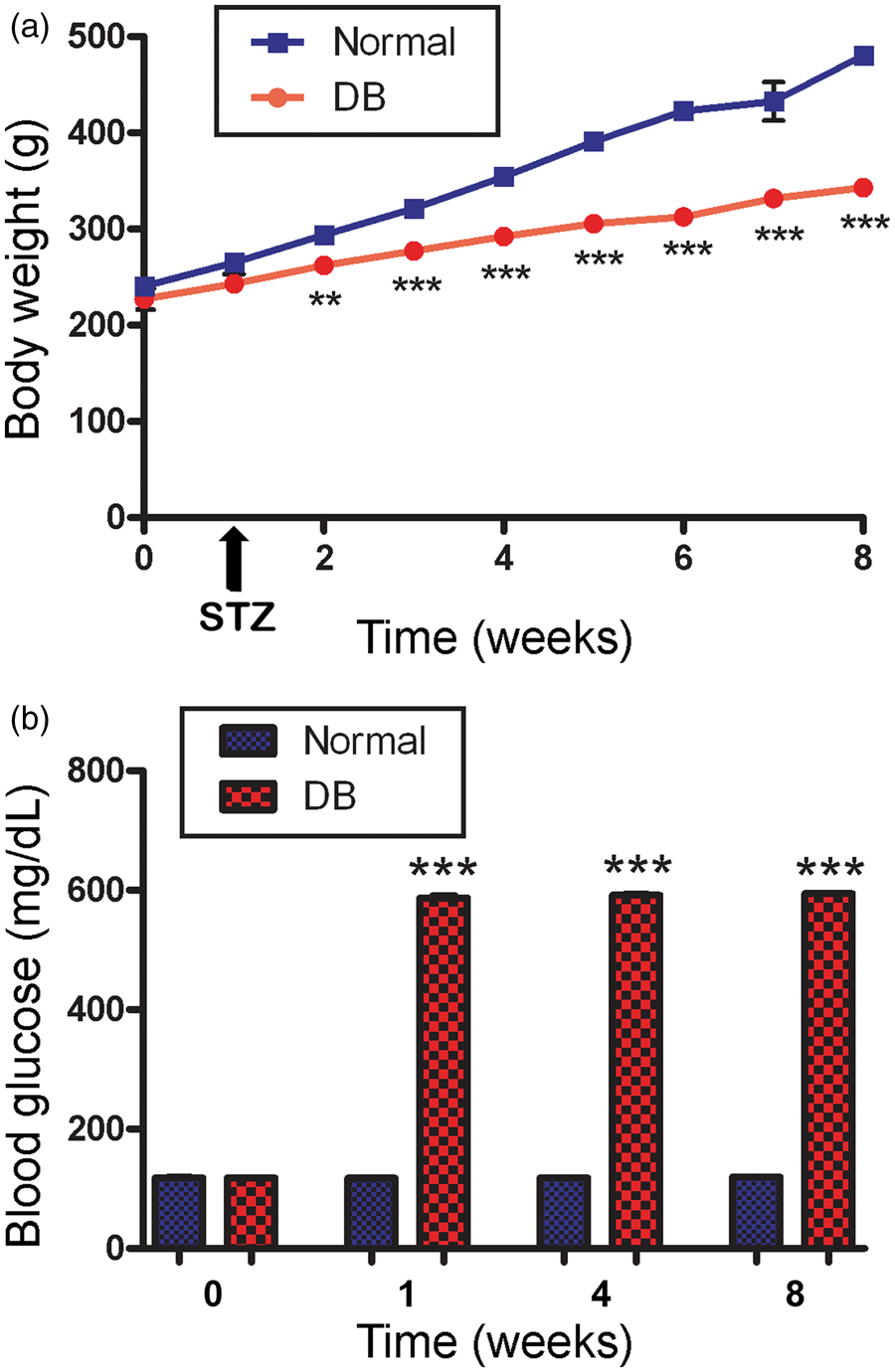
Full-thickness wound closure
Between 2 and 10 days, rats in the N + NTX group had reductions of 6–26% in wound size relative to normal rats receiving vehicle; residual wounds after day 12 were minimal (Figure 2). Between days 2 and 16 following surgery, diabetic rats receiving vehicle had 3–14% larger wounds relative to normal animals receiving sterile saline in vehicle, with residual wounds being up to four-fold larger than those in the N + vehicle group. Exposure to topical NTX reduced the residual wound area in diabetic rats at every time point examined between days 2 and 16; reductions in residual wound size for the DB + NTX group ranged from 5% to 88% relative to the DB + vehicle group. On days 10, 12, and 14, the diabetic group receiving NTX had residual wounds that were reduced 62–89% from those in diabetic rats receiving vehicle. Between days 6 and 18, the residual wound area of diabetic rats treated with NTX was comparable with those for normal rats receiving vehicle (Figure 2); on day 8, the diabetic group receiving NTX had significantly smaller wounds than those recorded for the N + vehicle rats.
Full-thickness wound closure following application of topical NTX to normal and hyperglycaemic rats. (a) Photographs of full-thickness wounds created on the dorsal surface of normal and type 1 diabetic rats. Wounds were treated three times daily with either 10−5 mol/L NTX (NTX) or saline (vehicle) dissolved in Neutrogena moisturizing cream. Photographs were taken immediately after surgery (day 0), and every other day for 18 days. Bar = 5 mm. (b) Histograms of residual defects (%) of 6 mm wounds treated with either NTX or vehicle over an 18-day period of time. Significantly different from normal + vehicle measurements at *P < 0.05, **P < 0.01, and ***P < 0.001; significantly different from DB + vehicle group at ++P < 0.01 and +++P < 0.001. NTX: naltrexone; DB: diabetic. (A color version of this figure is available in the online journal)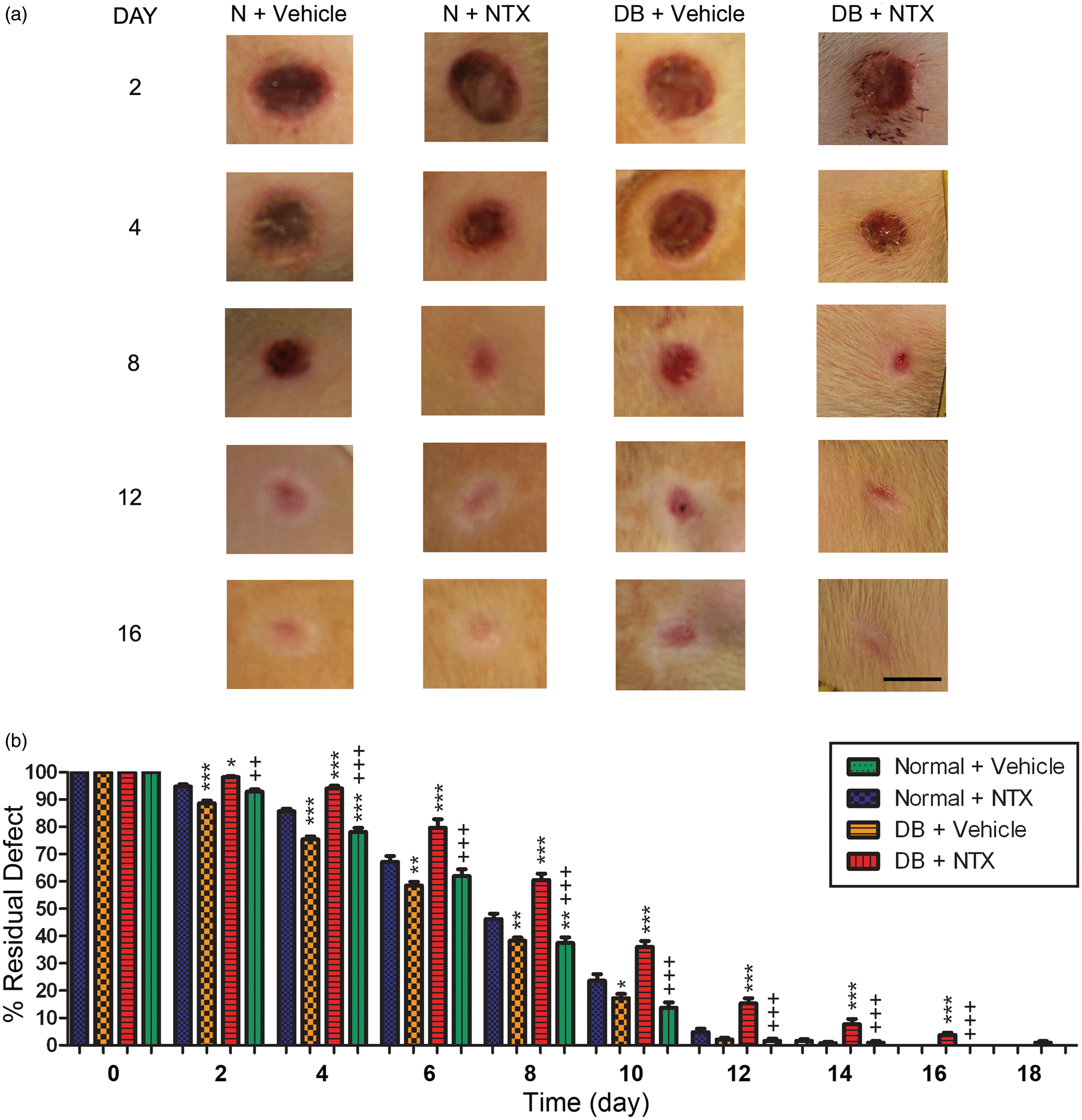
Analyses of wound closure across the 18-day period following surgery revealed significant interactions between treatment and condition on all days until day 19 when wound were nearly resolved. Treatment (NTX or saline) had a larger effect on rate of closure than condition, but interactions were significant on all days. Comparison of the rates of healing as indicated by the slopes of lines between days 6 and 10 revealed that DB/NTX animals had a faster rate of wound closure during that period in comparison with N/NTX rats.
Unwounded skin
In order to establish a basis for changes in inflammation and angiogenesis following the creation of full-thickness cutaneous wounds, unwounded skin from normal or diabetic rats was evaluated for the number of mast cells. Values for the number of mast cells, as well as positively stained blood vessels (i.e. FGF-2, VEGF, and α-SMA), in unwounded skin were comparable.
Inflammation phase of wound closure
The total number of mast cells within a 3.1 mm
2
area of granulation tissue was recorded as a measure of inflammation in tissue samples collected 3, 5, 8, 10, 15, and 20 days after wounding (Figure 3). Within three days of surgical wounding, mast cell number was elevated to 40–50 cells/area in all groups above baseline values (∼16 cells/3.1 mm2) for unwounded tissue. A two-factor ANOVA of these data revealed that diabetic rats receiving vehicle (DB + vehicle) had significant reductions in mast cell number on days 3, 5, and 8 from N + vehicle groups. In contrast, normal and diabetic rats exposed to NTX had increases in mast cell number on days 5 and 8, with differences between DB + vehicle and DB + NTX groups evident on days 5, 8, and 10. By day 10, the mast cell number in DB + vehicle tissues was equal to that of normal tissue on day 3 following wounding. Significant interactions between treatment (NTX, saline) and condition (DB, normal) were noted on days 8 and 10, suggesting that the enhancement of cell number of NTX was greater for DB rats than observed for the normals (Figure 3).
The number of mast cells present in granulation tissue surrounding wounds in diabetic (DB) and normal (N) rats topically treated with either NTX or vehicle. Values represent means ± SEM for the number of mast cells per area (3.1 mm2) of granulation tissue located within the original wound. Significantly different from N + vehicle at *P < 0.05, **P < 0.01, and ***P < 0.001; significantly different from DB + vehicle at ++P < 0.01 and +++P < 0.001. NTX: naltrexone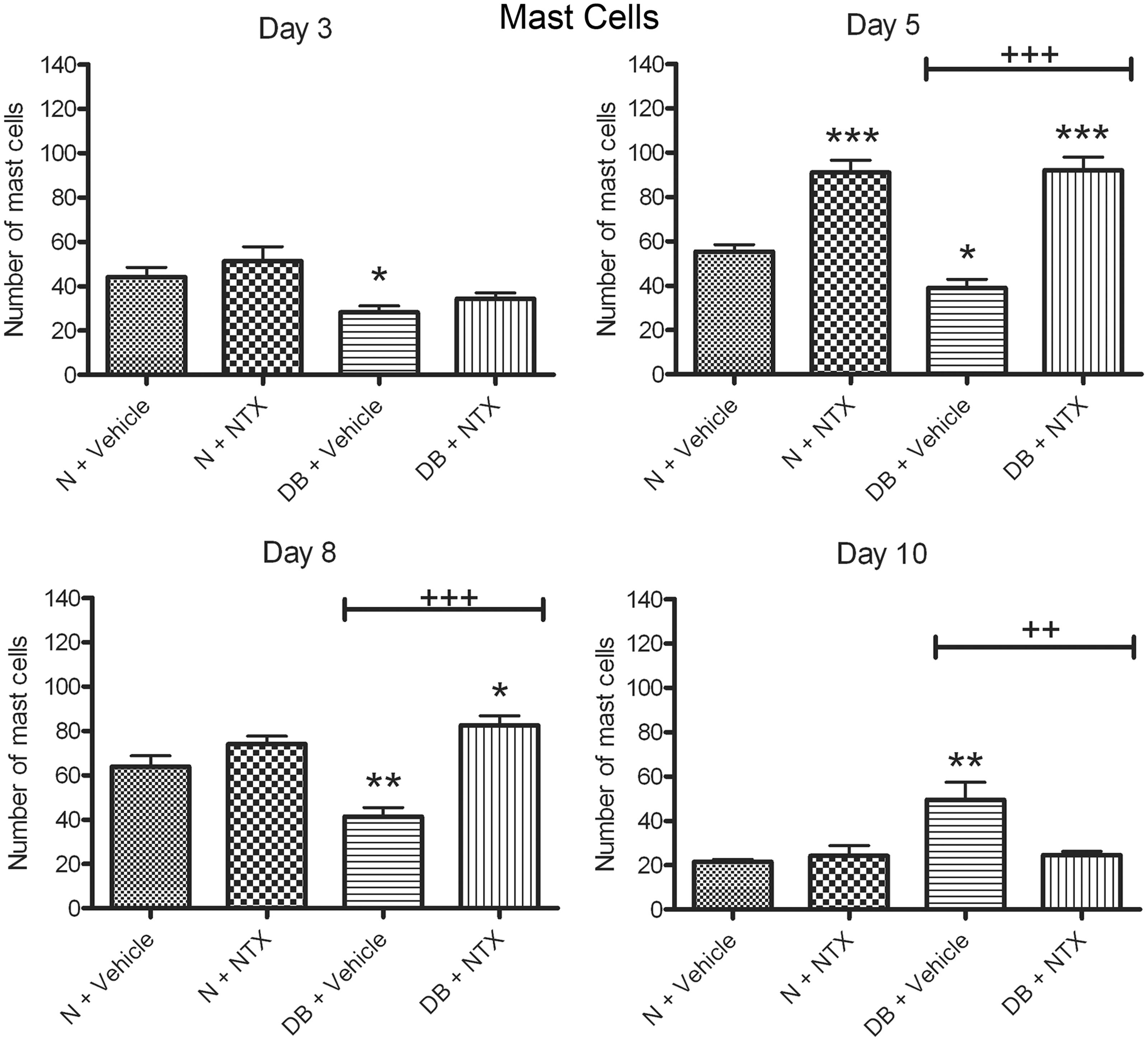
The infiltration of neutrophils to the wound site is an early response in healing. The number of neutrophils recorded in the granulation tissue ranged from 60 to 80 per area (3.1 mm2). Values were elevated in all groups within three days of wounding, and neutrophil number remained elevated above baseline unwounded values for at least 10 days in all groups.
Angiogenesis phase of wound closure
FGF-2 expression was increased following wounding (Figure 4) relative to unwounded skin. Two-factor analyses revealed significant interactions between condition (DB, normal) and treatment (NTX, saline) on days 3, 5, and 10 suggesting that the effects of NTX were more marked for DB rats than normals. On day 3 following surgical wounding, T1D rats receiving vehicle cream had 2.8-fold fewer blood vessels expressing FGF-2 relative to tissue taken from normal rats receiving vehicle (Figure 4), whereas diabetic rats with wounds treated with NTX had an increase of 46% in FGF-2 positive cells relative to N + vehicle rats, and a four-fold increase in FGF-2 stained blood vessels relative to those in the DB + vehicle group (F1,21 = 4.5; P < 0.04). On days 8 (F1,20 = 7.9; P < 0.01) and 10 (F1,20 = 9.85; P < 0.005), when the N + vehicle and DB + NTX groups displayed 5–11 FGF-2 positive blood vessels per region, the animals in the DB + vehicle group had 3.7 - to 4.1-fold more FGF-2 positively stained vessels relative to all other groups. By days 15 and 20, FGF-2 expression was negligible in blood vessels of diabetic animals, and comparable to that of unwounded tissue.
FGF-2 expression in full-thickness skin wounds from normal (N) and diabetic (DB) rats receiving topical NTX or vehicle for 3, 5, 8, or 10 days. Representative photomicrographs of blood vessels positively stained for FGF-2 on day 3 following wounding (bar = 25 µm). Values represent mean ± SEM number of vessels with FGF-2 stained cells. Significantly different from N + vehicle group at *P < 0.05 and **P < 0.01; significantly different from the DB + vehicle group at ++P < 0.01 and +++P < 0.001. FGF: fibroblast growth factor; NTX: naltrexone. (A color version of this figure is available in the online journal)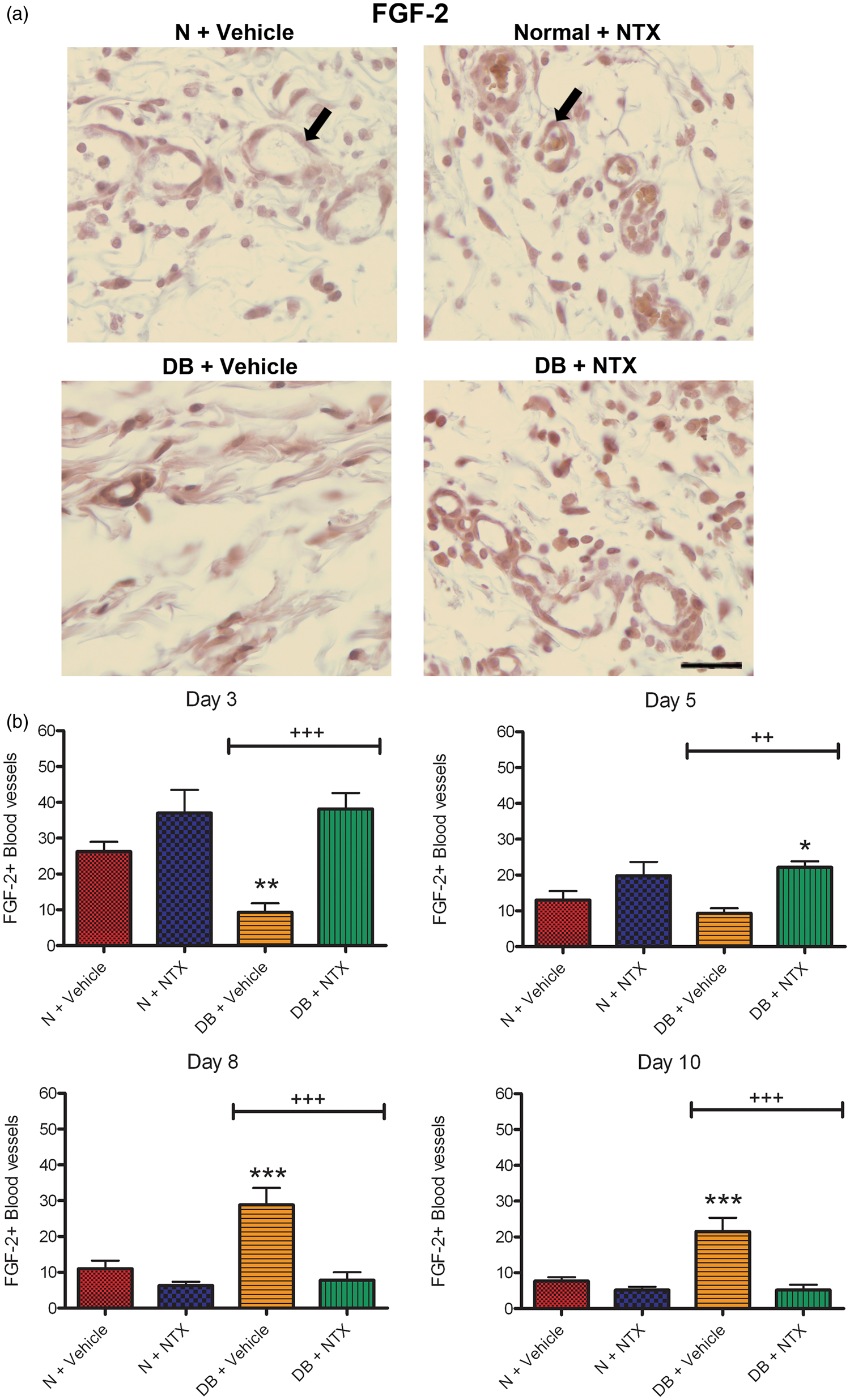
The number of VEGF-positive cells was significantly elevated at three and five days after wounding in both N + NTX and DB + NTX groups. The number of VEGF-positive vessels at three, five, and eight days between diabetic rats receiving NTX and diabetic rats receiving vehicle (Figure 5) were significantly different. Two-factor analysis of the number of blood vessels stained with VEGF revealed significant interaction (F1,18 = 14.52; P < 0.0013) on day 8 between condition (diabetic, normal) and treatment (NTX, saline). Within three days of wounding, VEGF stained cells were detected in ∼45 vessels per area monitored in both the N + NTX and DB + NTX groups in comparison to 22 vessels/area in the N + vehicle group and 14 vessels/area in the DB + vehicle group. The number of VEGF stained vessels in the NTX-treated groups remained markedly elevated in the respective vehicle-treated wounds on day 5, with reductions of more than two-fold fewer vessels noted in the DB + vehicle group relative to the DB + NTX group. By days 15 and 20 following the surgical wounding, the number of vessels with VEGF staining in all groups averaged less than half a vessel per region.
VEGF expression in full-thickness skin wounds from normal (N) and diabetic (DB) rats receiving topical NTX or vehicle for 3, 5, 8, or 10 days. Representative photomicrographs of blood vessels positively stained for VEGF taken on day 5 following wounding (bar = 25 µm). Histograms (mean ± SEM) represent the number of vessels with VEGF stained cells. Significantly different from N + vehicle group at *P < 0.05, **P < 0.01, and ***P < 0.001; significantly different from the DB + vehicle group at ++P < 0.01 and +++P < 0.001. VEGF: vascular endothelial growth factor; NTX: naltrexone. (A color version of this figure is available in the online journal)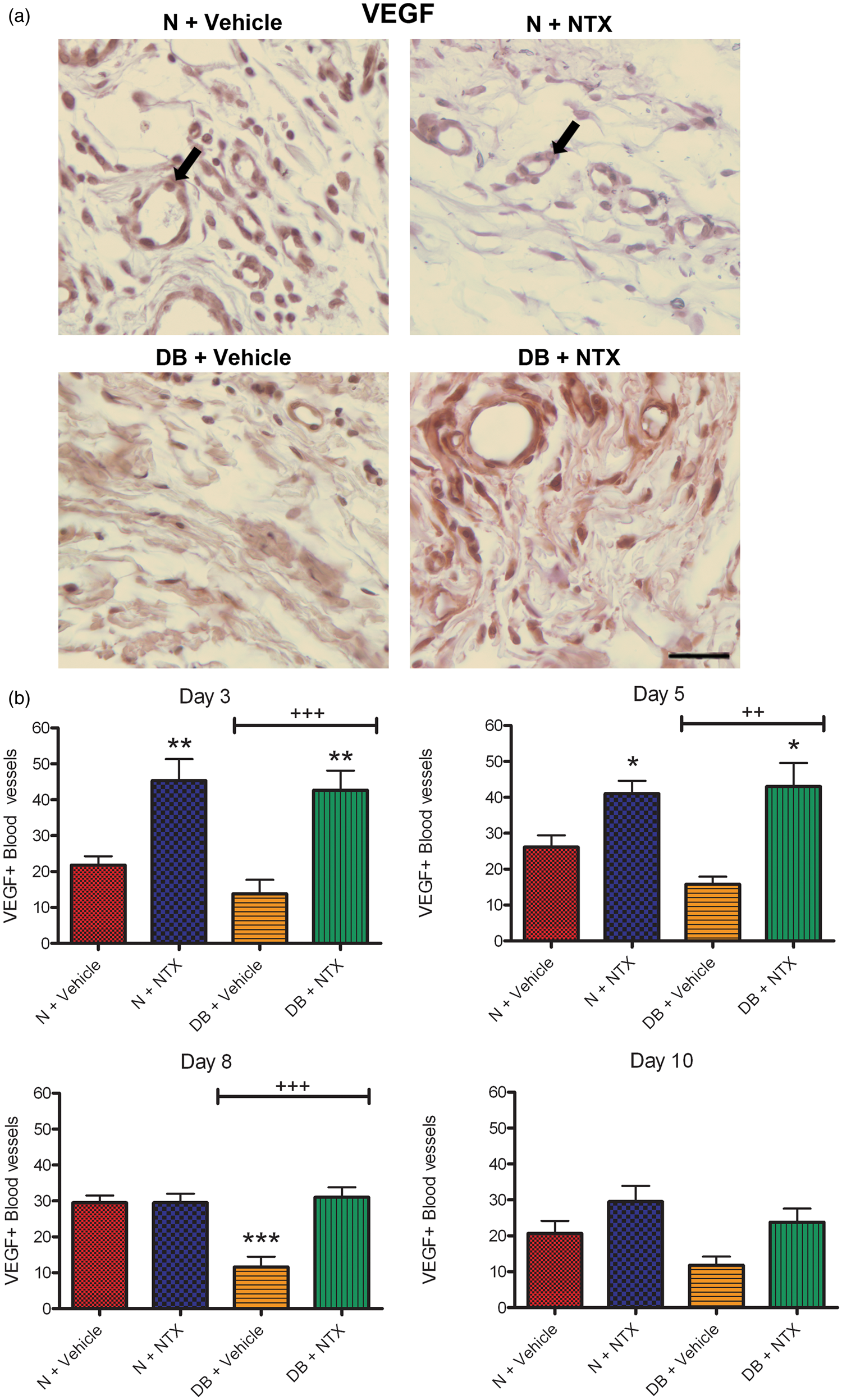
A third marker indicating the growth of new blood vessels is α-SMA. Examination of granulation tissue adjacent to the wound revealed a stimulated appearance of α-SMA on days 8 and 10 in normal tissues treated with NTX relative to N + vehicle samples (Figure 6) with more than 47 vessels/area staining with α-SMA in both NTX treated groups relative to ∼21 vessels stained in the vehicle-treated wounds. On days 3, 5, and 10, significant interactions between condition and treatment were noted, suggesting that the effect of NTX on DB rats was greater than on normal rats. NTX treatment altered the number of vessels with positive α-SMA reactivity in both DB and normal rats. Differences in the number of blood vessels that expressed α-SMA proteins between DB + vehicle and DB + NTX groups were evident on days 3, 5, 8, and 10, with as many as two-fold more vessels recorded in the DB + NTX group relative to DB + vehicle specimens. By days 15 and 20, treated and untreated groups had comparable expression of α-SMA.
Expression of α-smooth muscle actin (α-SMA) in full-thickness skin wounds from normal (N) and type 1 diabetic (DB) rats receiving topical NTX or vehicle for 3, 5, 8, or 10 days. Representative photomicrographs of blood vessels positively stained for α-SMA five days after wounding (bar = 25 µm). Histograms represent mean ± SEM number of vessels with α-SMA stained cells within the granulation tissue. Significantly different from N + vehicle group at *P < 0.05 and **P < 0.01. Diabetic rats receiving NTX differed from the DB + vehicle rats at +P < 0.05 and ++P < 0.01. NTX: naltrexone. (A color version of this figure is available in the online journal)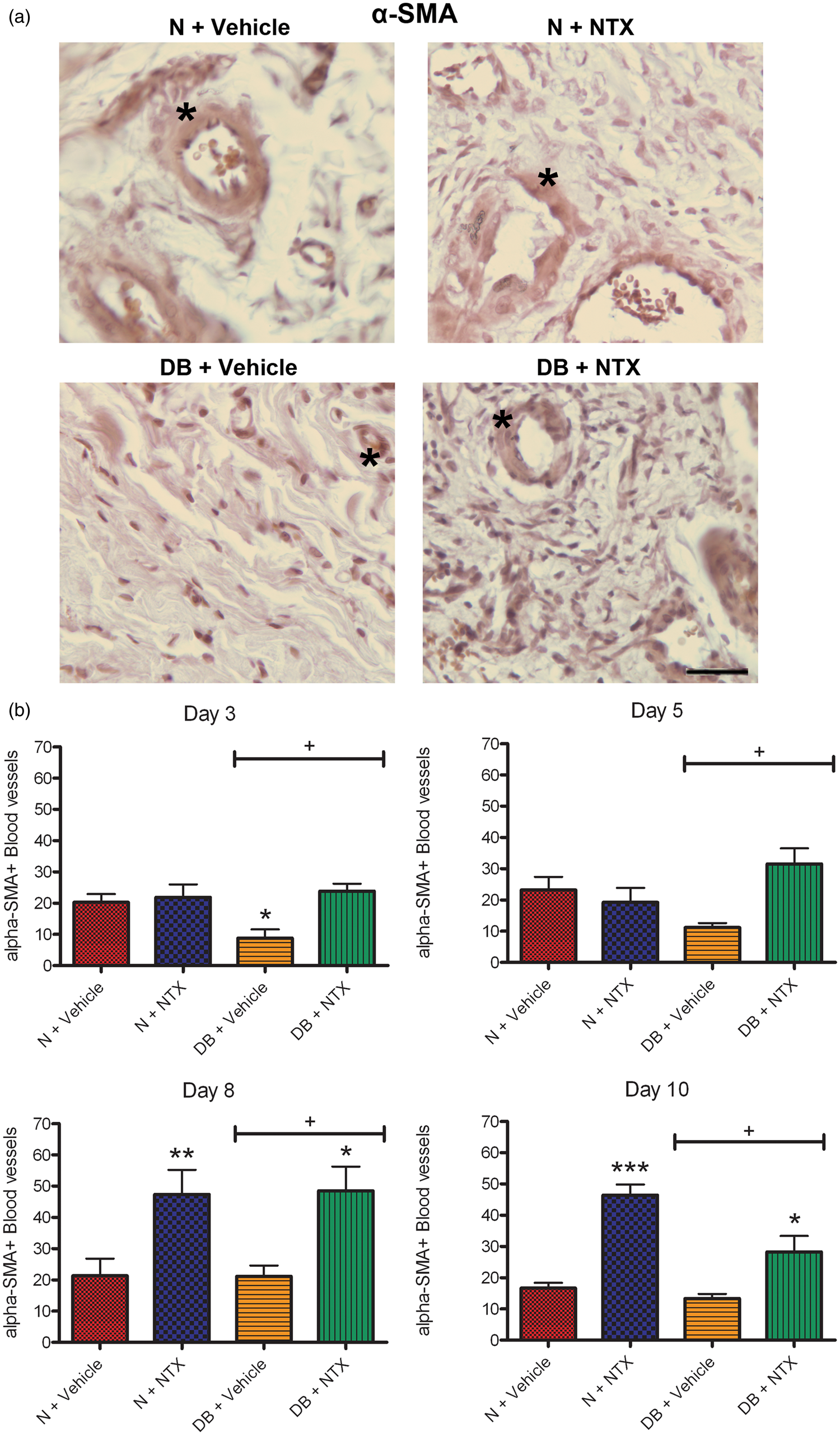
Discussion
Wound healing occurs more slowly under diabetic conditions in both humans and animal models relative to normal conditions,21–25 and thus provides an opportunity for infection or other complications to ensue. In this report, we have evaluated for the first time several of the cellular mechanisms associated with wound closure, and highlighted some of the underlying pathophysiology associated with the delays recorded in full-thickness wounds in T1D rats. In previous studies, we reported delayed re-epithelialization and documented that the delays were related to changes in DNA synthesis rates in basal epithelial cell layers. 1 However, the initial phase of wound closure is the inflammatory phase which begins immediately after injury. 18 The response involves infiltration of neutrophils and mast cells into the wound site in order to release cytokines and histamines to elicit inflammation and swelling. Diabetic rats were found to have fewer mast cells infiltrating the granulation tissue associated with the wound relative to the number observed in normal rat tissues. The delays in mast cell infiltration were observed at three, five, and eight days; by 10 days, diabetic tissue had the level of mast cells seen on day 3 in normal specimens. Thus, despite having comparable levels of mast cells prior to the injury, diabetic animals have a delayed inflammatory response to injury.
Angiogenesis is a major part of the proliferation phase of wound closure and involves the formation of new blood vessels in order to stimulate granulation tissue and remodelling. Three markers for blood vessel formation that include new endothelial cells and smooth muscle cells can be detected by FGF-2 and VEGF staining (endothelial cells), as well as α-SMA (smooth muscle cells) staining. FGF-2 staining was decreased in diabetic tissues on day 3, but by days 8 and 10, the number of FGF-2 stained cells in blood vessels was comparable to normal on day 3. The lack of FGF-2 staining suggested a delayed initiation of blood vessel formation. The expression of VEGF and α-SMA stained cells also were delayed in appearance and reduced in magnitude in surgically wounded diabetic tissues over the course of the 10-day observation period. However, evaluation of tissues from diabetic rats 15 and 20 days following surgery indicated that the number of mast cells and the number of blood vessels with FGF-2, VEGF, and α-SMA staining returned to levels comparable to normal controls. These results suggest that while there are initial delays in cell proliferation following wounding in the diabetic rats, there appears to be an eventual compensation. Whether the delayed time table for angiogenesis and inflammatory responsiveness invokes other complications or weakens the integrity of the wound healing processes is not known, but our preliminary data on tensile strength suggest that NTX reinforces the skin in diabetic rats.
Topical treatment of full-thickness wounds with NTX appears to enhance cell proliferative events on a number of levels. In addition, to enhancing re-epithelialization and accelerating residual wound closure in diabetic rats, topical application of NTX increased mast cell number at five and eight days, and the number of FGF-2 positive blood vessels at three and five days, in diabetic rats. VEGF positive blood vessels were increased by NTX treatment at three, five, and eight days in diabetic rats, while α-SMA staining was increased at all time points examined in diabetic rats treated with NTX, demonstrating that blockade of the endogenous opioids inhibiting DNA synthesis can be reversed. Receptor blockade by NTX thus targets a biological pathway underlying the delayed repair processes in diabetics and can be stimulated to enhance wound repair. Data analyses revealed significant interactions between treatment and condition at most time points for the number of positive α-smooth muscle cells and FGF-2 stained vessels suggesting that NTX treatment upregulated proliferation of these cells to a greater extent than altered under normal conditions.
A third comparison was made between normal animals receiving NTX and those receiving only vehicle. NTX also stimulated wound closure in normal rats, but that there were minimal effects on mast cell proliferation. Application of NTX to the wounds of normal rats did result in an increased number of VEGF-positive blood vessels at three and five days, and α-SMA-positive blood vessels on days 8 and 10.
In general, T1D appears to retard early processes of wound closure that involve cell proliferation. This may well be a result of the increased OGF levels associated with the disease.6–8 Furthermore, there are temporal delays in expression of markers for angiogenesis in the diabetic rat which again suggests delayed proliferation. Our data suggest that full-thickness wound closure could be delayed as much as 48 h in diabetic rats compared to normal rates. The processes of wound closure that involved proliferative events were stimulated by NTX treatment, and diabetic rats receiving topical NTX had wound closure rates that were comparable to normal within four days of treatment. Likewise, new blood vessel formation was increased in NTX-treated diabetic tissues compared to diabetic rats receiving vehicle treatment. The present study confirms and extends earlier research 1 that identified the optimal method of delivery for topical NTX. In that study, NTX in concentrations ranging from 1 to 100 µmol/L was dissolved in a variety of potential delivery agents, and moisturizing cream was found to be optimal. NTX at a dosage of 10−5 mol/L was effective at enhancing wound closure when applied once a day or three times daily, and increased DNA synthesis in the epidermis of rat skin. The present study has now shown that topical NTX stimulates blood vessel formation by stimulating proliferation of endothelial and smooth muscle cells.
Impaired wound healing is a well-known complication of diabetes.21–25 A number of topical treatments have been devised that enhance wound closure in both type 121,25 and type 222,24 diabetic mice and rats including the addition of platelet-derived growth factor, 21 human platelet preparations, 22 and endothelial cell progenitor transplantation 24 onto excisional wounds. Other studies have shown that elevated toll-like receptor-2 25 or an estrogen deficiency 23 plays a role in the increased inflammation, delayed angiogenesis, and/or decreased cell proliferation that accompanies the complications of delayed wound closure in diabetes. Many of the studies examine simple closure of wounds either by contraction or re-epithelialization and limit their morphological observations to the first week following surgical wounding. These studies support that there are biological events underlying the delayed healing processes, and that a multifactorial approach to acceleration of healing is needed.
Given the knowledge that diabetic animals have heightened levels of enkephalins, one of which is known to be inhibitory for cell proliferation, the use of NTX to block the biological pathway used by [Met 5 ]-enkephalin (OGF) and its receptor OGFr, provides a novel therapeutic approach that targets the pathophysiological defect in diabetes.
Footnotes
Author contributions
All authors participated in the design, data analyses, and review of the manuscript. JAI performed much of the research. ISZ and PJM interpreted the data and wrote the manuscript.
Acknowledgements
This research was supported by a grant from the American Diabetes Association (PJM).