
Abstract
Increasing body mass indices (BMIs) across the globe reflect pandemic shifts towards habitual positive energy imbalances. Excess body fat in individuals is often associated with high-energy and high-fat diets scanty in fresh produce. Carotenoids are fat-soluble pigments plentiful in many fruits and vegetables. They are well-known for provitamin A and antioxidant functions, but little research has been done related to carotenoid-body mass interactions. Serum carotenoids were analyzed relative to body fat to determine correlations between major serum carotenoids, retinol, BMI, fat mass, and lean mass. Healthy women (n = 76), 19–50 years old, were categorized into two comparison groups determined by percent body fat measured by air displacement plethysomography (BOD POD®), i.e. <31% and ≥31% fat mass. Anthropometric and three-day diet records were completed for BMI and nutrient intake calculations, respectively. Serum α-carotene concentrations were strongly inversely associated with all measures of body composition (P < 0.001 α-carotene) controlling for dietary intake and age, while β-carotene, lutein, and lycopene were not (P > 0.05). Dietary intake between groups did not differ, including carrot consumption (a high dietary source of α-carotene). These results confirm previous carotenoid-health research and propose the need for further investigation of potential protective roles that α-carotene may perform for optimal health. Serum α-carotene may provide a deeper and clinically relevant purpose, beyond previous suggestions for its use as a biomarker for fruit and vegetable consumption, in that α-carotene may be a biomarker for chronic disease risk frequently linked with obesity.
Impact statement
Carotenoids are important pigments in fruit and vegetables and found in human serum. This study isolated a negative relationship between serum α-carotene and body fatness. As humans begin to live over a century, determining biomarkers of ultimate health is important. α-Carotene does not have the same distribution in the food supply as β-carotene and therefore is often overlooked in surveys. In part, this is due to the fact that β-carotene provides two molecules of vitamin A, while α-carotene provides one upon central cleavage. This study shows a very clear association between α-carotene and body fatness, which appears to go beyond its fat-soluble nature. Dietary intake data were not able to explain the association. Further work is needed to determine what dietary components infer health benefits.
Introduction
Obesity has earned the reputation as a global health pandemic leading to the escalation of non-communicable diseases along with coincident under- and over-nutrition occurring in the same households. 1 Body fat is commonly estimated by calculating an individual’s body mass index (BMI), which is highly correlated with actual body fat across both genders from childhood through adulthood.2,3 Current guidelines from the US Center for Disease Control and Prevention and the World Health Organization define the normal BMI range as 18.5–24.9, overweight as BMI ≥25–30, and obese as BMI ≥30 kg/m2. Excess body fat, estimated at BMI ≥25 for most adults, has been associated with increased morbidity and mortality. 4
Clinicians classify the constellation of pathologies associated with excess fat mass as “metabolic syndrome,” characterized by having three or more abnormal measurements of central adiposity, glucose regulation, insulin sensitivity, blood lipids, and blood pressure. 5 People with metabolic syndrome are estimated to have twice the risk for cardiovascular disease (CVD) and over five-times the risk for type 2 diabetes. Indeed, diabetes and obesity are so frequently associated that the condition is sometimes referred to as “diabesity”. 6 With nearly a quarter of all adults in the US diagnosed as having metabolic syndrome, and over 40% of these over the age of 50 years, 7 unambiguous motivation exists to understand the underlying pathophysiologic processes related to these poor health outcomes.
Beyond adipose tissue’s role as a storage site for triglyceride and lipophilic components, it is involved in metabolic homeostasis by secreting adipocytokines, such as leptin and interleukin-2. Adipose is associated with increased inflammation, which plays a role in endothelial dysfunction, hypertension, and atherogenesis. 8 Oxidative stress, caused from an imbalance in pro- and antioxidants, occurs more often in individuals with metabolic syndrome 9 and is likely a key player in the onset of diabetes and CVD. 10 Dietary carotenoids may play a protective role against the onset of many chronic diseases, including atherosclerosis,11,12 stroke, 13 hypertension, 14 inflammatory diseases, 15 diabetic retinopathy, 16 cancer, 17 and all-cause mortality. 18 Inverse associations exist between many serum carotenoid concentrations with body fat19–24 and metabolic syndrome.21,25,26 Low serum carotenoid concentrations may not indicate a causal link to disease but a relative absence of other protective dietary factors, such as fiber, minerals, or other antioxidants and phytochemicals found in fruits and vegetables. This has been demonstrated by three clinically controlled trials in which β-carotene supplementation failed to produce protective effects.27–29
Carotenoids are lipophilic compounds found primarily in colorful plant tissues. While α-carotene, β-carotene, and β-cryptoxanthin are retinol precursors, others, such as lycopene, are potent antioxidants. 30 Serum carotenoids are sensitive indicators of dietary fruit and vegetable intake in healthy non-obese subjects,31,32 but may be independent of dietary intake in obese individuals.19,20,23 Fruits and vegetables contain complex combinations of nutrients and carotenoids; therefore, specific foods have been proposed to be more protective against chronic disease than others. For example, Boggs et al. 33 found an inverse relationship between breast cancer and carrot consumption, but overall fruit and vegetable intakes were not associated. Li et al. 34 concluded that serum α-carotene concentrations were inversely associated with mortality risk from CVD, cancer, and all other causes, asserting that high fruit and vegetable intakes may prevent premature death.
Understanding the underlying metabolic processes associated with obesity are of paramount importance. The aim of this analysis was to further explore the relationship between common dietary carotenoids and body fat. The associations between serum and dietary α-carotene, β-carotene, lutein, and lycopene, and vitamin A (retinol) with actual measures of body fat composition were examined in healthy adult women living in Wisconsin, USA.
Subjects and methods
Subjects
Characteristics and serum concentrations of subjects included in this comparison characterized as fat mass <31% (lean) or ≥31% (overweight)
ND: not determined.
Values expressed as means ± SD (ranges). All characteristics of lean and overweight subjects are significantly different (P value ≤ 0.002), except for serum β-carotene (P value = 0.38), lutein (P value = 0.18), and lycopene (P value = 0.90).
Body composition and serum analyses
Percent fat mass (%FM), percent lean mass (%LM), total fat mass (TFM), and total lean mass (TLM) were measured using air displacement plethysomography (BOD POD®, Life Measurements, Inc., Concord, CA) by standardized procedures.
37
Height was measured using a wall-mounted stadiometer and body weight was measured using the same BOD POD® scale in both studies, which was calibrated daily. Subjects for this analysis were first categorized into “Lean” and “Overweight” groups based on BMI cutoff criteria for normal weight and overweight status.
38
The Lean group (n = 34) included women with BMIs ranging from 18.5 to 24.9 kg/m2 and the Overweight group included women with BMIs >28 kg/m2 (n = 42). Although BMI is highly correlated with actual body fat, it can be an inaccurate measure of actual body fat of an individual.
38
In this study, four women had %FM >31 with normal BMI and two women had %FM <31 with an overweight BMI (Figure 1(a)). For this reason, we ultimately used %FM as the group-defining criteria. This provided for a Lean group (n = 29) with <31 FM% and an Overweight group (n = 47) with ≥31.0 FM%.
(a) Estimated versus actual body fat. According to BMI classifications, the majority (80%) of women in the Overweight group are classified as “obese”. No women were “underweight” with a BMI < 18.5. Six subjects had incompatible measures of estimated and actual measures of body fat: n = 4 subjects had excess actual body fat (%FM ≥ 31%) and normal estimated body fat (BMI < 25.0), and n = 2 subjects had normal actual body fat (%FM < 31%) and excess estimated body fat (25.0 ≤ BMI < 30.0). This illustrates how diverse female body composition can be at the individual level, and how valuable it can be to validate BMI in research subjects by measuring actual body fat. (b) Correlation between %FM and BMI. There was a relatively strong linear relationship between %FM and BMI (R2 = 0.85) for this group of adult women, confirming previous studies validating BMI is an estimator of body fat at the population level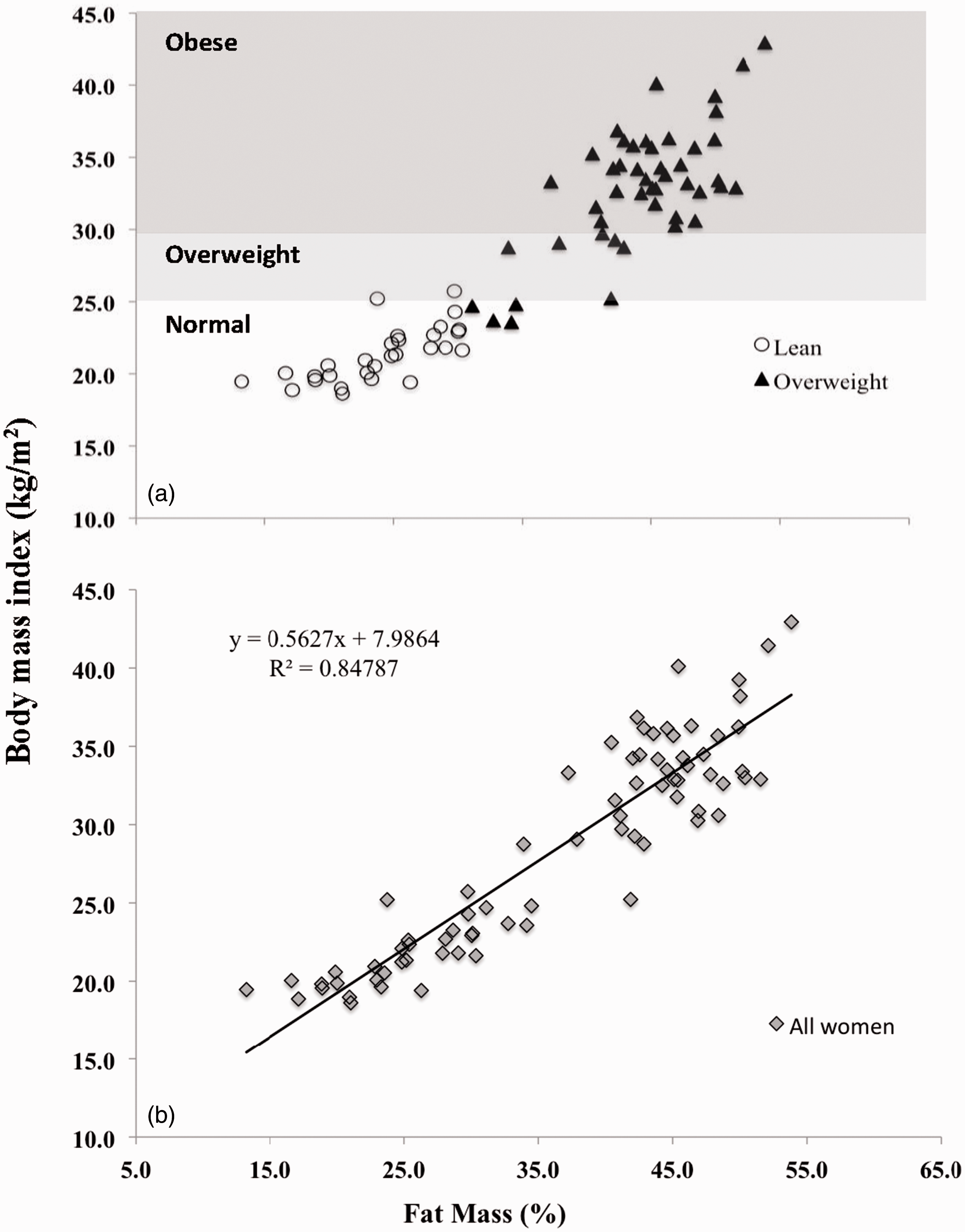
Blood samples for all subjects were taken in fasted conditions (at least 8 h). Serum carotenoids and retinol were analyzed as previously published by the same person (ARV) using the detailed protocol. 39 Retinol-binding protein 4 (RBP4) was also measured for overweight women using ELISA. 40
Dietary intake
Dietary intake information was collected using three-day diet records (2 weekdays and 1 weekend day) upon enrollment. These were analyzed for carotenoids (α-carotene, β-carotene, lutein, and lycopene) and vitamin A (retinol activity equivalents) using Nutritionist Pro version 3.1.0 (Axxya Systems; Stafford, TX, 2007). Mean daily total fruit, vegetable (with and without fried potato products), and carrot intakes were calculated for both Lean and Overweight groups. Carrot intake was specifically targeted due to its high α-carotene concentration.
Statistical analyses
Values are expressed as means ± SD and significance was determined by two-sided Students’ unpaired t tests. The linear relationships between body composition measures, such as BMI, %FM, %LM, TFM, TLM, and plasma carotenoid concentrations, were examined by calculating and testing Pearson correlation coefficients (r). Multiple linear regression using the MIXED procedure was performed to adjust other factors. All analyses were performed using SAS (version 9.1.3, SAS Institute, Inc., Cary, NC, 2001). Statistical significance was set at α = 0.05 for all analyses. Potential outliers (i.e. obese and >45 years old) were omitted to see if significance changed.
Results
By design, subject body composition measures were significantly different between the Lean and Overweight groups. Subject age also differed; lean subjects were almost a decade younger than overweight subjects (Table 1). The vast majority, nearly 80%, of subjects in the Overweight group had a BMI that exceeded 30 kg/m2, qualifying them as obese. Results for all measures were repeated after omitting obese women >45 years old (n = 3), but there were no shifts in statistical significance; therefore, all subjects remained in the analysis. Figure 1(a) and (b) demonstrates the relationships between BMI and %FM of all subjects, as well as disagreements between categories of BMI and %FM for six women.
Correlation coefficients (r) between body composition and serum carotenoid concentrations across all women. a

BMI: body mass index.
Pearson correlation coefficients.
0.08 < P < 0.09 (trend).
P < 0.005 (significant).
P < 0.0005 (highly significant).
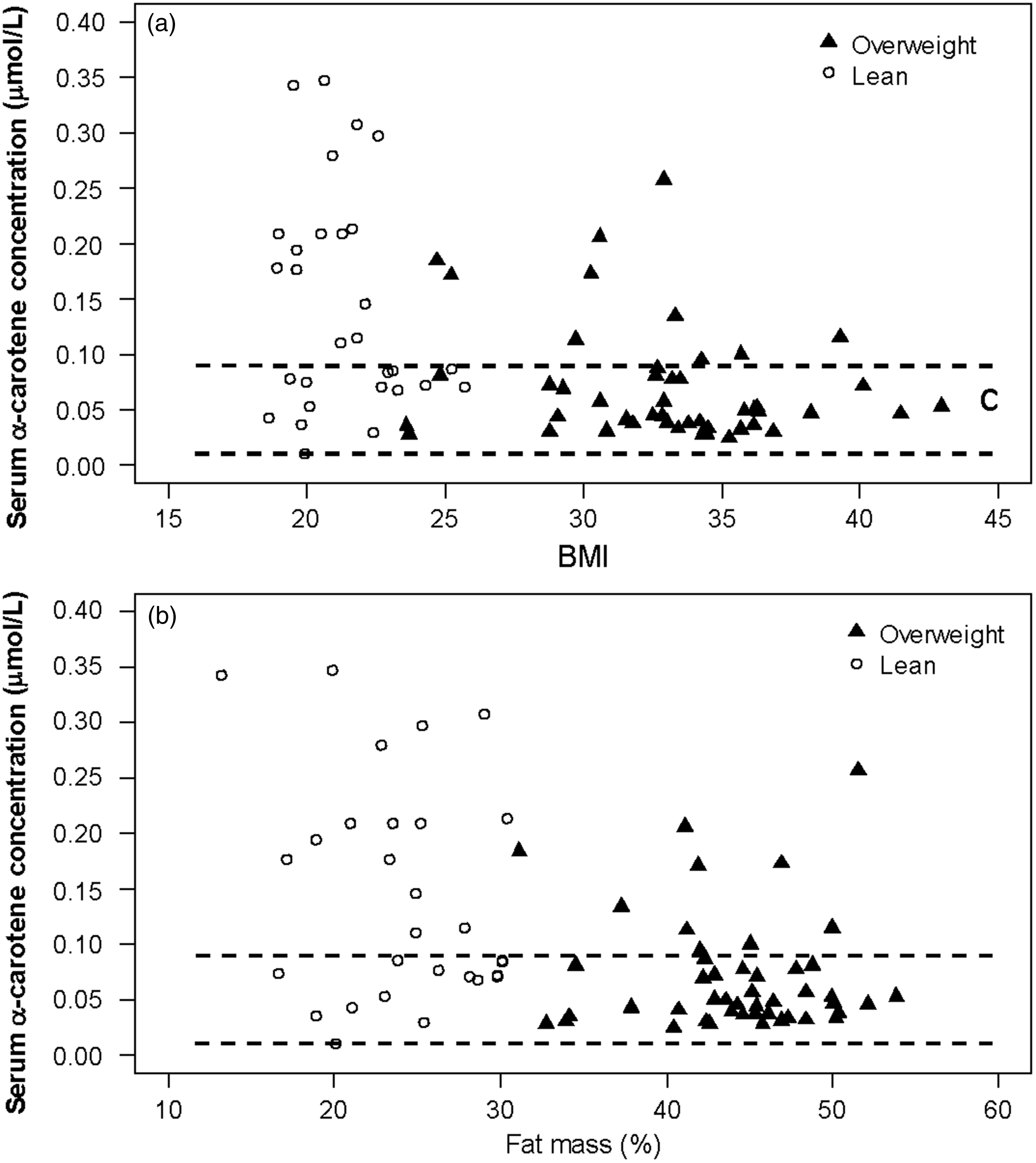
Serum α-carotene concentration was significantly higher in lean individuals than that in obese individuals, 0.14 ± 0.10 µmol/L vs. 0.07 ± 0.05 µmol/L, P = 0.0007. Dotted lines specify serum concentrations at which suggest statistical protection against (>0.09 µmol/L) or high-risk for (<0.01 µmol/L) chronic diseases suggested by Li et al. 34 Subjects with concentrations below 0.01 µmol/L may be at an increased risk for chronic diseases. Using these cutoffs, no women in this analysis may be considered as high-risk for chronic diseases, but the Overweight group had a higher prevalence below the cutoff for protection (P = 0.0061). (a) Scatter plot of individual subjects illustrates significant associations between serum α-carotene concentration and BMI (P < 0.001). But there was no significant interaction of %FM and group (P = 0.38) as well as group effect (P = 0.29). (b) The significant association between serum α-carotene concentration and %FM was also observed (P < 0.001). No significant interaction of %FM and (P = 0.16) and group effect (P = 0.065) were observed
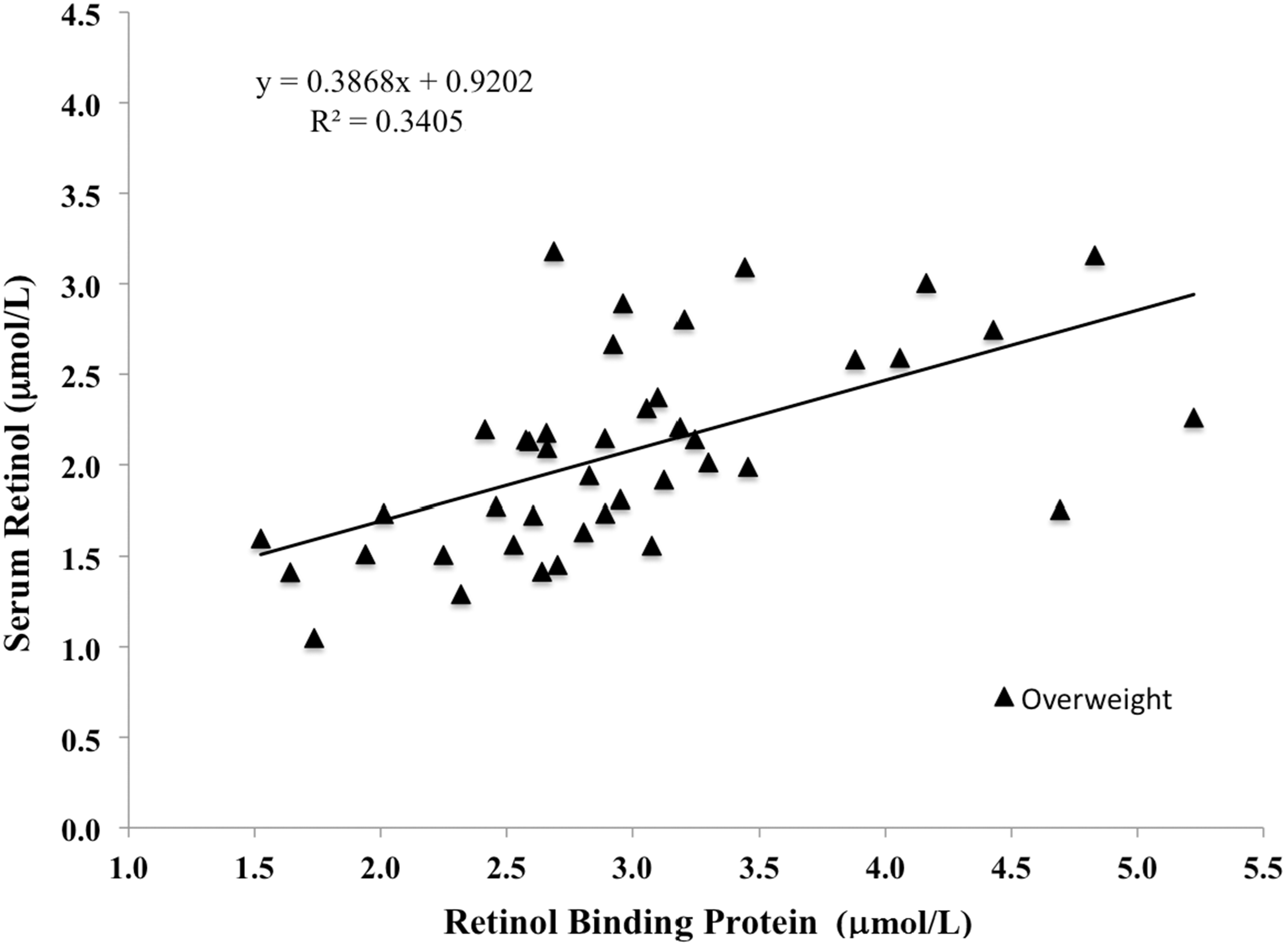
The mean serum RBP4 concentration in overweight subjects was 2.99 ± 0.82 µmol/L and mean serum retinol concentration was 2.12 ± 0.54 µmol/L indicating 71% saturation. Serum RBP4 concentration increased proportionally to serum retinol in overweight and obese women. Serum retinol’s association with measures of body composition were weakened by controlling for dietary retinol and age
Mean daily fruit and vegetable intakes in lean (<31% FM) and overweight (≥31% FM) women determined from 3-d diet records
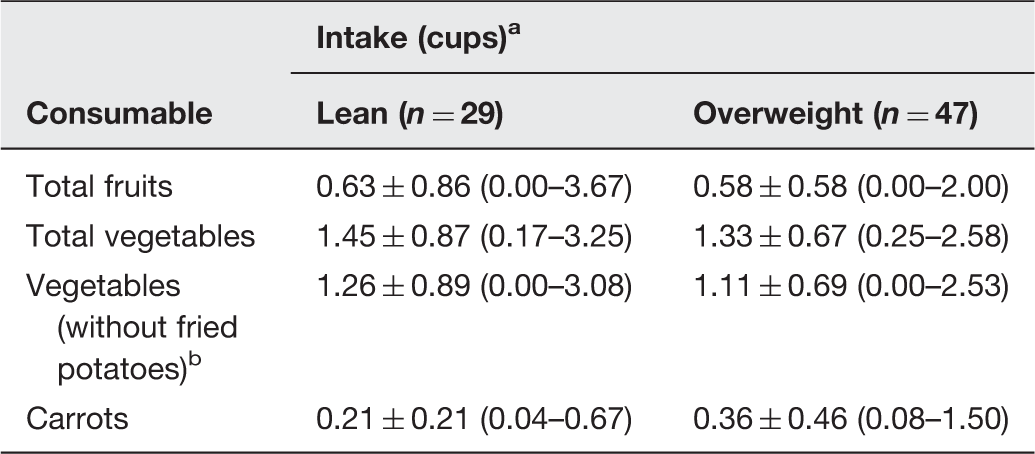
Values expressed as means ± SD (ranges). All intakes between lean and overweight subjects are not different (P ≥ 0.43).
Fried potatoes include hash browns, crisps, chips, and fries.
Discussion
Serum concentrations of α-carotene were negatively associated with body fat in women. α-Carotene may be indirectly related to body fat, or a marker of fat mass, because a strong association was maintained after controlling for dietary α-carotene intake and age. Lycopene, lutein, and β-carotene were not significantly associated with any indicator of body composition in these women. The results related to β-carotene and lutein do not reflect prior research.19,20,22,24–26 In men, serum β-carotene was not significantly associated with central adiposity after adjustment for body fat 23 suggesting that site-specific adiposity deposition could be affecting β-carotene serum concentrations in women.
Our results illustrate a possible metabolic shift in the way α-carotene is utilized and mobilized with excess body fat. The lower serum concentrations of α-carotene during the obese state may reflect the fact that adipose tissue is a storage depot for α-carotene or there is a functional role that remains unrecognized. α-Carotene may be the preferred carotenoid pulled out of circulation into adipose tissue for storage, or it is metabolically active (as a carotenoid or cleaved retinoid product) leading to decreased serum levels. Previous research has shown similar inverse relationships between BMI and carotenoid concentrations suggesting that carotenoids may be sequestered in specific tissues in the body. 42 In obese individuals, enlarged fat mass may act as reservoirs for incoming (newly eaten) carotenoids leading to fewer total carotenoids in the serum. 23 A small controlled study 43 suggested that lean body mass might also serve as a dynamic reservoir that actively takes up carotenoids from plasma, but does not explain the positive relationship between %LM and carotenoids in this study. These data suggest that the inverse relationship between body fat and serum carotenoids is primarily due to sequestering in adipose tissue.
Serum retinol concentrations may also be influenced by fat mass indirectly, seen by a weakened association after controlling for dietary intakes and age, although RBP4 has shown opposite associations. 40 RBP4 has been referred to as an adipokine that is positively associated with BMI. 44 RBP4 analysis of overweight women confirms prior research that serum RBP4 is higher relative to “normal” levels in lean adults. 44 Relatively high serum RBP4 in overweight subjects despite lower retinol levels suggests that some of the serum RBP4 in overweight individuals may be functioning unbound to retinol. Elevated RBP4 with excess body fat has been associated with insulin resistance mediated through suppressed GLUT4 transporter expression. 45 Insulin resistance is one characteristic of type 2 diabetes commonly associated with excess body fat, illustrating how nutrient utilization can be modified by health.
Studies that directly targeted carotenoid and retinol accumulation in human adipose tissue have been predominantly sourced from biopsies, breast reconstruction surgery tissue, and autopsies. 46 Adipose tissue is likely a major storage compartment for α-carotene. Relative serum carotenoid-to-adipose tissue concentrations appear to be highly variable among individuals, but long-term adequate carotenoid consumption would result in lower ratios between serum and adipose. Moreover, specific foods may significantly increase serum carotenoid levels without affecting adipose stores, such as β-carotene from lettuce, while others may have no effect on serum concentrations while increasing adipose storage, such as α-carotene from carrots. 47 Site-specific adipose tissue deposition may also influence carotenoid accumulation. For example, most carotenoids including α-carotene, are sequestered at significantly higher levels in abdominal fat than buttocks fat, and buttocks fat has higher levels of α-carotene and β-carotene than inner thigh fat, 48 suggesting abdominal fat may impact overall carotenoid status. Similarly, waist circumference has been suggested as an independent predictor of fat α-carotene in both men and women, whereas BMI was a predictor of β-carotene, and smoking a predictor of retinol in women from nine European and Middle East countries. 49
Uncharted roles of α-carotene may explain its highly significant associations with excess body fat that were unparalleled by other serum carotenoids in this study. Perhaps α-carotene’s functions in health only become apparent under systemic stress related to obesity. Potential and poorly researched possibilities may be that α-carotene is the preferred provitamin A carotenoid for cleavage into active vitamin A when it is in circulation. Chai et al. 19 showed that serum provitamin A carotenoids decreased almost three-fold relative to non-provitamin A carotenoids in obese women versus lean women. However, β-carotene was not lower in the obese state in our study. Perhaps this points towards the other half of the cleaved molecule, α-retinol, as the active product with retinoid-functioning at the DNA level.
A second possibility for α-carotene includes its preferred use as an antioxidant in obesity-induced oxidative stress. Serum carotenoid concentrations were indeed lower in Japanese smokers with metabolic syndrome relative to non-smokers 21 potentially demonstrating antioxidant activities under fat-induced oxidative stress. Serum carotenoids are also associated with underlying markers of obesity, such as γ-glutamyl transferase (GGT), indicated by a previous positive association between BMI and GGT 50 and an inverse association between GGT and serum carotenoids. 50 These findings propose that inflammation and stress associated with excess body fat may enhance the metabolism of α-carotene; however, this same trend was not observed with other carotenoids measured.
Thirdly, few foods are naturally rich in α-carotene, such as carrots (∼35 µg/g raw). The link between serum α-carotene and body composition may partially reflect higher consumption of fruits and vegetables, such as carrots. In this analysis, only one-fifth of subjects consumed carrots regardless of treatment group. Furthermore, fruit and vegetable consumption was equal between lean and overweight subjects, as well as low relative to established diet recommendations. 41 Thus it is unlikely that lean subjects had higher serum α-carotene due to diet alone suggesting underlying metabolic changes in carotenoid handling with obesity.
This study is limited in that it was a cross-sectional evaluation of premenopausal women in the Midwest; therefore, the results are not generalizable to other populations without further research. While seasonality can affect carotenoid concentrations in the body, this is usually more apparent in countries with greater access to specific fruits or vegetables at certain times of the year, such as mango season in tropical countries. 51 Nonetheless, most of the recruitment for the Lean group was in March and April (spring), which is in contrast to the Overweight group recruited in June through August (summer). Therefore, seasonality does not explain these differences because in the Midwest more produce would be available in summer versus spring season. Future investigation of the α-carotene-to-body composition relationship should include not only collecting data from subjects of various backgrounds, activity levels, and lifestyle choices, but also focus on dietary intakes of specific carotenoid-rich foods. Perhaps low α-carotene concentrations in overweight/obese individuals can be increased in those who begin eating foods rich in α-carotene. Longitudinal feeding interventions related to α-carotene containing foods may be of exceptional interest for understanding α-carotene’s role in disease incidence in people with and without excess body fat. Of note, the serum α-carotene concentration of the Lean group was similar to that of Midwestern women (0.15 ± 0.06 µmol/L) who lived to be ∼100 years old. 52 Indeed, higher serum carotenoids, including α-carotene, were also associated with lower risk of metabolic syndrome in Chinese adults 50–75 years old. 53
Conclusion
This cross-sectional analysis showed associations between serum carotenoids and retinol with various measures of body fat but did not reveal mechanisms. However, it is clear that body composition influences serum nutrient profiles. Body fat was correlated with lower retinol and drastically lowers α-carotene concentrations in the serum of young to middle-aged women. Underlying metabolic parameters related to high body-fat mass, such as oxidative stress and inflammation, may influence such changes in nutrient levels. While high fruit and vegetable consumption remains of paramount importance for achieving optimal health as previous research shows, this analysis suggests that perhaps particular foods, such as α-carotene-rich carrots, may decrease risk of chronic disease associated with weight gain more effectively than others. In summary, dietary carotenoids may contribute to overall human health; however, serum α-carotene may be an early serum biomarker for chronic disease risk independent of, but commonly associated with overweight and obesity. There are many pieces to the carotenoid-and-health puzzle and α-carotene may be a uniquely functioning, clinically relevant carotenoid that has been hiding in β-carotene’s shadow for the past few decades of vitamin A research.
Footnotes
Authors' contributions
ETN compiled the data, wrote the first draft of the manuscript, and worked with the lead statistician (ZZ). ARV oversaw the human studies and performed the carotenoid analyses. ZZ and HJL were responsible for statistical evaluation. SAT revised the manuscript. All authors participated in the interpretation of data.
Acknowledgment
This work was funded by the National Research Initiative of the USDA Cooperative State Research, Education and Extension Service, grant number 2003-35200-05377 and NIHNIDDK 61973.
Declaration of Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.