
Abstract
The current study aimed to investigate the relations of three single nucleotide polymorphisms of matrix metalloproteinase-9 gene, and single nucleotide polymorphisms-smoking interaction to subarachnoid hemorrhage risk. The optimal pattern of the interaction among single nucleotide polymorphisms and smoking was selected by generalized multifactor dimensionality reduction. The association between the three single nucleotide polymorphisms within the matrix metalloproteinase-9 gene was analyzed by logistic regression test. As well as genetic risk of subarachnoid hemorrhage interactions with smoking, the risk of subarachnoid hemorrhage in carriers with the rs3918242 (T) was significantly higher than in carriers carrying CC (genotype: CT + TT vs. CC), adjusted OR (95% CI) = 1.58 (1.25–2.03), and in carriers carrying rs17576- (genotype: AG + GG vs. AA), adjust OR (95% CI) = 1.62 (1.19–2.13). However, after adjusting for covariates, we did not find any direct association between rs17577 and subarachnoid hemorrhage risk. The generalized multifactor dimensionality reduction model shows a potential relation between rs3918242 and smoking risk for subarachnoid hemorrhage (P = 0.0010). After covariates adjustment, current smokers with rs3918242-CT or TT genotype, compared to never-smokers with rs3918242-CC genotype, OR (95% CI) = 2.57 (1.74–3.46), have a higher subarachnoid hemorrhage risk. Our study showed that the rs3918242 (T) and rs17576 (G), the cross reaction between rs3918242 and smoking increased the risk of subarachnoid hemorrhage.
Impact statement
Matrix metalloproteinase-9 (MMP-9) is a possible candidate gene for some diseases, including metabolic syndrome, stroke, coronary artery disease (CAD). But to date, limited data focused on the relationship between MMP-9 gene SNPs and SAH susceptibility. The purpose of this study was to evaluate SNPs of MMP-9 gene and their interaction with environmental factors with SAH risk based on a Chinese population.
Keywords
Introduction
Subarachnoid hemorrhage (SAH) was a severe stroke, accounting for 1–7% of all stroke cases. 1 Although SAH is relatively rare, has a great impact on health.2,3 Many risk factors for SAH have been evaluated, including old age, female, hypertension, and tobacco.4,5 The etiology of SAH includes both environmental and genetic risk factors.6–8
Matrix metalloproteinases (MMPs) were zinc-dependent endopeptidases. Its biological effects include involvement in the remodeling and degradation of extracellular matrix (ECM). 9 MMPs are secreted mainly by astrocytes, endothelial cells, microglia, and neurons. The gene family has more than 20 members, and it has been shown a relationship of increased MMP activity and progression of aortic diseases. 10 Matrix metalloproteinase-9 (MMP-9) was an important and candidate gene for some diseases, including metabolic syndrome (MetS), 11 stroke, 12 coronary artery disease (CAD). 13 But to date, limited data focused on the relationship between MMP-9 single nucleotide polymorphisms (SNPs) and SAH susceptibility. The objective of current study was to evaluate relations of MMP-9 SNPs, and their interaction with environmental factors to SAH risk based on Chinese population.
Materials and methods
Subjects
All study subjects were selected from June 2010 to March 2016 at the Affiliated Hongqi Hospital of Mudanjiang Medical University. The patients with SAH were diagnosed by at least two experienced doctor. The diagnosis of aneurysmal SAH was based on subarachnoid blood CT and conventional angiography. Four patients with myocardial ischemia or cerebral infarction history were excluded from analysis. The control groups were randomly selected from those persons who received physical examination in our hospital. Based on age and gender, nearly 1:2 patients were matched cases. Both the SAH cases and the control group had nothing to do with the Han Chinese population. Demographic information, clinical, and biochemical indicator data were obtained through a questionnaire survey.
Participants measured body weight and height. The current smokers were those who self-report smoking at least once daily for > 1 year.
The amount of alcohol consumed is expressed as the sum of wine, beer, and spirits per week in mL. Blood samples, after fasting for at least 8 h were collected. All participants got informed consent. For this study, diagnostic criteria for T2DM include fasting blood glucose ≥126 mg/dL (7.0 mmol/L) or, during this time, the initiation of hypoglycemic therapy (oral medication or insulin). Hypertension was defined as: diastolic blood pressure (DBP) not less than 90 mmHg or systolic blood pressure (SBP) not less than 140 mmHg and/or subjects taking antihypertensive drugs.
Genomic DNA extraction and genotyping
Three SNPs of the MMP-9 gene, including the SNPs associated with SAH, IS, and Mts, were selected for investigation, but these associations have not been well documented in the Chinese population and a uniform conclusion has not yet been reached. According to the DNA Blood Mini Kit instructions (Qiagen, Hilden, Germany), participants' gDNA was obtained from EDTA-treated whole blood. All three SNPs were genotyped by PCR-RELP using 200 ng/2 µl of DNA template (Table 1). The genotyping for three SNPs was carried out according to previous studies. 14 The blind DNA duplicates were used to control the quality of genotyping for random samples. Twenty samples were also randomly chosen for each genotype and the amplicons were sequenced in CEQ, 8000 System (Beckman Coulter, England); 100% consistency was observed between genotyping assays.
Description and probe sequence for three SNPs used for PCR analysis.

SNPs; single nucleotide polymorphisms; PCR: polymerase chain reaction.
Statistical analysis
SPSS version 22.0 (SPSS, Inc., Chicago, IL, USA) was used for data analysis. Continuous variables of the experimental data are expressed as mean ± standard deviation (SD); the categorical variables are expressed in absolute values and percentages. Continuous variables were compared by t test; categorical variables were analyzed by Chi-square test. SNPstats (http://bioinfo.iconcologia.net/SNPstats) was used for Hardy–Weinberg equilibrium (HWE) test. Among SNPs and smoking, the best combination of interaction was determined by generalized multifactor dimensionality reduction (GMDR). Logit model was performed to assess the relationship between three SNPs within MMP-9 gene, and the additional stratified analysis of risk of SAH by gene-smoking interactions. Two-tailed test with P < 0.05 indicated statistically significant.
Results
A total of 1383 participants (855 men, 528 women) were investigated, including 460 patients with SAH and 923 control participants. Their average age was 62.8 ± 14.3 years. Table 2 shows the general characteristics of the case group and the control group. The average age and distribution of sex and alcohol drinkers did not differ significantly between cases and controls, but the proportions of BMI and smokers, T2DM and high blood pressure were higher than those of controls.
General characteristics for all study participants in SAH cases and controls.
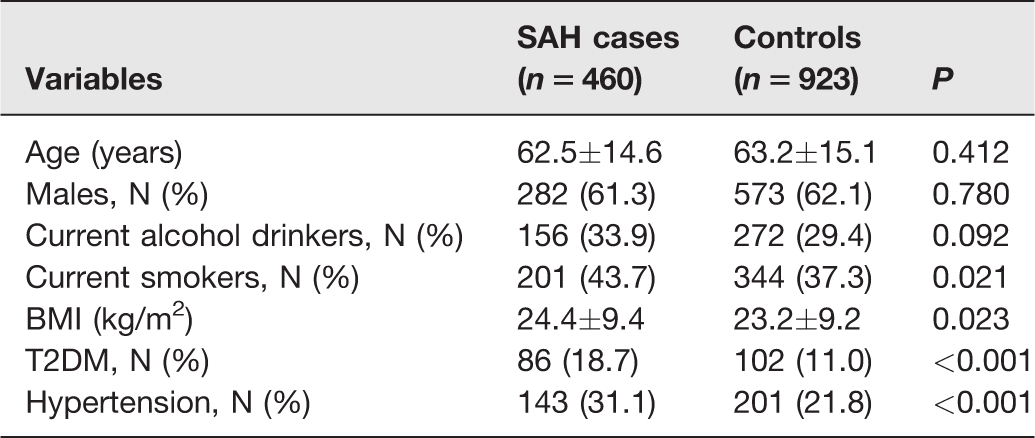
BMI: body mass index; T2DM: type 2 diabetes mellitus; N: number; SAH: subarachnoid hemorrhage.
HWE genotype frequencies were tested, and no significant differences were observed for any tested SNPs in the controls. In SAH cases, the frequencies for the rs3918242-T allele and rs17576-G allele were significantly higher than in controls (29.0% vs. 19.5%, 31.4% vs. 20.4%). The risk of SAH analyzed by logistic regression was significantly higher in the rs3918242-T carriers than those in CC carriers, adjusted OR (95%CI) =1.58 (1.25–2.03). The risk of SAH in rs17576-G carriers was higher than those in AA carriers, adjusted OR (95% CI) = 1.62 (1.19–2.13). The SNP-rs17577 is not related to covariate adjusted SAH risk (Table 3).
Association between three SNPs within MMP-9 gene and SAH susceptibility.
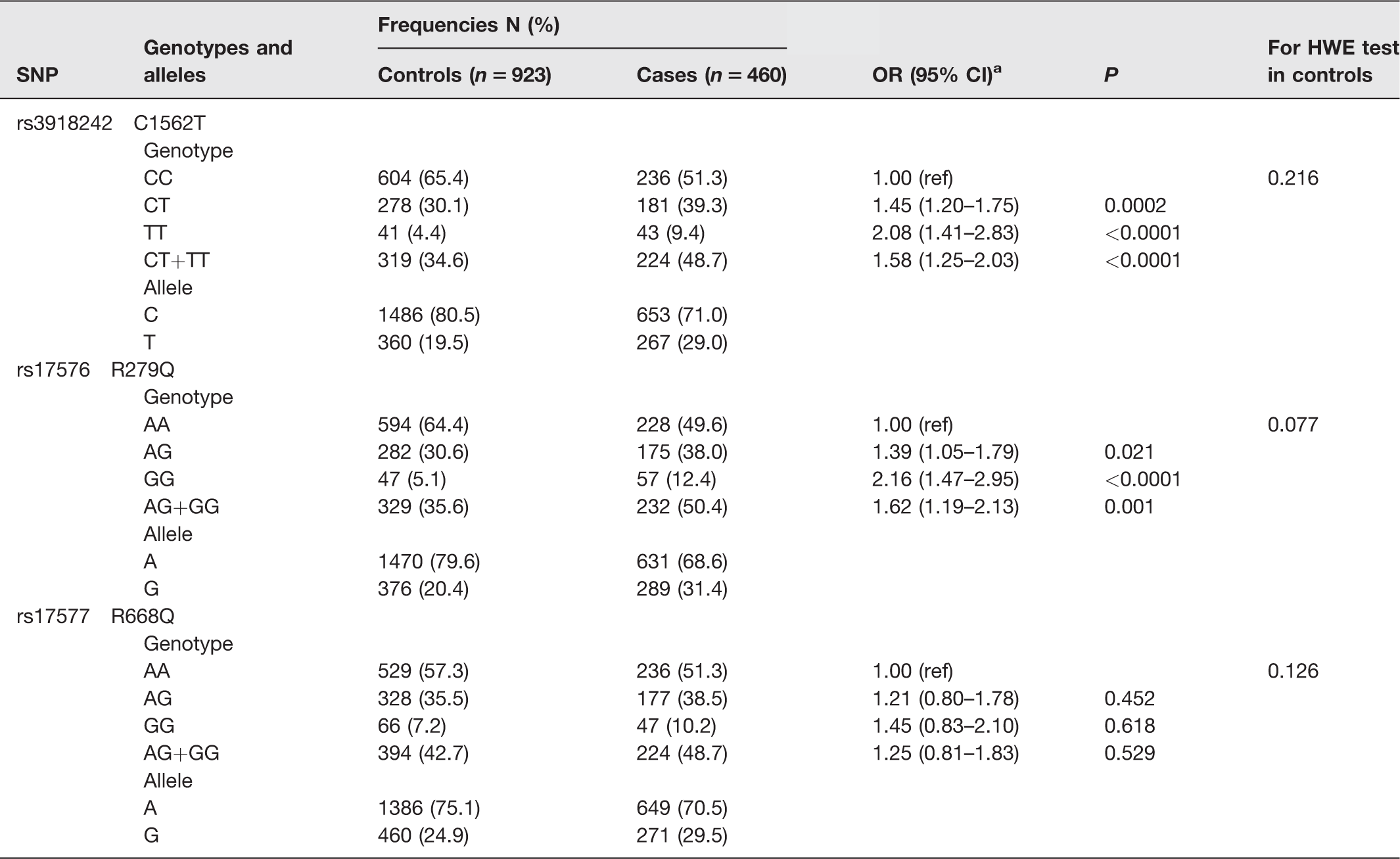
aAdjusted for gender, age, smoking and alcohol drinking, BMI, T2DM and hypertension.
SNPs; single nucleotide polymorphisms; SAH: subarachnoid hemorrhage; MMP-9: matrix metalloproteinase-9.
GMDR analysis on the best gene–gene and gene-current smoking interaction models.
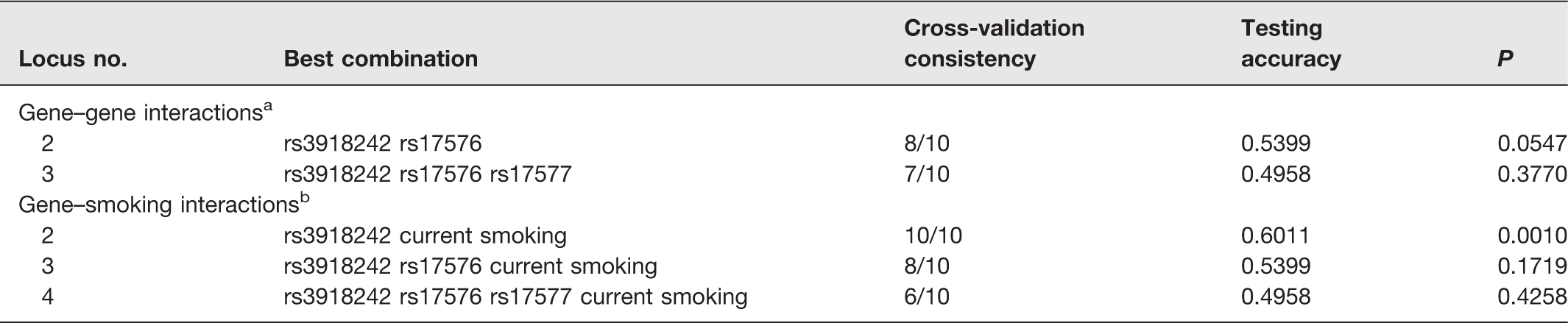
aAdjusted for gender, age, current smoking and current alcohol drinking, BMI, T2DM and hypertension for gene–gene interaction analysis.
bAdjusted for gender, age, current alcohol drinking, BMI, T2DM and hypertension for gene–smoking interaction analysis.
GMDR: generalized multifactor dimensionality reduction.
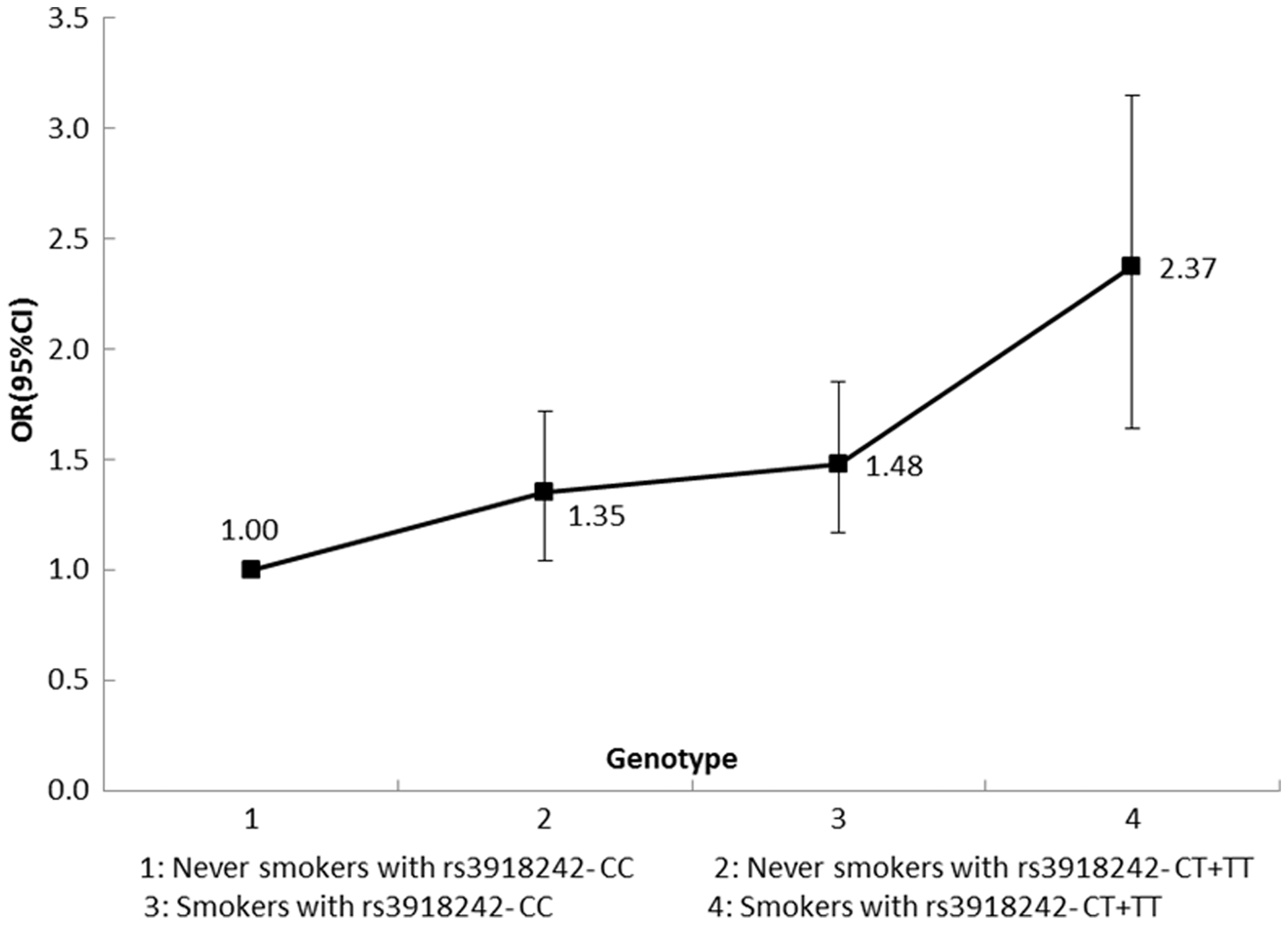
Stratified analysis for gene-smoking interaction by using logistic regression.
Discussion
In this study, we verified that rs3918242 (T) and rs17576 (G) were significantly related to the elevated SAH risk, but there was no association of the rs17577 with SAH risk after covariates adjustment. MMP-9 was a possible candidate gene for some diseases, including metabolic syndrome, 11 stroke,12,15–17 CAD. 13 But to date, limited data focused on the relationship between MMP-9 SNPs and SAH susceptibility. The SNP-rs3918242 has been more studied previously in relationship with some cerebrovascular related disease. A study conducted by Hao et al. 15 suggested that IS risk was higher in those with minor alleles of MMP-9-rs3918242 polymorphism; the authors also found a significant interaction between its polymorphism and tobacco smoking. Another study 16 showed that T allele of MMP-9 rs3918242 is correlated with lower hemorrhagic transformation of IS. Zhao et al. 17 showed that the rs3918242 is closely related to the pathogenesis of IS, and the interaction between this gene polymorphism and the risk of BMI in IS risk provides a new possibility for the effect of MMP-9 gene polymorphism on the susceptibility to stroke. In addition, the potential association of several polymorphic sites of MMP-9 with primary hypertension has also been extensively investigated,18–20 which was a main risk factor for SAH. Huang et al. 18 indicated that MMP-9 rs3918242 was correlated with primary high blood pressure, but this correlation was not reported in other investigations.19,20 A meta-analysis 21 indicated that MMP-9-rs3918242 polymorphism was correlated with essential hypertension risk. Yadav et al. 11 suggested that a higher serum level of MMP-9 in the presence of MMP-9–rs3918242 might be at a risk developing MetS. Several studies also investigated the association between MMP-9 gene and CAD. Zhang et al. 22 provided evidence that rs3918242 polymorphism may have modification effects on CAD susceptibility in Asians, but another meta-study 23 suggested that the MMP-9-rs3918242 was associated with an increased CAD trend in Chinese Han population. Therefore, the Han Chinese-1562T carriers may increase the risk of CAD.
SAH susceptibility was affected by both genetic and environment factors. Many risk factors for SAH have been previously assessed, including age, female, hypertension, and tobacco.4,5 Among them, smoking has been considered to play a crucial effect on increasing the risk of SAH. In this study, the rate of smoking in patients with SAH was higher than that in controls. For SNPs – smoking cross reaction, we investigated gene–environment interactions while investigating the effects of gene–gene interactions on SAH. Our study indicated that there is a potential cross reaction between rs3918242 and smoking on the risk of SAH, compared to never-smokers with rs3918242-CC genotype, the current smokers carrying rs3918242-CT or TT has the highest risk of SAH.
The limitations in this study are: Firstly, the number for studied SNPs within MMP-9 gene was relatively little and more SNPs within MMP-9 should been included in the analysis. Secondly, cases and control individuals were from a single hospital in China. Thirdly, when considering the compliance in this study, the most participants were relatively old persons, participants cannot represent the general population and there may be selection bias in our study.
In conclusion, MMP-9–rs3918242 (T) and rs17576 (G) and interaction between rs3918242 and smoking are related to the increased risk of SAH.
Footnotes
Authors’ contributions
Jing Wang: wrote the manuscript, conceived and designed the experiments. Wanxing Fu, Shuang Song and Yanlong Han: cellular experiment operation. Lihong Yao and Youkui Lu: data processing and statistical analysis. Junshuai Zheng and Tao Wang: experimental guidance and data verification.
Acknowledgements
We thank our colleagues from the School of Basic Medical Sciences of Mudanjiang Medical University, the Affiliated Hongqi Hospital of Mudanjiang Medical University and the first People's Hospital of Mudanjiang, and all the partners and staffs who helped us during the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Project of Health and Family Planning Commission of Heilongjiang Province (2016–380).