
Abstract
Based on evidence extracted from a cross-sectional review of the literature, we sought to advance a novel conceptual framework that the physiology of hemorrhagic shock from exsanguination and maximal oxygen uptake (
Impact statement
Disturbance of normal homeostasis occurs when oxygen delivery and energy stores to the body’s tissues fail to meet the energy requirement of cells. The work submitted in this review is important because it advances the understanding of inadequate oxygen delivery as it relates to early diagnosis and treatment of circulatory shock and its relationship to disturbance of normal functioning of cellular metabolism in life-threatening conditions of hemorrhage. We explored data from the clinical and exercise literature to construct for the first time a conceptual framework for defining the limitation of inadequate delivery of oxygen by comparing the physiology of hemorrhagic shock caused by severe blood loss to maximal oxygen uptake induced by intense physical exercise. We also provide a translational framework in which understanding the fundamental relationship between the body’s reserve to compensate for conditions of inadequate oxygen delivery as a limiting factor to
Introduction
Maintaining a balance between delivery and utilization of oxygen in various organs of the body represents a fundamental premise for sustaining “adequate” tissue oxygenation and cell function. As the requirement for oxygen uptake and utilization (
“Shock” has been described as a pathophysiological condition of “inadequate tissue oxygenation”1,2 that ensues when DO2 fails to meet the tissue
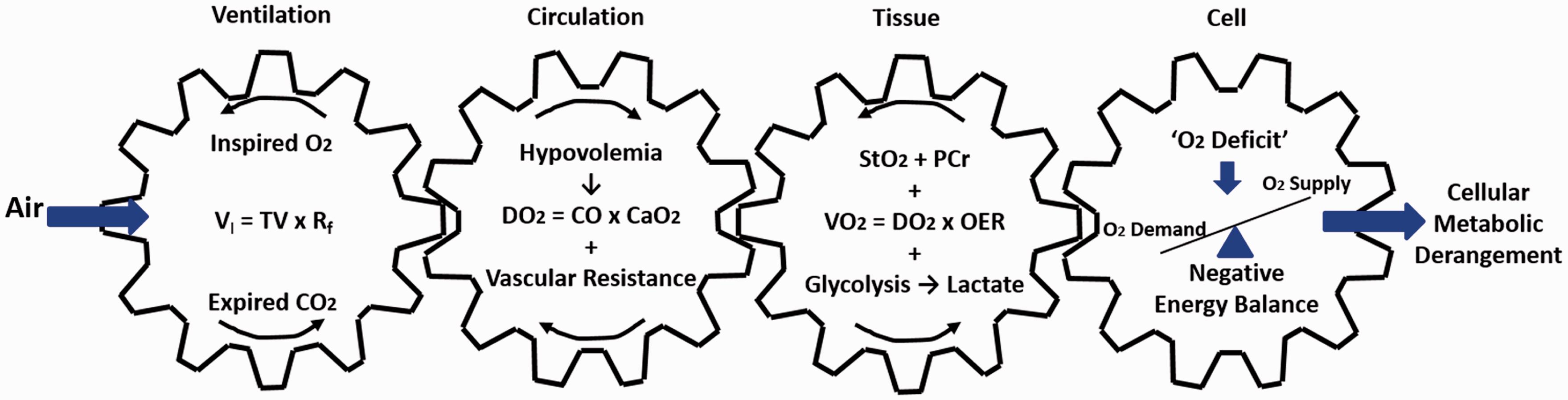
Conceptual model to illustrate the cascade coupling of ventilation, circulation, tissue metabolism, and energy balance in the mitochondria to cell function that defines common pathways to hemorrhagic shock and V̇O2max. VI: inspiratory volume; TV: tidal volume; Rf: respiratory frequency; DO2: oxygen delivery; CO: cardiac output; CaO2: oxygen carrying capacity; V̇O2: oxygen uptake; OER: oxygen extraction ratio; StO2: tissue oxygen saturation; PCr: phosphocreatine. Conceptually adopted from Wasserman. 9 (A color version of this figure is available in the online journal.)
Absolute vs. relative hypovolemia
Central hypovolemia represents another common fundamental physiological state that underlies the inadequate DO2 resulting from both hemorrhage and many instances of physical exertion at

Conceptual comparison of normal circulating blood volume (normovolemia) with absolute and relative hypovolemia. Orange indicates circulating blood volume; Pink indicates capacitance of vascular space. Adopted from M.N. Sawka with permission. (A color version of this figure is available in the online journal.)
Clinical concepts of oxygen deficit and debt
The terms oxygen “deficit” and or “debt” are routinely used in emergency and critical care medicine to reflect a mismatch between cellular energy requirement and
Inadequate DO2 created by
O2max
Inadequate DO2 can be defined as inability of O2 delivery to tissues to meet cellular energy demand. Figure 3 provides a conceptual schematic of the continuum of DO2 moving from normal rest. Moving to the right of resting baseline
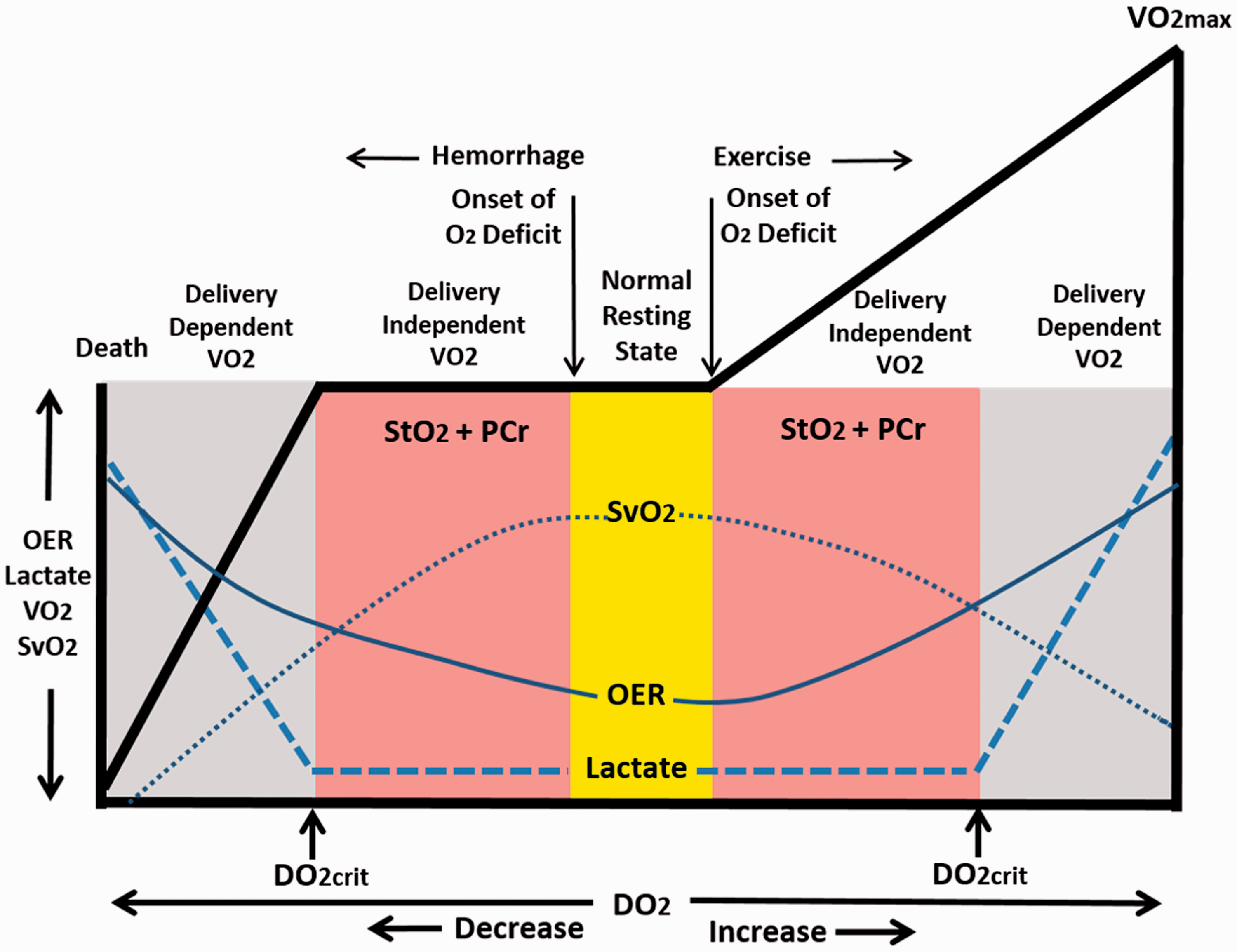
Conceptual representation of the continuum of metabolic relationship of oxygen delivery (DO2) to utilization (V̇O2) responses from hemorrhagic shock (left of Normal Resting State) to exertion at V̇O2max (right of Normal Resting State). OER: oxygen extraction ratio; SvO2: venous oxygen saturation; StO2: tissue oxygen saturation; PCr: phosphocreatine; DO2crit: critical oxygen delivery. Responses to progressive hemorrhage modified from Hooper et al. 13 See text for explanations.
Inadequate DO2 created by hemorrhage
The extrapolation of metabolic events that lead to

Time course of responses of systemic oxygen delivery (DO2; Panel A), systemic oxygen uptake (V̇O2; Panel B), tissue oxygen saturation (StO2; Panel C), and oxygen extraction ratio (Panel D) during progressive central hypovolemia induced by lower body negative pressure (LBNP). Data are means ± SD; n = 18. Modified from Ward et al. 25
Within this construct of timing, the clinical description of an onset of O2 deficit as the point in time at which tissue metabolism converts to anaerobic glycolysis to produce lactate in an effort to sustain the total energy requirement of the cell during hemorrhage has been misleading.1,13,14 Contrary to this hypothesis, failure to reach DO2crit in the presence of reduced O2 extraction reserves (Figure 4) supports the concept that O2 deficit, defined by reduced O2 extraction reserve, must occur in advance of reaching DO2crit. As such, the onset of O2 deficit during hemorrhage, like exercise, is initiated by a compensatory utilization of the O2 extraction reserves before there is increased anaerobic glycolysis. As such, we propose a revision in the biphasic relationship between DO2 and
Physiologic similarities between hemorrhagic shock and
O2max
The ultimate challenge of the cardiopulmonary and metabolic systems in both conditions of hemorrhagic shock and
Similarities in qualitative and quantitative cardiopulmonary, metabolic and autonomic responses for hemorrhagic shock and exertion at

StO2: tissue oxygen saturation; PtO2: partial pressure of tissue oxygen; SNA: sympathetic nerve activity; OER: oxygen extraction ratio; SvO2: venous oxygen saturation; [LA]: lactate concentration; BD: base deficit; Rf: respiration frequency; Vt: tidal volume; EtCO2: end-tidal carbon dioxide.
aData from animal experiments.bCase study of one trauma patient.
Hemodynamic mechanisms
Despite stark differences in systemic arterial blood flow, blood pressure, DO2, and
Similar to exercise, the cardiac response to hemorrhage relies on optimizing cardiac output in an effort to maintain perfusion (arterial blood) pressure. Despite vast differences in cardiac filling, severe hemorrhage can elicit tachycardia greater than 120–180 beats per minute (bpm) in shock1,32,49 similar to the pronounced elevation in heart rate of 140–200 bpm during exercise requiring maximal effort.33,34 Whether supporting the low cardiac filling states of acute hemorrhage or high cardiac filling during physical exercise, increased cardiac rate represents a common compensatory mechanism for optimizing cardiac output.
Autonomic mechanisms
Autonomically mediated elevations in heart rate are controlled by a combination of cardiac vagal withdrawal and sympathetic nerve activation. 33 Although the direct measurement of parasympathetic nerve activity is not readily accessible in humans, the use of frequency-domain analysis R-R interval variability has provided an indirect metric for changes in cardiac vagal activity by demonstrating nearly complete elimination of the high-frequency spectra (0.15–0.40 Hz) during muscarinic receptor blockade. 50 Calculating heart rate variability (HRV) from frequency-domain analysis has revealed that significant vagal withdrawal is an underlying mechanism of increased heart rate during both hemorrhagic shock 51 and maximal exercise.33,52,53
Hypovolemia is a very potent stimulus for activation of sympathetic activity. Catecholamine levels in the blood have been used as an indicator for adrenergic response to hemorrhage and exercise since the relationship between HRV measures and sympathetic activity is not as established as that for cardiac vagal activity.
52
In addition to vagal withdrawal, significant elevations in heart rate can be explained by blood levels of norepinephrine (NE) that become several times normal during both physical exercise at
The underlying mechanisms that elicit increased sympathetic nerve activation during physical exertion may provide insight to sympathetic control in conditions of blood loss. During exercise, heart rate can increase in the face of elevated arterial blood pressure because of a resetting of the cardiac baroreflex to a higher operating set point.
54
In contrast, the elevation in sympathetic nerve activity and heart rate associated with the central hypovolemia of hemorrhage is accompanied by reduced cardiac baroreflex sensitivity.
55
Since the pressure stimulus to arterial baroreceptors differs in direction between the hypotension associated with blood loss and the hypertension of exercise, metabolic stimuli that elicit activation of chemically-sensitive nerves in the tissues may represent a more likely common mechanism for activation of sympathetically mediated heart rate effects at
Oxygen extraction ratio and tissue oxygenation
Utilizing the O2 extraction reserve (e.g. hemoglobin bound O2, myoglobin-bound O2) represents a compensatory mechanism from which O2 can be provided to cells during hemorrhage and physical exercise when DO2 cannot meet the cellular requirement of
OER represents the ratio of
The premise that DO2crit occurs well after the onset and accumulation of O2 deficit is a fundamental relationship that evolved from the early work in exercise physiology that demonstrated an immediate development of an O2 deficit because of the difference between energy requirement and
The reliance on elevations in OER is reflected by normal resting levels of 20% to 30%
57
rising to as high as >50% during blood loss
25
and > 85–90% at
StO2 represents the amount (%) of myoglobin-bound O2. The myoglobin disassociation curve requires a significant reduction in the partial pressure of oxygen (pO2) in the tissue before O2 will be disassociated from myoglobin. Indeed, tissue pO2 has been reported to be as low as ∼5 mmHg compared to a baseline level of ∼34 mmHg in both hemorrhage
30
and maximal exercise.
31
A reduction in StO2 reflects a compensatory increase in the availability of O2 to support cellular
Glycolysis and lactate
When
Acid–base buffering
In contrast to lactate, the ultimate challenge during hemorrhagic shock and
Another sensitive means of assessing tissue oxygenation and O2 deficit is by measuring the base deficit, which represents the number of millimoles of base required to correct the pH of one liter of whole blood to 7.4.41,49 Indeed, the capacity to buffer blood acidity is reflected by a high correlation between increased base deficit and reduced arterialized blood pH,
32
with base deficits > 5 mmol/L being associated with both hemorrhagic shock32,42 and
Relatively small base deficits of only 6 to 10 mmol/L observed during hemorrhagic shock have been associated with “metabolic decompensation” when there is increasing requirements for blood transfusion
42
and the probability of death rises exponentially.
12
Although the reliance on tissue oxygen extraction reserves, phosphocreatine, and glycolysis exists with inadequate DO2 during both hemorrhage and
Mechanisms of pulmonary ventilation
Pulmonary ventilation is usually associated with gas exchange and is critical to the maintenance of adequate DO2 by maintaining optimal hemoglobin saturation of the blood in both hemorrhagic shock and exercise at
Comparisons of pulmonary ventilation responses during hemorrhagic shock and
Like respiration rate, the time kinetics of the tidal volume (VT) response to progressively increasing intensity of exercise leading to
Compensatory reserve
The physiological parameters listed in Table 1 represent responses of compensation to the combination of accumulated tissue O2 shortfall and inadequate DO2 associated with hypovolemic states of hemorrhage or exercise at maximal intensity. The capacity for compensation that “protects” against low tissue perfusion during states of compromised DO2 is known as the compensatory reserve.10,63–65 A historical challenge has been to develop a capability to measure the integration of compensatory mechanisms, particularly as it relates to DO2, rather than their physiological outcomes (e.g. blood pressure, SpO2, blood pH). Novel monitoring technologies have been developed that include the application of advanced real-time signal analysis and machine learning of hundreds of thousands of photoplethysmographic waveforms during progressive states of central hypovolemia. Application of such advanced computer processing algorithms has demonstrated that measures of arterial waveform features reflect the integration of all compensatory mechanisms recruited to sustain adequate DO2 during conditions of progressive hypovolemia with greater specificity and sensitivity compared to standard vital signs and metabolic markers.66–70 Specifically, changing features of the ejection wave reflect the sum of all compensatory mechanisms that control myocardial function, while reflected wave features reflect the sum of all mechanisms associated with compensation for compromised cellular energy requirements. 63
From the initial onset of hemorrhage or exercise (illustrated in Figure 3, broken lines), recruitment of the entirety of all compensatory mechanisms (e.g. autonomically-mediated tachycardia and blood flow redistribution, O2 extraction reserve, respiration, etc.) is required to maintain adequate DO2. With progression along the DO2 time continuum (Figure 3), the reserve capacity to compensate would be expected to gradually deplete until energy requirements for oxygen at the cellular level can no longer be sustained during progressively severe hypovolemia. This concept is supported by a linear relationship between compensatory reserve and DO2 (Figure 5). Ultimately, it is the depletion of compensatory reserve that leads to an inability to sustain energy requirements of the cells in the face of inadequate DO2 that leads to impending hemodynamic decompensation from blood loss63,72 or failure to continue muscular work at
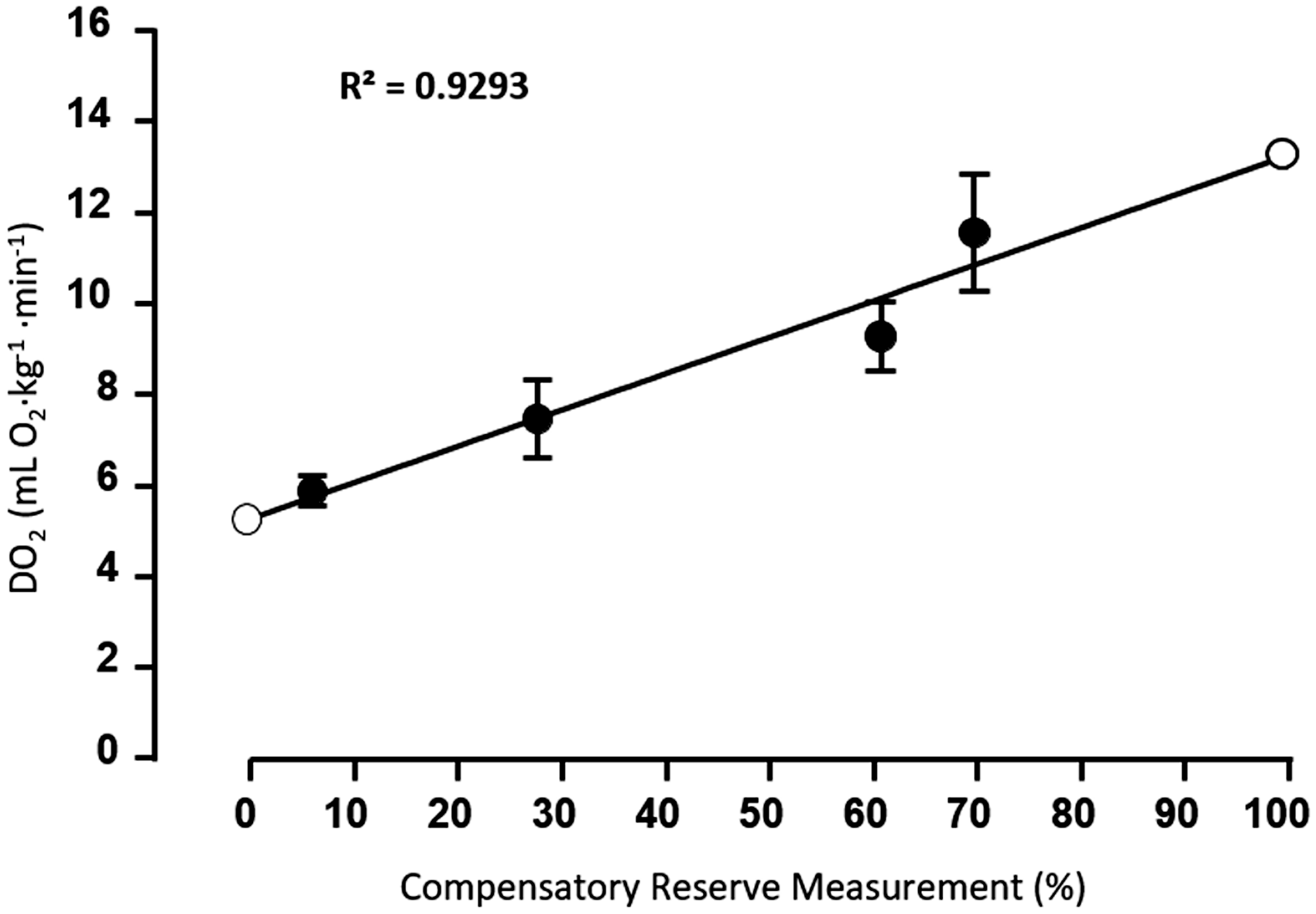
Linear regression of the relationship between systemic oxygen delivery (DO2) and compensatory reserve measurement (CRM) expressed by DO2 (mL O2·kg−1 ·min−1) = 0.08 × CRM (%) + 5.3. Open circles represent extension of the regression line to 0% and 100% CRM. Data, collected from non-human primates, are expressed as mean ± SEM; N = 12. Modified from Koons et al. 71
Individual variability in compensatory responses: A different perspective
Although the physiological responses listed in Table 1 represent generalizable direction and magnitude of changes in both conditions of hemorrhagic shock and physical work at
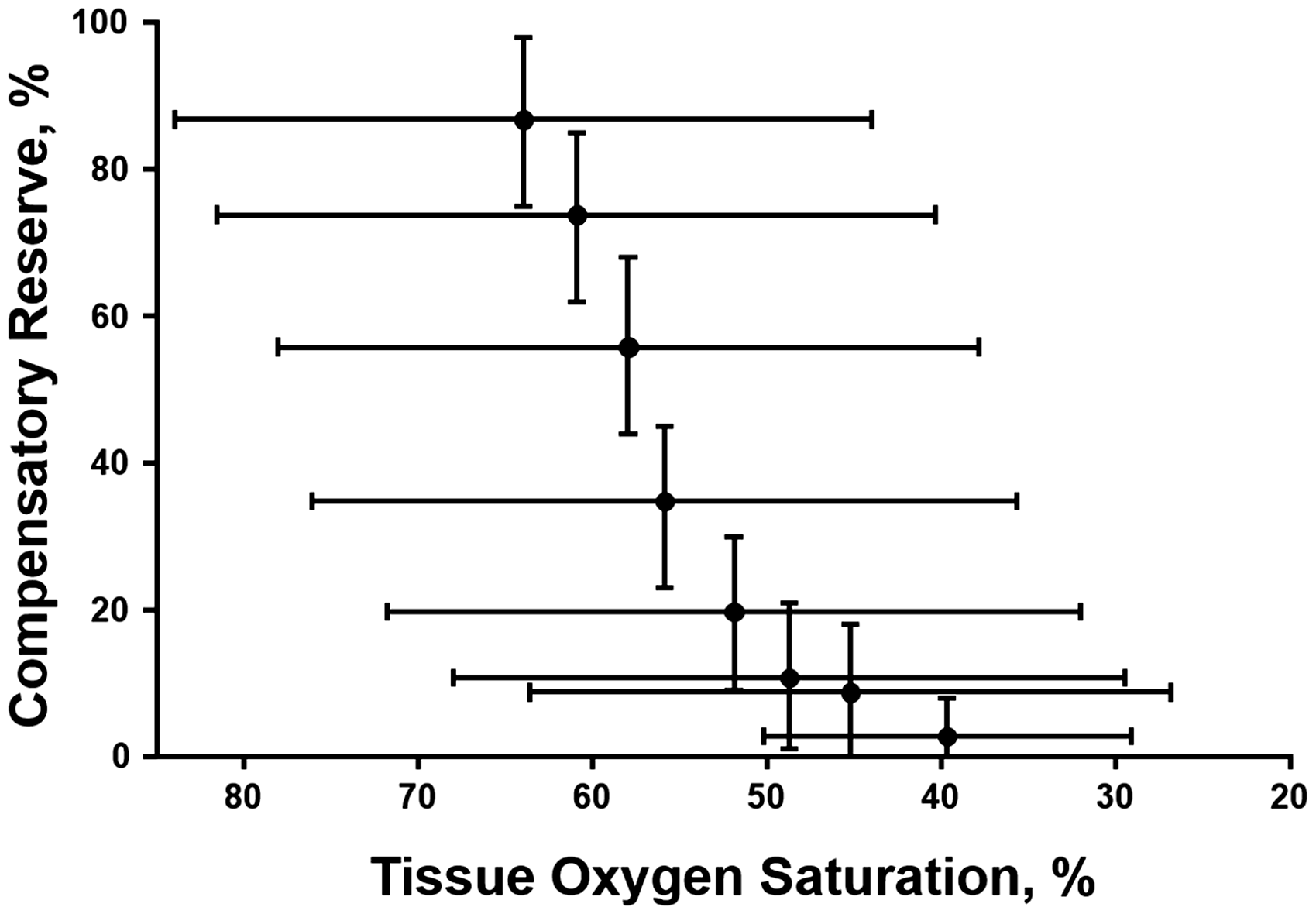
Relationship between tissue oxygen saturation and compensatory reserve. Symbols are average (±95% CI) values generated from 55 healthy volunteer subjects exposed to 0, −15, −30, −45, −60, −70, −80 and −90 mmHg LBNP. Amalgamated r2 = 0.965. Modified from Convertino and Sawka. 10
One approach to test this hypothesis is to compare individual variability in global compensatory response to hypovolemia in normal sedentary people to exercise-trained individuals and world class endurance athletes who have extraordinarily high blood volume, capillary density, cellular mitochondrial content, and aerobic enzyme activities.19,23 If tissue capacity for storing and utilizing oxygen contributes to mitigating the accumulation of O2 deficit, it might be expected that the endurance athlete’s physiology designed to support high
Hemorrhagic shock vs.
O2max conceptual framework: Other factors to consider
In addition to sharing key common physiological features, it is important to consider that reaching the threshold of hemorrhagic shock or
Clinical translation from the exercise experience
Accurate guidance for resuscitation of patients suffering from hemorrhagic shock represents a significant challenge to emergency medicine caregivers in their efforts to avoid the sequela associated with over- or under-resuscitation. A metric of inadequate DO2 reflects the most sensitive quantifier of the degree of shock,
13
but accurate assessment of DO2 has been limited by technology gaps in the ability to measure a bleeding trauma patient’s O2 shortfall and repayment O2 extraction reserve in real time.
13
As a result of this monitoring limitation, use of devices in pre-hospital critical care medicine that provide measures of blood lactate or tissue oxygen saturation has been proposed.13,77 However, challenges associated with the use of blood lactate or tissue oxygen as surrogate measures of compromised DO2 for guidance to clinical intervention are numerous. First, blood lactate levels do not necessarily reflect pathophysiology since their rise at
The key to effective resuscitation in patients with hemorrhagic shock is an appreciation “that it is not enough to simply halt the accumulation of oxygen debt (i.e. shortfall); it (O2 shortfall) must be repaid.” 13 The challenge, however, is that the clinical community has not realized a way to assess O2 shortfall in real time. 13 Figure 5 provides data obtained from experiments conducted on healthy baboons illustrating that measurement of the capacity to compensate (i.e. compensatory reserve) during whole blood resuscitation is closely correlated to DO2. 71 These results reflect the ability of changing features of the arterial waveform to provide a real-time measurement of integrated mechanisms that contribute to control of physiological factors that influence the development of O2 deficit. As such, it is compensatory reserve data collected with measures of exercise O2 deficit during exercise that provide a basis for using such technology for early identification of bleeding patients with hemorrhagic shock and for guiding accurate fluid or whole blood resuscitation leading to O2 deficit repayment.
Summary
Evidence provided by a cross-sectional review of the literature supports our conceptual framework that hemorrhagic shock in bleeding patients and
Footnotes
Authors’ contribution
All authors contributed to parts of the conceptualization, drafting or revising the article critically for important intellectual content, and final review and approval of the version submitted for publication.
ACKNOWLEDGMENTS
The authors thank Dr. Taylor Schlotman, Ms. Aiyana Helme, and Ms. Denise Woods for their technical assistance in the preparation of this manuscript.
DECLARATION OF CONFLICTING INTERESTS
The authors have no conflict of interests to report. The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the Department of the Army or the Department of Defense.
FUNDING
Funding for this work was provided in part by appointments to the Internship/Research Participation Program at the United States Army Institute of Surgical Research, administered by the Oak Ridge Institute for Science and Education (KRL, NJK) through an interagency agreement between the U.S. Department of Energy and Environmental Protection Agency, and grants from the US Army Medical Research and Materiel Command Combat Casualty Care Research Program (D-023–2011-USAISR; D-009–2014-USAISR; STO R.MED.2016.20).