
Abstract
Prediabetes, an intermediate stage between normal glucose regulation and type 2 diabetes, is diagnosed based on documentation of impaired fasting glucose, impaired glucose tolerance, or a hemoglobin A1c level of 5.7–6.4%. Individuals with prediabetes have increased risks for the development of type 2 diabetes and multiple vascular complications. Randomized controlled trials have demonstrated the feasibility of preventing progression from prediabetes to type 2 diabetes, using lifestyle or pharmacological interventions. Lifestyle modification has a sustained effect on diabetes prevention, whereas medications lose efficacy when discontinued. Few studies have pre-specified reversal of prediabetes as the primary outcome. There is emerging evidence that reversal of prediabetes (i.e. restoration of normal glucose regulation) confers significant protection from future diabetes and complications, including premature death, during long-term follow-up. Current lifestyle intervention protocols have been more effective in preventing progression from prediabetes to type 2 diabetes than restoring normal glucose regulation; thus, interventions that prevent type 2 diabetes in people with prediabetes do not always reverse prediabetes. Given the compelling benefits of restoration of normal glucose regulation, specific protocols for reversal of prediabetes need to be developed and tested. The design of such protocols requires a deeper understanding of the pathobiology of prediabetes and early glucose dysregulation. The present review focuses on those studies that have assessed the impact of interventions on regression of the prediabetes state and restoration of normal glucose regulation. Furthermore, we discuss alterations in adiposity, glucoregulatory mechanisms, metabolomics, inflammatory markers, and other factors that predict the initial escape from normoglycemia. Such knowledge could inform the future development of novel, refined, and targeted interventions for the reversal prediabetes/early dysglycemia and restoration of normal glucose regulation.
Impact statement
Prediabetes increases the risks of future type 2 diabetes (T2D) and vascular complications, risks that can be prevented by restoring normal glucose regulation (NGR). Few studies have pre-specified reversal of prediabetes and restoration of NGR as primary outcome, and current approaches that prevent T2D in people with prediabetes do not always reverse the prediabetes. The present review focuses on studies that have assessed reversal of the prediabetes, and discusses known and emerging predictors of prediabetes. We argue that fuller knowledge of such predictors could inform the discovery of novel, targeted interventions for reversing prediabetes.
Keywords
Introduction
Diabetes mellitus describes a group of disorders of glucose metabolism characterized by hyperglycemia. Currently, diabetes mellitus is diagnosed if fasting plasma glucose (FPG) is equal to or greater than 7.0 mmol/L (126 mg/dL), or a two-hour plasma glucose (2hrPG) is equal to or greater than 11.1 mmol/L (200 mg/dL) during an oral glucose tolerance test (OGTT). An hemoglobin A1c (HbA1c) level of 6.5% or greater also is diagnostic of diabetes mellitus. 1 The term “prediabetes” refers to an intermediate stage between normal glucose regulation (NGR; i.e. normal FPG and normal 2hrPG) and type 2 diabetes (T2D), and is characterized by impaired fasting glucose (IFG) and/or impaired glucose tolerance (IGT). 1 Currently, prediabetes is diagnosed if FPG is between 5.5 mmol/L and 6.9 mmol/L (100–125 mg/dL), or a 2hrPG is between 7.8 mmol/L and 11.0 mmol/L (140–199 mg/dL) during an OGTT. An HbA1c level of 5.7–6.4% can also be used to diagnose prediabetes (Table 1). 1
Current diagnostic criteria for prediabetes and diabetes. a
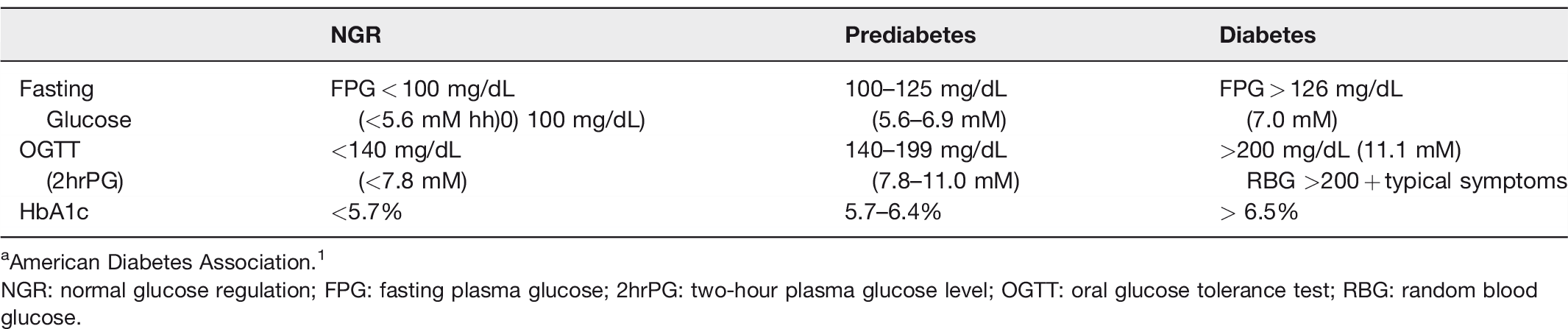
aAmerican Diabetes Association. 1
NGR: normal glucose regulation; FPG: fasting plasma glucose; 2hrPG: two-hour plasma glucose level; OGTT: oral glucose tolerance test; RBG: random blood glucose.
Worldwide estimates by the International Diabetes Federation indicate that approximately 463 million adults currently have diabetes and 374 million adults have prediabetes; the global diabetes prevalence is projected to increase to 700 million by 2045. 2 The transition from a state of NGR to prediabetes and T2D has been studied extensively and is known to be preceded by weight gain along with defects in insulin sensitivity, pancreatic beta-cell function and alterations in inflammatory cytokines, incretin response, and hepatic glucose production.3,4 Individuals with prediabetes progress to T2D at an annual rate of ∼10% and have increased risks for early development of the microvascular and macrovascular complications that typically occur in people with long-standing diabetes. 3 While the exact mechanisms are unclear, the accelerated manifestation of diabetic complications in some people with prediabetes is of significant public health importance.3,4
Numerous randomized controlled trials (RCTs) have demonstrated the feasibility of preventing progression from prediabetes to T2D, using lifestyle or pharmacological interventions.5–7 However, data from the RCTs showed that a substantial proportion of subjects still had persistent prediabetes or progressed to T2D, despite interventions.5–7 Few studies have pre-specified regression of prediabetes as the primary outcome. Given the emerging understanding of prediabetes as a toxic cardiometabolic state, the present review focuses on studies that have assessed regression of prediabetes during lifestyle interventions. We discuss the likelihood, methodology, mechanisms, and clinical implications of achieving reversal of the prediabetes state and restoration of NGR in contemporary practice and research.
Predicting progression from normal glucose regulation to prediabetes
Relatively, few studies (Figure 1) have focused on the transition from NGR to prediabetes.8–12 Among a high-risk population of Pima Indians with baseline normal glucose tolerance (NGT), the incidence of progression to prediabetes (IGT) was approximately 8% per year during four years of follow-up. 8 The significant predictors of incident prediabetes among the Pima included weight gain, insulin resistance, and progressive loss of insulin secretory capacity. 13 The PIMA Indians who maintained NGT status during follow-up had a mean weight change of +2.6 kg versus +5.6 kg in those subjects who progressed from NGT to IGT. 13 In the Baltimore Longitudinal Study of Aging (BLSA), 488 adults were determined to have NGT at baseline. During 10 years of follow-up, 62% of the initially NGT participants progressed to prediabetes, yielding an annualized incident prediabetes rate of 6.2% in the BLSA. Notably, the BLSA enrolled predominantly (96%) Caucasian subjects. 9 In a cross-sectional study of 27,552 Chinese adults, prevalent prediabetes (27.2% of the population) was significantly associated with body mass index (BMI) and waist circumference. 10 Waist circumference had a stronger association with prediabetes than BMI, consistent with the known dysmetabolic impact of visceral adiposity. 10
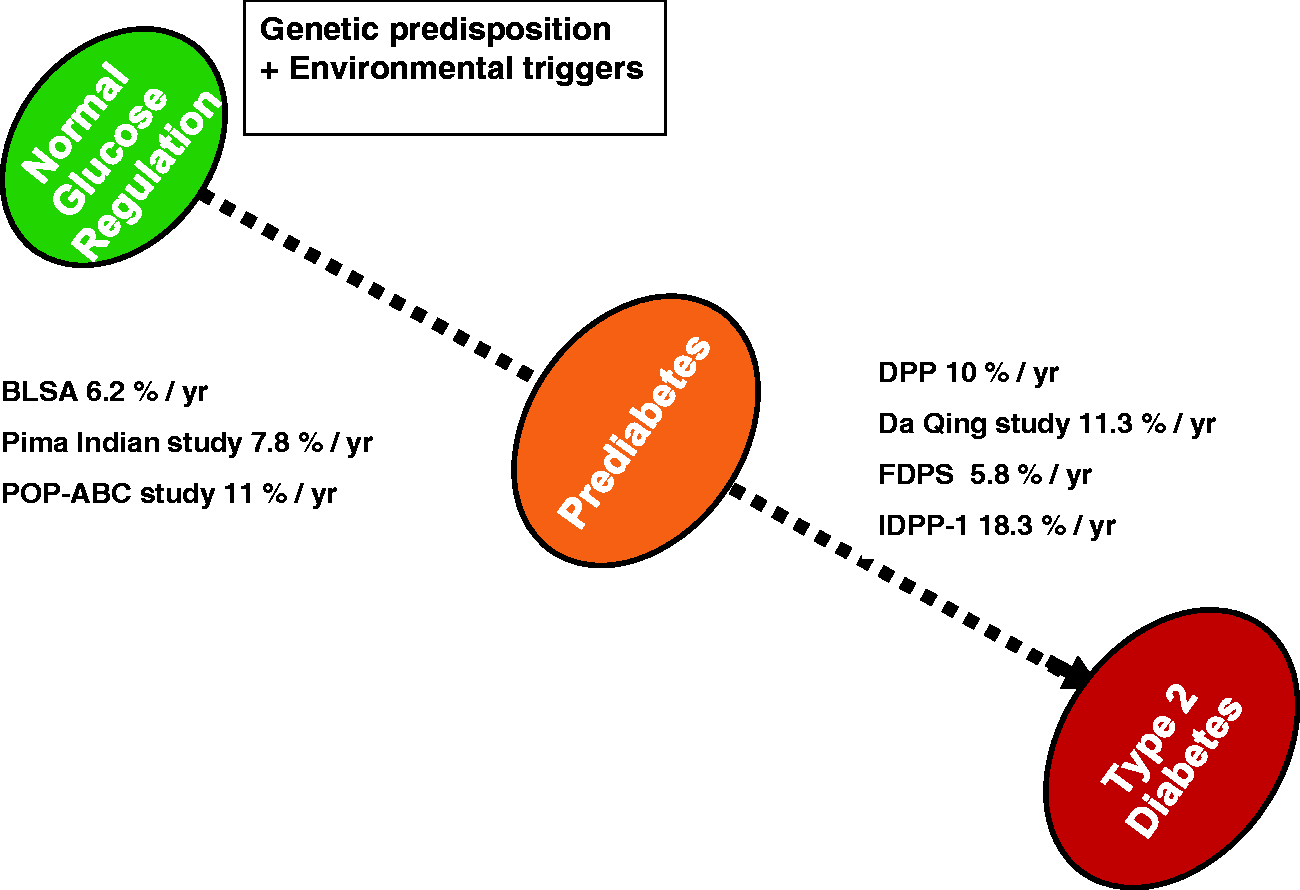
Longitudinal natural history and intervention studies on the transition from normal glucose regulation through prediabetes to type 2 diabetes.
In a Japanese study, 3879 participants with NGR were followed longitudinally for the outcome of incident prediabetes (based on combined FPG >6.1 mmol/l and HbA1c > 5.5%). 11 After five years of follow-up, 21 participants reached the combined prediabetes criteria, 1730 subjects reached one of the two criteria for prediabetes, and 2128 others maintained NGR. 11 The factors which predicted increased risk of transition from NGR to any prediabetes endpoint included baseline levels of hematocrit, alanine aminotransferase, triglycerides, and low-density lipoprotein cholesterol. 11 The Pathobiology of Prediabetes in a Biracial Cohort (POP-ABC) study enrolled healthy Caucasian and African-American offspring of parents with T2D and followed them for the primary outcome of incident prediabetes. 12 During the initial five years of follow-up (mean 2.62 years), ∼30% of participants developed prediabetes (annualized rate ∼11%). 12 The initially normoglycemic POP-ABC study cohort has now been followed up for more than 12 years, during which ∼44% of participants have progressed to prediabetes.
Thus, even among individuals with parental history of T2D, the occurrence of impaired glucose regulation is not universal. Because initial transition to prediabetes is a necessary intermediary step toward development of T2D, predicting individuals at risk for early dysglycemia would be valuable information that could help target preventive interventions to those at most risk. The baseline factors predictive of future progression from NGR to prediabetes among the POP-ABC study cohort included older age, male gender, higher BMI, larger waist, and higher total and abdominal fat mass. Participants whose FPG and 2hrPG were at the upper end of the normal range and those with lower values for insulin sensitivity, insulin secretion and disposition index were also more likely to progress to prediabetes. 12 The progressors to prediabetes also had higher baseline plasma levels of triglycerides and LDL cholesterol, and lower HDL cholesterol and adiponectin levels.17–19 Furthermore, analysis of 18 amino acids in the POP-ABC study showed that progression to prediabetes was predicted by higher baseline levels of asparagine and aspartic acid, glutamine and glutamic acid, and lower histidine levels. 19
These predictive factors (Table 2) can be modeled to formulate risk engines for stratifying currently normoglycemic subjects into those likely to maintain long-term NGR versus those at risk for early glucose abnormalities.
Predictors of transition from normal glucose regulation to prediabetes. a
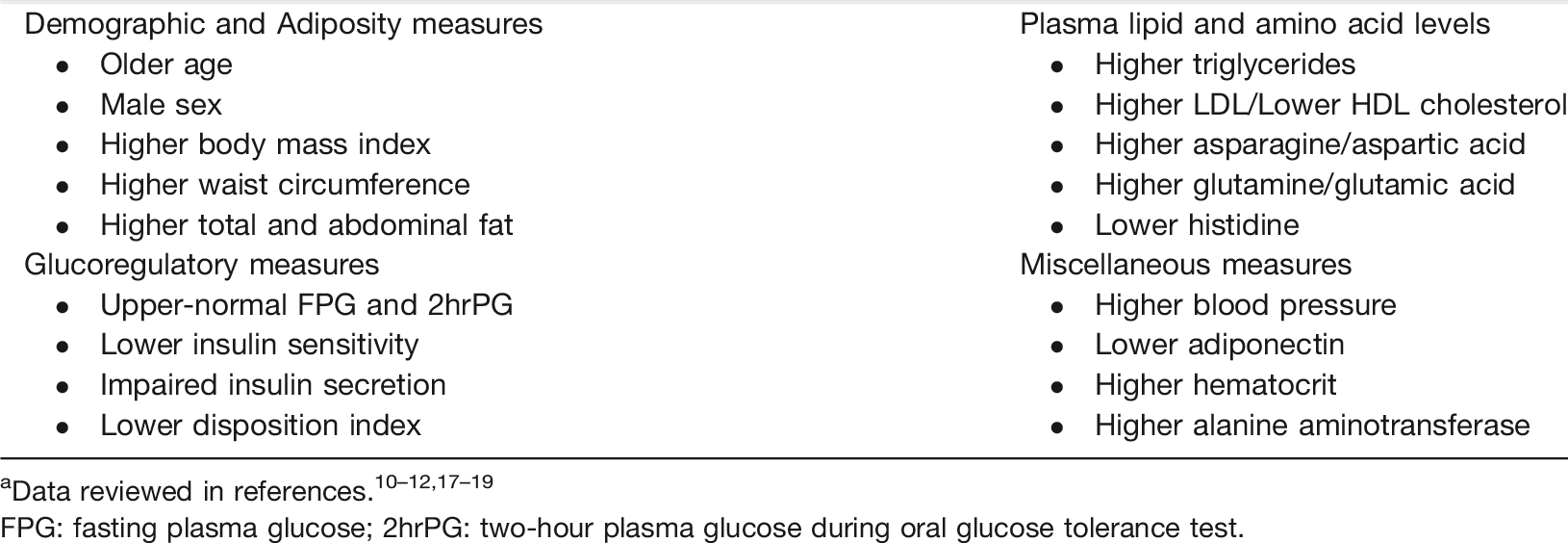
FPG: fasting plasma glucose; 2hrPG: two-hour plasma glucose during oral glucose tolerance test.
Overview of randomized controlled trials of type 2 diabetes prevention
The landmark RCTs that have tested interventions for preventing or delaying progression from prediabetes to T2D are discussed briefly (Figure 1).14–16,20,21The Diabetes Prevention Program (DPP), a large multicenter study based in the United States, enrolled an ethnically diverse population with IGT and high-normal FPG. The participants were randomized to three treatment groups: standard lifestyle recommendations plus metformin group; standard lifestyle recommendations plus placebo group; and an intensive lifestyle modification group (low calorie, low-fat diet, and at least 150 min per week of moderate intensity physical activity with the goals of at least a 7% weight loss). 14 After an average follow-up period of 2.8 years, the reduction in the incidence of T2D was greatest in the group randomized to intensive lifestyle modification (58%), followed by the metformin group (31%), compared with placebo. 14
The findings of the DPP were concordant with the effects of lifestyle intervention observed in the Da Qing diabetes prevention study (launched in 1986) among Chinese subjects with IGT. 20 Active intervention in the Da Qing study ceased after six years; however, extended follow-up outcomes were ascertained in 2006 (20 years), 2009 (23 years), and 2016 (30 years). Evidence of long-term benefit of prior lifestyle intervention on diabetes risk reduction was seen at every post-study assessment period. The most recent, 30-year follow-up, results from the Da Qing Study strengthened previous positive reports from the study by showing significant reductions in the incidence of T2D, microvascular and macrovascular complications, and cardiovascular and all-cause mortality in the lifestyle intervention group compared with control.22,23 The lifestyle group showed a consistent (26–35%) risk reduction across the various morbidity and mortality outcomes. Indeed, only 10 people with IGT would need to be treated with lifestyle intervention to prevent one death during 30 years of follow-up in the Da Qing study. Few medical interventions achieve such a remarkable mortality benefit: for comparison, approximately 250 people would need to be treated with a statin drug for one to six years to prevent one death in a high-risk primary prevention cohort. 24
The results of other RCTs, including the Finnish Diabetes Prevention Study, the Indian Diabetes Prevention Program (IDPP)-1 and IDPP-2, showed significant reduction in the risk of progression from prediabetes to T2D following lifestyle intervention.15,16,21 The IDPP-1 tested the effects of a control intervention (standard healthcare advice), lifestyle modification, metformin only, and metformin plus lifestyle intervention on progression from IGT to T2D. 16 After three years of follow-up, the relative risk reduction in the incidence of T2D was 28.5% with lifestyle modification, 26.4% with metformin, and 28.2% with lifestyle modification plus metformin. 16 The IDPP-2 determined whether the addition of pioglitazone to lifestyle modification would result in an additive effect on diabetes risk reduction. 21 The results of IDPP-2, similar to those of IDPP-1, did not show additive effect of medication plus lifestyle intervention. 21 The major lesson from the landmark RCTs is that lifestyle modification is a potent antidote to progressive dysglycemia in people with prediabetes.
Reversal of prediabetes and restoration of normal glucose regulation
Several RCTs of lifestyle interventions or pharmacological agents for diabetes prevention have reported additional data on the proportion of subjects who experienced reversal of prediabetes and restoration of NGR (Table 3).14,21,25–31 Clearly, a return to NGR is of benefit because of decreased risk of development of T2D and long-term complications when achieved.
Prevention of type 2 diabetes and reversal of prediabetes in randomized controlled trials using lifestyle and/or medication interventions.
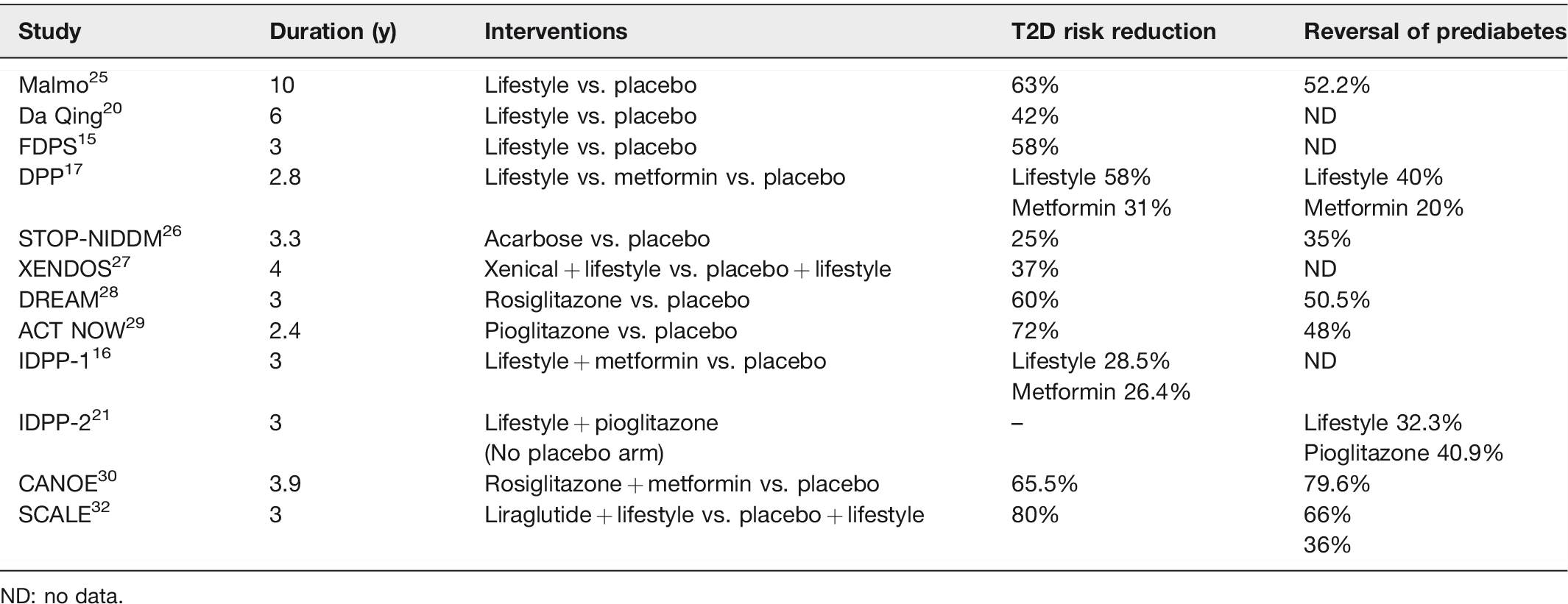
ND: no data.
The Malmö study enrolled Swedish men with IGT (N = 181) or early-stage T2D (n = 41) in a prospective study to test the feasibility of long-term intervention with lifestyle modification. 25 Participants randomized to the lifestyle intervention group received supervised physical training by a physiotherapist (60 min two times in a week of calisthenics, walking, jogging, soccer and badminton) for six months and dietary advice by a physician and a dietitian (less sugar, increased fiber and unsaturated fat, reduced energy intake) for another six months. The average BMI of the participants at enrollment was 27.0 kg/m2. Body weight decreased by 2.3–3.7% in the lifestyle group. For comparison, body weight of IGT subjects who did not receive lifestyle intervention and that of normal control subjects increased by 0.5–1.7%. 25 After ∼ 6 years of follow-up, 52.2% of IGT participants in the intervention group had reverted to NGT with lifestyle modification and 50% of the patients with early T2D went into remission. 25 The glycemic improvements were accompanied by favorable changes in blood pressure, lipids, and hyperinsulinaemia, and restoration of acute insulin secretory response to glucose. 25
Similarly, after three years of follow up in the DPP study, ∼40% of participants randomized to the intensive lifestyle modification arm achieved NGT versus ∼20% in the metformin or placebo arms.14,33 DPP participants with lower baseline FPG and 2hrPG were more likely to experience regression of prediabetes; younger age, greater insulin secretion, and weight loss also significantly predicted the likelihood of reversal to NGR. 33 Thus, both Malmö study and DPP demonstrated that lifestyle-based intervention achieved reversal from prediabetes to NGR in some 40–50% of participants.
Some pharmacological agents have also been tested alone or in combination with lifestyle interventions to determine if there is an additive effect on regression of prediabetes. The multinational Study to Prevent Non-insulin-dependent diabetes mellitus (STOP-NIDDM) trial was a placebo-controlled randomized study in participants with IGT. 26 The mean age of the participants was 54 years and the mean BMI was 31.0 kg/m2. Participants were randomized to either acarbose (100 mg three times a day) or placebo, and assessed for the outcome of conversion from IGT to T2D. After approximately three years of follow-up, 35% of participants with IGT randomized to acarbose had reverted to NGT. However, after three months of cessation of acarbose, there was glycemic rebound, and the regression to NGT was not sustained. 26
The XENical in the Prevention of Diabetes in Obese Subjects (XENDOS) study randomized 3305 obese patients to lifestyle modification plus either orlistat 120 mg or placebo, three times daily and followed them for four years. 27 The participants had normal (79%) or impaired (21%) glucose tolerance at enrollment. The results showed a diabetes risk reduction of 37% with orlistat combined with lifestyle modification relative to lifestyle intervention plus placebo. Orlistat treatment was associated with a mean weight loss of 5.8 kg (versus 3.0 kg with placebo) over a four-year period. The weight loss effect was noted in both the IGT and the NGT subgroups; however, the reduction in T2D incidence was driven by responses among participants with IGT at enrollment. Among participants with NGT at enrollment, the rate of progression from NGT to IGT over four years was similar between orlistat- and placebo-treated groups (27.6% vs. 30.5%). 27 The XENDOS investigators did not report the rate of reversion from IGT to NGT among their participants.
In the DREAM (Diabetes Reduction Assessment with ramipril and rosiglitazone Medication) study, participants from 21 countries with IFG or IGT or both were randomized to rosiglitazone (4 mg once daily for the first 2 months and then 8 mg once daily) or placebo. The mean age of participants was 55 years, and the mean BMI was 31 kg/m2. After three years of follow-up, 50.5% of participants in the rosiglitazone group achieved normoglycemia compared to 30.3% in the placebo group. 28 As was observed with acarbose, the effect of rosiglitazone was not sustained when the drug was withheld for three months. 34 Another thiazolidinedione, pioglitazone, was tested in the Actos Now for Prevention of Diabetes (ACT NOW) study that enrolled participants with IGT (mean age 52 years, mean BMI 34 kg/m2). 29 After a median follow-up of 2.4 years, 48% of participants in the pioglitazone group, compared with 28% in the placebo group, had reverted to NGT. 29 Approximately 11 months after discontinuation of pioglitazone, the proportion with NGT decreased to 23%, indication loss of drug efficacy. 35
As previously discussed, participants in IDPP-2 were randomized to lifestyle modification plus pioglitazone (started at 15 mg and increased to 30 mg after 6 months) and lifestyle modification plus placebo. The average age of the participants was 45 years, with a BMI of 26 kg/m2. After three years of follow-up, 40.9% of participants receiving pioglitazone reverted to NGT compared to 32.3% randomized to placebo. The addition of pioglitazone did not have an additive effect to that obtained with lifestyle modification. 21 Yet another RCT, the Canadian Normoglycemia Outcomes Evaluation (CANOE) study, randomized participants with IGT (mean age 52 years, mean BMI 32 kg/m2) to treatment with a fixed dose combination capsule (metformin 500 mg plus rosiglitazone 2 mg taken two times daily) or placebo. After a median follow-up of 3.9 years, reversion from IGT to NGR occurred in 80% of participants randomized to metformin plus rosiglitazone combination, as compared to 53% subjects in the placebo group. 30
Additional insight on regression of prediabetes was provided by a subgroup analysis of participants in a multi-center RCT that evaluated the safety and efficacy on weight loss of liraglutide when added to lifestyle modification. 31 Among the subgroup of participants who had prediabetes at enrollment (N = 2285, ∼60% of the study population), 69% of those randomized to the liraglutide plus lifestyle modification group reverted to normoglycemia at 56 weeks of follow-up, compared to 36% of participants in the placebo plus lifestyle modification group.31,32 After three years of follow-up, the proportion of participants achieving regression of prediabetes persisted (66% in the liraglutide group and 36% in placebo). 32 However, the reversed state was not sustained, and prediabetes recurred in some participants after ∼3 months of stopping liraglutide. 32
The lack of sustained effect following cessation of medications contrasts with the sustained benefits observed with lifestyle modification.34–37 After the completion of the active intervention stage of the Malmö study, the 12 years follow-up report showed a mortality benefit among the IGT subjects who received prior lifestyle intervention. The DPP, Finnish Diabetes Prevention Study, and the Da Qing Study all demonstrated sustained reduction in the incidence of T2D in the lifestyle modification group, 10 to 30 years after cessation of active intervention.5–7,22,37
Bariatric surgery induces massive weight loss (∼25% to >95% depending on the study population, type of surgery, and length of follow-up. 38 Rapid resolution or amelioration of diabetes and other co-morbid conditions, such as hypertension and dyslipidemia, has been reported following bariatric surgery. Schauer et al. 39 randomized 150 patients with T2D (age 49 ± 8 years; BMI ∼37; HbA1c 9.2%) to medical therapy, sleeve gastrectomy or Roux-en-Y gastric bypass (RYGB) and assessed the effects on the primary outcome of attainment of HbA1c <6.0%. 39 After one year of follow-up, the mean weight loss was 5.4 kg, 25.1 kg, and 29.4 kg in patients assigned to medical therapy, sleeve gastrectomy, and RYGB, respectively. The proportion of patients attaining HbA1c of <6.0% was 12%, 42%, and 37% in patients assigned to medical therapy, sleeve gastrectomy, and RYGB, respectively. 39 Concordant results from other studies underscore the efficacy of bariatric surgery on remission of T2D.40–42 However, re-assessment at 10 years after bariatric surgery showed recurrence of diabetes in ∼50% of patients who had previously enjoyed remission. 41
Bariatric surgery has also been associated with decreased incidence of T2D. Among individuals who did not have diabetes at enrollment in the Swedish Obese Subjects study, bariatric surgery was associated with ∼90% reduction in the risk of incident T2D during 15 years of postoperative follow-up. 43 Thus, there is little doubt that bariatric surgery, through numerous mechanisms (including weight loss, improved insulin sensitivity, alterations in inflammatory cytokines, etc.), could reverse or prevent T2D. However, the amount of weight loss (∼5–7%) required for diabetes prevention in people with prediabetes is achievable by non-surgical means, and prediabetes, per se, is currently not one of the indications for bariatric surgery in professional guidelines.44,45
Clinical impact of regression from prediabetes to normal glucose regulation
Apart from the ever-present risk of prediabetes progressing to T2D, the prediabetes state is associated with microvascular complications (retinopathy, neuropathy, and nephropathy) and macrovascular complications (myocardial infarction, stroke, or cardiovascular death). 4 Thus, the clinical benefits of regression from prediabetes to NGR cannot be overemphasized. In the Diabetes Prevention Program Outcome Study (DPPOS), the observational extension of the DPP, participants with prediabetes who achieved NGR at least once during long-term follow-up had a 56% lower risk of incident T2D compared with those who maintained persistent prediabetes and never achieved NGR. 46 Furthermore, the number of times a participant achieved NGR was shown to have a direct association with the risk reduction in incidence of T2D: 47% when NGR was achieved once, 61% when NGR was achieved twice, and 67% when NGR was achieved three times. 46 This benefit of risk reduction in incidence of T2D derived from the reversion to NGR was independent of prior treatment group. Thus, even transient periods of maintaining NGR in a patient with prediabetes decreases risk of development of T2D. 46
The decreased incidence of T2D in patients who attained NGR in DPP translated clinically to a corresponding reduction in the prevalence of microvascular disease after a median follow-up of the participants for 15 years during the DPPOS phase. 47 Regression of prediabetes and restoration of NGR in the DPP/DPPOS cohort also was associated with decreased macrovascular risk. 48 A recent analysis of the long-term observational cohort, the Whitehall II study, revealed that most people with HbA1c-defined prediabetes had persistent prediabetes or progressed to T2D during five years of follow-up. 49 By contrast, some people with FPG or 2hPG-defined prediabetes experienced reversion to normoglycemia. As the Whitehall study did not include intervention, such reversion to NGR likely occurred spontaneously or by random fluctuations among the free living study participants. Further analysis of comorbidities indicated that reversion from 2hPG-defined prediabetes to normoglycaemia was associated with reduction of future risk cardiovascular disease and mortality. 49
Conclusions and future directions
The term “prediabetes” has been used in the medical literature since 1918. 50 The modern definition of prediabetes, based on precise blood glucose measurement, includes individuals with IFG and/or IGT. Numerous observational, cross-sectional, and randomized clinical studies indicate that the prediabetes state is associated with increased risks for T2D and vascular complications.3,4,6,7,9 Thus, the weight of evidence rebuts the notion that prediabetes is a “dubious” diagnosis. 51 Indeed, after 30 years’ follow-up in the Da Qing study, the cumulative incidence of T2DM was 95.9% in the control group and 88.7% in the lifestyle intervention group. 22 Thus, the natural history of prediabetes bends toward either persistence of the prediabetes state or development of T2D, rather than spontaneous reversal to NGR. The RCTs reviewed here provide compelling evidence that lifestyle modification can decrease the risk of progression to T2D in people with prediabetes, with an effect size of ∼60% risk reduction compared with placebo.5–7 However, many subjects maintained persistent prediabetes or progressed to T2D, despite such intervention. Thus, prevention of diabetes is not synonymous with reversal of prediabetes, and the latter had been largely an incidental outcome of most diabetes prevention studies.
Given the known associations of prediabetes with microvascular and macrovascular complications, reversal of prediabetes and restoration of NGR ought to be the goal of intervention. Data from the Malmo and DPP studies show that lifestyle intervention can restore NGR in a substantial proportion (∼40%–50%) of individuals with IGT, even though those studies did not specifically aim to induce regression of prediabetes. The extant data from RCTs show that the lifestyle intervention protocols utilized in the studies might have been more effective in preventing progression from prediabetes to T2D than they were at inducing regression of prediabetes and restoring NGR. With the emerging evidence that restoration of NGR, even if transiently, is associated with robust reductions in future risks of diabetes and vascular complications, specific protocols for reversal of prediabetes need to be developed and tested. The design of such protocols requires a deeper understanding of the pathobiology of prediabetes, so that the triggers and predictors of early dysglycemia can be better targeted. In the present minireview, we have presented current knowledge of the alterations in adiposity, glucoregulatory mechanisms, metabolites, lipid profile, inflammatory markers, and other factors that predict the initial escape from normoglycemia. These factors (listed in Table 2) can be modeled to generate risk engines that could help predict which normoglycemic subjects are likely to experience glycemic progression. Importantly, exploitation of these predictors could inform the future development of novel, refined, and targeted interventions for the reversal prediabetes/early dysglycemia and restoration of NGR.
Footnotes
Authors’ contributions
SD-J designed and created outline of this review and edited and finalized drafts produced by AS.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SD-J is supported, in part, by Grant R01 DK067269 from the National Institutes of Health.