
Abstract
Despite the relative frequency of both bleeding and clotting disorders among patients treated in the neonatal intensive care unit, few clear guidelines exist for treatment of neonatal coagulopathies. The study and treatment of neonatal coagulopathies are complicated by the distinct hemostatic balance and clotting components present during this developmental stage as well as the relative scarcity of studies specific to this age group. This mini-review examines the current understanding of neonatal hemostatic balance and treatment of neonatal coagulopathies, with particular emphasis on emerging treatment methods and areas in need of further investigative efforts.
Impact statement
This mini-review provides a summary of recent as-yet unreviewed developments in the understanding of neonatal hemostasis, as well as standard-of-care and new treatments for many coagulopathies that present during the newborn period.
Introduction
The neonatal period presents a unique challenge for the clinician tasked with the care and management of hemostatic instability. During their first 30 days, infants may present with hemostatic irregularities related to a variety of etiologies: inborn errors of hemostasis, acquired thrombotic or hemorrhagic states, and imbalances of hemostasis secondary to another disease process or medical intervention. While the overall incidence of these problems is quite low in the general population, these disease processes present more frequently within the neonatal intensive care unit and a thorough understanding of their diagnosis and treatment is a clear expectation for any clinician working in the Neonatal Intensive Care Unit. 1 The treatment of such neonates is further complicated by the fact that while the neonatal hemostatic system is balanced, many elements are in different proportions than are found in the mature hemostatic system. As such, their diagnosis and treatment often deviate from the treatment of these same disease processes when they occur in the adult population. As our clinical and basic science understanding of the neonatal coagulation cascade deepens, the door opens to innovative new approaches to treatment of these diseases. As such, the object of this mini-review is to discuss developments in the understanding and treatment of neonatal coagulopathies, with particular emphasis on highlighting emerging treatment methods and areas in need of further investigative efforts.
Hemostasis in the newborn
Hemostasis in neonatal and pediatric populations has been understood to be distinct from adult hemostasis as early as the 1980s following the work of Andrew et al. to demonstrate the evolution of the hemostatic balance set point over the course of the infant and childhood periods.2–4 It has since been repeatedly validated that hemostasis changes from the neonatal period through childhood, with the most significant transformations occurring within the first year. 5 The unique and quickly evolving hemostatic balance that characterizes the newborn period results in increased difficulty in applying typical coagulation testing to aid in the diagnosis of coagulopathies. In 2016, a multicenter study by Toulon et al. showed no statistically significant change in prothrombin time (PT) over different age groups; however, both partial thromboplastin time (PTT) and activated partial thromboplastin time (aPTT) were significantly increased during the newborn period and overall highly dependent on age. 5 However, as this study did not measure any samples from neonates under two weeks old, it is difficult to determine the ranges’ accuracy in diagnosis of coagulopathy within the first half of the newborn period, especially considering that normal hemostatic values during this time exhibit significantly increased variability.6–8
While primary hemostasis in the newborn has suffered from less investigative effort, platelet counts are generally normal to elevated at birth and temporarily increase before reaching normal levels around one year old. 9 During this time, platelets are hyporeactive, and intraclot thrombin levels are significantly reduced, but bleeding time (BT) and platelet closure time (PFA-100) have been shown to be significantly reduced, although rate of clot growth is unaffected.9–11 Differences in platelet activity may result from reduced alpha-adrenergic receptors on the platelet plasma membrane in this population, which has been shown to lead to diminished aggregative response. 12 Additionally, the activation of the coagulation cascade that occurs during birth leads to elevated D-dimer levels that endure for at least three days but are indicative of no thrombotic irregularity in the newborn. 13 As such, it remains the case that diagnostic coagulation tests that are extremely useful in adult populations (BT, PFA-100, PTT, aPTT, D-Dimer) are of little use for diagnosis in the neonatal population. Viscoelastic tests, namely thromboelastometry and thromboelastography, provide a promising alternative, as they provide information about the clotting potential of whole blood rather than focusing on individual factor levels. More data are needed, however, to determine rigorous reference values in the neonatal population. 14
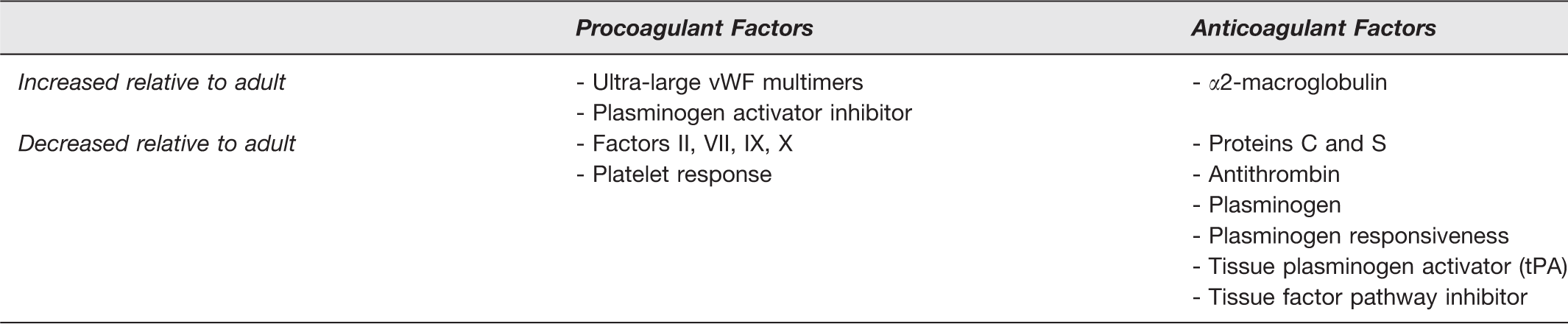
During the newborn period, many clotting factors are present in different concentrations than are present in normal adult blood (Figure 1, Table 1). During the first weeks of life, the newborn exhibits lower levels of the anticoagulants Protein C, Protein S, and antithrombin; however, it counteracts this in part with higher levels of the thrombin inhibitor α2-macroglobulin. 15 Neonatal hemostasis is balanced by having concurrent lower levels of the vitamin K-dependent pro-coagulant factors, II, VII, IX, and X (Figure 1). This is partially counterbalanced by higher levels of von Willebrand factor and ultra-large von Willebrand factor multimers. Low levels of many clotting factors during the neonatal period can be traced back to the immaturity of the fetal liver, which has reduced ability to provide the γ-carboxylation needed to produce the vitamin K-dependent factors, thereby creating a bottleneck for their production. 16 Additionally, newborns have 25–50% less α2-antiplasmin than is found in healthy adults, and their plasminogen is more difficult to convert to plasmin in the presence of tissue plasminogen activator. 17 It is frequently posited that the differences noted in neonatal hemostasis might provide a protective mechanism to reduce the likelihood of thrombosis or bleeding during this time period; however, more research is needed to validate this idea. 9 Most hemostatic factors can be expected to achieve adult levels and relative balance by age six months to one year. 18

Neonatal hemostasis. Factors that differ in concentration from adult values leading to either anticoagulant effects or pro-coagulant effects are encircled in red or teal, respectively. Figure created using BioRender.com. (A color version of this figure is available in the online journal.)
Hemostatic factors that demonstrate difference in concentration during the neonatal period.
The relative lack of anticoagulant factors during the newborn period, as compared to adult blood, is generally accepted as putting neonates at higher risk for acquired thrombotic states, particularly in the setting of extensive medical intervention in the sick neonate. While balanced, the low levels of many components lead to a much more fragile system than the balance achieved through the higher adult levels. It is likely that the differences noted between adult, child, and neonatal responses to anticoagulant medications derive from the differences described here, but more research is needed to validate this conclusion. Moreover, the relative scarcity of robust clinical data comparing treatment outcomes for diseases of hemostatic balance in the neonatal population means that almost all treatment guidelines from the American College of Chest Physicians are only grade 2 C, indicating a weak recommendation (risk-benefit assessment uncertain) based on low-quality evidence (observational studies, case studies, or clinical studies with serious flaws).19,20 As such, it becomes especially important for the clinician to have a robust understanding of the breadth of treatment options available and the relative pros and cons of any treatment choices in this population, and emerging technologies have the potential to have a large impact on treatment protocols in the near future.
In addition to differences in levels of clotting factors, the existence of neonatal-specific forms of clotting proteins has been described. Arguably the most notable of these age-specific clotting proteins is an immature form of fibrinogen, which has differing phosphorous and sialic acid content than adult fibrinogen. 21 The structural distinction between neonatal and adult fibrinogen lends unique properties to the respective clots they form.22,23 Clots formed using adult fibrinogen display high fiber density, a large amount of fiber branching, and significant three-dimensional structure. Clots formed from neonatal fibrinogen display increased porosity and are dominated by aligned fibers, ultimately forming sheet-like, two-dimensional clots (Figure 2). 22 Clots formed from neonatal fibrinogen display a significantly faster degradation rate than their adult fibrinogen counterparts, suggesting that the difference in neonatal fibrinogen structure makes these clots more sensitive to fibrinolysis (Figure 2). 22 Furthermore, isolated neonatal fibrinogen samples demonstrate significantly lower clottability. 23 The differences in clot structure indicate that differences in fibrinogen structure may lead to differences in polymerization, with neonatal fibrinogen preferring elongation over branching; however, further molecular investigation of fibrinogen polymerization is indicated for validation of these hypotheses. 22 Further investigation is warranted to determine the age-dependency and process of switching from synthesis of neonatal-type fibrinogen to synthesis of adult-type fibrinogen.
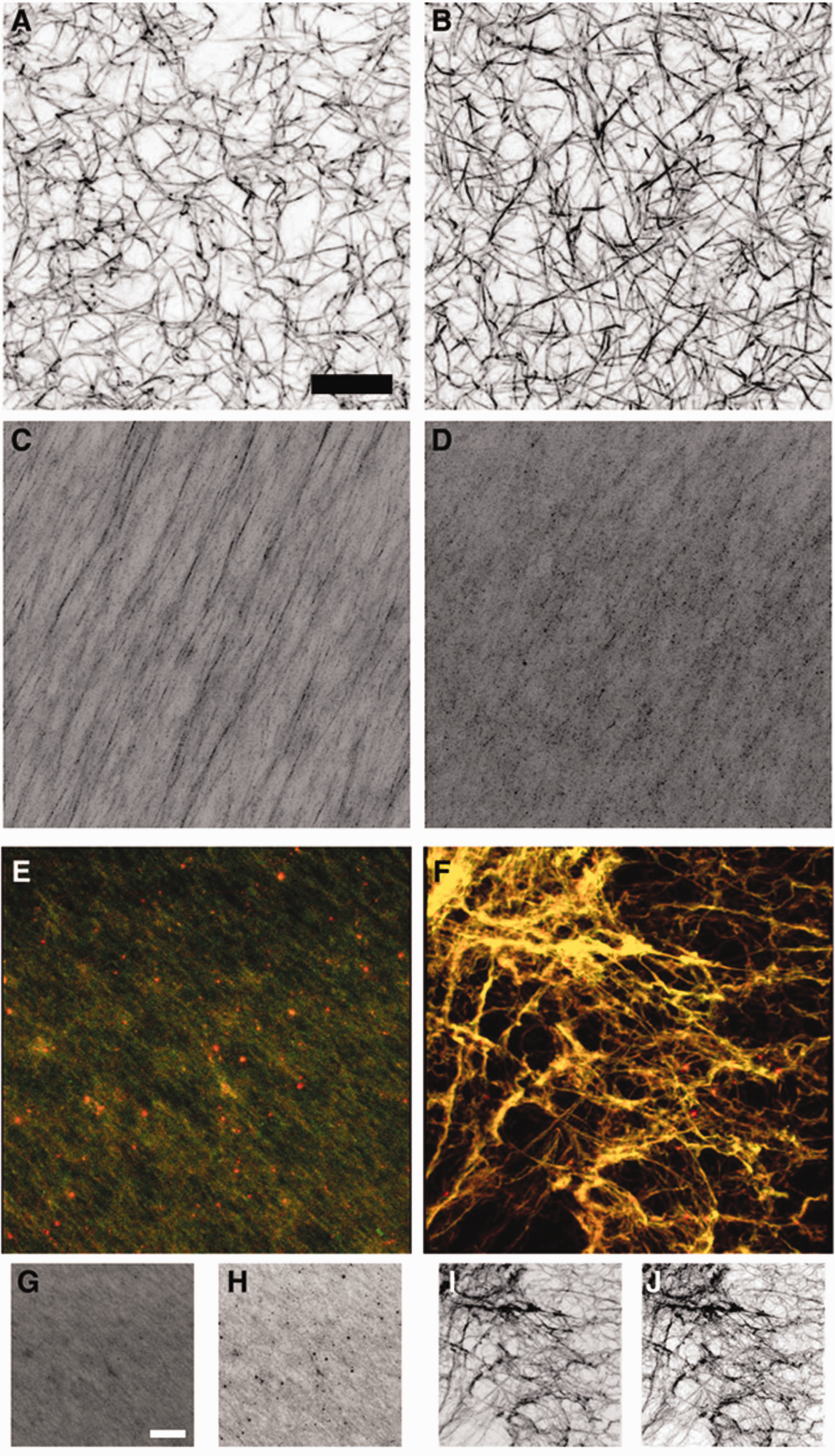
Confocal microscopy images of clots constructed from purified neonatal and adult fibrinogen. Clots formed from purified adult (a, b) or neonatal (c, d) fibrinogen at a concentration of 2.5 (a, c) or 3.5 mg/mL (b, d) fibrinogen in the presence of 10 μg/mL thrombin. Clots formed by combining neonatal and adult fibrinogen in a 2.5:1 (e, g, h) or 1:2.5 (f, i, j) ratio. Neonatal fibrinogen was labeled with Alexa-Flour 488 (green) to allow for separate visualization of adult and neonatal fibrinogen labeled with Alexa-Flour 555 (red). Representative images are presented. For combined fibrinogen samples, overlaid neonatal and adult fibrinogen channels (e, f) and corresponding individual neonatal (g, i) and adult fibrinogen (h, j) channels are presented. Scale bar = 20 μm. Reprinted by permission from Wolters Kluwer Health, Inc.: [Anesthesiology]. (Brown AC, Hannan RH, Timmins LH, Fernandez JD, Barker TH, Guzzetta NA. Fibrin Network Changes in Neonates after Cardiopulmonary Bypass. Anesthesiology 2016;124:1021–31). (A color version of this figure is available in the online journal.)
Hereditary factor deficiencies
While there are numerous inherited hemostatic diseases, some may first present during the neonatal period. Their treatment is relatively well described, although new treatment techniques continue to be discovered. Of note, only 10% of inherited coagulopathies first present before the end of the neonatal period, 1 meaning that treatment approaches during this time period are likely to center around only the most severe cases of only certain coagulopathies. The following sections will discuss treatments for hereditary coagulopathies that may present during the neonatal period.
Congenital protein C/protein S deficiency
This inherited disease may be treated with fresh frozen plasma (FFP), which is often the first line of treatment for the symptomatic neonate. Dosage is recommended at 20 mL/kg every 6 to 12 h until patient stability is achieved (i.e. all skin, ocular and CNS defects have returned to normal) and Protein C activity remains above 10 IU/dL. 24 Protein C concentrate (Ceprotin) may also be used as an intervention, but further comparative trials are needed to evaluate whether it is more effective than FFP, which is much easier to source.
Hemophilias
Hemophilia A (congenital factor VIII deficiency) and hemophilia B (congenital factor IX deficiency) are both most commonly diagnosed during the neonatal period, with hemophilia A patients more likely to be symptomatic during this time period due to the increased severity of their disease process. 25 Treatment of both of these factor deficiencies centers around replacement of their respective missing factors, and treatment of the symptomatic newborn with FFP (15–20 mL/kg) should proceed without waiting for imaging confirmation of ongoing bleed. Neonates are likely to require increased doses of replacement factors with greater frequency than adults. 26 Recombinant factors (rFVIII: Helixate FS, Advate, Kogenate FS, Xyntha; rFIX: beneFIX) have a lower associated risk of viral or bacterial communication, and therefore have been classically favored for treatment when possible; however, plasma-derived factor VIII concentrates (Humate-P, Alphanate, and Wilate) and factor IX concentrate (Alphanine) do exist and have been used when no recombinant factors are readily available. Patients may develop antibodies (known as inhibitors) to transfused factors over time, leading to the necessity of increased doses to provide effective treatment, and eventual failure of infusions of any dose to provide treatment. According to the SIPPET trial (conducted 2010–2014), hemophilia A patients treated with concentrates have lower rates of inhibitor development later on in life than those treated with recombinant factors. 27 Of particular note in treatment of neonatal populations, treatment with recombinant factors at a younger age or larger delivered volume during early treatments were both associated with increased likelihood of eventual inhibitor development. 26 As such, this consideration must be weighed against the small possibility of infectious disease communication, particularly in the treatment of neonates presenting with severe bleeds for which they will require significant factor transfusion. Cryoprecipitate should only be used in case of emergency when nothing else is available, as it does not contain factor IX.
Current innovation in the treatment of hemophilia focuses on avoidance of inhibitor production and the possibility of curative treatments. In a clinical trial of 10 adult patients with severe Hemophilia B, Nathwani et al. demonstrated that the use of gene therapy via a single dose facilitated by novel adeno-associated virus type 8 (AAV8) resulted in significant increase in factor IX levels and clinical improvement over a median period of 3.2 years, without toxic effect. 28 From this success, Iizuka et al. have demonstrated the success of gene therapy during the neonatal and infant periods in treating hemophilia B in mice. 29 By using a novel adenovirus vector (Ad-E4-122aT-AHAFIX), they were able to greatly improve vector efficiency and, using sequential injections, successfully address bleeding in a hemophilia B mouse model. 28 The newborn period is of particular interest for gene therapy treatment because while greater than 50% of hemophiliacs first present during this time, patients have not yet had sufficient viral exposure to build up immune responses that would impede the success of the viral vectors. 28 Although currently only in animal trials, this emerging treatment holds much promise for improved patient outcomes. As hemophilias result from variations in a single gene, cell-based approaches also hold promise for their treatment. Recent in vivo animal studies by Gao et al. achieved successful intramuscular engraftment of therapeutic cells in mice, and these cells were shown to express FVIII. 30 Importantly, cellular and genetic approaches avoid the possibility of long-term health effects from traumatic bleeds during infancy and childhood, allowing patients to lead lives requiring less medical intervention.
Von Willebrand disease
Von Willebrand disease can be caused by lower levels of vWF (types 1 and 3) or malformed vWF (type 2). Type 3 (complete lack of vWF) and some type 2 patients first present symptomatically during the neonatal period. Successful treatment is well-described in the literature with either plasma-derived or recombinant von Willebrand factor concentrate.16,31 The factor VIII concentrates Humate-P, Alphanate, and Wilate also contain von Willebrand factor, and are therefore useful in the treatment of von Willebrand disease.
Rare bleeding disorders
Rare bleeding disorders include disorders of platelet function and deficiencies of factors V, VII, X, XI, and XIII. 16 These hereditary disorders are associated with consanguinity and usually only present during the neonatal period when they are severe. Treatment is centered around replacement with recombinant factor concentrates or FFP when concentrates are not available. Further discussion of risks and benefits of transfusion with factor concentrates and adult blood products may be found later under the section “Cardiopulmonary Bypass and Transfusion-Induced Coagulopathy.”
Congenital thrombocytopenias
Thrombocytopenia is a factor in a number of congenital diseases and syndromes, such as Fanconi Anemia, Thrombocytopenia Absent Radius, and Glanzmann’s Thrombasthenia, among others. 32 Thrombocytopenia in these syndromes may be the result of underproduction of platelets or normal production of nonviable platelets. 33 As with any other neonate presenting with severe thrombocytopenia, platelet transfusion may be used as one part of a larger treatment protocol; however, discussion of specific treatment protocols for very rare congenital syndromes and diseases lies beyond the scope of this mini-review. Further discussion of risk-benefit analysis related to platelet transfusion in neonates may be found later under the section “Other Acquired Thrombocytopenias.”
Congenital vascular disorders
Hemangiomas and vascular malformations put neonates at increased bleeding risk due to rupture of the structure (as in congenital aneurysms) or through the sequestration of platelets in the structure leading to hemostatic imbalance and thrombosis within the structure or secondary bleeds. Kasabach–Merritt phenomenon, associated with 70% of all kaposiform hemangioendotheliomas and occasionally with tufted angiomas, is a rare coagulopathy resulting in consumption of platelets and fibrinogen. 34 It is caused by the trapping of platelets and localized consumption of fibrinogen within the body of a vascular tumor. These patients should only be given platelet transfusions in the context of intra- or post-operative bleeding, otherwise these transfusions may instigate further platelet trapping and tumor growth. 34 Similarly, cryoprecipitate and packed red blood cells (pRBCs) should also be transfused judiciously. Heparin should not be administered to these patients due to the risk of aneurysm and bleed from the tumor. 34 Ultimately, due to the rarity and complexity of this condition, treatment protocols vary greatly.35,36
Acquired diseases of hemostasis
Vitamin K deficiency bleeding (hemorrhagic disease of the newborn)
Due to the advent of routine neonatal vitamin K administration, bleeding due to insufficiency in vitamin K-dependent clotting factors (factors II, VII, IX, and X) has been brought from an estimated incidence of 1–2% to a rare occurrence today. 37 Guidelines for such administration include intramuscular administration (usually by heel stick) of 0.5 or 1 mg (dependent on birthweight) to all neonates within 6 h of birth, while still maintaining appropriate time for familial bonding with the child. 38 Oral prophylactic vitamin K treatment has been pursued as an alternative to intramuscular vitamin K, due to the possibility of emotional trauma for both the neonate and parents, but it was found to be associated with a significant increase in the occurrence of late hemolytic disease of the newborn (occurring at three to eight weeks of age rather than within first five days of life) when compared with standard prophylactic treatment in epidemiologic studies in Germany, Britain, Australia, and Sweden. 38 However, 2 mg of oral vitamin K at the first time of nursing, with repeated oral doses at two to four and six to eight weeks old, should be recommended for neonates whose parents refuse an intramuscular injection. 38 Although rare due to successful implementation of near-universal prophylactic treatment in the hospital setting, bleeding due to vitamin K deficiency may still occur in the setting of limited prenatal care or following maternal medication use (anticonvulsants, rifampin, isoniazid). 1 Treatment with vitamin K should be initiated emergently.
Neonatal alloimmune thrombocytopenia
NAIT may be thought of as an analog of hemolytic disease of the newborn that affects the platelets rather than RBCs. Platelet surface antibodies precipitate an immune response in the carrying parent, leading to thrombocytopenia and bleeding in the neonate. Although relatively rare, NAIT remains the leading cause of severe thrombocytopenia in neonates. 39 Unlike HDN, NAIT may occur during a first pregnancy and is usually characterized by a mild disease course, but may still cause intracranial hemorrhage and long-term disability in severe cases. 39 Of the 24 different human platelet-specific alloantigens (HPAs) that have been identified, HPA-1a (75–80% of cases) and HPA-5b (10–15% of cases) are the most likely to trigger the formation of NAIT-provoking antibodies. 39 Current treatment emphasizes maintenance of fetal platelet levels above 30,000 through the use of transfusions of maternal platelets that have been washed to remove antibodies, or pooled HPA-1a negative random donor platelets. 39 As only 1–2% of the population is HPA-1a negative, finding sufficient random donor platelets in an emergent situation may not be practical, and it may be appropriate to transfuse random donor platelets along with intravenous IgG. 39
Other acquired thrombocytopenias
Acquired thrombocytopenias (platelet count <150 × 109/L) comprise the most common class of neonatal bleeding disorder, affecting 1–5% of newborns at birth, and 18–35% of NICU patients.40,41 Furthermore, 6% of term neonates and 8% of preterm neonates are at risk for severe thrombocytopenia (platelet count <50 × 109/L). 33 Low-platelet counts may stem from either lowered platelet production or platelet overconsumption. Problems of lowered platelet production are associated with sepsis, congenital infections (toxoplasmosis, rubella, cytomegalovirus, and herpes simplex, among others), NAIT, and maternal drug exposures. 1 Diseases of platelet consumption include maternal autoimmune diseases (e.g. idiopathic thrombocytopenic purpura, lupus), heparin-induced thrombocytopenia, shock, maternal drug exposures, with thiazide diuretics being among the most common. 1 Regardless of cause, treatment involves addressing the underlying trigger and, frequently, platelet transfusion.
While platelet transfusion remains the only specific treatment for neonatal thrombocytopenia, there is significant disagreement as to what platelet levels warrant transfusion in a neonate, especially considering that severity of thrombocytopenia has low correlation with severity of bleeding risk.41,42 The lack of studies investigating efficacy of platelet transfusion in neonates has resulted in a lack of clear evidence-based guidelines. Furthermore, a multi-institutional study of transfusions in children indicated that of all blood products, platelet transfusions were linked to the highest rate of complications. 43 As such, the decision to transfuse platelets is left to clinical judgment, weighing an as-of-yet unquantified potential benefit against the risks associated with blood product transfusion (immune reaction, infectious disease transmission).
Disseminated intravascular coagulation
DIC, characterized by depletion of both pro- and anti-coagulant factors as well as platelets, is of particular concern for seriously ill neonates due to their low total blood volume. While sepsis remains the most common cause, many other disease processes may lead to DIC and resultant massive hemorrhage. Standard-of-care treatment emphasizes resolution of the underlying causative agent or disease, supplemented with administration of FFP or cryoprecipitate to replenish overconsumed clotting factors. 44 Of note, FFP transfusion is only recommended for treatment of active bleeding and has not shown any benefit when transfused based on coagulation studies alone. 45 Despite these guidelines, a multicenter study showed that 63% of transfusions in neonates were undertaken prophylactically when no bleeding was present. 45 In severe cases, recombinant activated factor VII may also be used. 46
Iatrogenic diseases of hemostasis
Catheter-related thrombosis
Catheter-related thrombosis is caused by multiple factors at play during intravenous and intraarterial line placement: endothelial damage and inflammation, introduction of turbulent blood flow, and the introduction of a foreign body. Additionally, bacteria may adhere if a fibrin sheath forms around the catheter, leading to further inflammatory response and thrombus growth. 16 CRT most frequently occurs in the deep venous system, including the superior and inferior vena cava. 47 Central lines are the leading cause of thrombosis among neonates, with widely varying estimates of incidence rates (as low as 1% up to 65%). 48 Thrombosis is most commonly noted in the inferior vena cava, right atrium, or hepatic vein. 49 Importantly, continuous heparin infusion through a central line is standard practice to maintain patency but its effects on thrombotic potential remain unclear. 49 Pretreatment with unfractionated heparin, diligent central line care, and adjustment of line placement protocols have had a significant reductive effect on incidence of CRT. Of note, due to their lower antithrombin levels and the heightened rate of removal from circulation, neonates require higher doses of unfractionated heparin than either adults or older children to successfully reach therapeutic range. General practice recommends an initial does of 75–100 U/kg followed by ongoing anticoagulation with 28 U/kg/h. 20
Once established, CRT is best addressed with therapeutic anticoagulation followed by prophylactic anticoagulation until catheter removal is indicated (if not already removed because of loss of functionality). Management of CRT varies between hospitals due to a lack of clear evidence-based guidelines; however, treatment generally follows the following standard-of-care, and this may be further complicated by the known association between catheter-associated blood stream infections and CRT among neonates. 47 Before anticoagulation treatment initiation, FFP should be administered to supplement naturally lower plasminogen levels during the newborn period. These lower plasminogen levels have been demonstrated to impact the efficacy of medical thrombolytics. Fibrinolysis with recombinant tissue plasminogen activator (rtPA) is recommended in pediatric populations due to its efficacy; in particular, rtPA formulations with a short half-life are preferred. 50 If catheter removal is indicated, pretreatment should be undergone with therapeutic anticoagulation for three to five days. 51 Therapeutic anticoagulation should continue for 5–7 days for arterial thrombi, and 6–12 weeks for catheters that remain functional. 20 The ongoing NEOCLOT multicenter prospective study in the Netherlands presents a critical step in determining evidence-based guidelines, as it examines the safety and efficacy of their national guidelines for CRT management and will result in the most comprehensive data on neonatal CRT management to date. 52
Extracorporeal membrane oxygenation
ECMO is a form of supportive therapy that provides temporary assistance to the function of the heart and lungs by passing blood through an artificial circuit wherein venous blood is removed, pressurized, oxygenated, and finally returned to the arterial circulation. Of note, ECMO is not in and of itself an intervention, but rather a temporary measure enacted while medical or surgical interventions are provided. The extensive interface between patient blood and machine tubing involved in ECMO leads to activation of the clotting cascade and inflammatory response; however, the changes precipitated in the hemostatic balance are not well characterized. 53 Even with the standard-of-care use of continuous infusion of unfractionated heparin as systemic anticoagulation during ECMO, one study showed that 17% of pediatric patients develop a clot within the device. 54 New tubing systems for ECMO devices with intrinsic anticoagulation (nitric oxide, unfractionated heparin, and direct thrombin inhibitors) are in various stages of development and use; however, none of them eschew the need for systemic anticoagulation.53,55
The use of systemic anticoagulation also introduces bleeding as a concern. According to summary statistics from 2009 to 2015, 11% of neonatal patients developed an intracranial hemorrhage during or after ECMO. 56 In another study, bleeding complications occurred in 33% of patients and thrombotic complications occurred in 29%. 57 While the neonatal share of total ECMO usage has gone down in recent years, up to 30–40% of pediatric ECMO patients die as a result of a thrombotic or hemorrhagic state, with bleeding complications significantly increasing the likelihood of mortality.53,58,59 As heparin works by amplifying the effects of antithrombin III (ATIII) and low ATIII levels have been associated with ECMO administration, current ELSO guidelines recommend the supplementation of low ATIII levels in the context of heparin resistance. 60 More investigation is needed, however, to determine rigorous methods for diagnosing heparin resistance, considering the aforementioned differences in most clotting tests in this age group. 60 Until recently, supplementation for low ATIII levels—regardless of heparin resistance—was standard-of-care in many hospitals. Work by Niebler et al. and Byrnes et al. indicated that ATIII activity was heightened for 24 h after administration, with no signs of increased bleeding or significant effect on heparin dose, infusion rate, or ACT, with Byrnes et al. further concluding that ATIII administration led to an increase in ECMO circuit failure.61,62 Furthermore, research is warranted to better characterize the age-dependent characteristics of heparin activity, as guidelines currently vary between institutions and are not rigorously evidence-based due to a lack of data. 53
Cardiopulmonary bypass and transfusion-induced coagulopathy
Cardiopulmonary bypass (CPB) is a crucial element of surgical intervention in the treatment of inborn structural heart disease; however, it is also a source of significant hemostatic destabilization. While there has been relatively little investigation into the effects of CPB on neonatal hemostasis, 63 its interaction with the coagulation cascade appears to be multifactorial. Hemodilution from the CPB prime, platelet inactivation, loss of von Willebrand factor receptors and fibrinogen receptors, extensive suture lines, activation of clotting through blood contact with man-made surfaces in the bypass unit, and release of inflammatory mediators all contribute to the increased risk of coagulopathy, which is known to continue for at least three days postoperatively. 64
Current standard of care for treatment of post-operative bleeding (and bleeding resultant from other etiologies) includes transfusion of adult blood products (packed red blood cells, platelets, cryoprecipitate, and fresh frozen plasma).64–66 However, the efficacy and safety of many of these treatments are called into question by recent work providing evidence that increased intraoperative blood product transfusion in neonates is associated with increased severity of the procoagulant profile upon ICU admission and increased likelihood of thrombotic events. 67 These findings strongly support the need for further systematic validation of the efficacy of transfusion of adult blood products in this population to warrant the risks associated with their transfusion.
Fresh frozen plasma is insufficiently potent to be useful in the restoration of fibrinogen levels in the hemorrhagic neonate. Additionally, it suffers from inconsistent concentration due to natural human variability, risk of infectious disease spread, and the inefficiencies associated with thawing, cross-typing, and matching frozen blood products. 23 Cryoprecipitate is more effective for this use case, but it suffers from the same disadvantages as FFP transfusion. 23 Moreover, Brown et al. demonstrated that when clots are formed from a mixture of adult fibrinogen and neonatal fibrinogen, the resultant clots are structurally and functionally different from clots made using solely neonatal fibrinogen. This mixture of the two types of fibrinogen provides an ex vivo simulation of the effects of cryoprecipitate administration on clot properties in newborns. These clots using mixed-source fibrinogen demonstrated characteristics somewhere between the adult and neonatal clot architectures described earlier, with the dominant volume determining the overall dominant clot structure. This likely indicates that the two subpopulations of fibrinogen do not fully integrate during clot formation. 22 Regardless of the proportions of fibrinogen types, all mixed-source clots demonstrated significantly slower degradation times. 22 This may provide insight into the increased risk of post-operative thrombosis among neonatal surgical patients.22,68 While not representative of all relevant complexities present in vivo, this investigation demonstrates compelling evidence for the root causes of decreased efficacy of adult blood products in neonatal patients and emphasizes the importance of developing treatments that improve native neonatal fibrin networks in CPB patients rather than attempting to replace them with adult fibrin networks.
Further work by Nellenbach and Brown et al. investigates the use of procoagulant agents that stimulate endogenous fibrin activity as rescue agents for treatment of post-CPB hemorrhage in neonatal patients. 69 This investigation focused on recombinant-activated factor VII (rFVIIa) and factor eight inhibitor bypassing activity (FEIBA; Shire US Inc., Lexington, MA, USA), which is comprised of mostly FVIIa with a small amount of FXa. 70 This ex vivo study determined that clots made using neonatal plasma collected post-CPB in conjunction with relevant of doses of FEIBA or rFVIIa demonstrated clot structure and degradation rates more closely resembling baseline neonatal clot characteristics than clots formed in the presence of cryoprecipitate. 70 A review of six trials using prothrombin complex concentrates (PCCs) to treat bleeding in children under one year old determined that PCCs were effective for use as treatment for patients with known coagulation factor deficiencies who present with bleeding, but evidence was too weak to support further applications. 71 A retrospective study of hemorrhagic neonates treated with rFVIIa demonstrated a statistically significant improvement in PT, aPTT, and fibrinogen content, without evidence of safety risks to treated patients. 72 Taken together, these results support the importance of further in vivo investigation of prothrombin complex concentrates and rFVIIa as safer and more effective potential alternatives to adult blood products for neonates. Many new treatments for hemostatic disruption as a result of CPB, both preventative and diagnostic, are promising but require additional validation. The off-label use of fibrinogen concentrate (RiaSTAP) to replete fibrinogen post-CPB has gained traction in the clinical setting, but this treatment (made from pooled human plasma) still represents the transfusion of adult fibrinogen that may not be compatible with neonatal hemostasis. 23 Ex vivo studies using both human samples and a validated porcine model of age-dependent neonatal fibrinogen characteristics have shown the fibrin network-strengthening properties of treatment with factor VII, factor eight inhibitor bypassing activity, RiaSTAP, and platelet-like particles. 23 The use of platelet-like particles had the additional effect of significantly increasing fiber density within formed clots. 23
Recent studies in adults investigated pre-treatment with high doses of methylprednisolone, which appears to decrease blood loss post-operatively; however, it remains unknown how this might interact with the neonatal hemostatic balance. 73 The use of lysine analog antifibrinolytics (e.g. tranexamic acid) to treat post-operative hemorrhage has been validated in adult populations, 74 as has the use of direct factor Xa inhibitors to address thrombotic states. In a clinical case series, recombinant-activated factor VII (two IV doses of 180 μg/kg two hours apart) was successfully used to return post-operatively hemorrhagic neonates to hemostatic balance; however, these results require further validation as the sample size was small and rVII has the potential to create dangerous hypercoagulable states. 75 New biomaterial coatings for CPB systems are also showing promising results in the effort to diminish the effects of blood interaction with nonvascular surfaces.
Summary and conclusions
Many different disease states and medical interventions may provoke bleeding or thrombosis in neonates due to their fragile hemostatic balance. However, in spite of their clear clinical significance, neonatal coagulopathies suffer from a lack of robust treatment guidelines. This is partly due to the fact that neonatal hemostasis is distinct from both adult and pediatric hemostasis, meaning that excellent studies in these groups do not necessarily provide information that is generalizable to the treatment of neonates. Recently, however, both clinical and ex vivo studies have led to significant developments in our understanding of neonatal hemostatic balance and differences in neonatal fibrinogen and clot structure. Many new approaches are emerging for the treatment of neonatal coagulopathies. On the other hand, the efficacy of many standard-of-care treatments, particularly transfusions of adult blood products, has recently been called into question. The rapid developments in this area, in conjunction with a lack of clear guidelines, leave much more responsibility in the hands of the practicing clinician to weigh the risks and benefits of different treatments on a case-by-case basis rather than simply being able to follow predetermined recommendations (Table 2). As such, it is of particular importance to remain up to date on emerging treatments and studies.
An overview of the use of blood products in the treatment of neonatal coagulopathies.
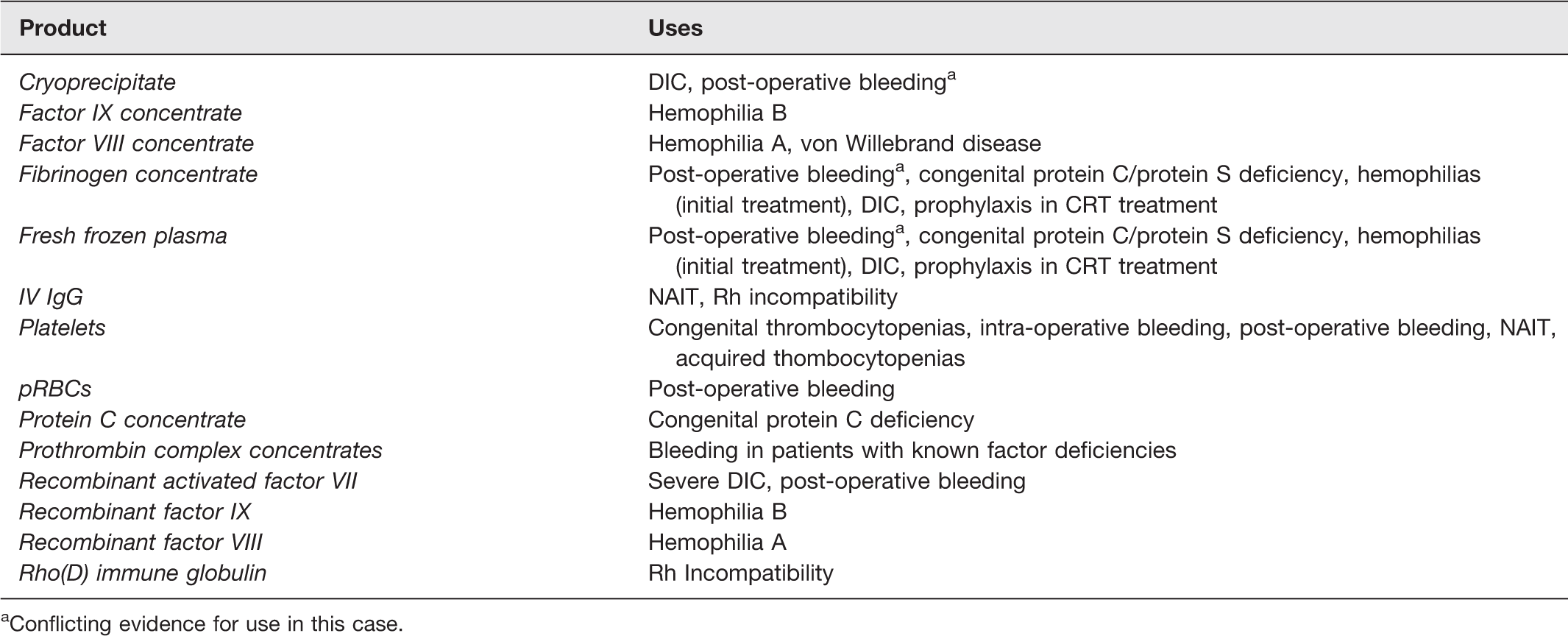
aConflicting evidence for use in this case.
Footnotes
AUTHORS’ CONTRIBUTIONS
NM and ACB wrote and edited the manuscript.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by CDMRP W81XWH-15–1-0485 from the U.S. Department of Defense (Washington, D.C.) and NIH NHLBI 1R01HL146701-01A1 from the National Institutes of Health (Bethesda, Maryland).