
Abstract
COVID-19 disease has been a problem in today’s society, which has worldwide effects on different areas, especially on the economy; also, from a health perspective, the disease affects the daily life quality. Physical activity is one major positive factor with regard to enhancing life quality, as it can improve the whole psychological, social, and physical health conditions. Current measures such as social distancing are focused on preventing the viral spread. However, the consequences on other areas are yet to be investigated. Elderly, people with chronic diseases, obese, and others benefit largely from exercise from the perspective of improved health, and preventive measures can drastically improve daily living. In this article, we elaborate the effects of exercise on the immune system and the possible strategies that can be implemented toward greater preventive potential.
Impact statement
This work encompasses a multidisciplinary approach toward current problems, as COVID-19 is a novel disease, and population heterogeneity shows different outcomes. The importance of systemic effects of exercise has been researched in various situations, and especially in populations that have high risk profile regarding COVID-19 outcome (e.g. individuals with comorbidities). There are no current guidelines on how to utilize exercise during the pandemic, and what type or form of exercise might be stated as safe to implement. The current worldwide measures do not utilize the preventive potential of exercise at all, which might not be beneficial in population that have impaired health, and where exercise might show improvement (e.g. heart disease). This paper critically approaches the problem and its potential mechanisms and effects and gives an insight into the potential benefits of its possible implementation. A proper implementation might reduce overburdening of health system and improve the risk profile in population.
Introduction
The primary worldwide concern in 2020 and 2021 is the focus on a potentially severe acute respiratory disease that has spread from Wuhan, China, now known as the coronavirus disease 2019 (COVID-19). In December 2019, clusters of patients were admitted to the hospital with respiratory disease from unknown origin. 1 Pathophysiology of COVID-19 has been described by previous research, 2 , 3 and symptomatology may range from mild symptoms to severe pneumonia. 1 , 2 At this point, there are over 100 million confirmed cases of infection and over 2.5 million confirmed deaths globally and increasing (https://ourworldindata.org/covid-deaths).
Worldwide COVID-19 reactions included social distancing, movement restrictions, and in some countries, lockdowns. These measures, while necessary to control viral spread, have detrimental implications for daily physical activity, which is already being demonstrated in the literature.4–6 In parallel, leading organizations such as the American College of Sports Medicine (ACSM) support daily physical activity as an important lifestyle behavior for a wide variety of patients populations, including cardiovascular disease, arthritis, and diabetes (https://www.acsm.org/read-research/trending-topics-resource-pages/physical-activity-guidelines). The elderly people are particularly vulnerable to a sedentary lifestyle, and exercise has numerous benefits including improved quality of life, 7 improvement in cardiac index and pulmonary function which is especially beneficial in heart failure patients, 8 and is considered so far effective and safe treatment in preventing bone mineral density loss, but further research is needed. 9 In this context, measures taken during the COVID-19 pandemic to control viral spread are of clear concern with respect to physical activity patterns, with implications for reduced quality of life and increased risk for untoward health complications (Figure 1). The present paper elaborates on factors related to the impact of exercise on human physiology and health. 10 In particular, we review the evidence that indicates moderate physical activity as an important preventive strategy in reducing the severity of viral infections through its immunomodulatory and adaptative effects.
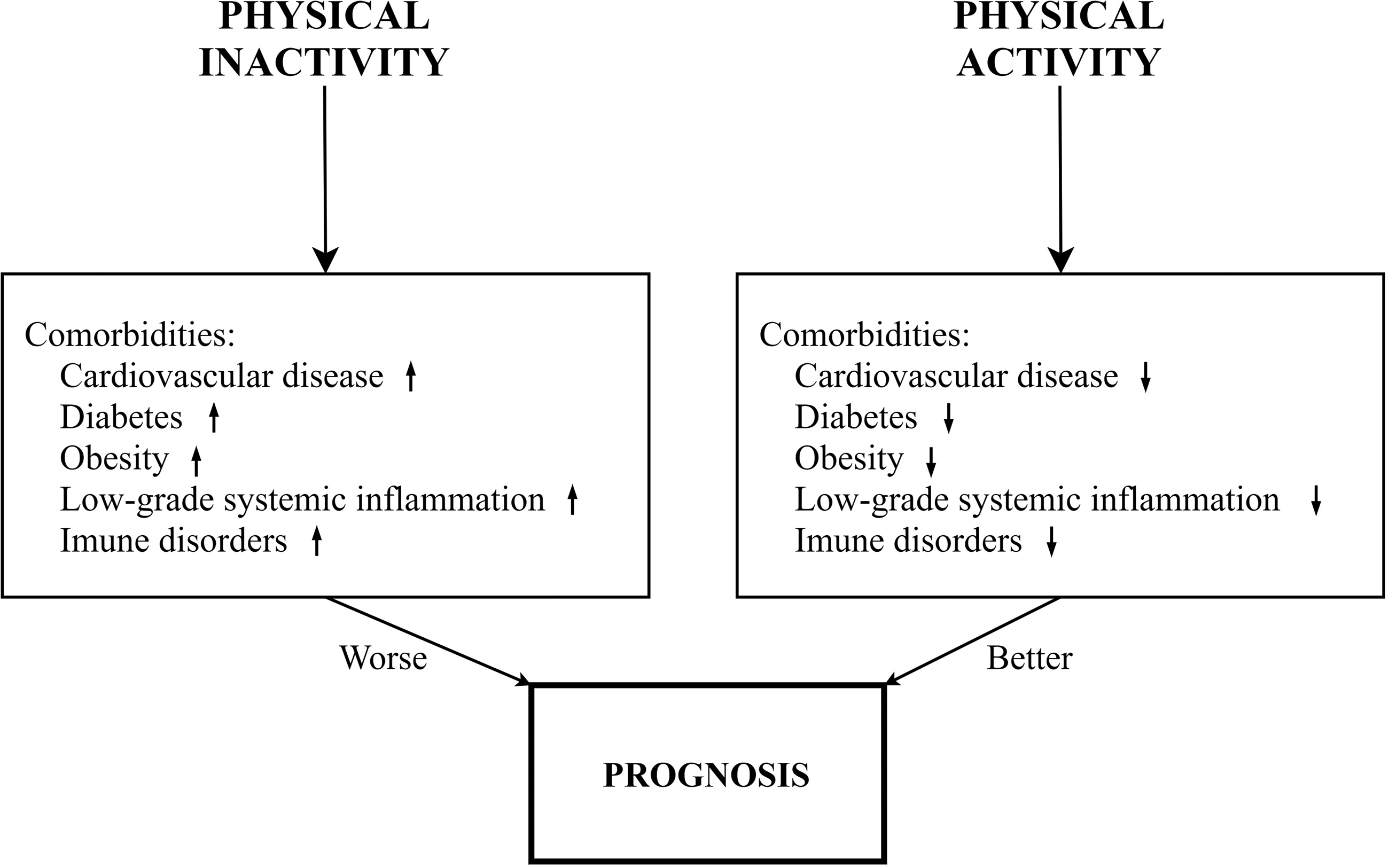
Relationship between comorbidities and physical activity as lifestyle intervention on COVID-19 prognosis.
Respiratory infections and exercise
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infects both the upper and lower respiratory tract; 2 , 11 , 12 we are only beginning to understand the connection between the severity of infection and patient outcomes, including the modulatory effects of physical activity and exercise.
It was stated that many of the studies that research the incidence of upper respiratory tract disease employ questionnaires and self-evaluation. 13 The incidence of acute respiratory infections between those who exercise and those who do not, indicate that more evidence is needed, given current data cannot definitively determine if exercise is effective in altering the occurrence of respiratory tract infections. 14 Moreover, not all respiratory diseases are infective, and future research should focus on the difference between allergies and those diseases which are infective. 13 It was thought that exercise decreases immune defense and provides an open window for respiratory infections, which has been proposed as a period where a person is most susceptible to infection. However, the converse seems to be true with respect to moderate intensity exercise training, 15 and that actually J-shaped curve, described by previous studies, might explain variations in the immune response with exercise where only those who chronically exercise at higher intensities and volumes (e.g. competitive athletes) may be at increased risk. 14
Carefully applied and planned exercise training has been shown to have positive effects in the prevention and treatment of obesity and diabetes, as well as reducing levels of inflammatory markers in people with low grade systemic inflammation. 10 , 16 , 17 In the context of COVID-19, individuals with chronic conditions and systemic inflammation have been identified to be at risk for poor outcomes with SARS-CoV-2 infection. 18
Studies have confirmed that there is high prevalence of obesity and chronic diseases in physically inactive/sedentary populations, 7 , 10 , 19 , 20 while in April WHO stated in their key facts that more than 1.9 billion people were obese (https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight). Currently, there is a surge of recommendations on how to be physically active and exercise during the COVID-19 pandemic, but they lack scientific evidence supporting the added benefits of physical activity and exercise in preventing SARS-CoV-2 infection, or, if an individual is infected, reducing severity of symptoms.
COVID-19 and immune response
It has been reported that, in severe cases, SARS-CoV-2 infection progresses in two steps. 2 First, SARS-CoV-2 infection spread leads to a destruction of lung cells, which triggers a local immune response. This is followed by an induction of acute respiratory distress syndrome (ARDS). ARDS is an inflammatory lung disorder that is connected to multiple organ system dysfunction, which potentially leads to systemic failure and death; mortality due to ARDS is high. 3
Major components of innate immunity are epithelial cells, macrophages, dendritic cells (DC) and natural killer cells (NK cells), all of which help to limit early viral spread. 21 Antigen presenting cells release cytokines and prime T and B cell immune response to resolve infection. This leads to series of reactions that in turn have a goal to remove the pathogen from the system. DC and macrophages phagocytize apoptotic cells which were previously infected by virus. 2 Previous research on the influenza virus indicates that apoptosis-dependent phagocytosis of virus-infected cells may lead to direct elimination of the pathogen and can also inhibit viral replication. 22 More research is needed to evaluate if a similar response exists with SARS-CoV-2 infection.
In mild cases of SARS-CoV-2 infection, the immune system can fend of the virus and the patient fully recovers. 2 However, in more severe cases, there is inadequate immune regulation and a dysfunctional immune response, which can cause severe lung and even systemic pathology. 2 , 3 Previous research conducted more than 10 years ago provides insight into the response of innate immunity in the lungs to SARS-CoV that can lead to cascade of severe lung tissue damage. 21 In more severe cases, cytokine storm, characterized as a massive release of proinflammatory cytokines, has been described to occur in COVID-19 cases, 2 , 3 which increases the risk for organ failure and subsequent death. 2
Data from previous studies indicate that both the virus and hyperinflammation, which is induced by an uncontrolled response of immune system, promote a much graver clinical scenario. 11 , 23 As such, treatments should target both the viral life cycle and the side-effects (such as cytokine storm) induced by SARS-CoV-2. 11 , 23 At this point, the exact factors that most significantly influence the path in disease progression and outcomes remain unclear.
The SARS-CoV-2 has a high affinity for angiotensin-converting enzyme 2 (ACE2) receptor which is the entry point for virus. 2 It is highly expressed on the apical side of lungs’ epithelial cells, 2 , 23 which are exposed to pathogens that we inhale. 21 Previous research suggests that ACE2 deficiency has been related to older age, hypertension, diabetes, and cardiovascular disease, which are conditions that are connected to severe complications with SARS-CoV-2 infection. 12
Besides ACE2 receptor, the cellular transmembrane serine protease 2 (TMPRSS2) enzyme is important for viral entry, since it is needed for priming the spike (S) protein of the virus. 11 , 12 As well as ACE2, TMPRSS2 gene is primarily expressed in bronchial cells. 11 Previous research indicates that membrane fusion with the virus leads to virus entry into the cell, and subsequent downregulation of this receptor. It is thought that this event promotes imbalance between the ACE→Angiotensin II→AT1 (ACE/AngII/AT1) and ACE2→Angiotensin1–7→Mas (ACE2/Ang(1–7)/Mas) receptor axis, favoring the ACE/AngII/AT1 receptor axis, and subsequently enhancing inflammatory process, which is thought to be a significant factor in patients with ACE2 deficiency. 12 Thus, the renin-angiotensin system (RAS) might be included in mechanisms that can lead to ARDS. 12
Severity of disease is shown to be related to concentration of IL-6 during the viral response, where overproduction of immune cells and cytokines occurs, especially of IL-6 and IL-8 which induce a surge of immune cells into lungs. 16 , 24 , 25 IL-6 is a proinflammatory cytokine that has multiple roles and is stimulated and produced by different types of cells, such as epithelial cells, macrophages, neutrophils, adipocytes, and muscle cells. It is one of the most widely studied cytokines, 26 and has an important role during the acute phase of a response to stress,27–29 and it has been shown that this cytokine can be used as an early marker of severe COVID-19 course. 27
Higher basal concentrations of IL-6 are related to higher concentration of body fat (BF). 26 , 30 In addition to obese individuals, a higher concentration of IL-6 is found in the elderly and those with chronic disease. 24 , 31 Production of IL-6 via adipocytes can increase basal concentration and may account for up to 35% of its total value. 32 , 33 Moreover, increased basal concentration of IL-6 has been linked to chronic low-grade systemic inflammation. 26
Previous research 19 dealing with obesity and chronic diseases showed that a high number of people will be at risk from the early start of infection due to high incidence of these factors in the global population. SARS-CoV-2 infection has a high prevalence of invasive mechanical ventilation use, which has been strongly associated with a higher body mass index. 34
The regulatory role of IL-6 can be explained by its influence on the hypothalamo–pituitary–adrenal (HPA) axis and cortisol stimulation. 34 HPA axis is activated after infection and leads to production of cortisol. Knowing that cortisol has an immunosuppressive effect, it would not be surprising that a dysregulated cortisol response occurs due to high basal concentration of IL-6, such as in chronic low-grade systemic inflammation. 31 ,35–39 This might affect disease progression, as the inflammatory balance becomes unregulated, which might be responsible for the occurrence of the cytokine storm syndrome. 2 , 3
IL-6 signals leukocytes, including neutrophils, to surge toward site of inflammation. Neutrophils might act there in two ways – eliminating virus but also inducing lung injury. 2 This might provide information on where to focus preventive strategies.
In patients with a severe clinical course following SARS-CoV-2 infection, pathological cytotoxic T cells (Tc) are present; these Tc can kill the virus but also damage lungs tissue, which can be seen as glass opacification, as mentioned in a previous review. 2 Moreover, CD4+ and CD8+, along with NK cells are exhausted during SARS-CoV2 infection, 2 , 40 demonstrating breakdown of the antiviral immunity in the early stages of infection. 40 It has been shown that identified markers of T lymphocyte exhaustion, such as programmed death 1 (PD-1), T-cell immunoglobulin mucin-3 and lymphocyte activation gene 3 (LAG-3) are elevated in COVID-19 disease, and related to more severe symptoms.40–42 A previous study shows that there is association between high viral replication in patients with chronic hepatitis B and exhaustion of T cells. 42
Data also suggest that the HPA axis, through the induction of PD-1 expression on NK cells, protects against cytokine-mediated damage during viral infection in mouse, and that glucocorticoid receptor induction of PD-1 was dependent on NK cytokine microenvironment, which indicates that it is tissue specific. 43 More studies are needed to provide evidence whether a similar mechanism is present in humans infected with SARS-CoV-2, due to complexity of systemic pathways. Alterations of PD-1 that are away from normal expressions can dramatically affect health. 44 This would promote the assumption that dysregulated HPA axis might not protect against cytokine-mediated damage, which might explain variability in severity of disease. Future research is needed to provide an answer.
Exercise and leukocytes
The relationship between exercise and immunity, both acquired and innate, suggests moderate intensity exercise training 45–47 improves the immune response, including beneficial effects on all leukocyte groups. 46 All major subpopulations of leukocytes are increased in numbers as a result of exercise training; however, regular exercise does not appear to change blood leukocyte count. 48
NK cells increase their activity during exercise and revert to basal levels following the exercise bout. 49 Their cytotoxic activity is reduced only if the exercise session is long and intense. 48 These effects are exercise intensity and volume dependent – the higher the exercise intensity/volume, the greater the reduction in cytotoxic activity. 49 Prolonged activity does not influence these changes, while higher cytokine concentration, such as IL-6, has proven impact. 48 IL-6 level increases in plasma and is volume, intensity, and activated muscle mass dependent during exercise. 50 , 51 Interestingly, PD-1 expression is increased after exercise and affects NK cells in a manner that it promotes anti-inflammatory environment in healthy adults. 44 But, it should be noted that PD-1 expression in different clinical settings is still yet to be evaluated as it was stated that the expression is reduced in autoimmune and increased in cancer patients. 44 We might assume that high levels of IL-6 (e.g. obese) induce an increase in glucocorticoids, thus affect PD-1 expression in basal situation. Therefore, reduction of PD-1 expression in diabetic type 2 patients, for example, 52 might be adaptive response. Further clinical research might provide evidence.
The ability for phagocytosis and neutrophil activation is lower during vigorous, longer exercise sessions. 53 There is also lower proliferative ability of lymphocytes with higher intensity exercise. 46 However, with moderate intensity exercise, neutrophil oxidative burst activity is increased. 46
The regulatory response would support improved immune processes by higher migration of leukocytes in all exercising tissues from circulation during recovery period, which might explain the decline in circulating lymphocytes and macrophages. 46 , 54 Research also shows that proinflammatory monocytes/macrophages infiltrated inside the muscle produce high IL-6 level during the early regeneration phase. 54
Additionally, the stress that occurs on respiratory epithelial tissue during exercise via higher ventilation, in combination with muscle damage, can increase levels of IL-6, as acute phase response proteins, potentially producing a positive adaptative immune regulation. 16 , 32 , 34 , 48 How this affects the course during SARS-CoV-2 infection requires further study.
Cortisol, exercise, and immune response
We suggest that a dysregulated cortisol response may have a role in proinflammatory reaction in the progression of COVID-19. 55 During training, IL-6 increases due to metabolic changes, especially glucose regulation, 56 which might interfere with cortisol levels by increasing it. 35 , 37,57--60 Also mechanism between IL-6 and cortisol in response to stress has been described, and both exercise and viral infection are known stressors. 32 , 34 , 35 , 37 In both cases, inflammatory reaction occurs during stress (response of IL-6) followed by HPA axis activation that stimulates cortisol secretion which was mentioned previously in a paper. The connection between viral and exercise stress responses can be seen through this relationship of IL-6 and HPA as opposite arms (inflammation and immunosuppression). Previous research shows that the cortisol response during exercise is intensity dependent, and that the amount of work in adequate training zones is important for an adequate response.61–65 When it comes to cortisol, there is threshold related to maximal oxygen consumption (VO2max) that affects its concentration. 66 , 67 Previous data show that exercise at 40% of VO2max reduces cortisol levels, while higher intensity exercise increases cortisol levels. 66 Moreover, exercise intensities over 60% VO2max were proposed to be a threshold for eliciting a significant cortisol response. 66 Of note, the circadian nature of cortisol, pre-exercise level of glucose, and percentage of BF may all have an impact on results gathered and reported, thus requiring more caution in interpretation.
Knowing that cortisol has an immunosuppressive effect, previous research could support our conclusion that during moderate physical activity, the immune response is not impaired. 32 , 35 , 39 , 56 , 58 , 68 Overall stress level, glucose levels, intensity and volume of exercise are factors that must be taken into consideration by future research, as the interplay of these parameters can possibly effect the immunoregulatory adaptation to stress due to long-term exercise. Combining hormonal therapy and physical activity in primary and secondary prevention of COVID-19 infection may be a novel effective approach, although further investigation is required.
Exercise implementation during COVID-19 pandemic
In theory, regulatory mechanisms that occur during exercise, stress itself and its transfer to pathophysiological changes during viral infection, 2 , 16 , 33 ,35–37, 69 may explain the role of exercise in the management of COVID-19 infection (Figure 2). Exercise as a stress mechanism, and changes to the immune system and hormone response due to the physiologic stress induced by exercise, may be highly beneficial in the current viral pandemic environment. Chronic controlled stress, such as that imposed as a result of exercise training, might stimulate positive adaptation to regulation of the immune response in such manner that the inflammatory response to viral infection has a lower likelihood of being excessive, which is characteristic during the cytokine storm syndrome. This would support moderate exercise as an important approach in reducing the risk of a severe clinic course.
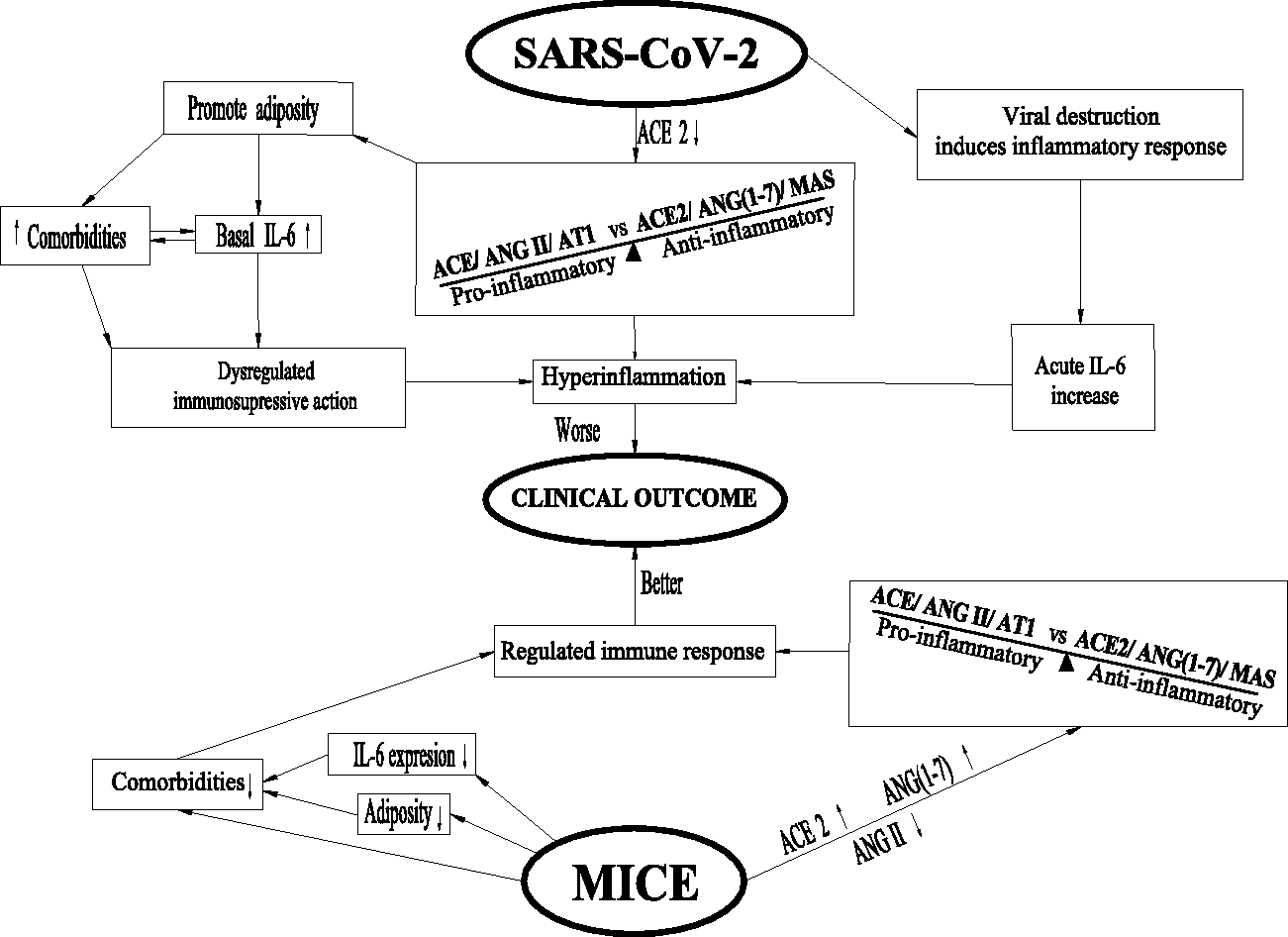
Mechanisms related to clinical outcome of COVID-19 patients.
One of the goals of exercise as a preventive strategy could be manifested through the impact on body composition change. 24 , 27 , 31 Regulation of BF might affect the immune profile because of its connection to circulating IL-6 in high risk individuals and positive result on associated risk factors. Evidence confirms the positive health effects of exercise on the circulating proinflammatory profile. 17 , 26 , 45 It has been shown that longer training periods downregulate the IL-6 expression 45 and produce anti-inflammatory effects. 16 , 58
As mentioned before, it has been shown that ACE2 deficiency caused by viral invasion might increase the dysregulation between the ACE/AngII/AT1 receptor and the ACE2/Ang(1–7)/Mas receptor axis, in favor of the first one, and that it could worsen the response to COVID-19, especially in categories of people who already have a deficiency of this receptor. 12 Also, previous research indicated that in experimental and clinical models of lung inflammation, Ang(1–7) exerted anti-inflammatory effects through lesser infiltration of lymphocytes and neutrophils, reduction of perivascular and peribronchial inflammation, and prevention of subsequent fibrosis. 70 ACE2 activation, associated with physical exercise is shown to potentiate the reduction of pulmonary fibrosis and may be a possible tool in the treatment of pulmonary fibrotic diseases, 70 which might also be applicable in COVID-19. Considering the fact that previous studies indicated that exercise upregulates ACE2 and Ang(1–7) expression and downregulates AngII, negative effect of the SARS-CoV-2 infection on the ACE2/Ang(1–7)/Mas receptor axis might be attenuated by this approach. 71
On top of that, it was stated that ACE/AngII pathway stimulates adiposity, 72 which can promote inflammatory imbalance that was elaborated previously in this paper. Exercise, through changes in body composition, might affect the balance in regulation between the ACE/AngII/AT1R and ACE2/Ang(1–7)/MasR regulatory axes. 12 , 72 , 73 Previous review states that the (Ang1–7)/MasR arm inhibits lipogenesis and stimulates lipolysis, 73 and we suggest that moderate-intensity continuous exercise (MICE) might prove beneficial in this pathway. It can be implemented in various populations in the form of weight reduction and cardio program. While being able to produce benefits related to comorbidities in few ways, by reducing amount of adipose tissue (thus affecting immune profile) and improving systemic functional capacity (e.g. cardiorespiratory system), and by altering ACE/ACE2 activity, it can be seen as a potent tool in reducing risk for more serious clinical outcome. There is still not enough evidence when it comes to vigorous exercise as it might seem detrimental due to its immuno-depressive effect. 46 , 48 , 74 It has been shown that high intensity interval training (HIIT), as well as MICE, can influence plasma and urinary levels of ACE and ACE2 in humans, and that both exercise approaches increased urinary levels of Ang(1–7). However, greater increase of Ang(1–7) concentration occurred in the MICE when compared with the HIIT approach. 73 Regional hypoxia might provide some of the potential targets of future research, as blood flow restricted training upregulates ACE2 receptors, prevents muscle wasting, and increases circulating ACE2 levels, 72 but it is yet to be studied to determine precise mechanisms by which exercise elicits its effects in humans. Considering all mentioned above, promotion of ACE2/Ang(1-7)/Mas receptor axis through MICE might be beneficial in reducing the probability of cytokine storm and the tissue damage that it causes.72,75 Compared to HIIT, MICE would seem as more practical to implement, monitor, and control (both intensity and volume wise). Tools invented are more applicable for MICE (e.g. wrist watches) and general population is more familiar of its implementation, with currently known guidelines and stands toward comorbidities. Thus, quantifying data that can be analyzed, interpreted, and uniform is much more practical, in general. Future research should also focus on the exercise effect on modulation of the RAS axis, as there might be potential therapeutic benefit in the prevention of rapid lung damage in combination with regulation of the inflammatory response. 12 , 16 , 70 , 72 , 76 , 77
Increases of PD-1 and LAG-3 expression after single HIIT bouts in healthy young males are reported, 44 but more research is still needed to provide evidence regarding clinical populations. Since PD-1 expression is reduced in autoimmune patients, 44 , 52 we assume that increase in its expression, in combination with reduction of basal IL-6 concentration, by regulation of body composition and exercise, might be beneficial for these patients. Nevertheless, assumption regarding in which populations this would be applicable is yet to be studied, since it has been shown that in cancer patients, we have different starting point. 44 As such MICE might be more beneficial as it promotes gentler and not so drastic changes in immunity, and overall stress, due to lower intensity, while promoting positive environmental regulation. Longitudinal studies with planned exercise protocols should be conducted to provide supportive evidence.
Conclusions
In conclusion, moderate long-term exercise training might be seen as an effective strategy to reduce the likelihood of severe presentation of COVID-19. Improved resistance to infection can be seen in two ways, by affecting immune-regulatory pathway (IL-6/cortisol), through improvement of functional capacity and body composition, and by improving ACE/ACE2 balance. Both pathways play important roles in comorbidities linked to severe COVID-19 outcome and are modified by physical activity. Thus, the mechanism of beneficial effects of exercise training are multifactorial, including the alteration of body composition in patients with excess body mass as well as the positive effects of exercise training on immune regulation. 13 , 24 , 33 , 46 , 48 , 78 , 79
Additional evidence on how a history of exercise training prior to viral infection enhances immune regulation once the viral infection occurs is needed. However, when conclusions from previous studies are applied, it could be assumed that the benefits of regular exercise have a convincingly positive effect on comorbidities that are related to more severe symptoms. 2 , 3 , 23 , 28 , 33 , 80 Given the benefits, both proven and theoretical, of exercise training are numerous, measures should be taken to promote a physically active lifestyle. Exercise is a medicine that has enormous potential to improve global health, both from the perspective of chronic disease and viral pandemics.
Footnotes
AUTHORS’ CONTRIBUTIONS
All authors participated in the design, interpretation of the studies and analysis of the data and review of the manuscript; StSe designed the study, StSe, SSD, VI, MT and StSt analyzed and interpreted the data, StSe and SSD drafted the paper and wrote the manuscript, RA and DP revised the paper and DP gave the final approval.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.