
Abstract
An observational study was conducted in Ukraine to determine the independent mortality risks among adult inpatients with COVID-19. The results of treatment of COVID-19 inpatients (n = 367) are presented, and waist circumference (WC) was measured. Logistic regression analysis was applied to evaluate the effects of factors on the risk of mortality. Odds ratios and 95% CIs for the association were calculated. One hundred and three of 367 subjects had fasting plasma glucose level that met the diabetes mellitus criteria (≥7.0 mmol/L), in 53 patients, diabetes mellitus was previously known. Two hundred and eleven patients did not have diabetes or hyperglycemia. Diabetes mellitus/hyperglycemia odds ratio 2.5 (CI 1.0–6.1), p = 0.045 loses statistical significance after standardization by age, waist circumference or fasting plasma glucose. No effect on gender, body mass index-determined obesity, or hypertension was found. The fasting plasma glucose (>8.5 mmol/L), age (≥61 years), and waist circumference (>105 cm) categories were associated with ORs 6.34 (CI 2.60–15.4); 4.12 (CI 1.37–12.4); 8.93 (CI 3.26–24.5), respectively. The optimal model of mortality risk with AUC 0.86 (CI 0.81–0.91) included the diabetes/heperglycemia and age categories as well as waist circumference as a continued variable. Waist circumference is an independent risk factor for mortality of inpatients with COVID-19.
Impact statement
The question of the independence of the risk factors for mortality in patients with COVID-19 remains unclear. Estimates of such risk factors like diabetes, hypertension, and obesity have been controversial. Most of such studies used body mass index (BMI) instead of waist circumference (WC) as an indicator. Our hospital cohort of COVID-19 patients found no effect of obesity (BMI ≥ 30 kg/m2) or high blood pressure (BP ≥ 140/90 mmHg) on the chances of death. However, the fasting plasma glucose (>8.5 mmol/L), age (≥61 years), and WC (>105 cm) categories were associated with a multiple increase in the risk of death. The optimal model, which includes the categories of diabetes diagnosis or diabetic glycemia level, age, and WC, indicates even a negative risk for the diabetes category. Thus, the risk of death in patients with COVID-19 is associated with abdominal obesity rather than diabetes.
Introduction
At the end of 2019, a novel coronavirus (named SARS‐CoV‐2) has emerged, causing coronavirus disease 2019 (COVID‐19) and by 11 March 2020, the World Health Organization has declared COVID‐19 a pandemic. One and a half years after the beginning of the pandemic, the question of the independence of some of the risk factors for mortality in patients with COVID-19 remains unclear.
Patients with diabetes mellitus (DM) are considered to be more prone to severe COVID-19.1–3 The pathogenesis of this phenomenon remains unanswered: is it directly related to elevated blood glucose, is it a consequence of chronic complications of DM, or is it the result of certain hypoglycemic or antihypertensive treatment of patients with DM and COVID-19. Unfortunately, some estimates have been controversial: one observational study performed in Wuhan, China, failed to confirm the negative impact of DM on COVID-19 mortality, 4 while another similar study from the same region reports the opposite results. 5 The effect of hypertension and obesity on the risk of severe consequences of the combination of DM and COVID-19 is also still the subject of research. While some authors point to hypertension and/or obesity as risk factors for mortality in patients with COVID-19,2,3,6 others do not mention them among the independent factors.1,7,8 Moreover, elevated systolic blood pressure was associated with a reduction (!) in mortality from COVID-19 in individuals with type 2 diabetes, and the use of antihypertensive drugs was associated with a slightly higher risk of mortality. This study, conducted in England, also points to the non-linear connection between BMI and related COVID-19 mortality of patients with type 2 DM. 9 It should be noted that all of the studies used BMI instead of waist circumference as an indicator.
That is, the results of the epidemiological study highlight the need to deepen the study of the results of treatment with COVID-19 in people with diabetes, taking into account the level of hyperglycemia, blood pressure, and obesity indicators. Below are the results of an observational study conducted in the Infectious Diseases Hospital of Kostiantynivka, Donetsk region, Ukraine, which is directly involved in providing hospital care to patients with COVID-19.
Materials and methods
The study was conducted by analyzing the archives of one of the infectious disease hospitals of Ukraine (Kostiantynivka, Donetsk region). In 2020, 650 patients with clinical symptoms and symptoms similar to COVID-19 were hospitalized at the Infectious Diseases Hospital, which provides care to 961,000 residents. Diagnosis of COVID-19, selection of patients for hospitalization, clinical examinations, and treatment were performed according to relevant national standards, 10 which were updated according to WHO recommendations. Details of hospitalization criteria are presented in supplement Table 1. The diagnosis of COVID-19 was confirmed by PCR (n = 363) or by detection of specific antibodies (n = 4). Two hundred and eighty patients with similar symptoms were not included in the analysis due to the lack of laboratory confirmation of SARS-CoV-2 or relevant antibodies. Three children with COVID-19 were also not included in the study. Electronic dataset was developed by Komisarenko Institute of Endocrinology and Metabolism, Kyiv, Ukraine. The results of treatment of all adult laboratory-confirmed COVID-19 inpatients (n = 367, men 43.1%) from 31 March 2020 to 15 January 2021 are presented.
Anthropometric and clinical characteristics of hospitalized COVID-19 patients depending on their affiliation to diabetes/hyperglycemia or normal glucose categories.

Note: Data are medians and interquartile range (QI–QIII) or n and %.
aMann-Whitney test.
bFisher's exact test.
cFrom 109 patients with measured BMI.
BMI: body mass index; Obesity: BMI ≥ 30 kg/m2; High blood pressure: BP ≥ 140/90 mmHg; SpO2: peripheral capillary oxygen saturation; WBC: white blood cells; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein test, semi-quantitative.
In addition to standard clinical and anthropometric characteristics of patients, fasting plasma glucose (FBG), peripheral capillary oxygen saturation (SpO2); white blood cells (WBC); lymphocytes, granulocytes count, erythrocyte sedimentation rate (ESR); c-reactive protein (CRP) test, body mass index (BMI); systolic and diastolic blood pressure, waist circumference (WC) were measured. BMI was determined as the body weight (kg) divided by the height (m) squared (kg/m2). WC was measured in the standing position, midway between the bottom rib and iliac crest, directly on the skin. Clinical and anthropometric characteristics of patients were assessed on the first day of hospitalization.
Leaving the hospital due to recovery or death was considered as a dichotomous treatment outcome.
Statistical analysis
MedCalc® Statistical Software version 20.009 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org; 2021) was used for statistical analysis. Numerical variables were found to be non-normally distributed (p < 0.05 by Shapiro–Wilk test); therefore, they were presented by the median (Me) and interquartile range (QI–QIII). Mann–Whitney U-test was used for comparison of numerical variables of two groups. Logistic regression analysis was applied to evaluate the effects of factors on the risk of mortality, odds ratio (OR) and 95% confidence intervals (95% CIs) for the association were calculated. For selection of the independent variables that influence the dependent variable, the stepwise method was used. The predictive accuracy of the models was assessed by the area under the ROC curve (AUC). The level of significance was <0.05.
Results
Analysis of the treatment outcomes in an infectious hospital between 31 March 2020 and 15 January 2021 of 367 patients with COVID-19 (men 43.1%) showed the following:
One hundred and fifity-six of these subjects had fasting venous plasma hyperglycemia that met the DM criteria (7.0 mmol/L or higher), and the corresponding hyperglycemia was detected for the first time in a hospital study in the majority (n = 103) of these patients. In 53 patients, diabetes was previously known, and the duration of diabetes was Me = 9.98 years (QI–III 4.08–13.67). Accordingly, 211 patients did not have diabetes or hyperglycemia (Table 1).
The duration of hospital treatment in the group with diabetes and hyperglycemia was 21 (16–27) days, Me, (QI–III), and did not differ from the corresponding rate in persons with normal glycemia. Patients with diabetes/hyperglycemia more often required treatment with mechanical ventilation, were older, had lower oxygen saturation, higher levels of systolic BP, WC, and BMI. High blood pressure was observed in 50.6%, and obesity assessed by BMI in 43.1% of patients in diabetes/hyperglycemia category. Inflammation markers (C-reactive protein, WBC and granulocytes count, ESR) for this category of COVID-19 patients were also higher (Table 1).
The median age of all patients (n = 367) was 62 (52.6–69.8) years. Of these, 345 (94%) were cured and left the hospital, and 22 (6%) died. For patients with DM and hyperglycemia (n = 156), the age of patients was 62.2 (55.8–70.3) years, of whom 142 (91%) were cured and left the hospital and 14 (9%) died. The corresponding indicators in the group without DM/hyperglycemia (n = 211) were 59.2 (49.8–68.7) years, 203 (96.2%), and 8 (3.8%).
Regression analysis indicates factors that influenced the chances of death in patients with COVID-19 (Table 2): these included an increase in blood glucose, WC, decreased oxygen saturation (SatO2), increased white blood cell, and granulocyte counts.
One-factor regression and ROC analysis of the death probability for hospitalized patients with COVID-19 (continued variables).
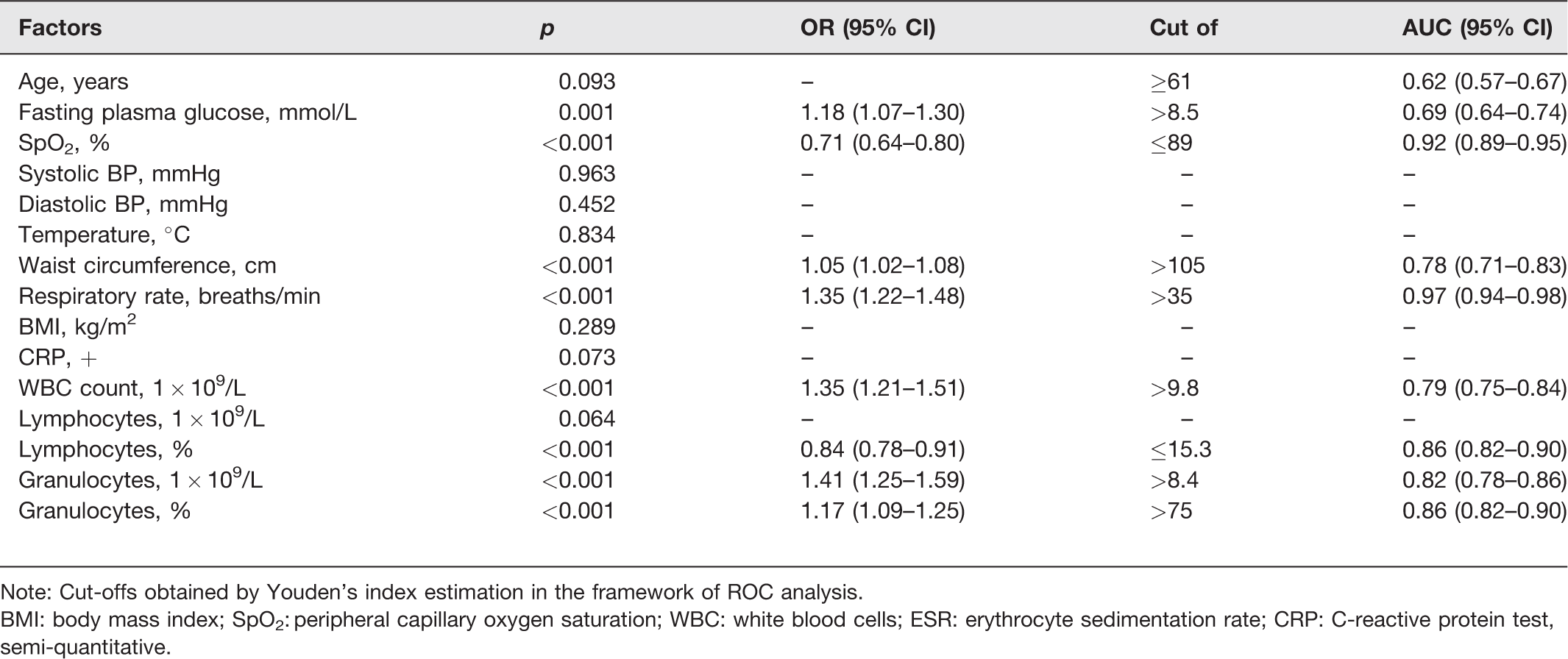
Note: Cut-offs obtained by Youden's index estimation in the framework of ROC analysis.
BMI: body mass index; SpO2: peripheral capillary oxygen saturation; WBC: white blood cells; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein test, semi-quantitative.
According to one-factor regression analysis, DM/hyperglycemia significantly increases the probability of death in hospitalized patients with COVID-19: OR 2.5 (CI 1.0–6.1) (p = 0.045).
Surprisingly, our cohort of COVID-19 patients found no effect of gender, obesity (BMI ≥ 30 kg/m2) or high blood pressure (BP ≥ 140/90 mmHg) on the chances of recovery or death.
However, the FBG (>8.5 mmol/L), age (≥61 years), and WC (>105 cm) categories obtained by the ROC analysis were associated with a multiple increase in the risk of death: corresponding ORs were 6.34; 4.12; 8.93, respectively. Thus, the maximum of these risks may be associated with abdominal obesity. Other high risks indicate a presumed association between respiratory failure, inflammation, and probability of death (ORs 21.8 to 97.8), and are unlikely to differ depending on the presence of hyperglycemia (Table 3).
One-factor regression and ROC analysis of the death probability for hospitalized patients with COVID-19 (categorical variables).

Note: Other cut-offs obtained by Youden's index estimation in the framework of ROC analysis.
Diabetes/hyperglycemia: known diabetes mellitus diagnosis or fasting plasma glucose ≥ 7.0 mmol/L at admission; High blood pressure: BP ≥ 140/90 mmHg regardless of the presence or absence of antihypertensive treatment; Obesity: BMI ≥ 30 kg/m2.
Thus, for the cohort of patients with COVID-19 whose treatment we observed in 2020, the main risk factor for mortality was the anthropometric indicator that characterizes the presence of abdominal obesity. The effect of gender, BMI, and blood pressure on the chances of dying was not found.
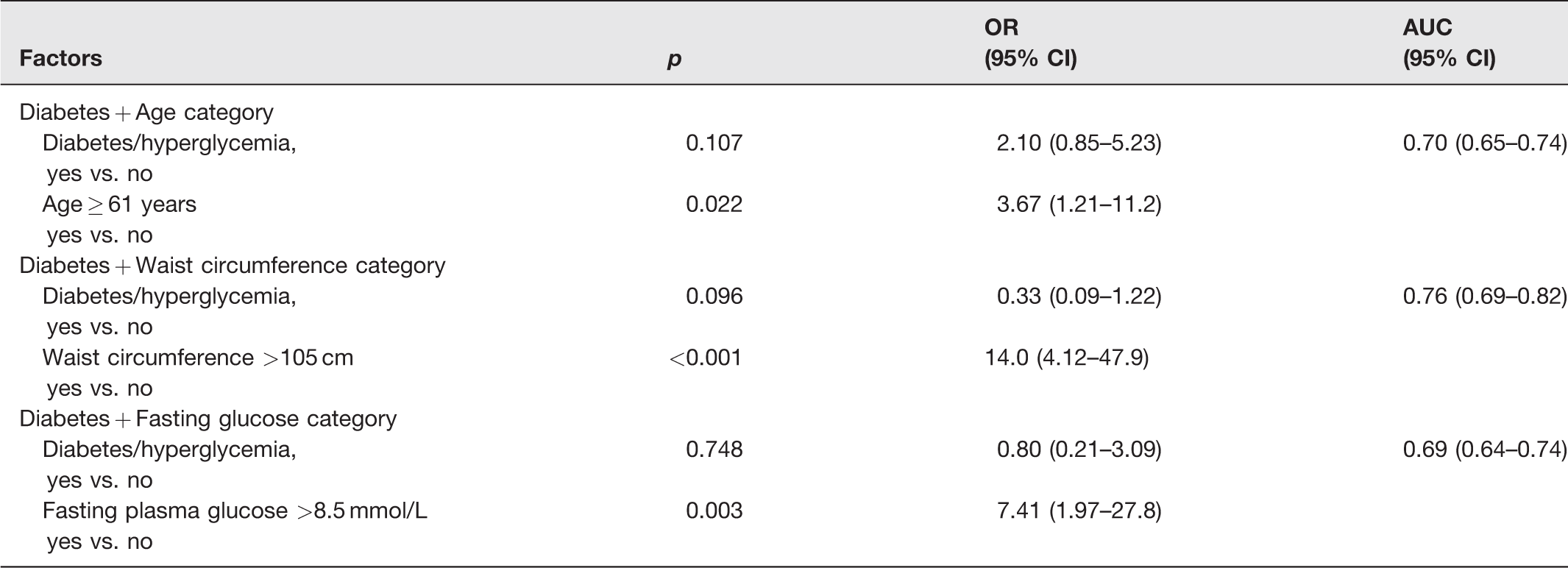
Two-factor analysis according to the logistic regression model (Table 4) indicates that the risk of death associated with the diagnosis of diabetes or diabetic glycemia level during hospitalization loses statistical significance in case of standardization by age (≥61 years), WC (>105 cm), or fasting glucose (> 8.5 mmol/L).
Two-factor logistic regression modeling of the probability of death for inpatients with COVID-19.
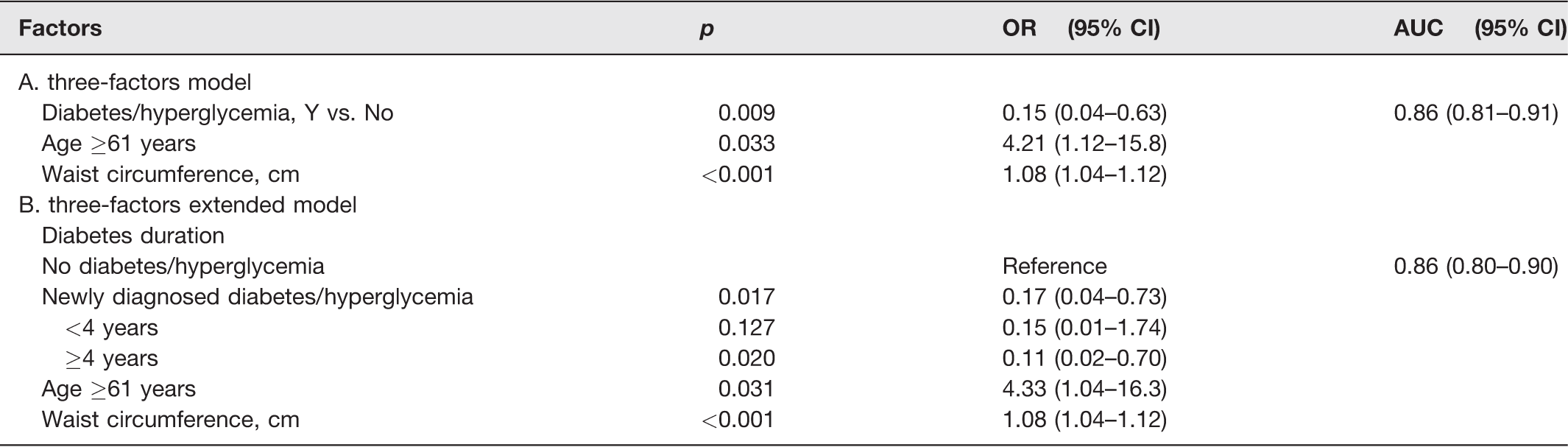
The optimal three-factor model of mortality risk, obtained by stepwise logistic modeling (Table 5, A, Figure 1), which includes the categories of diabetes or diabetic glycemia level and age as well as WC as a continued variable, indicates even a negative risk for the diabetes category 0.15 (CI 0.04–0.63).
Multifactorial logistic regression modeling of the probability of death of inpatients with COVID-19.
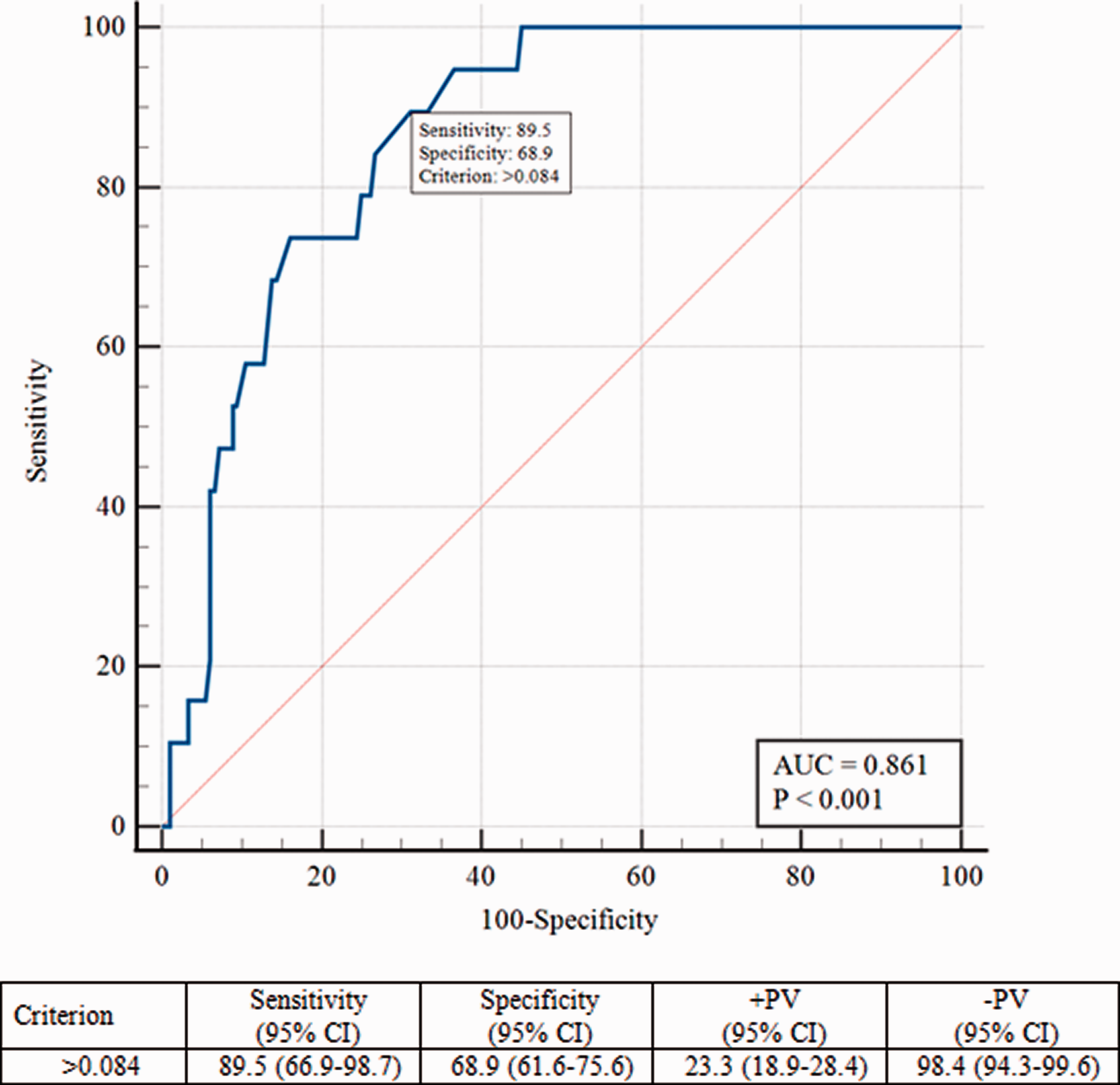
ROC-curve of the three-factors (diabetes duration, age, waist circumference) logistic model of the death prediction for the inpatients with COVID-19. (A color version of this figure is available in the online journal.)
The addition of diabetes duration factor (Table 5, B) does not increase the area under the ROC curve (AUC) and does not improve the quality of the model.
At the time of admission, patients who were later treated with mechanical ventilation, were more severe in terms of respiratory rates and SpO2 (supplement Table 2). ROC analysis of factors that predict treatment with mechanical ventilation, indicates that there was an increase in WC, FBG, and age. The WC AUC = 0.664 (95% 0.594–0.729), addition of glucose, and age to the model increases the AUC to 0.712 (95% CI 0.644–0.774).
Discussion
According to our assessment of treatment of 367 COVID-19 inpatients, abdominal obesity was the highest predictor of mortality from those factors that are uncharacteristic to the clinical course of this infection but reflect the initial characteristics of patients.
A feature of our study is the measurement of not only body mass index but also waist circumference in patients with COVID-19, which can be attributed to the advantages of our study. Morys F and Dagher A, 11 who analyzed the mortality of 1148 patients with COVID-19, found that an increase in WC, glycemia (but not DM diagnosis), and systolic BP (but not diagnosis of hypertension) associated with increased mortality. In contrast to our study, they did not build a general model for these three identified factors, i.e. did not study the independent influence of each of them, while taking into account the other two. The study, Morys F and Dagher A, 2021 as well as our study, was conducted before the start of mass vaccination, which excluded its impact on the results. The disadvantages of our study include a somewhat unusual categorization: the “diabetes” group (n = 156) included people with hyperglycemia that met the DM criteria, and the corresponding hyperglycemia was detected for the first time in the majority (n = 103) of these patients. In 53 patients, diabetes was previously known. Thus, the “diabetes” group is quite heterogeneous in relation to the known history of hyperglycemia, but this approach has made it possible to overcome the quantitative limitations of our sample. Unfortunately, at the beginning of the pandemic, we failed to assess the impact of further drug treatment on the risk of death, which also remains one of the shortcomings of the study. However, it should be noted that our categorization was not affected by dexamethasone treatment, as glucose was taken into account at the time of hospitalization (before the treatment started).
Of the 367 patients, 43.1% were men, which indicate female predominance in the COVID-19 population studied in Ukraine. Reports from other regions show more men than women in the COVID-19-infected population. 12 Given that women generally have higher total body fat than men, whereas men tend to have greater abdominal fat, the gender distribution of our study population might have influenced COVID-19 outcomes.
Nevertheless, we failed to confirm the connection between gender and mortality in the sample studied (Table 3). In addition, we did not find a statistically significant gender difference in WC in hospitalized men and women with COVID-19 (data not shown). It is possible that the presence of abdominal obesity in women who were hospitalized contributed to the equalization of gender chances of death.
Possible explanations for the increased chances of death in patients with abdominal obesity and COVID-19 include an increase in the position of the diaphragm, which makes it difficult to breathe. An additional explanation may be the difficulty of following the existing guidelines for patients with acute respiratory distress syndrome (ARDS) to stay in a supine position for more than 12 h a day 10 due to abdominal obesity.
WC is a well-known risk factor for cardiovascular disease (CVD), 13 so the association between increased waistline and higher mortality from COVID-19 can be reasonably explained by the different prevalence of CVD.
Other significant factors include age over 61 years and glycemia >8.5 mmol/L. Several other studies have obtained similar results.3,14 However, hypertension cannot be attributed to significant mortality factors in patients with COVID-19. In part, these data are consistent with the results of Morys F and Dagher A. 11 We have not been able to prove the effect of known duration of diabetes on the chances of dying from COVID-19. However, the level of FBG > 8.5 mmol/L is associated with a multiple increase in the chances of dying: OR 7.41 (CI 1.97–27.8), regardless of history of diabetes. Acording to the CORONADO study 15 in people with diabetes hospitalized for COVID-19, long-term glucose control assessed by HbA1c was not associated with tracheal intubation and/or death within seven days. Even an opinion formulated 16 that hyperglycaemia at the time of hospital admission is associated with poor outcomes, but it may simply be considered a marker of severity of the infection. Our data do not contradict this assumption. Moreover, our data are rather consistent with the findings of a study by Liu et al. 4 that diabetes does not affect the prognosis of patients with COVID-19 than with Shang et al., 2021 study, that DM is an independent risk factor for the COVID-19 mortality forecast. 5
Thus, the risk of death in patients with COVID-19 is associated with abdominal obesity rather than a diagnosis of DM, the presence of which can sometimes even reduce the associated risk. In this context, it is worth recalling clinical and experimental data that suggest that DM may counteract the development of acute lung injury/ARDS, 17 which raises the question of causation.
Conclusions
WC measurement can provide useful information on the prognosis of treatment of inpatients with COVID-19.
Supplemental Material
sj-pdf-1-ebm-10.1177_15353702211054452 - Supplemental material for Relationship between hyperglycemia, waist circumference, and the course of COVID-19: Mortality risk assessment
Supplemental material, sj-pdf-1-ebm-10.1177_15353702211054452 for Relationship between hyperglycemia, waist circumference, and the course of COVID-19: Mortality risk assessment by Mykola Khalangot, Nadiia Sheichenko, Vitaly Gurianov, Viola Vlasenko, Yulia Kurinna, Oksana Samson and Mykola Tronko in Experimental Biology and Medicine
Supplemental Material
sj-pdf-2-ebm-10.1177_15353702211054452 - Supplemental material for Relationship between hyperglycemia, waist circumference, and the course of COVID-19: Mortality risk assessment
Supplemental material, sj-pdf-2-ebm-10.1177_15353702211054452 for Relationship between hyperglycemia, waist circumference, and the course of COVID-19: Mortality risk assessment by Mykola Khalangot, Nadiia Sheichenko, Vitaly Gurianov, Viola Vlasenko, Yulia Kurinna, Oksana Samson and Mykola Tronko in Experimental Biology and Medicine
Footnotes
DATA AVAILABILITY
The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.
AUTHORS’ CONTRIBUTIONS
MK and MT conceived the study design. NS, VV, YuK participated in data collection. MK, NS, and OS participated in data analysis and interpretation. VG carried out the final statistical analysis. MK and VG drafted the article and designed the figure. All authors approved the final version of the paper.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
ETHICAL APPROVAL
The study was approved by the ethics committee of the Institute of Endocrinology and Metabolism (National Academy of Medical Sciences of Ukraine). The Declaration of Helsinki (2000) and the applicable national standards as they relate to the involvement of human subjects in research were enforced.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.
SupplementAL MATERIAL
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.