
Abstract
The correlation of maternal serum alpha-fetoprotein (AFP) variants (AFP-L2, AFP-L3), free beta-human chorionic gonadotropin (free β-hCG), and open neural tube defects (ONTDs) during the second trimester, and the screening efficiency of different risk models remain indistinct. We conducted a retrospective case-control study, and studied 57 pregnant women with ONTD fetuses and 569 pregnant women with normal fetuses. The receiver operating characteristic curve method indicated the best cutoff value and area under the curve (AUC). The predictive value of ONTD risk models by free β-hCG, AFP, AFP-L2, and AFP-L3 was investigated via integrated discrimination improvement (IDI), net reclassification improvement (NRI), and decision curve analysis (DCA). Compared to the control group, AFP, AFP-L2, and AFP-L3 levels were significantly higher, while free β-hCG level was significantly lower in the study group. The triple-index model of free β-hCG + AFP-L2 + AFP-L3 and the dual-index model of AFP-L2 + AFP-L3 showed the best predictive values, respectively (AUC = 0.905; AUC = 0.885). The order of the single-index model AUCs was AFP-L3 > AFP-L2 > AFP > free β-hCG. The negative predictive value, false positive rate, and negative likelihood ratio of AFP-L2, AFP-L3 alone, or combined with free β- hCG were better than those of AFP alone; however, the positive likelihood ratio was the opposite. The replacement of AFP by AFP-L2 or AFP-L3 combined with free β-hCG increased the IDI and NRI for predicting ONTD. The top five DCAs were AFP-L2 + free β-hCG, free β-hCG, AFP-L3, AFP + free β-hCG, and AFP. Indicators of maternal serum free β-hCG, AFP-L2, and AFP-L3 in the second trimester exhibited high sensitivity and specificity screening for ONTD fetuses. Risk models constructed using AFP-L2 + AFP-L3 and AFP-L2 + AFP-L3 + free β-hCG demonstrated better screening efficiency.
Keywords
Impact Statement
Open neural tube defects (ONTDs) are common birth defects of the central nervous system; the optimal time for screening ONTDs is during the second trimester. Alpha-fetoprotein (AFP) is widely utilized as a crucial screening marker for ONTDs; however, the efficiency of this screening has been unsatisfactory. Serum AFP combines with lens culinaris agglutinin and is later divided into three bands by electrophoresis, namely, AFP-L1, AFP-L2, and AFP-L3. Serum AFP-L2 and AFP-L3 have been previously utilized for the screening of Down syndrome. This study focused on the discovery of new markers for ONTD to improve the efficiency of prenatal screening. We conducted a retrospective case-control study including 57 pregnant women with ONTD fetuses and 569 pregnant women with normal fetuses, and constructed different models using free β-hCG, AFP, AFP-L2, and AFP-L3. Results indicated that risk models constructed using AFP-L2 + AFP-L3 and AFP-L2 + AFP-L3 + free β-hCG demonstrated better screening efficiency.
Introduction
Neural tube defects (NTDs) are general birth defects of the central nervous system with a prevalence of 1.2 per 1000 live births, including a series of defects of varying severity. 1 NTDs can appear on any part of the nerve axis and have a specific level of clinical intensity; NTD subtypes are identified according to the anatomic location and severity of the defects. The most serious form of NTD is anencephaly or craniorachischisis, where the forebrain and entire central nervous system fail to convert from the neural plate to a neural tube. NTD may be affected by numerous types of genetic variation. 2 According to whether the involved nerve tissue is disposed to the body surface, NTDs are classified as open neural tube defects (ONTDs) or closed NTDs. ONTDs, including open spina bifida and anencephaly, are among the most common birth defects in neonates, and the clinical manifestations vary according to the physical severity of the defects.3,4 Spina bifida is a neurogenetic disease with complex etiology involving genetic and environmental factors. It occurs in two main forms, namely, open spina bifida (or spina bifida hole) and closed spina bifida (or spina bifida occulta). 5
The optimal time for the screening of the three types of NTDs (open spina bifida, anencephaly, and encephalocele) is during the second trimester (15 weeks–20 weeks 6 days). The risk that a pregnant women may be carrying an ONTD fetus is calculated using levels of AFP combined with the gestational age, last menstrual period, and maternal weight.6,7 AFP is widely utilized as one of the main markers for screening for Down syndrome. The physiological mechanism involves the slow release of AFP into the amniotic fluid through the defective tissues, followed by its entry into the maternal serum through the maternal placental barrier in the ONTD fetus. Therefore, increased levels of AFP in the maternal serum are also widely used for predicting the occurrence of ONTD 8 ; however, numerous studies report that the efficiency of such testing is unsatisfactory. Our preliminary work also showed that the detection rates of screening for fetal anencephaly, spina bifida, and encephalocele were 52.63% (10/19), 53.33% (32/60), and 39.13% (9/23), respectively. 9 Therefore, a search for new markers of ONTD is warranted to improve the efficiency of prenatal screening.
Serum AFP combines with lens culinaris agglutinin and is later divided into three bands by electrophoresis, called AFP-L1, AFP-L2, and AFP-L3. 10 AFP-L3 combined with lentil is usually termed AFP heterogene, representing the latest formation of tumor markers.11,12 As mentioned above, serum AFP-L2 and AFP-L3 have been utilized for the screening of Down syndrome.13,14 In a previous study, we evaluated risk models of maternal serum AFP-L2 and AFP-L3 in only 21, 16, and 38 cases of ONTD, abdominal wall defect (AWD), and control, respectively. The results showed that AFP-L2 and AFP-L3 were encouraging biomarkers in screening for ONTD and AWD fetuses. 15 However, there is a lack of studies with large samples focusing on AFP-L2 and AFP-L3 screening for ONTD. Consequently, a large, retrospective and case-control study was conducted to explore the relationship and compare the screening efficiency of AFP-L2 and AFP-L3 screening for ONTD in the second trimester.
Materials and methods
Subjects
Our study was performed on 57 pregnant women with ONTD fetuses diagnosed by ultrasound imaging (43, 8, and 6 cases of open spina bifida, anencephaly, and encephalopathy, respectively), and 569 pregnant women with normal fetal development randomly selected in the corresponding period. Pregnant women (15 weeks–20 weeks 6 days) were recruited in two prenatal screening clinics from October 2007 to September 2019. The normal group was used to determine the distribution and normal reference intervals of serum AFP, AFP-L2, AFP-L3, and free beta-human chorionic gonadotropin (free β-hCG) levels in different periods of gestation between 15 weeks and 20 weeks 6 days. This study was approved by the Ethics Committee of our hospital (approval number: (2018) medical ethics (004) No. 01).
Diagnostic and exclusion criteria
Diagnosis was reached according to the American College of Obstetricians and Gynecologists Clinical Management Guidelines. 16 The exclusion criteria were (1) multiple pregnancies; (2) combination with other medical diseases, such as diabetes and severe pregnancy complications; (3) smoking; (4) pregnancy through in vitro fertilization; (5) follow-up outcomes revealing trisomy 21, trisomy 18, trisomy 13, and other birth defects; and (6) insufficient data.
Instruments and reagents
The following instruments and consumables were used in this study: a 1235 Auto time-resolved fluoro immunoassay (DELFIA®) immunoassay analyzer (PerkinElmer, Shelton, USA); an RT-6100 microplate analyzer (Rayto, Shenzhen, China); a 988 washer (Tianshi, Beijing, China); a dual labeling kit (AFP/free β-hCG); enhancer, lotion, quality standards, and standards (PerkinElmer); AFP-L2 and AFP-L3 (BIM, San Francisco USA).
Test methods
Fasting venous blood (2–3 mL) was drawn, separated after 30 min, stored at 2–8°C, and the AFP and free β-hCG were examined within one week. The two screening institutions uniformly used the DELFIA® method, and the detection steps were carried out according to the instructions provided by the manufacturer. Prior to the test, the stored serum samples were prepared as recommended in the instructions, and low-temperature centrifugation and batch tests were performed. The enzyme-linked immunosorbent assay sandwich technique was used for determination of AFP-L2 and AFP-L3 concentration.
Indicator levels were expressed in multiples of media
The following is the definition and calculation formula for multiples of media (MoM):

where Original Conj. denotes the original concentration value of AFP, free β-hCG, AFP-L2, and AFP-L3; Median denotes the median of the original concentration of the corresponding index. 15
For the purpose of decreasing the deviation resulting from gestational age and maternal weight, we calibrated the MoM value of each index and replaced the original concentration with that value.
The MoM value was calibrated using the median equation of gestational age and maternal weight. For example, the calculation for AFP-L3 was performed as follows 17 :

where GA is gestational age.

Similarly, AFP, free β-hCG, and AFP-L2 were analogized. The calculation of the MoM value was adjusted to the (4) formula according to the (2) and (3) formulae. Finally, the adjusted MoM value was applied to modeling calculation. 15

Establishment of risk models
The sample likelihood ratio (LR) was calculated by the probability density function of normal distribution, and the results were used as the risk prediction score of the samples in the ONTD group.
The calculation of LR15,17 was performed as follows:

Single-, dual-, and triple-index models were calculated using the one-dimensional normal distribution likelihood, two-dimensional normal distribution probability density function formula, and three-dimensional normal distribution probability energy density function. The log10 logarithm of free β-hCG MoM, AFP-L2 MoM, and AFP-L3 MoM was obtained; the LR was calculated; and the final risk of ONTD was determined using the following formula:

We separately constructed nine screening models based on the process described above. The single-index models included free β-hCG MoM, AFP MoM, AFP-L2 MoM, and AFP-L3 MoM. The dual-index models included AFP + free β-hCG, AFP-L2 + free β-hCG, AFP-L3 + free β-hCG, and AFP-L2 + AFP-L3. The triple-index model was free β-hCG + AFP-L2 + AFP-L3.
Statistical analysis
We used Excel 2007 software (Microsoft, Redmond, WA, USA) to establish a database using the test results, and SPSS v.21.0 (IBM, Armonk, NY, USA) software for statistical analyses. The one-sample Kolmogorov–Smirnov test was employed for data normality. The median and percentile (M (P2.5, P97.5)) were expressed for the skewed data. The Mann–Whitney U or Mann–Whitney H test was used to compare groups. A multivariate normal probability model was constructed using Python 3.8 language (https://www.python.org/), based on Bayes’ theorem. The receiver operating characteristic (ROC) curve method was used to determine the cutoff value and area under the curve (AUC). Integrated discrimination improvement (IDI) and net reclassification improvement (NRI) indicators 18 were used to evaluate the performance of the risk model for ONTD constructed by a variety of biomarkers. P values < 0.05 denoted statistically significant differences. A large AUC and high sensitivity indicated the superior diagnostic value of risk models. Decision curve analysis (DCA) was employed for the clinical applicability of different models for predicting ONTD. 19
Results
Comparison of baseline information
Maternal age and gestational age were lower, whereas maternal weight was higher in the ONTD group compared to the normal group; however, the differences were similar (Z = 0.443, Z = 1.335, Z = 1.283, respectively; all P > 0.05). Among 569 normal pregnant women, the maternal age at 15–17 gestational weeks was higher than that noted at 20 gestational weeks, and the differences were all significant (all P < 0.05). There existed no significant difference in maternal age throughout the remaining gestational weeks (all P > 0.05). The difference in maternal weight was not significant between 19 and 20 gestational weeks (Z = 2.605, P = 0.138); nevertheless, it reached statistical significance between the other gestational weeks (all P < 0.05). Comparison of gestational age between groups at each gestational week yielded similar findings (all P > 0.05), see Table 1.
Comparison of basic data in two group.
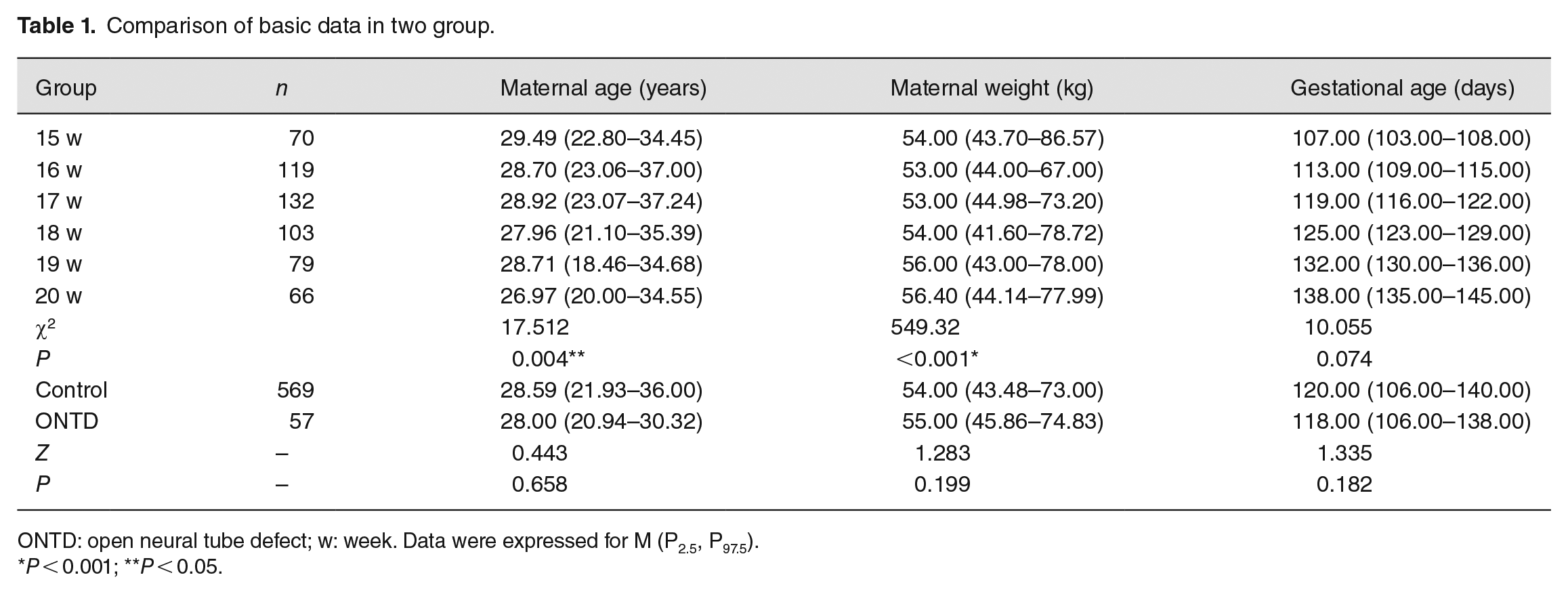
ONTD: open neural tube defect; w: week. Data were expressed for M (P2.5, P97.5).
P < 0.001; **P < 0.05.
Comparison of serum indicators
Levels of serum AFP-L2, AFP-L3, and AFP in pregnant women with ONTD fetuses were significantly higher than those measured in pregnant women with normal fetuses (1.54 vs 0.83 MoM; 1.64 vs 0.85 MoM; and 1.73 vs 1.01 MoM, respectively; all P < 0.001). In contrast, levels of serum free β-hCG in the ONTD group were significantly lower than those recorded in the normal group (0.63 vs 0.98 MoM, respectively; P = 0.002); see Table 2 and see Figure 1. In contrast with the original concentration levels of free β-hCG in the normal group, we found no significant differences between 15 and 16, 15 and 17, 16 and 17, 18 and 19, and 19 and 20 gestational weeks (all P > 0.05). Notably, the differences between the other groups were significant (all P < 0.05). Regarding AFP, the differences were similar between 15 and 16, 16 and 17, 18 and 19, and 19 and 20 gestational weeks (all P > 0.05). The differences between the other groups were significant (all P < 0.05). For AFP-L2 concentration, the differences between gestational weeks were not significant (all P > 0.05). For AFP-L3 concentration, the differences between gestational weeks were similar (P > 0.05), except for 16 and 20 gestational weeks (Z = 3.550, P = 0.006) and 17 and 20 gestational weeks (Z = 3.197, P = 0.021); see Figure 2.
Comparison of serum free β-hCG, AFP, AFP-L2, and AFP-L3 levels in two groups.

Free β-hCG, free β subunit of human chorionic gonadotropin; AFP: alpha-fetoprotein; AFP-L2: alpha-fetoprotein variant L2; AFP-L3: alpha-fetoprotein variant L3; ONTD: open neural tube defect; MoM: multiple of median; w: week. Data were expressed for M (P2.5, P97.5).
P < 0.001; **P < 0.05.
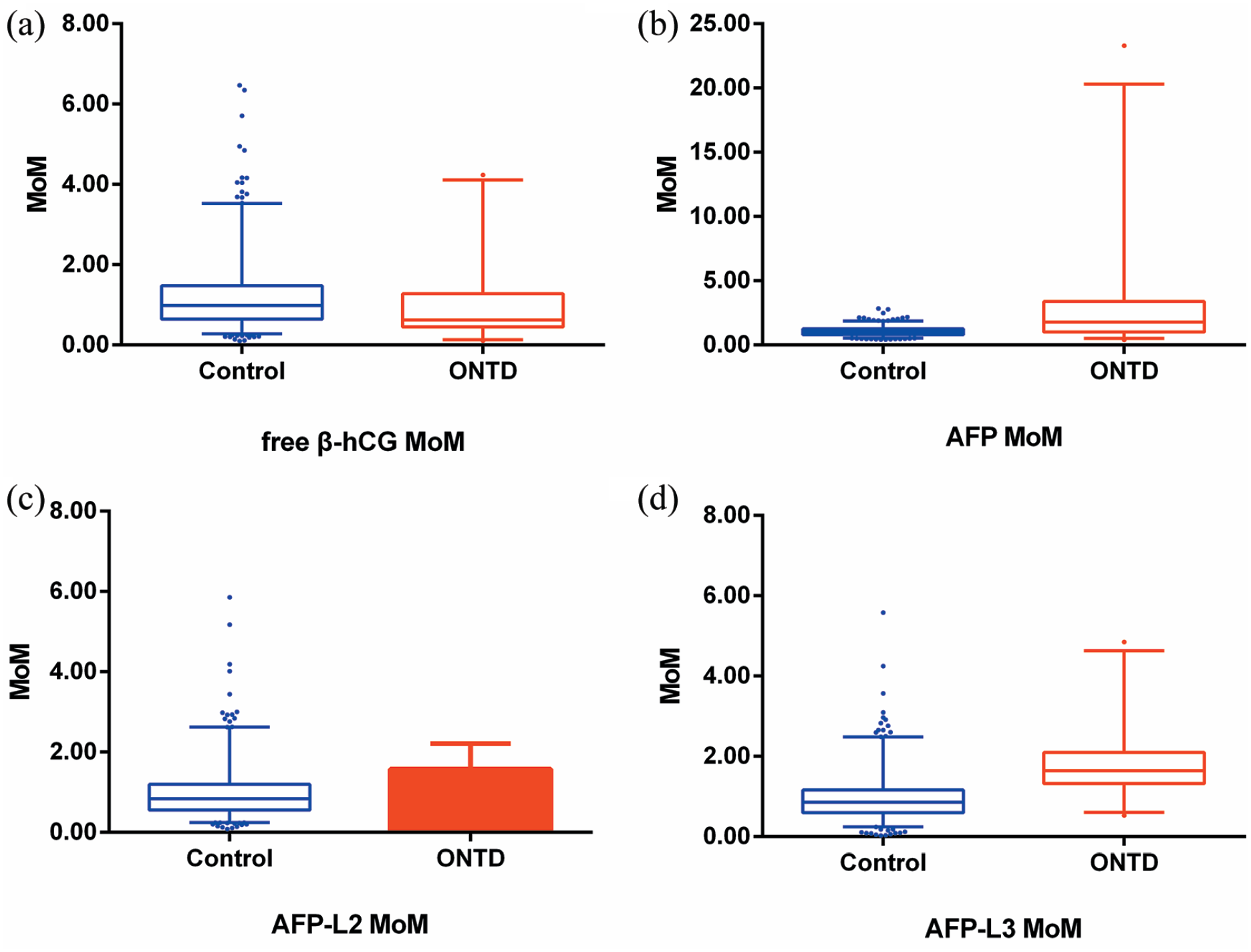
Comparison of serum indicators MoM in two groups. (A color version of this figure is available in the online journal.)

Comparison of normal pregnant women serum indicators in different gestational weeks. (A color version of this figure is available in the online journal.)
In comparison with the MoM value of each marker in the normal group, the free β-hCG MoM at 15 gestational weeks was significantly lower than that recorded at 17 gestational weeks (Z = 3.298, P = 0.015). The AFP MoM at 15 gestational weeks was significantly lower than that determined at 16 gestational weeks (Z = 3.118, P = 0.027). The AFP-L2 MoM at 16 and 17 gestational weeks was significantly lower than that observed in the remaining gestational weeks (P < 0.05). The AFP-L3 MoM at 16 and 17 gestational weeks was significantly lower than that calculated at 15 and 20 gestational weeks (P < 0.05). Of note, the differences were not significant between the remaining groups (all P > 0.05); see Figure 3.
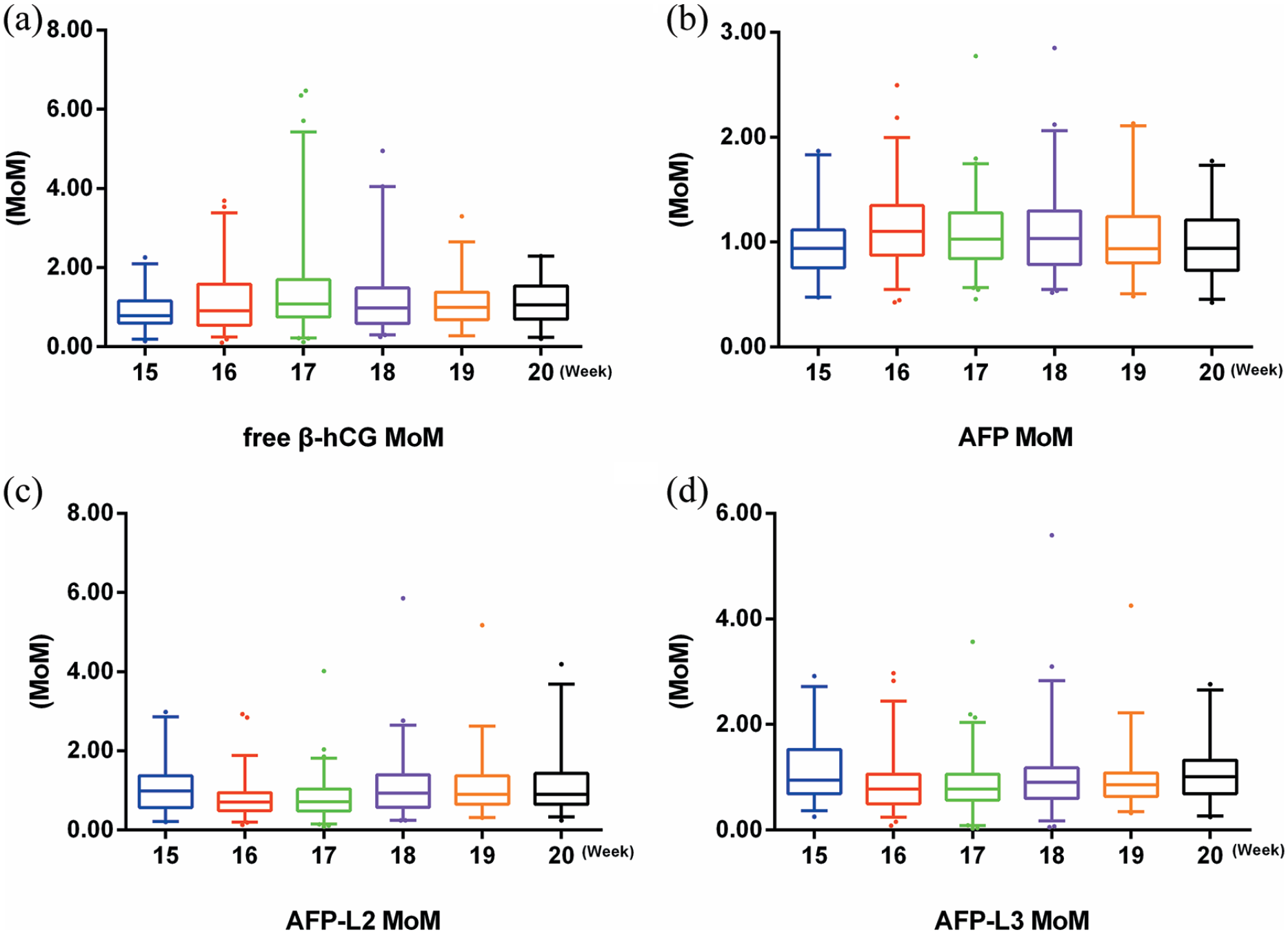
Comparison of normal pregnant women serum indicators MoM in different gestational weeks. (A color version of this figure is available in the online journal.)
Value of individual and combined serum indicators screening for ONTD
The AUCs of AFP-L2 and AFP-L3 screening for ONTD fetuses were 0.804 (95% confidence interval (CI): 0.750–0.858, P < 0.001) and 0.837 (95% CI: 0.787–0.887, P < 0.001), respectively (Table 3). According to the ROC curves of AFP-L2 and AFP-L3, the optimal cutoff values were 1.12 MoM and 1.31 MoM; the sensitivity values were 0.825, and 0.707; and the specificity values were 0.772 and 0.815, respectively (Figure 4). Among the nine models predicting ONTD, the triple-index model of free β-hCG + AFP-L2 + AFP-L3 exhibited the best performance (AUC = 0.905). Among the dual-index models, AFP-L2 + AFP-L3 showed the best predictive value (AUC = 0.885). The order of the AUCs of the single-index models was AFP-L3 > AFP-L2 > AFP > free β-hCG (Table 3; Figure 4).
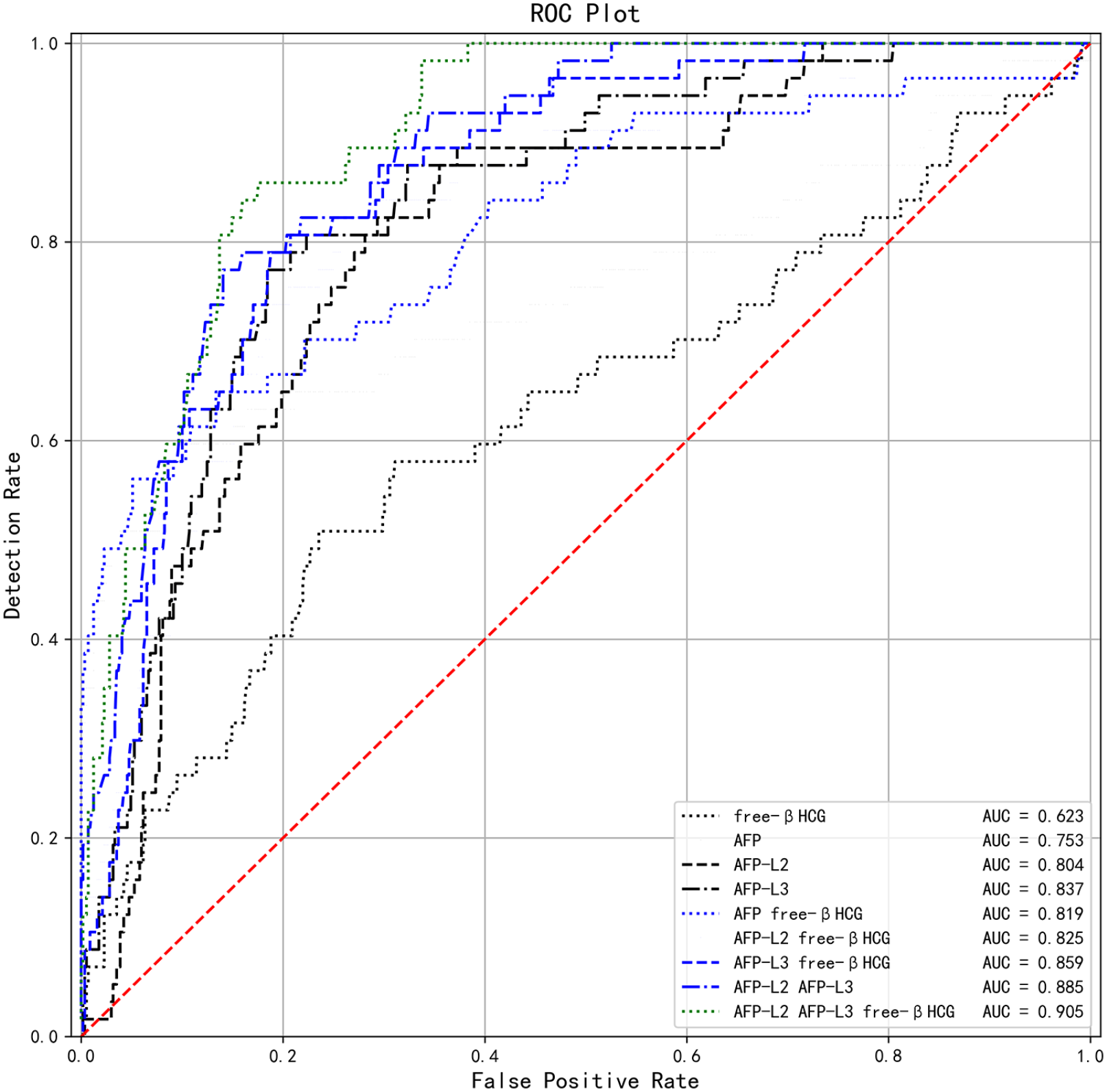
ROC curves of ONTD predicted by different models. (A color version of this figure is available in the online journal.)
The value of individual and combined index screening for ONTD.

ONTD: open neural tube defect; free β-hCG: free β subunit of human chorionic gonadotropin; AFP: alpha-fetoprotein; AFP-L2: alpha-fetoprotein variant L2; AFP-L3: alpha-fetoprotein variant L3; MoM, multiple of median; AUC: area under the curve.
P < 0.001; **P < 0.05.
Predictive evaluation of individual and combined serum indicators for ONTD
In the single-index models, the negative predictive value, false positive rate, and negative LR (−LR) of AFP-L2 and AFP-L3 were better than those of AFP in predicting ONTD. In the dual-index models, negative predictive value, false positive rate, and −LR of AFP-L2 + free β-hCG and AFP-L3 + free β-hCG were better than those of AFP + free β-hCG in predicting ONTD. However, the positive LR (+LR) of AFP and AFP + free β-hCG were preferred. Among the combined models, AFP-L2 + AFP-L3 or AFP-L2 + AFP-L3 + free β-hCG demonstrated superior predictive ability (Table 4).
The predictive evaluation of individual and combined index for ONTD.

ONTD, open neural tube defect; free β-hCG, free β subunit of human chorionic gonadotropin; AFP, alpha-fetoprotein; AFP-L2, alpha-fetoprotein variant L2; AFP-L3, alpha-fetoprotein variant L3; MoM, multiple of median; DR, detection rate; FPR, false positive rate; FNR, false negative rate; PPV, positive predictive value; NPV, negative predictive value; +LR: positive likelihood ratio; –LR: negative likelihood ratio.
The replacement of AFP by AFP-L2 and AFP-L3 reduce the IDI (by 0.89% and 3.65%, respectively) and NRI (by 5.64% and 9.28%, respectively) for predicting ONTD. However, the differences were similar (all P > 0.05). The IDI and NRI for ONTD predicted by AFP-L2 and AFP-L3 combined with free β-hCG instead of AFP were 4.86% and 21.05%, and 7.23% and 21.05%, respectively (Table 5). When the risk threshold was <0.40, the top five decision curve analyses for predicting ONTD using different models were AFP-L2 + free β-hCG, free β-hCG, AFP-L3, AFP + free β-hCG, and AFP (Figure 5).
AFP-L2 and/or AFP-L3 combined with free β-hCG for IDI and NRI of ONTD.
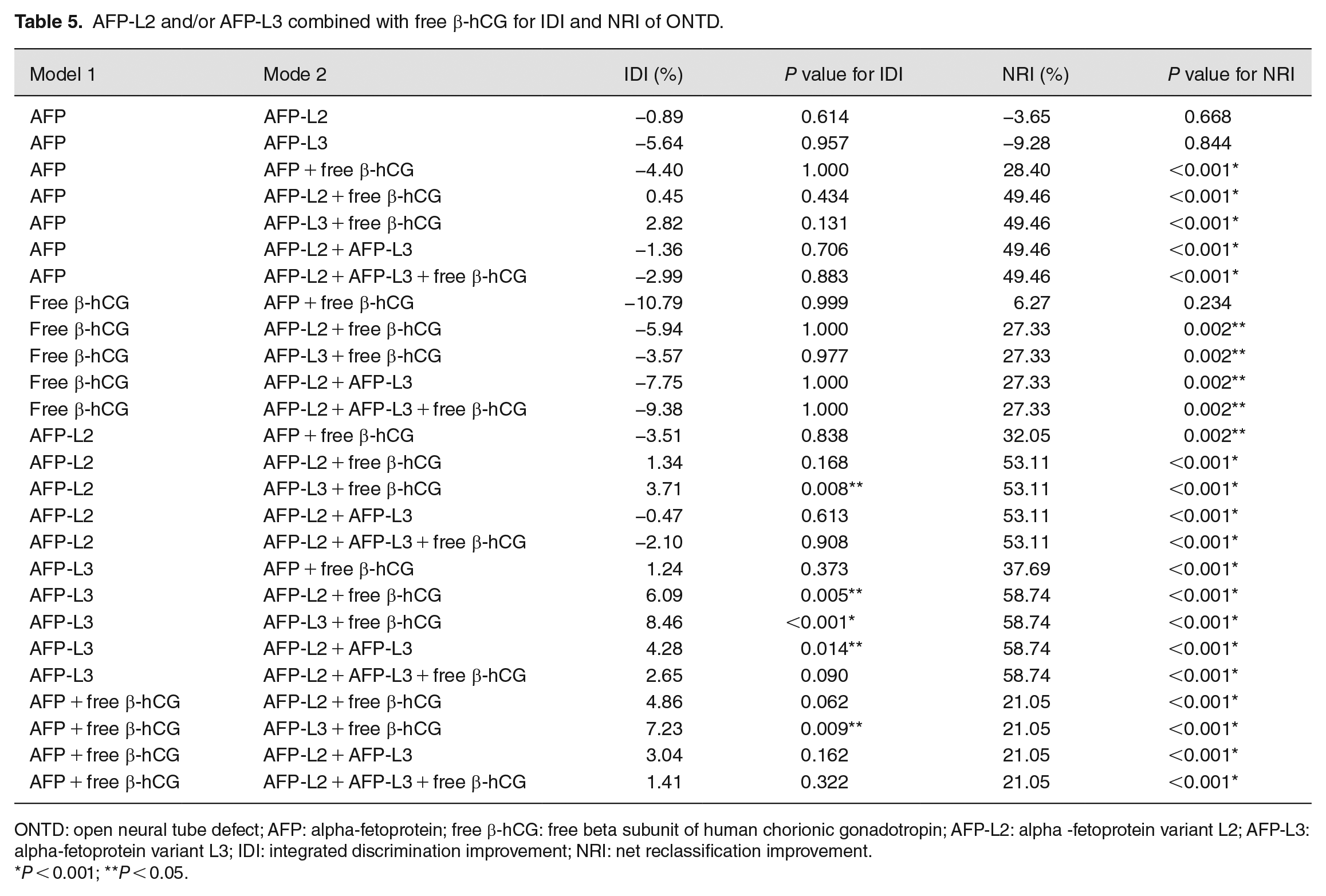
ONTD: open neural tube defect; AFP: alpha-fetoprotein; free β-hCG: free beta subunit of human chorionic gonadotropin; AFP-L2: alpha -fetoprotein variant L2; AFP-L3: alpha-fetoprotein variant L3; IDI: integrated discrimination improvement; NRI: net reclassification improvement.
P < 0.001; **P < 0.05.
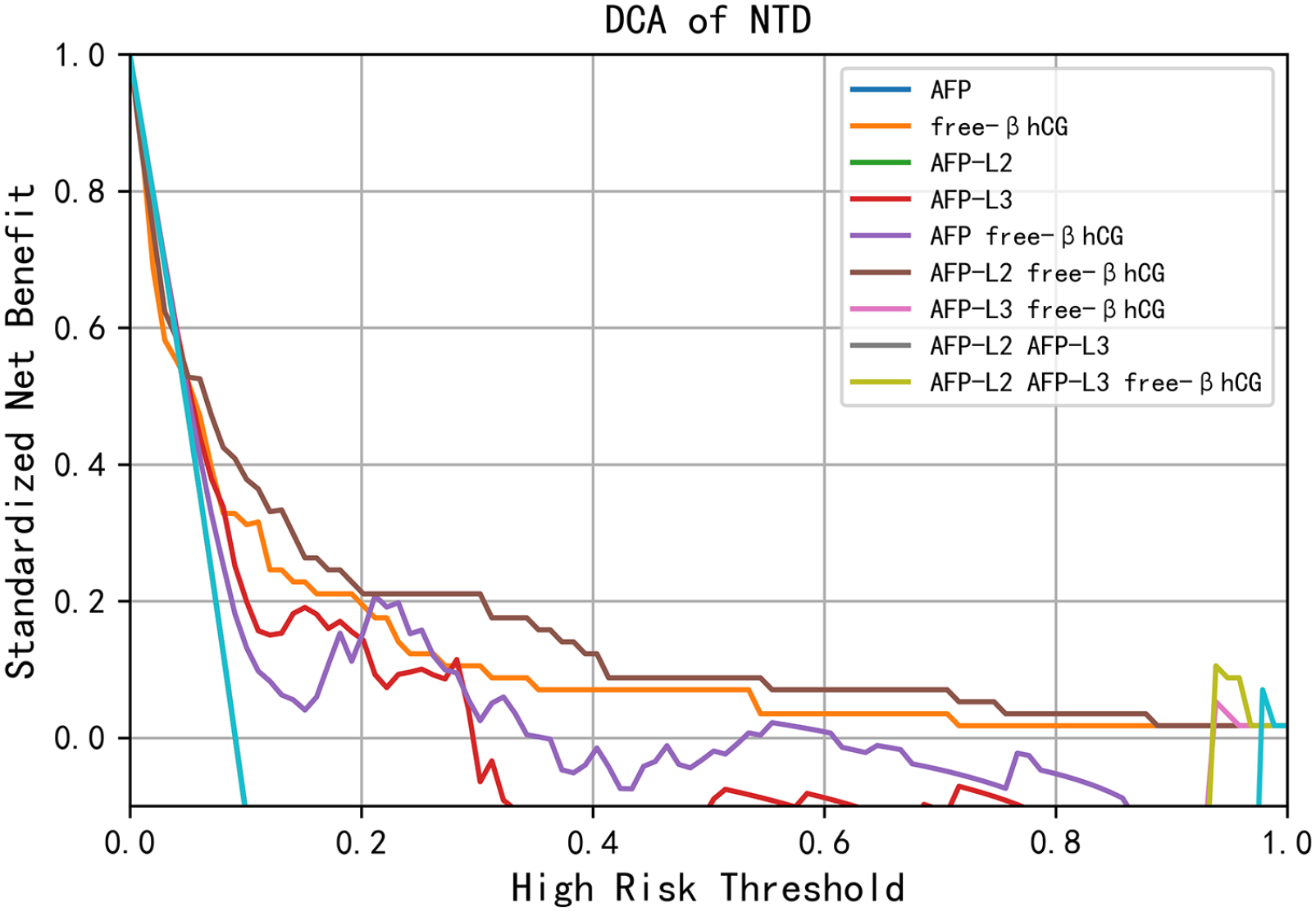
DCAs of ONTD predicted by different models. (A color version of this figure is available in the online journal.)
Discussion
Kelleher et al. 20 and Buamah et al. 21 revealed that measurement of the percentage of AFP unconjugated with lens culinaris agglutinin was a valuable method for the diagnosis of abnormal fetuses, particularly when the increase in AFP concentration in the amniotic fluid was inconspicuous (2–5 standard deviations above the average), the gestational period was unclear, or the total AFP concentration in the amniotic fluid was in conflict with ultrasonographic data. Few studies have reported thus far on maternal serum AFP-L2 and AFP-L3. Hence, this study revealed that serum levels of AFP-L2 and AFP-L3 in pregnant women with ONTD fetuses were significantly higher than those measured in pregnant women with healthy fetuses (all P < 0.001). The results were consistent with previous findings by our research group that the concentrations of AFP-L2 and AFP-L3 in the ONTD and AWD groups were significantly increased, in contrast with the normal group (P < 0.001). 15
As shown in Tables 2 and 3, the levels of free β-hCG in pregnant women with ONTD fetuses were significantly lower than those observed in the normal group (0.63 vs 0.98 MoM, respectively; P = 0.002; AUC = 0.623; 95% CI: 0.538–0.708; P = 0.002). These findings indicated that free β-hCG had diagnostic power for ONTD. As illustrated in Figure 5, the risk calculation model constructed using AFP-L2 + free β-hCG exhibited the best screening efficiency for ONTD, indicating that the combination of free β-hCG improved the efficiency of prediction. This result was different from the traditional belief that AFP rather than free β-hCG could be used in screening for ONTD.8,22,23
Table 2 also showed that the original concentration of AFP-L2 in normal pregnant women was similar between different gestational weeks (all P > 0.05). The AFP-L2 MoM at 16 and 17 gestational weeks was significantly lower than that calculated during the other gestational weeks (all P < 0.05). Inconsistency in the original concentration and MoM value of AFP-L2 at different gestational weeks may be attributed to data normalization and model construction in the modeling process. The concentration of AFP-L2 was calibrated using the gestational age and maternal weight; notably, the sample size at some gestational weeks was small. In addition, Table 1 showed that maternal age and maternal weight in 569 normal pregnant women at different gestational weeks were significantly different (P < 0.05 and P < 0.001, respectively). Therefore, replacing the original concentration with the MoM value is essential to decrease the deviation promoted by gestational age and maternal weight. The original concentrations would decrease with increasing maternal weight.24,25 To reduce the influence of maternal weight and gestational age on the concentration of free β-hCG, AFP, AFP-L2 and AFP-L3, the MoM value was used to calibrate the various markers.26,27
In this study, the AUCs of AFP-L2 and AFP-L3 screening for ONTD fetuses were 0.804 and 0.837, respectively. The order of AUCs for the single-index models was AFP-L3 > AFP-L2 > AFP > free β-hCG; the sensitivity and specificity of AFP-L2 and AFP-L3 were higher than those of AFP. As shown in Tables 4 and 5, the single-index model of AFP-L2, AFP-L3, or combined with free β-hCG, the predictive effect of negative predictive value, false positive rate, and −LR for ONTD were better than those of AFP; however, opposite results were obtained for the +LR. The replacement of AFP by AFP-L2 or AFP-L3 enhanced the IDI and NRI for predicting ONTD. The results confirmed that AFP-L2 and AFP-L3 exhibited dominant performance screening for ONTD versus the traditionally used AFP.
The order of the constructed models for predicting ONTD according to their AUC was as follows: the triple-index model, free β-hCG + AFP-L2 + AFP-L3 (AUC = 0.905); the dual-index model, AFP-L2 + AFP-L3 (AUC = 0.885). The top five decision curve analyses of different models predicting ONTD were AFP-L2 + free β-hCG, free β-hCG, AFP-L3, AFP + free β-hCG, and AFP. Collectively, these results revealed that the multi-index model established by AFP-L2 and AFP-L3, instead of AFP combined with free β-hCG, could enhance ONTD screening efficiency.
DCA is a method for evaluating a predictive model to facilitate decisions regarding test selection and use. AUC is known to be a concordance index, which is the probability that a patient who experiences an event will have a risk score compared to a patient who does not experience the event, but it does not explain whether the actual risk of the predictive model is accurate. 28 In our results, the top DCAs were AFP-L2 + free β-hCG, free β-hCG, and AFP-L3, indicating that AFP-L2 and AFP-L3 might have a superior clinical application value over AFP. NRI and IDI give additional support when evaluating the predictive models. 29 As shown in this study, replacing AFP with AFP-L2 or AFP-L3 in combination with free β-hCG increased the IDI and NRI predicted for ONTD. It demonstrated that replacing AFP with AFP-L2 or AFP-L3 could boost the screening efficiency of the risk model.
The limitations of this study should be acknowledged. First, the MoM values of AFP-L2 and AFP-L3 were indirectly calculated based on the AFP MoM value of 21,656 maternal serum samples in the second trimester. 15 This may have caused some bias in the results. However, MoM values of AFP-L2 and AFP-L3 were calculated in 569 pregnant women with healthy fetuses in this study. Although the present investigation included a larger sample size than our previous study, the number of patients remained low compared with modeling using larger amounts of data. Second, our study was a retrospective, case-control study of accumulated data from two clinical centers. Finally, NRI depended on the definite risk stratification category employed. 30 These factors may have influenced the results of this study.
Conclusions
In summary, maternal serum AFP-L2 and AFP-L3 showed superior performance to AFP with higher sensitivity and specificity screening for ONTD fetuses during the second trimester. Therefore, free β-hCG, AFP-L2, and AFP-L3 are new indicators for screening for ONTD fetuses. The risk calculation model constructed using free β-hCG + AFP-L2 + AFP-L3, or AFP-L2 + free β-hCG exhibited the highest screening efficiency.
Footnotes
Acknowledgements
The authors acknowledge the assistance of Songhe Chen from the medical records room of Hangzhou Women’s Hospital for case collection and data matching. They also thank Xiao Lu, Qianyun Zhou, and Shaolei Lv of the Data Analysis Department of Zhejiang Biosan Biochemical Technologies for their contribution to data matching and model building.
Authors’ contributions
YMC and XW designed the study and performed the statistical analysis. YJC and WWN wrote the first draft of the manuscript. XW, YXY, and WZ contributed to provision of study materials or patients. HW contributed to administrative support, and provision of study materials or patients; JJL and LC performed laboratory measurements; YMC and XW contributed to writing – review and editing. All the authors have accepted responsibility for the entire content of this submitted manuscript and approved submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by Hangzhou Women’s Hospital (Hangzhou Maternity and Child Health Care Hospital) ethics committee, and the approval number was (2018) medical ethics (004) No. 01. The data used in this study were anonymized before its use. Patients’ consent was not required because this was a retrospective study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Zhejiang Public Welfare Technology Research Program/Social Development (Grant number LGF19H040006); Hangzhou Science and Technology Plan Guidance Project (20181228Y13); Hangzhou Medicine and Health Scientific Research Project (2017A055).
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.