
Abstract
Platinum-based chemotherapy, especially carboplatin, is the primary measure to treat patients with ovarian cancer (OC). However, OC patients still have an adverse prognosis due to emergency of chemotherapy resistance. Ovarian serous cystadenocarcinoma (OSC) is the most common histological subtype of OC. Therefore, identifying the key factors that affect chemotherapy resistance and searching novel treatments had become a top priority. In this study, we analyzed carboplatin response-related mRNA, miRNA, DNA methylation, and alternative splicing (AS) and established a drug-resistant signature for carboplatin in OSC. This drug-resistant signature was obviously higher in resistant group than in non-resistant group and had accuracy predictive performance, which demonstrated that this signature could be considered as a superior indicator for OSC patients with carboplatin resistance. Furthermore, we selected three potential small molecule drugs including liranaftate, siguazodan, and tramiprostate to inhibit carboplatin resistance of OSC. In addition, we also identified ZINC00000205417, ZINC00000140928, and ZINC00021908260 were potential small molecule compounds for SLC17A7 based on Molecular Operating Environment (MOE) virtual screening. Finally, we confirmed the drug-like properties of these small molecule drugs via evaluating absorption, distribution, metabolism, elimination, and toxicity (ADMET) property. In summary, the signature could be used as biomarker for carboplatin resistance and small molecule drugs targeting these genes could improve clinical treatment for OSC in the future.
Keywords
Impact Statement
Increasing evidences demonstrated that carboplatin resistance for ovarian cancer (OC) was closely related to DNA methylation. Therefore, it is very meaningful to study the effect of methylation on carboplatin resistance in OC. Nevertheless, the significance of AS in carboplatin resistance for OC has not been fully analyzed. In this study, we systematically evaluated the function of the genome-wide OC-specific mRNA, miRNA, DNA methylation, and AS on carboplatin resistance in OC. Furthermore, we identified an integrated biomarker to indicate the prognosis of patients. Finally, we predicted several potential small molecule compounds, which may be able to fight carboplatin resistance in OC patients.
Introduction
Ovarian cancer (OC) is one of the malignant cancers and is an important cause of death only second to breast cancer in gynecological malignancies. 1 It is estimated that there will be about 21,410 new cases and 13,770 deaths of OC in the United States during 2021. 1 Currently, aggressive surgical reduction plus platinum-based chemotherapy, especially carboplatin, were mainstay treatment for OC to improve their quality of life and decrease mortality.2–4 However, some patients receiving chemotherapy still develop recurrence or metastasis due to high incidences of chemotherapy resistance. Therefore, seeking out indicators for chemotherapy resistance and developing effective therapeutic drugs have become the urgent priority of OC research.
Increasing evidences demonstrated that carboplatin resistance for OC was closely related to DNA methylation. 5 Researchers found the combination of low-dose decitabine (hypomethylation drug) and carboplatin significantly improved the clinical efficacy, including response rate (RR) and progression-free survival (PFS) in a phase II clinical trial. 6 Moreover, Fang et al. 7 also revealed that DNA methylation aberrations were correlated with the acquired resistance of OC to platinum-based drugs. Hence, it is very meaningful to study the effect of methylation on carboplatin resistance in OC. In addition, Chou et al. 8 indicated that cisplatin or carboplatin could restore the enzalutamide sensitivity through degrading the androgen receptor splicing variant 7 (ARv7) in prostate cancer. However, the significance of alternative splicing (AS) in carboplatin resistance for OC has not been fully analyzed.
In this study, all patients downloaded were ovarian serous cystadenocarcinoma (OSC). Moreover, a few studies have identified and clarified key factors of OSC. Therefore, we systematically analyzed the effect of the genome-wide mRNA, miRNA, DNA methylation, and AS on carboplatin resistance in OSC. Furthermore, we identified an integrated biomarker to indicate the prognosis of patients. Finally, we predicted several potential small molecule compounds, which provide the possibility for treating carboplatin resistance of OSC patients.
Materials and methods
Data collection
The gene expression RNAseq, miRNA expression RNAseq, SpliceSeq data, DNA methylation level profiles (Illumina Human Methylation 450 level 3), copy number variation data (CNV, Masked Copy Number Segment hg38), somatic mutation data (SNV, VarScan2 Variant Aggregation, and Masking), and clinical information including drug treatment records of patients were obtained from the TCGA database (https://portal.gdc.cancer.gov/).
Distinguishing drug-non-resistant and drug-resistant OSC patients
OSC patients with “complete response” and “partial response” were regarded as the drug-non-resistant group. OSC patients with “stable disease” and “progressive disease” were regarded as the drug-resistant group.
Differential expressed gene analysis
Differential expressed mRNAs (DEGs) and miRNAs were analyzed between drug-non-resistant and drug-resistant groups by “limma” package with R.
DNA methylation analysis
The “limma” package was used to normalize gene methylation matrices and analyze genes with different DNA methylation levels between drug-non-resistant and drug-resistant groups.
AS events analysis
SpliceSeq was used to quantify the mRNA splicing levels in TCGA samples and to calculate a Percent Spliced In (PSI) value from 0 to 1 for seven kinds of AS events. The PSI value of AS events was used to analysis different AS events between drug-non-resistant and drug-resistant groups.
Construction and validation of drug-resistant-related signature
We established a drug-resistant-related signature using key DEGs, miRNAs, DNA methylation genes, and AS for OSC patients with drug treatment. The univariate Cox regression and LASSO-COX analyses were implemented to determine useful prognostic factors. The integrated signature was established based on the corresponding coefficients.
The Kaplan–Meier curves and time-dependent receiver operating characteristic (ROC) curves were implemented to assess the predictive performance of signature using the “survivalROC” package in R. The univariate and multivariate Cox regression analyses were implemented to assess prognostic effect of signature and clinical characteristics using forest plot R package. Nomogram plot was performed by “rms,” “nomogramEx,” and “regplot” R package. Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway was analyzed using “clusterProfiler” package in R.
Estimation of tumor immune cells infiltrating
The CIBERSOFT algorithm was used to assess 22 types tumor-infiltrating immune cells in OSC, through characterizing the cellular composition of complex tissues based on normalized gene expression profiles. The Mann–Whitney U test was used to compare the distribution of immune cells between the drug-non-resistant and drug-resistant groups.
Identification of potential small molecular drugs and ADMET prediction
The Connectivity Map (CMap) database (https://clue.io) was used to screen small molecule drugs, and the three-dimensional (3D) structure of above small molecule drugs was obtained from the PubChem database (http://www.pubchem.ncbi.nlm.gov). The 3D structure of SLC17A7 was predicted from phyre2 (http://www.sbg.bio.ic.ac.uk/phyre2). Then, we downloaded 1945 small molecule compounds from the ZINC15 database (http://zinc.docking.org/). 9 Virtual screening and molecular docking were implemented using Molecular Operating Environment (MOE) to identify potential drug-repurposing. 10 The PreADMET website (https://preadmet.bmdrc.kr) was used to predict absorption, distribution, metabolism, elimination, and toxicity (ADMET) of small molecule drugs. 11
Statistical analysis
All statistical analyses were performed using R (https://www.r-project.org/, v3.5.1), SPSS 24.0 (SPSS Inc., Chicago, IL, USA). All statistical tests were bilateral, and P < 0.05 was statistically significant.
Results
Differentially expressed gene analysis
To identify key mRNAs and miRNAs that affect carboplatin resistance in OSC, differential expressed mRNAs and miRNAs between drug sensitive and resistant patients were analyzed. In total, 639 DEGs and 22 miRNAs were identified and volcano plots were depicted in Figure 1.
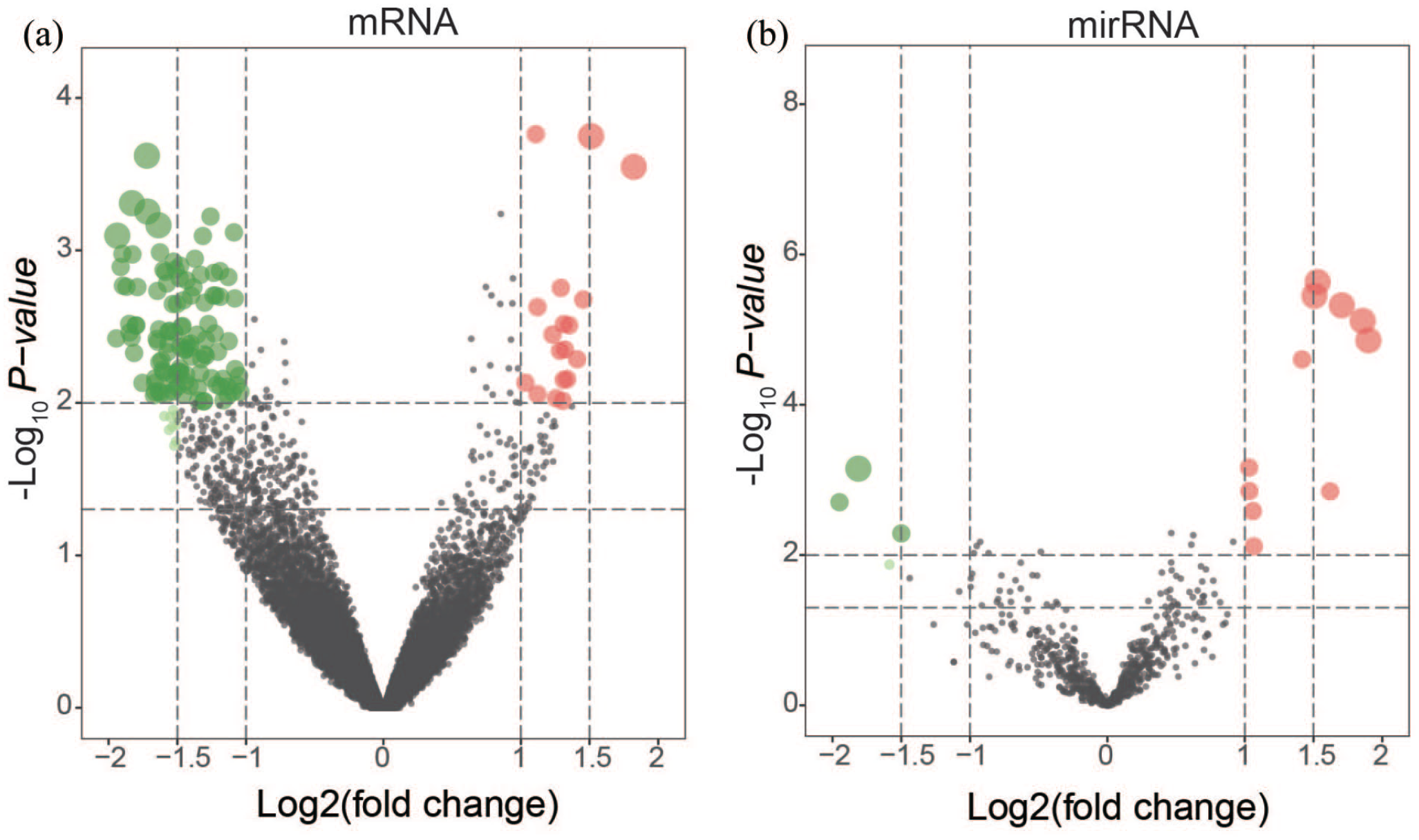
Differential mRNAs and miRNAs between sensitive and resistant OSC patients. (a) The Kaplan–Meier plots between patients with carboplatin resistance and non-resistance. (b) Volcano plot of differential mRNAs. (C) Volcano plot of differential miRNAs. (A color version of this figure is available in the online journal.)
Differences in DNA methylation and AS associated with drug resistance
To investigate the influence of drug resistance on DNA methylation and AS, we identified 1505 genes with different DNA methylation genes and 385 different AS events (The top 100 DNA methylation genes and AS events shown in Supplemental Tables S1 and S2).
Construction and validation of drug-resistant-related signature
The differential genes identified by the above results may affect carboplatin resistance in OSC. Therefore, to identify key prognostic markers, we performed univariate Cox analysis and LASSO-COX regression analysis (Supplemental Figure S1A and B) and built a drug-resistant-related signature based on the corresponding coefficients: risk score = AT of LACTB * (−0.5804) + KIAA2013|693|AT * (−1.7657) + methylation of IFNG-AS1 * 1.1216 + methylation of CDV3 * 0.4417 + methylation of ARPC4-TTLL3 * (−0.2189) + mRNA of FAR2P4 * 0.0956 + mRNA of LRRC31 * (−0.0150) + mRNA of EEF1A1P42 * 0.0273 + mRNA of SLC17A7 * 0.0009. The risk score was higher in drug resistant than in non-resistant group (Figure 2(a)). The Kaplan–Meier analyses were performed and showed that patients with resistance had shorter OS and RFS (Figure 2(b) and Supplemental Figure S2). Then, ROC curves were plotted and showed that the signature exhibited a robust predictive property with area under the curve (AUC) of 0.730, 0.780, and 0.879 at 3-, 5-, and 10 years (Figure 2(c)). Furthermore, univariate and multivariate Cox regression analysis showed that this signature was potential independent prognostic biomarker (P < 0.001, Supplemental Figure 2D and E). These results demonstrated that this signature could be considered as a superior indicator for OSC with carboplatin resistance. We also constructed a prognostic nomogram integrating signature and clinical information, analyzed the relationship between signature and clinical characteristics of OSC patients, and found risk score was obviously related to cancer status (Supplemental Table S3). These results indicated that the combination of this signature and clinical information has better prognostic value. Furthermore, we have performed survival analysis of signature in patients with high-grade and low-grade OSC, respectively, and found this drug-resistant signature had favorable predictive prognostic value both in high- and low-grade OC groups (Supplemental Figure 2G and H). These results indicated that this signature had broad prognostic value for OSC patients.

Evaluating of signature for OSC with carboplatin. (a) The distribution of signature between non-resistant and resistant OSC patients. (b) The Kaplan–Meier plots of signature in patients with carboplatin. (c) The ROC curves for OS of signature in patients with carboplatin. Forest plots of hazard ratios of risk score and clinical characteristics from univariate Cox analyses (d) and multivariate Cox analyses (e). (f) The nomogram to predict patients’ 3- and 5-year OS. The Kaplan–Meier plots of signature in low-grade (g) and high-grade (h) ovarian serous cystadenocarcinoma. (A color version of this figure is available in the online journal.)
To further explore biological process as well as signaling pathways of signature, GO and KEGG analyses were performed using DEGs between high-risk and low-risk groups (Figures 3 and 4). Interestingly, it was observed that GO analysis was mainly concentrated in immune-related pathways including humoral immune response, lymphocyte mediated immunity, and so on in high-risk group (Figure 3).
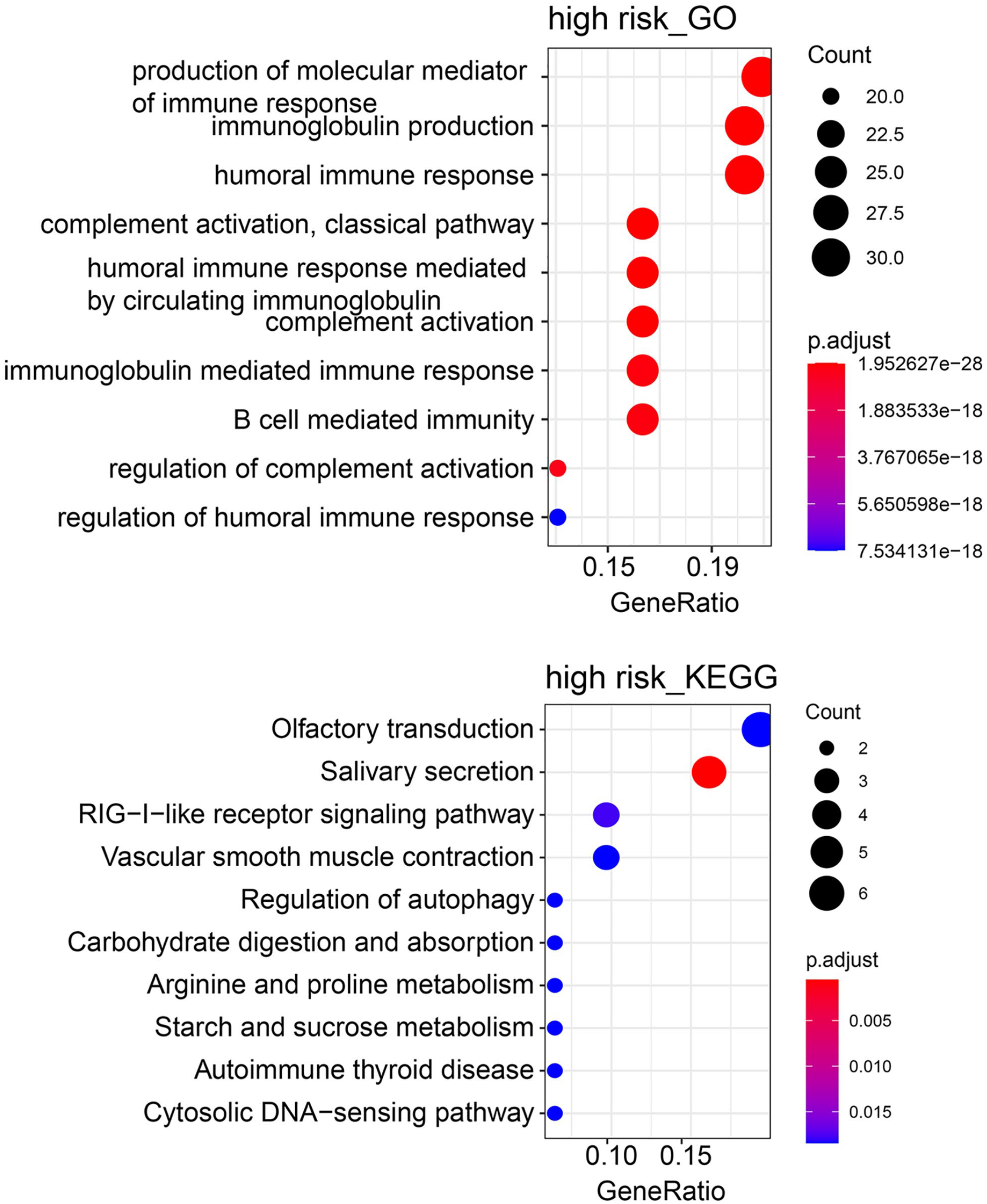
GO and KEGG analyses of high-risk group. (A color version of this figure is available in the online journal.)
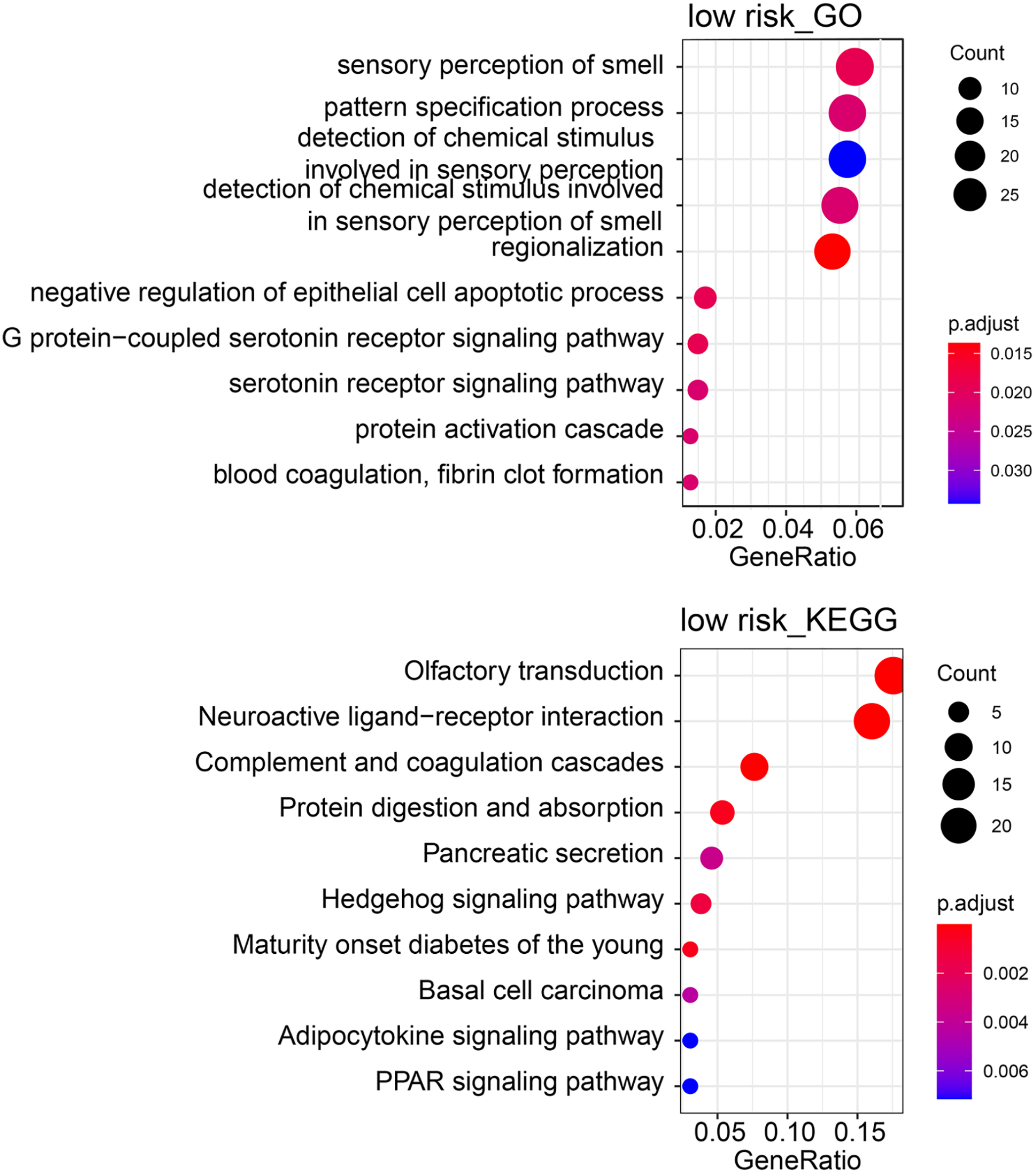
GO and KEGG analyses of low-risk group. (A color version of this figure is available in the online journal.)
Tumor microenvironment cell infiltration characteristics associated with drug resistance
The above results demonstrated that the signature had a well association with immune response. Hence, we concentrated further analysis on the signature tumor microenvironment (TME) cell infiltration characteristics. The results revealed that Dendritic cells resting and the fraction of B cells naive were significantly higher in high-risk than that in low-risk group, indicating that the higher the risk score, the more immune infiltration in OSC (Figure 5).
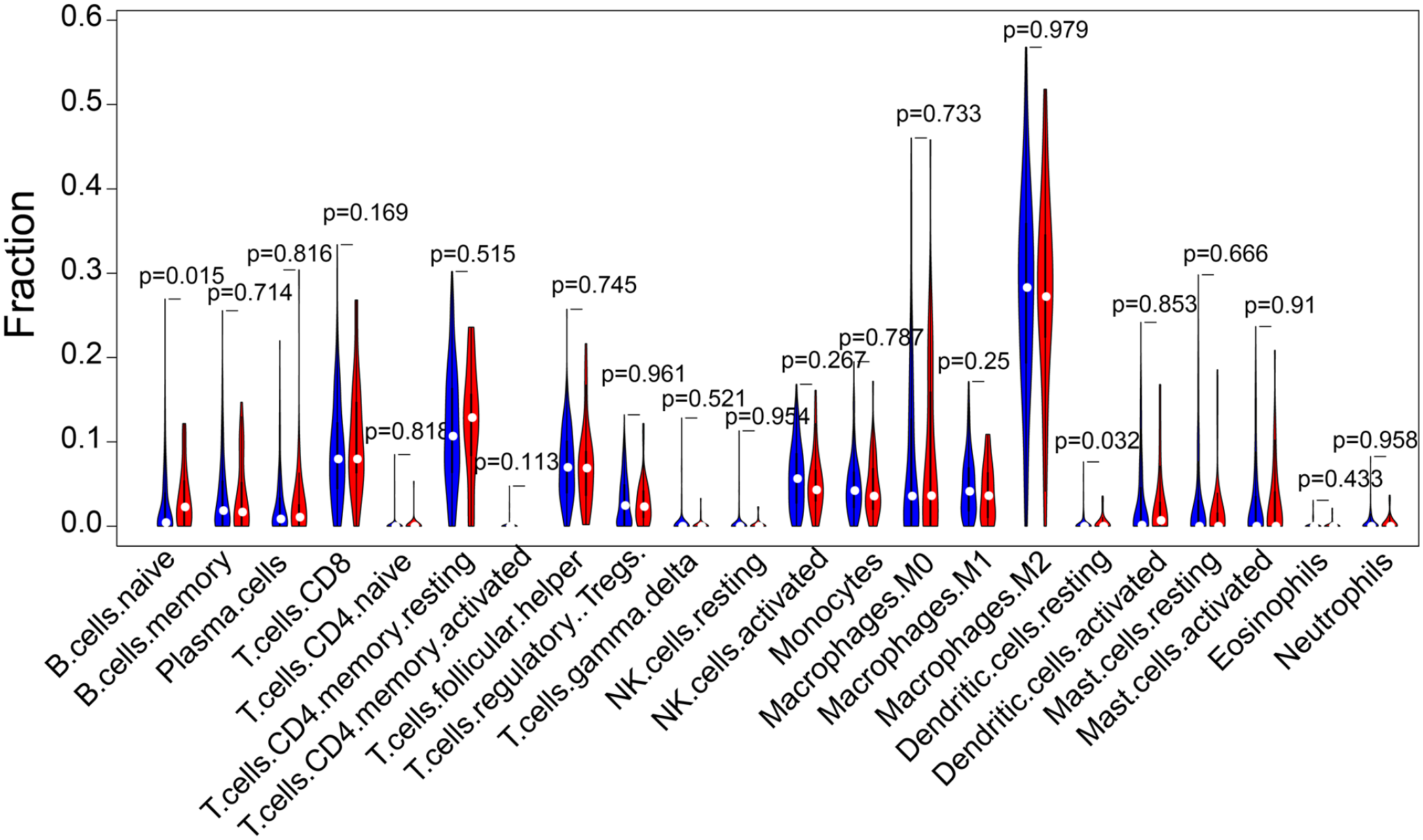
The violin plot of the 22 immune cell proportions between high-risk and low-risk groups. (A color version of this figure is available in the online journal.)
Related small molecule compounds screening
To solve the OSC patients’ drug resistance, we tried to predict several potential small molecule compounds. We identified some differential genes between high- and low-risk groups as well as put those genes into CMap database for screening small molecule drugs. In the results, we selected the top three small molecule drugs, including liranaftate, siguazodan, and tramiprostate and showed the 3D structure of these compounds (Figure 6). These drugs might improve sensitivity of OSC for carboplatin.
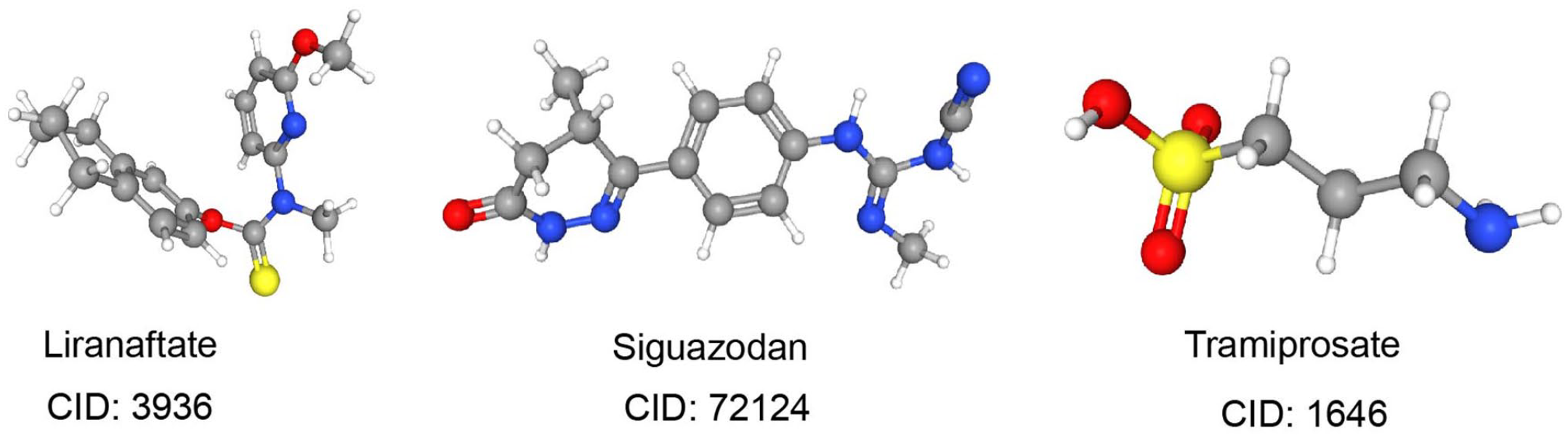
The 3D structure of the top three significant small molecule drugs. (A color version of this figure is available in the online journal.)
Furthermore, in our signature, SLC17A7 was encoding protein and had a poor prognosis, which might promote the development of OSC. First, we predicted a 3D protein structure of SLC17A7 using phyre2 database. Then, we identified the top three small molecule compounds including ZINC00000205417, ZINC00000140928, and ZINC00021908260 that have binding sites with SLC17A7 using the MOE software (Table 1 and Figure 7). Supplemental Table S4 showed the top 100 compounds that bind to SLC17A7. We noticed the main hydrogen bonding interactions between SLC17A7 and three small molecule compounds as well as the active site residues. For ZINC00000205417, an amino group accepted an H-bond from His263. For ZINC00000140928, the carbonyl group and side chain oxygen produced two H bonds with Arg61 and His263, separately. ZINC00021908260 formed five H-bond interactions with Lys290, Gln495, Lys494, and Gly279, respectively. These results manifested that these small molecule compounds might potentially inhibit the resistance of OSC.
The structure and docking results of the top three small molecules.

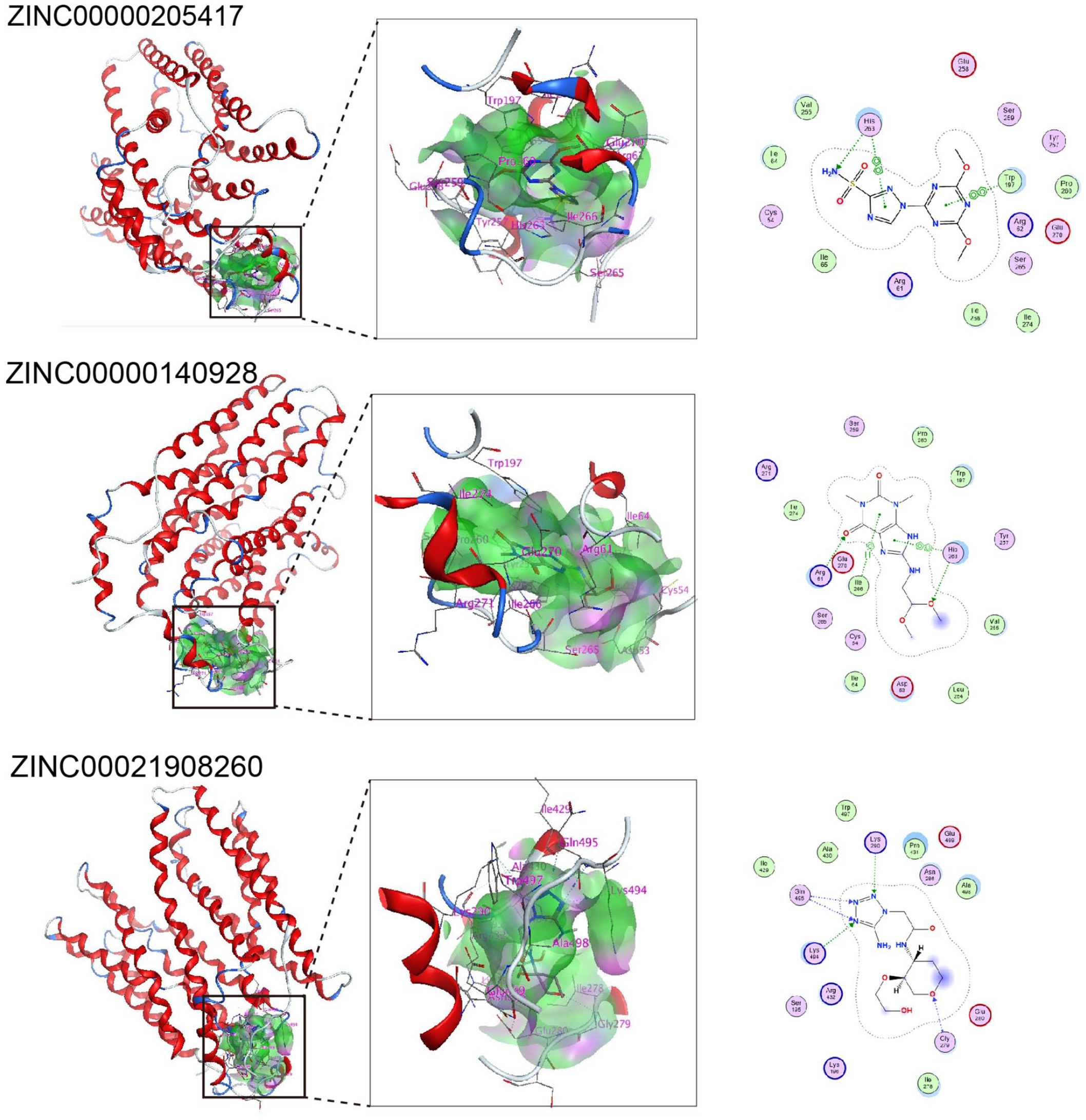
Binding interactions of the top three molecules and SLC17A7. (A color version of this figure is available in the online journal.)
ADMET prediction of small molecule drugs
It is critical for drug development to have advantageous ADMET properties. 11 Adverse pharmacokinetics and toxicity were two important reasons for the high cost in the late-stage of drug development. 12 Thus, the ADMET properties of these molecules were necessary to explore. In this study, we analyzed some ADMET characteristics such as buffer solubility, blood–brain barrier (BBB) penetration, Caco-2 permeability, human intestinal absorption (HIA), plasma protein binding (PPB), cytochrome P450 2D6 (CYP2D6) modulation, and human ether-a-go-go-related gene (hERG) inhibition. The results were shown in Table 2. Buffer solubility and HIA were the two basic factors that influence oral bioavailability. The results showed that tramiprosate, ZINC00000205417, ZINC00000140928, and ZINC00021908260 had extremely high solubility. It was found that all these compounds have low BBB permeability, which helped to reduce brain’s side effects and toxicity. Moreover, C.brain/C.blood in all compounds was less than 1, indicating that they might be inactive in the central nervous system (CNS). These compounds’ suitability for oral administration could be evaluated by Caco-2 permeability. According to the results, liranaftate had better human intestinal permeability, whereas tramiprosate and ZINC00021908260 had worse human intestinal permeability. And liranaftate had better bioavailability compared with other compounds based on the results of HIA. Liranaftate had high plasma protein binding, which indicated it had a long half-life and better curative effect. The functional changes of CYP2D6 could lead to adverse drug reactions and even reduce drug efficacy. 13 Fortunately, the results demonstrated none of these drugs might inhibit CYP2D6. The high risk of hERG inhibition may cause cardiotoxicity and lead to drug failure.14,15 As shown in Table 2, all of these compounds had low risk or medium risk of hERG inhibition, suggesting that they might have little cardiac problems. More ADMET prediction results for these compounds are shown in Supplemental Tables S5 and S6.
The absorption, distribution, metabolism, elimination, and toxicity (ADMET) prediction for the investigated compounds.
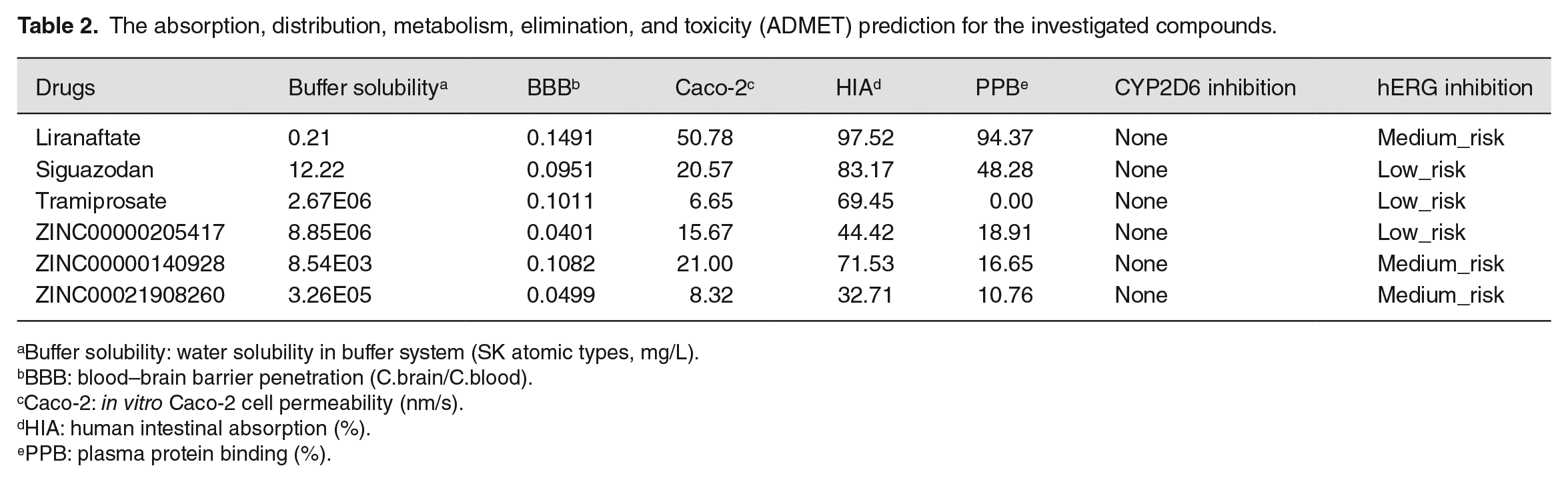
Buffer solubility: water solubility in buffer system (SK atomic types, mg/L).
BBB: blood–brain barrier penetration (C.brain/C.blood).
Caco-2: in vitro Caco-2 cell permeability (nm/s).
HIA: human intestinal absorption (%).
PPB: plasma protein binding (%).
Discussion
In recent years, malignant OC has been greatly improved due to the use of chemotherapy, especially platinum-based chemotherapy. 1 However, drug resistance and high recurrence rate might lead to chemotherapy failure and become a new challenge for OC. Accumulating studies has explored some potential mechanisms of platinum resistance in OC. For example, Zhou et al. 2 found adipocytes could promote carboplatin resistance of OC via ANGPTL4. Autophagy and gene mutation lead to platinum-drug resistance.16,17 In addition, some researchers were looking for novel drugs to inhibit resistance. WEE1 inhibitor AZD1775 was proven to improve the carboplatin’s curative effect in patients with TP53-mutated OC. 18 IAP inhibitor DEBIO1143 could reverse carboplatin resistance of OC. 19 Unfortunately, no satisfactory answer had been found for carboplatin resistance in OC, especially OSC. Therefore, it is an urgent to find new targeted drugs for OSC. In this study, we analyzed the mRNA, miRNA, AS, and DNA methylation levels of patients treated with carboplatin for OSC, aiming to explore the key factors affecting carboplatin resistance. Moreover, we predicted several potential small molecule drugs to reduce carboplatin resistance, which provides a foundation for future clinical research.
The dysregulation of AS events had been found to be related to OC tumorigenesis. For example, Michael et al. 20 found RBFOX2-mediated AS regulated by MALAT1 could promote OC progression. In addition, Roscoe et al. 21 discovered 48 highly cancer-specific AS events in OC via high-throughput reverse transcription polymerase chain reaction (RT-PCR) platform. Furthermore, AS could disrupt genes related to drug response in cancer cells. These abnormal splicing events, which may be take part in drug metabolism, DNA damage reactions, and so on. 22 Studies have observed abnormal drug targets’ splicing in melanomas and prostate cancer. More than 50% of melanomas carry BRAF mutations, which makes cells insensitive to RAF inhibitors.23,24 However, a few studies have observed AS genes for drug resistance in OSC. Fortunately, in this study, we identified the AT type of LACTB and KIAA2013 were related to the survival of patients treated with carboplatin. It is reported that LACTB has multiple splice isoforms in leukemia cell lines, including XR1, V1, V2, and V3. However, the significance of LACTB and KIAA2013’s splice isoforms in cancers had not been discovered. These results provide the possibility that AS also affects the response of OSC to carboplatin.
Platinum-based chemotherapy includes carboplatin could exert cytotoxic effects through combining with DNA to produce platinum-DNA adducts, causing inter- or intra-strand crosslinks, which can damage the DNA helix and influence DNA replication. However, if the repair pathway that causes cell death is epigenetically inactivated by DNA methylation after platinum-based chemotherapy, cell death might not be triggered. 25 Therefore, targeting DNA methylation might enhance the sensitivity of OSC to platinum drugs. Furthermore, increasing studies have demonstrated that DNA methylation is participated in carboplatin resistance in OC. For example, Andrew et al. 26 revealed that HOX antisense intergenic RNA (HOTAIR) and its alternative DNA methylation could serve as marker to indicate carboplatin resistance. Aberrant SERPINE1 DNA methylation was found to be participated in epithelial–mesenchymal transition induced by carboplatin in OC. 27 In this study, the DNA methylation of IFNG-AS1 and CDV3 was related to prolonged survival, whereas methylation of ARPC4-TTLL3 was associated with poor survival. Although theses genes’ roles in OSC or other cancers were presently unclear, our studies indicate that they are worthy of further investigation.
In addition, we also identified several key resistance-associated mRNAs including FAR2P4, LRRC31, EEF1A1P42, and SLC17A7. Chen et al. 28 suggested LRRC31 could sensitize cancer to radiation therapy via inhibiting DNA repair. Our research also proved that LRRC31 played an inhibitory effect. SLC17A7 was confirmed as a prognostic biomarker for uveal melanoma 29 and colon cancer. 30
More importantly, we screened out three small molecule compounds including liranaftate, siguazodan, and tramiprostate to inhibit carboplatin resistance for OSC using CMap database. Liranaftate is considered as a type of thiocarbamate antifungal agent, which has fungicidal activity. Siguazodan with inotropic and vasodilator activities is a selective phosphodiesterase (PDE) inhibitor. 31 Tramiprostate was reported to have a potential protective effect on Alzheimer’s disease. 32 However, the effects of these small molecule drugs on OSC still need further verification. Moreover, we also explored potential small molecule drugs by virtual screening and molecular docking targeting SLC17A7. We identified ZINC00000205417, ZINC00000140928, and ZINC00021908260 were potential drugs for treatment of SLC17A7. These small molecule drugs provide the possibility to reduce carboplatin resistance of OSC.
Finally, we predicted the ADMET properties of these molecules via PreADMET server. Liranaftate and siguazodan have favorable ADMET properties except low buffer solubility, which should be improved in the future. Tramiprosate had extremely low Caco-2 permeability and plasma protein binding rate. According to results, ZINC00000205417, ZINC00000140928, and ZINC00021908260 might become helpful and valuable drugs to improve the treatment of OSC.
In conclusion, we identified an integrated prognostic biomarker consisting of mRNA, AS, and methylation for OSC patients with carboplatin resistance. Eventually, we screened out several small molecule compounds to inhibit carboplatin resistance. These findings might provide help for the development of drugs and the improvement of patients’ prognosis.
Supplemental Material
sj-docx-1-ebm-10.1177_15353702221083254 – Supplemental material for Inferences of carboplatin response-related signature by integrating multiomics data in ovarian serous cystadenocarcinoma
Supplemental material, sj-docx-1-ebm-10.1177_15353702221083254 for Inferences of carboplatin response-related signature by integrating multiomics data in ovarian serous cystadenocarcinoma by Jia-qing Yan, Min Liu, Ying-lin Ma, Kai-di Le, Bin Dong and Guo-hui Li in Experimental Biology and Medicine
Footnotes
Authors’ Contributions
All the authors participated in the design, interpretation of the studies and analysis of the data, and review of the manuscript; GHL participated in conceptualization; JQY conducted the experiments and wrote the original draft; ML, YLM, KDL, and BD contributed to review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.