
Abstract
Mechanical ventilation (MV) is a lifesaving therapy for patients with acute or chronic respiratory failure. Despite, it can also cause lung injury by inducing or worsening inflammatory responses and oxidative stress. Several clinical approaches have protective effects on the lungs, including the prone position and exogenous surfactant; however, few studies have evaluated the association between the two strategies, especially in individuals without previous lung injury. We tested the hypothesis that the effects of the homogenization in lung aeration caused by the prone position in association with the anti-inflammatory properties of exogenous surfactant pre-treatment could have a cumulative protective effect against ventilator-induced lung injury. Therefore, Wistar rats were divided into four experimental groups: Mechanical Ventilation in Supine Position (MVSP), Mechanical Ventilation in Prone position (MVPP), Mechanical Ventilation in Supine Position + surfactant (MVSPS), and Mechanical Ventilation in Prone Position + Surfactant (MVPPS). The intranasal instillation of a porcine surfactant (Curosurf®) was performed in the animals of MVSPS and MVPPS 1 h before the MV, all the rats were subjected to MV for 1 h. The prone position in association with surfactant decreased mRNA expression levels of pro-inflammatory cytokines in ventilated animals compared to the supine position; in addition, the NfκB was lower in MVPP, MVSPS and MVPPS when compared to MVSP. However, it had no effects on oxidative stress caused by MV. Pre-treatment with exogenous surfactant was more efficient in promoting lung protection than the prone position, as it also reduced oxidative damage in the lung parenchyma. Nevertheless, the surfactant did not cause additional improvements in most parameters that were also improved by the prone position. Our results indicate that the pre-treatment with exogenous surfactant, regardless of the position adopted in mechanical ventilation, preserves the original lung histoarchitecture, reduces redox imbalance, and reduces acute inflammatory responses caused by mechanical ventilation in healthy adult Wistar rats.
Impact Statement
Each year, millions of patients require mechanical ventilation (MV), although it has an important therapeutic role MV can induce lung injury. Multiple strategies have been studied and one is prone positioning, another strategy is the administration of exogenous surfactant. The results show that healthy animals submitted to MV with high tidal volume, pre-treatment with surfactant, regardless of the position used to ventilate the animals, promoted a protective effect on the lungs. Our data suggest that the administration of exogenous surfactant may represent a safe alternative to reduce the deleterious effects of MV, especially when prone position is contraindicated or difficult to perform.
Introduction
Mechanical ventilation (MV) is a tool used in patients with acute or chronic respiratory failure. Its main aim is to maintain an adequate gas exchange in the lungs. 1 Each year, millions of patients worldwide require ventilatory support because of several factors, including surgery, unconsciousness, or lack of physiological oxygenation, as for severe cases of COVID-19.2,3 Although, MV has an important therapeutic role, it may cause an acute lung injury, called ventilator-induced lung injury (VILI). 4 The mechanisms involved in the development of VILI are not understood, however, studies have shown that the mechanical forces exerted on the components of the pulmonary parenchyma led to recruitment of leukocytes, production of inflammatory mediators, and tissue injury.5,6 MV activates NF-κB, a transcription factor responsible for inducing immune responses, increasing the expression of cytokines such as IL-6, IL-8, and TNF-α.7,8 Also, MV increases alveolar permeability, allowing the influx of inflammatory cells, especially neutrophils. 5 The cyclic stretching of pulmonary epithelial cells that occur during ventilatory incursions performed by MV induces the release of reactive oxygen species (ROS). 9 ROS plays an important physiological role because of their performance as secondary messengers, which modulates intracellular signaling. 10 However, when the concentrations of ROS are temporarily or chronically increased, as during MV, it causes oxidative stress, a condition that causes disorders in cellular metabolism and damages in cellular components such as lipids, proteins, and DNA.11,12
Multiple strategies have been investigated to minimize the adverse effects of MV, one of them being the prone positioning of patients. Studies have already been shown using the prone position (PP) during MV raises oxygenation, 13 and attenuates VILI. 14 These improved outcomes have been associated with a decrease in the hyperinflation of the alveoli because of a more homogeneous distribution of the mechanical forces and the aeration of the lungs, which recruits a greater part of the lungs during ventilation. 15 Furthermore, studies suggest that early adoption of the prone position during MV reduces mortality in severe conditions. 16 The pandemic caused by the new coronavirus boosted the number of patients admitted to intensive care units and the use of invasive ventilatory support. 17 In this context, the prone position was a widely used strategy to improve survival. Studies indicate mechanical ventilation in a prone position increases the oxygenation of the critically ill patient with COVID-19,18,19 and it is associated with a lower risk of progression from moderate to severe or critical cases. 20
Another strategy to prevent lung injury caused by MV is the administration of exogenous surfactant. Surfactant is a phospholipid substance produced by type II epithelial cells, in which, its main function is to reduce surface tension at the air–liquid interface inside the alveoli.21,22 The pre-treatment with exogenous surfactant has proven to reduce inflammation and oxidative stress in the lungs induced by ventilator-induced lesions in different experimental models and clinical studies.22 –25 However, there are no experimental or clinical studies that evaluate the effects of the prone position in association with the administration of surfactant in preventing or reducing VILI. Therefore, this study aims to evaluate the effects of the prone position associated with exogenous surfactant administration in Wistar rats submitted to mechanical ventilation.
Materials and methods
Animals
In this study we used 20 male Wistar rats, aged between 12 and 14 weeks, weighing between 350 and 400 g, from the Center of Animal Science of the Federal University of Ouro Preto (CCA/UFOP). The animals were kept under controlled conditions of temperature (21°C ± 2°C), humidity (50 ± 10%), luminosity (12 h light/dark cycle), and received water and balanced standard feed ad libitum. The experimental procedures performed followed the Ethical Principles of Animal Experimentation established by the Ethics Commission on the Use of Animals of the Federal University of Ouro Preto (CEUA-UFOP) and were approved on protocol number No. 1492160320.
Experimental design
Twenty animals were divided into four experimental groups (n = 5): Mechanical Ventilation Group in Supine Position (MVSP), in which, the animals were artificially ventilated for 1 h in the supine position; Mechanical Ventilation group in Prone position (MVPP), where the animals were artificially ventilated for 1 h in the prone position; Mechanical Ventilation Group in Supine Position + surfactant (MVSPS) where the animals received exogenous surfactant through intranasal instillation and were artificially ventilated for 1 h in the supine position; Mechanical Ventilation Group in Prone Position + Surfactant (MVPPS), in which, the animals were administered exogenous surfactant through intranasal instillation and were subjected to artificial ventilation in the prone position and received exogenous surfactant through intranasal instillation.
Surfactant administration
The animals of the groups MVSPS and MVPPS received exogenous surfactant, phospholipid fraction of porcine lung, poractant alfa (Curosurf®) intranasally. The animals were placed in a chamber for sedation with isoflurane 2%. Anesthesia was performed to ensure complete inhibition of upper airway reflexes causing the solutions to be transferred to the lung. Each animal received 2.0 mL/kg of surfactant in a single dose 1 h before the beginning of the experimental procedures.24,25
Collection of hemodynamic parameters
The evaluation of the different cardiovascular parameters was performed through the direct recording of blood pressure in anesthetized animals. For that, we inserted a catheter into the femoral artery, and coupled it to a computerized data acquisition system. Initially, the animals were anesthetized intraperitoneally with a mixture of ketamine (80 mg/kg) and midazolam (5 mg/kg). We then made a small incision in the skin to separate the musculature and expose the femoral vascular-nervous bundle, allowing the cannulation of the femoral artery. Mean blood pressure (MAP) was monitored by a Gould pressure transducer connected to an amplifier (ML221 Bridge Amp). The heart rate (HR) was continuously sampled by a 16-bit analog/digital conversion system (PowerLab 4/30) at a sample rate of 100 Hz, and the range amplitude was previously defined at 20 mV. Subsequently, the signal was processed by a software (Lab Chart 7) to obtain the MAP, time characteristics and maximum changes of the desired parameters. MAP and HR were derived in real-time from pulsatile blood pressure pulses using Chart 5 software.26,27 In addition, the body temperature of the animals were monitored throughout the mechanical ventilation procedure.
Mechanical ventilation
After cannulation of the femoral artery, the animals were prepared for mechanical ventilation. We have made a median incision in the anterior cervical region; the musculature was dissected and then the trachea was exposed. The tracheostomy was performed using an 18G catheter. Then, we introduced the ventilator cannula into the trachea and the animal connected to the mechanical ventilator (Inspira, Advanced Safety Ventilator, Harvard/Holliston Apparatus, MA, USA). The animals of the groups MVPP and MVPPS were maneuvered into the prone position after the tracheostomy procedure.
The ventilator was configured in volume-controlled mode, with adjusted parameters: tidal volume (TV) of 12 mL/kg, positive end expiratory pressure (PEEP) of 3 cmH2O, mean respiratory rate (RR) of 70 breaths/min, Inspiration/Expiration ratio (I: E) of 1:2 and inspired oxygen fraction (FiO2) of 21%, for 1 h. After being connected to the mechanical ventilator, the neuromuscular blocker suxamethonium (1 mL/kg) chloride was administered intravenously. 28 During the course of mechanical ventilation, the peak pressure was monitored and static compliance as well as airway resistance were calculated. At the end of ventilation, the animals were euthanized by exsanguination and cardiac puncture.
Bronchoalveolar lavage fluid collection
Immediately after euthanasia, the bronchoalveolar lavage fluid (BALF) was collected according to protocol. The rats were tracheostomized with a catheter (18G) coupled to a 1-mL syringe and the lungs were perfused with saline solution (0.9% NaCl). This procedure was performed three times, totaling a final volume of 2.5 to 3.0 mL of collected fluid. The samples were stored in polypropylene tubes and kept on ice until the end of the experimental procedure to avoid cell lysis.26,27 At the end of the experiment BALF samples were stored in a −80°C freezer and used for the determination of myeloperoxidase activity.
Lung tissue collection
After the performance of BALF collection, the right ventricle was infused with saline solution for blood removal in the lungs. The lung was removed and its mass was determined. Subsequently, 100 mg aliquots of the right lung were made and stored at −80°C for the biochemical analysis and the gene expression analysis of inflammatory markers. The left lung was immersed in a fixative solution (10% buffered formaldehyde) and included in paraffin. Five-µm slides of the paraffinized lung were stained with hematoxylin and eosin for morphometric analysis of the pulmonary parenchyma. 27
Analysis of antioxidant defense and biomarkers of oxidative stress
In order to perform the analyses of oxidative stress markers 100 mg of lung were homogenized with 1 ml of phosphate buffer (0.01 M; pH 7.8). The samples were centrifuged at 4°C for 10 min and 13,000 r/min, and the supernatant stored at −80°C. Pulmonary homogenate was used to analyze antioxidant defense and oxidative damage. The superoxide dismutase (SOD) activity was determined as described by Marklund and Marklund, which is based on the ability of the enzyme to inhibit pyrogallol auto-oxidation. 29 Catalase activity (CAT) was determined according to the method described by Aebi. 30 Glutathione analysis was determined using the method adapted from commercial kit (CS0260, Sigma, St. Louis, MO, USA). The method is based on the reduction of 5.5′-dithio acid-bis-(2-nitrobenzoic acid) to thio-2-nitrobenzoic acid according to Griffith assay. 31 In order to calculate the concentration of total glutathione (GSHt) and oxidized glutathione (GSSG), a standard serial dilution curve is prepared, and the concentration of reduced form (GSH) is calculated from subtracting the total value of total glutathione by the value of oxidized glutathione. 32 Myeloperoxidase (MPO) enzyme activity was determined as described by Xia et al., 33 using samples of BALF, pipetted in duplicate into 96-well plates. Samples were incubated at 37°C for 5 min with 3,3′,5,5′-tetramethylbenzidine, then the samples were incubated with hydrogen peroxide and read afterward in a spectrophotometer at 630 nm.
In order to measure lipid peroxidation, the Buege and Aust method was used, in which thiobarbituric acid reacts with oxidized lipids (TBARS), evaluated in a spectrophotometer at 535 nm. 34 The quantification of oxidized proteins was determined according to the protocol adapted from the methodology described by Reznick and Packer. 35 The activity of the enzymes, as well as the markers of oxidative damage, was determined in relation to the total concentration of proteins, which were determined according to the protocol described by Bradford. 36
mRNA expression analysis of inflammatory markers in pulmonary tissue
mRNA expression analysis of IL-6, IL-8, NF-κB, and TNF-α was performed to determine inflammatory marker levels in the lungs. RNA extraction was performed using the Trizol method as described by Chomczynski. 37 Twenty milligrams of pulmonary tissue was used for RNA extraction. Strand cDNAs were synthesized from 1.0 µg of total RNA using the ThermoScript RT-PCR System (Invitrogen Brasil) with oligo-dT primers according to the instructions by the manufacturers.
qRT-PCR was performed on an ABI Prism 7000 DNA Sequence Detection System using 5 µL Go-Taq BRYT Green PCR Master Mix (Promega, Sao Paulo, SP, Brazil) with 3 µL of primer solution (forward + reverse, 2.5µmol/µL) (Table 1) and 2 µL of cDNA. The samples were incubated at 95°C for 2 min and then subjected to 40 cycles of 95°C for 15 s and 60°C for 1 min, during which time fluorescence data were collected. The efficiency of each primer pair was evaluated by serial dilutions of cDNA according to the protocol developed by PE Applied Biosystems. In order to evaluate expression of the inflammatory markers IL-6, IL-8, NF-κB, and TNF-α, qRT-PCR was utilized using the same specific primers used by Attafi et al. 38 (Table 1). For the analysis, the same strategy was applied as used by Attafi et al. 38 Triplicate analyses on the mRNA expression (fold change) were performed normalizing the results with the constitutive gene β-actin (ΔCt).
Primer sequences used for RT-PCR reactions.
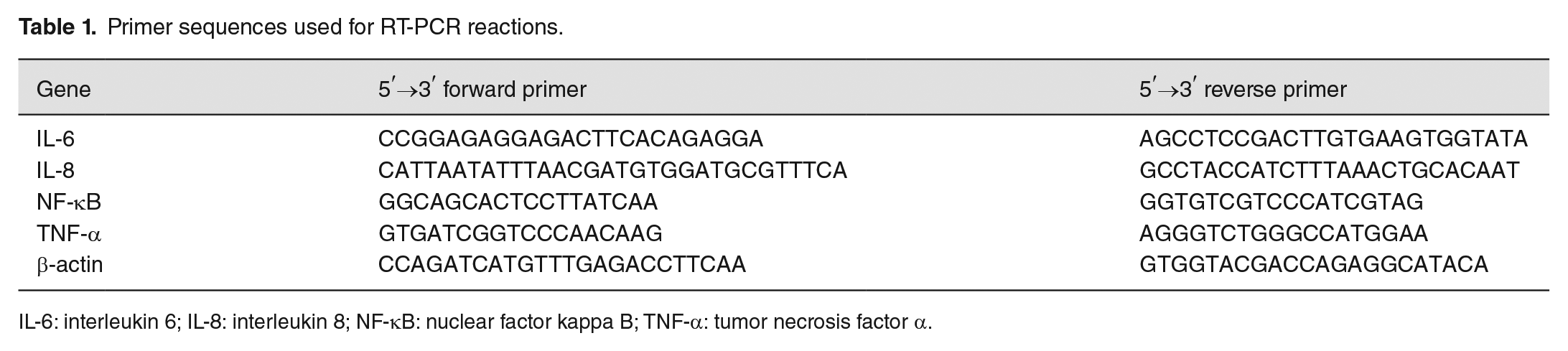
IL-6: interleukin 6; IL-8: interleukin 8; NF-κB: nuclear factor kappa B; TNF-α: tumor necrosis factor α.
Morphometric analysis of the pulmonary parenchyma
The effects of surfactant and mechanical ventilation in the prone position on the alveoli was determined stereologically using a microscope. Subsequently to the staining of the tissue, as described in 3.9, the differences in Alveolar volume density as well as septum density are noted and analyzed. The determination of alveolar volume density and septum density is done in a 16-point test system and a known test area, as described by Mandarim-de-Lacerda. 39 For this analysis, a light microscope is used with a 400× magnification.25,27,28
Statistical analysis
All statistical analyses were performed using GraphPad Prism 8.4.2 software. The parametric distribution of the data was evaluated using the Shapiro–Wilk normality test, the parametric data are expressed as mean and standard deviation, and nonparametric data are expressed as median and interquartile interval (percentile 25 and 75). The data were analyzed using two-way analysis of variance (ANOVA) to determine the effects of position during MV and pre-treatment with surfactant, and if there was an interaction between the factors. In order to evaluate the difference between the experimental groups, Tukey’s post-test was performed. The statistical significance was set at the level of 5%.
Results
Hemodynamic and ventilatory parameters
We measured the hemodynamic and ventilatory parameters throughout the experimental procedure. The repeated measures two-way ANOVA analysis showed no effect or interaction between pre-treatment and position for the analyzed parameters. In addition, there was no difference between the experimental groups (P > 0.05) (Table 2).
Hemodynamic and ventilator parameters of male Wistar rats subjected to mechanical ventilation with and without pre-treatment with exogenous surfactant.
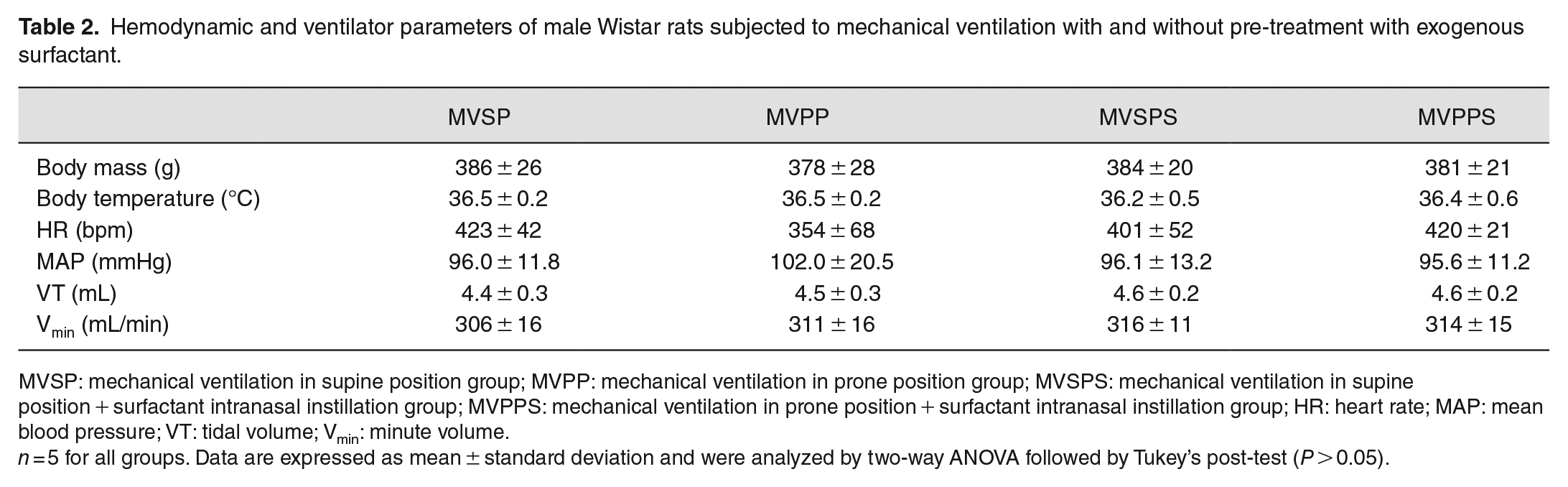
MVSP: mechanical ventilation in supine position group; MVPP: mechanical ventilation in prone position group; MVSPS: mechanical ventilation in supine position + surfactant intranasal instillation group; MVPPS: mechanical ventilation in prone position + surfactant intranasal instillation group; HR: heart rate; MAP: mean blood pressure; VT: tidal volume; Vmin: minute volume.
n = 5 for all groups. Data are expressed as mean ± standard deviation and were analyzed by two-way ANOVA followed by Tukey’s post-test (P > 0.05).
Respiratory mechanics
At the end of the experimental protocol, the lung function parameters were calculated. In peak pressure and airway resistance there were no effects or interactions between the factors, and no differences between the experimental groups. However, the repeated measures two-way ANOVA analysis of the static lung compliance parameter showed an effect of pre-treatment with surfactant, F(1.16) = 5.52, P = 0.03. The post-test revealed an increase in lung compliance in animals that received surfactant and were ventilated in the prone position (MSPPS) compared with ventilation in the supine position (MVSP) (P = 0.03) (Table 3).
Respiratory mechanics of male Wistar rats subjected to mechanical ventilation with and without pre-treatment with exogenous surfactant.
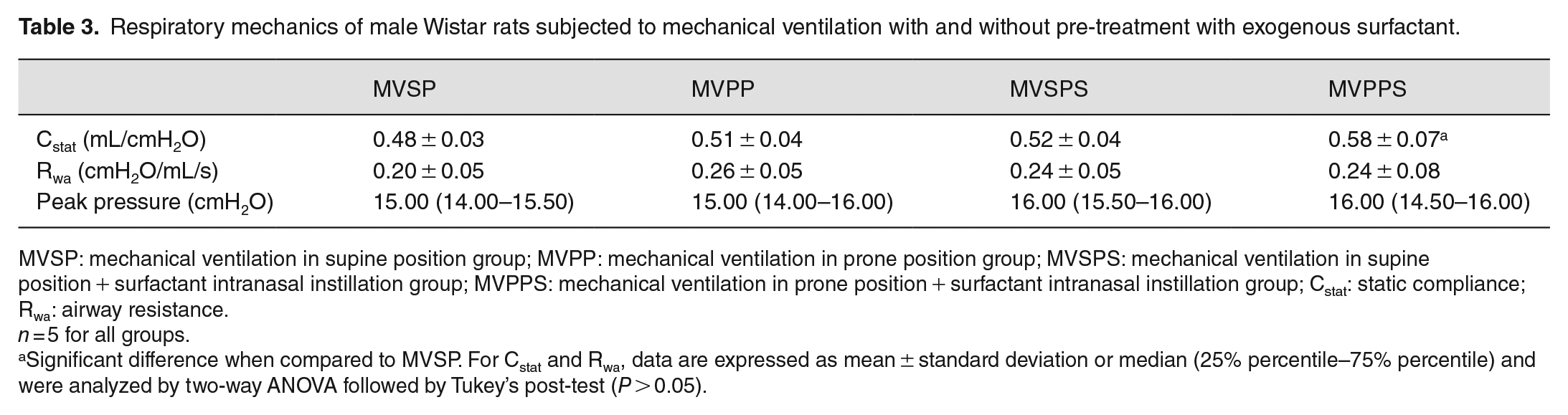
MVSP: mechanical ventilation in supine position group; MVPP: mechanical ventilation in prone position group; MVSPS: mechanical ventilation in supine position + surfactant intranasal instillation group; MVPPS: mechanical ventilation in prone position + surfactant intranasal instillation group; Cstat: static compliance; Rwa: airway resistance.
n = 5 for all groups.
Significant difference when compared to MVSP. For Cstat and Rwa, data are expressed as mean ± standard deviation or median (25% percentile–75% percentile) and were analyzed by two-way ANOVA followed by Tukey’s post-test (P > 0.05).
Antioxidant defense biomarkers and oxidative damage
The exogenous surfactant administration promoted protective effects in ventilated animals in both supine and prone position. The two-way ANOVA analysis of total protein concentration revealed an effect of surfactant pre-treatment, F(1.16) = 13.29, P = 0.002, and an interaction between position versus surfactant, F(1.16) = 5.44, P = 0.03. The total protein concentration was lower in MVSPS when compared to MVSP (P = 0.003) and MVPP (P = 0.024). The analysis activity of antioxidant enzyme SOD showed an effect of pre-treatment with surfactant, F(1.16) = 61.97, P < 0.0001, and position during the MV, F(1.16) = 7.24, P = 0.016. The SOD activity was lower in MVSPS when compared to MVSP (P = 0.002) and MVPP (P = 0.01), and significantly lower in MVPPS compared to MVSP (P < 0.0001), MVPP (P < 0.0001), and MVSPS (P = 0.033). The analysis of catalase activity revealed an effect of surfactant pre-treatment, F(1.16) = 14.66, P = 0.0015. The enzyme activity was lower in MVSPS and MVPPS when compared to MVSP (P = 0.02). The repeated measures two-way ANOVA analysis of GSH/GSSG ratio showed an effect of surfactant, F(1.16) = 10.97, P = 0.004, and position during mechanical ventilation, F(1.16) = 5.43, P = 0.033. The GSH/GSSG ratio was higher in MVSPS (P = 0.03) and MVPPS (P = 0.005) when compared to MVSP.
Lipid peroxidation was measured by the TBARS method. The two-way ANOVA analysis of thiobarbituric acid reactive substance showed an effect of pre-treatment with surfactant, F(1.16) = 16.49, P = 0.0009. A decrease in lipid peroxidation was observed in MVSPS and MVPPS compared to MVSP (P = 0.02). The repeated measures two-way ANOVA analysis of carbonylated protein levels showed an effect of pre-treatment with surfactant, F(1.16) = 30.96, P < 0.0001. The post-test revealed a difference between MVSPS and MVPPS compared to MVSP (P = 0.01) and MVPP (P = 0.001). In addition, MPO activity in the BALF was determined. The analysis of MPO activity showed an effect of pre-treatment with surfactant, F(1.16) = 31.41, P < 0.0001. The oxidant enzyme activity was lower in MVSPS and MVPPS when compared to MVSP (P = 0.004) and MVPP (P = 0.01) (Table 4).
Biomarkers of oxidative stress in lung parenchyma and BALF of male Wistar rats subjected to mechanical ventilation with and without pre-treatment with exogenous surfactant.
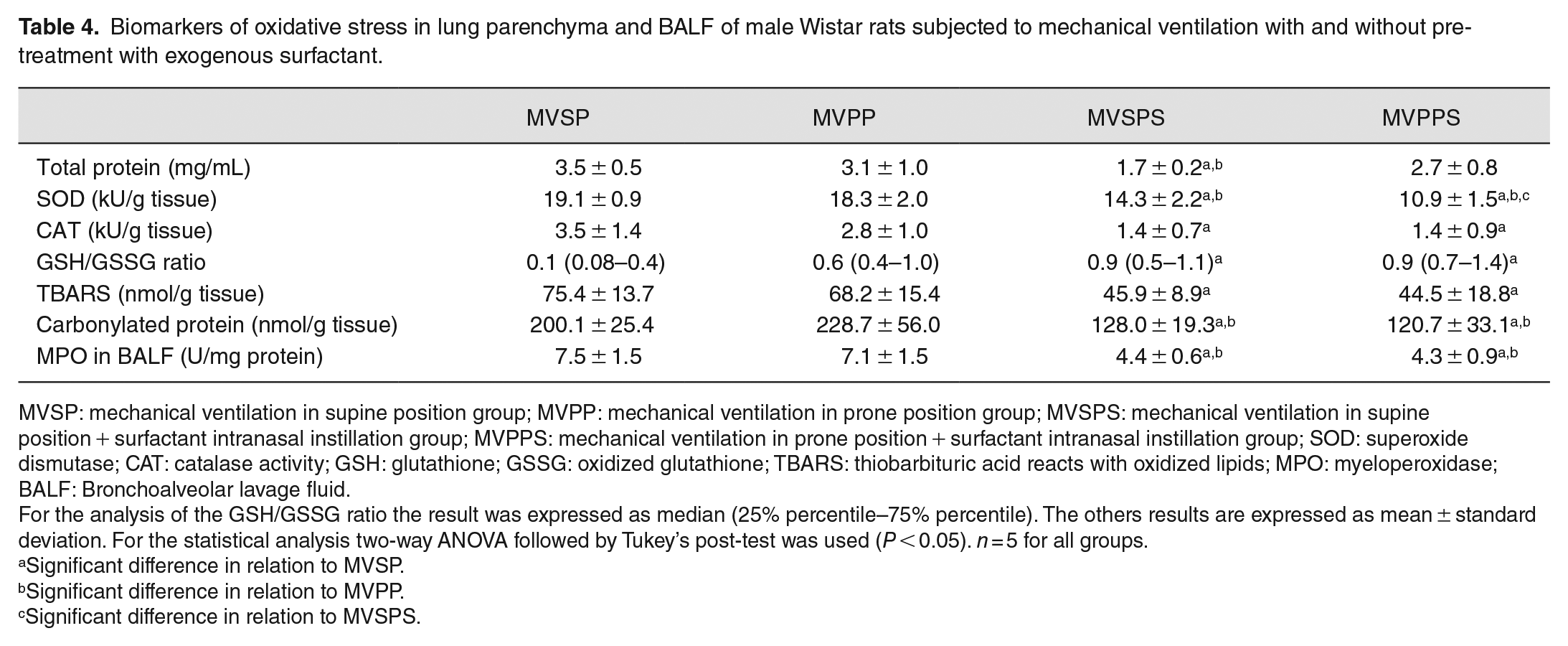
MVSP: mechanical ventilation in supine position group; MVPP: mechanical ventilation in prone position group; MVSPS: mechanical ventilation in supine position + surfactant intranasal instillation group; MVPPS: mechanical ventilation in prone position + surfactant intranasal instillation group; SOD: superoxide dismutase; CAT: catalase activity; GSH: glutathione; GSSG: oxidized glutathione; TBARS: thiobarbituric acid reacts with oxidized lipids; MPO: myeloperoxidase; BALF: Bronchoalveolar lavage fluid.
For the analysis of the GSH/GSSG ratio the result was expressed as median (25% percentile–75% percentile). The others results are expressed as mean ± standard deviation. For the statistical analysis two-way ANOVA followed by Tukey’s post-test was used (P < 0.05). n = 5 for all groups.
Significant difference in relation to MVSP.
Significant difference in relation to MVPP.
Significant difference in relation to MVSPS.
mRNA expression analysis of inflammatory markers in pulmonary parenchyma
In order to evaluate the inflammatory response caused by mechanical ventilation, we performed mRNA expression analysis of NF-κB, TNF-α, IL-6, and IL-8. Results of the mRNA levels of NF-κB showed an effect of surfactant pre-treatment, F(1.16) = 8.55, P = 0.009, and position during MV, F(1.16) = 7.47, P = 0.01, as well as a surfactant vs position interaction, F(1.16) = 4.67, P = 0.04. The post-test revealed a decrease in mRNA levels of NF-κB in MVPP (4.89 ± 0.36), MVSPS (4.86 ± 0.17), and MVPPS (4.79 ± 0.17) when compared to MVSP (5.52 ± 0.38) (P = 0.01) (Figure 1(A)). For the mRNA levels of TNF-α, an effect of surfactant, F(1.16) = 6.22, P = 0.02, and position, F(1.16) = 5.10, P = 0.03, was observed. The post-test revealed a decrease in MVPPS (6.76 ± 0.89) when compared to MVSP (8.41 ± 0.46) (P = 0.01) (Figure 1(B)). Regarding the analysis of IL-6 mRNA levels, an effect of position during mechanical ventilation, F(1.16) = 13.12, P = 0.002, was observed. A decrease in IL-6 mRNA levels was seen in MVPPS (7.61 ± 1.85) compared to MVSP (11.27 ± 0.80) and MVSPS (11.24 ± 1.00) (P = 0.005) (Figure 1(C)). For the IL-8 mRNA levels, an effect of surfactant, F(1.16) = 12.18, P = 0.003, and position, F(1.16) = 5.48, P = 0.03, was observed. There was a decrease in MVPPS (3.42 ± 1.14) when compared to MVSP (6.38 ± 0.67) (P = 0.004) (Figure 1(D)).
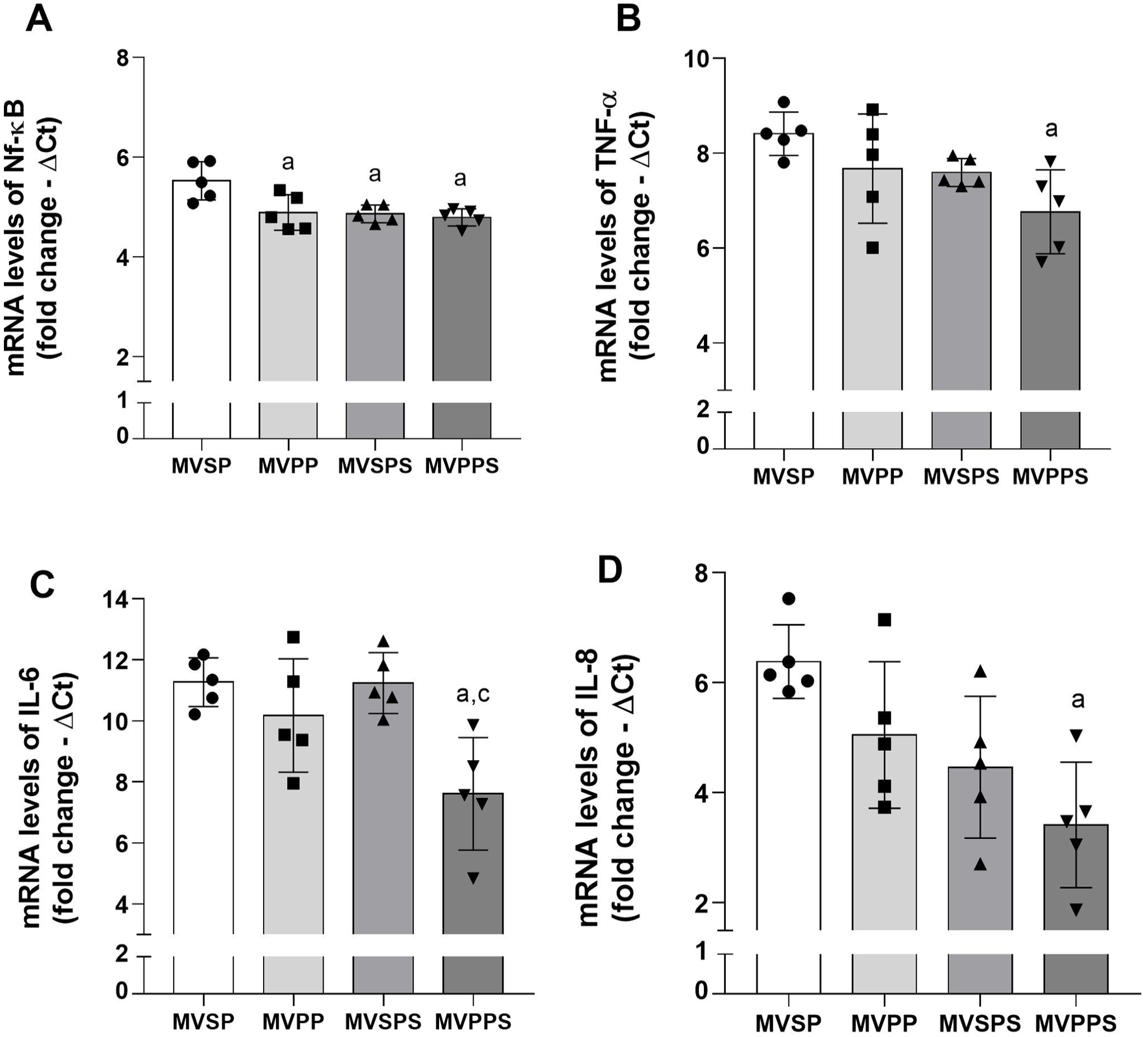
mRNA expression levels of inflammatory markers in the lung parenchyma. (A) mRNA levels of Nf-κB. (B) mRNA levels of TNF-α. (C) mRNA levels of IL-6. (D) mRNA levels of IL-8.
Morphometric evaluation of the pulmonary parenchyma
The two-way ANOVA analysis of volume density of alveolar airspace (Vv[a]) showed an effect of surfactant pre-treatment, F(1.16) = 8.26, P = 0.01, and position during MV, F(1.16) = 17.81, P = 0.0007, as well as a surfactant versus position interaction, F(1.16) = 8.05, P = 0.01. Animals in MVSP (71.19 ± 4.21) presented higher volume density of alveolar air spaces when compared to MVPP (59.06 ± 5.15), MVSPS (61.38 ± 3.66), and MVPPS (59.00 ± 1.13) (Figure 2(E)). Regarding the analysis of alveolar septa volume density (Vv[as]) two-way ANOVA revealed an effect of surfactant, F(1.16) = 26.8, P < 0.0001, and position during MV, F(1.16) = 19.47, P = 0.0004. These effects were observed by an increase in MVPP (27.00 ± 1.54), MVSPS (32.25 ± 2.24), and MVPPS (36.00 ± 3.05) compared to MVSP (23.94 ± 2.76) (P = 0.002) (Figure 2(F)).
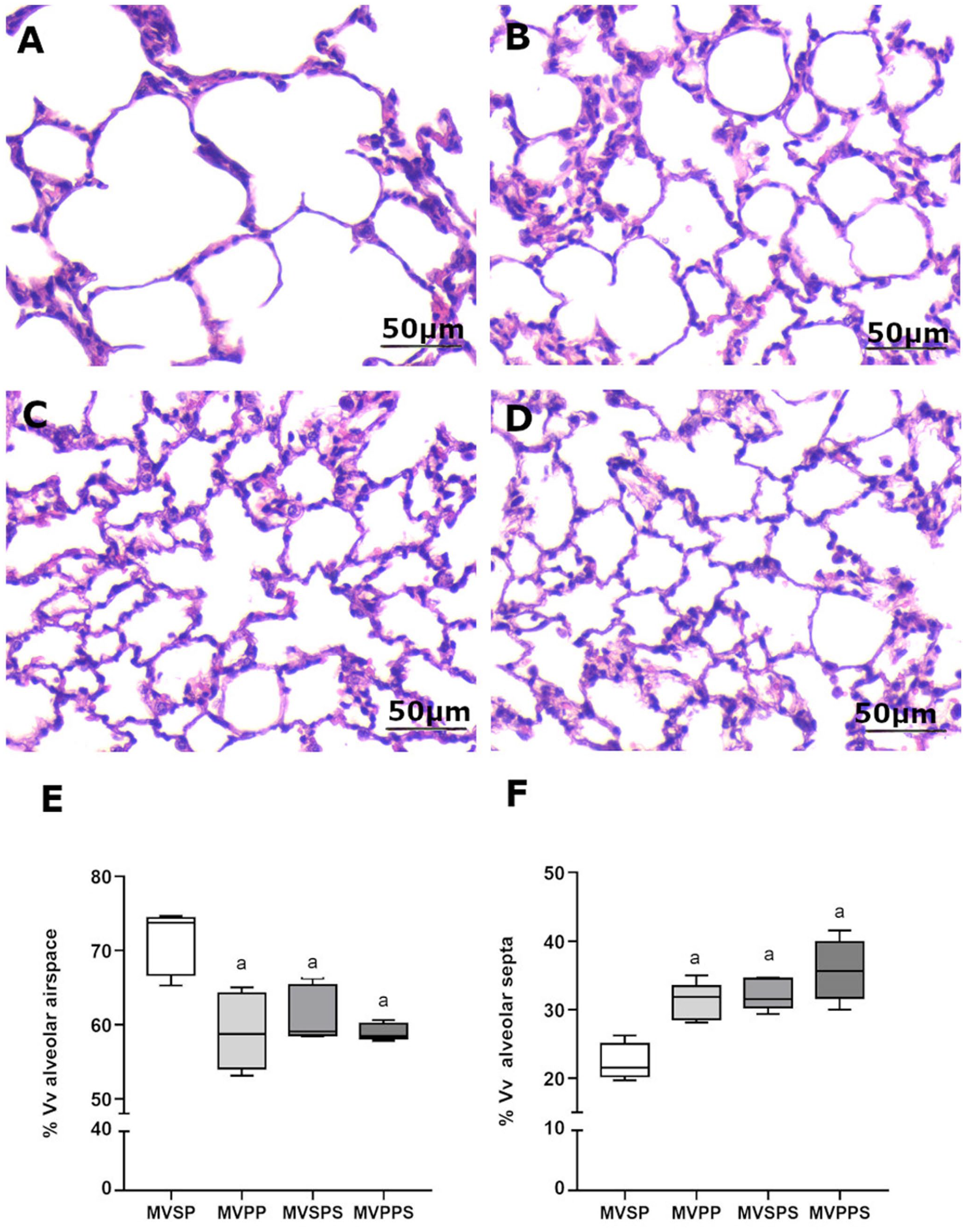
Representative photomicrograph of lung parenchyma stained with Hematoxylin and Eosin (HE). Bar = 50 μm, 400× magnification. (A) MVSP: Mechanical Ventilation in Supine Position group; (B) MVPP: Mechanical Ventilation in Prone Position group; (C) MVSPS: Mechanical Ventilation in Supine Position + Surfactant intranasal instillation group; (D) MVPPS: Mechanical Ventilation in Prone Position + Surfactant intranasal instillation group; Stereological analyses of lung sections. (E) Volume density of alveolar airspace. (F) Volume density of alveolar septa. For E and F, the data are expressed in median, minimum and maximum values.
Discussion
In this study, we observed that in healthy animals submitted to mechanical ventilation with high tidal volume, pre-treatment with surfactant, regardless of the position used to ventilate the animals, promoted a protective effect on the lungs, reducing the redox imbalance and the inflammatory response, and preserving the pulmonary histoarchitecture. The prone position had a protective effect on pulmonary histoarchitecture and reduced the inflammatory markers in ventilated animals, but had no effects on oxidative stress caused by MV. Prone position increases oxygenation and improves the outcomes in patients diagnosed with acute respiratory distress syndrome (ARDS). 40 This enhanced oxygenation is due to the combinational effects of the prone position causing a better homogenized aeration of the lungs by recruiting more vertebral parts, which receive most of the pulmonary blood flow, and the decrease in alveolar overstretching. 15 Pre-treatment with exogenous surfactant was efficient in minimizing the oxidative damage caused by mechanical ventilation; however, it was not efficient in improving ventilatory parameters, which was observed only when surfactant was associated with the prone position. Thus, our results suggest that exogenous surfactant could be an alternative therapy to enhance survival during MV in severe cases, particularly when the use of the prone position is contraindicated.
Lung compliance is determined by the number of alveoli open during ventilation. 41 In patients with ARDS, lung compliance decreases because of alveolar collapse caused by inflammatory cells. 42 Although, Chírico et al. 25 did not observe changes in lung compliance during MV, Gommers et al. 43 showed that static compliance improved in rabbits subjected to MV when applying exogenous surfactant therapy, but not dynamic compliance. Therefore, dynamic compliance alone does not assess the effects of exogenous surfactant. In this sense, exogenous surfactant therapy boosts gas exchange in a murine model of a two-hit lung injury. 44 Also, exogenous surfactant halts the hyperoxia-induced lung injury in mice. 24 The effect of the prone position on lung compliance remains disputed in the literature. A previous study showed that static lung compliance in patients with acute lung injury (ALI) increased only when patients were repositioned back into the supine position after being subjected to the prone positioning. 45 However, a recent study on the recruitment of new alveoli during prone positioning raises static compliance in patients with ARDS. 46 Previous findings have shown divergent effects from both prone position and exogenous surfactant treatment on the lungs. Our findings suggest that the association of these two strategies promotes an increase of static compliance in animals submitted to mechanical ventilation with high tidal volumes. Likely, the association of the two factors promoted an increase in lung distention capacity, thus improving pulmonary oxygenation.
Cytokines control and influence leukocyte recruitment, inflammation, and tissue injury. NF-κB is a transcription factor and a central mediator for pro-inflammatory gene expression. 47 Mechanical forces applied to the lung during mechanical ventilation stimulate alveolar macrophages, epithelial and endothelial cells, and allow the influx of inflammatory cells, related to the activation of the NF-κB pathway, increasing the production of cytokines.8,48 Our results corroborate previous findings demonstrating the use of high tidal volumes during MV increase the expression of Nf-κB and activates its signaling pathway.48,49 Notably, both the prone position and the administration of exogenous surfactant lowered the expression of Nf-κB induced by MV. In this sense, a previous study suggested that the prone position delays the progression of VILI because the stretch caused by mechanical ventilation is more evenly distributed, possibly due to a reduced activation of pro-inflammatory signaling pathways. 50 In addition, Lan et al. 51 observed that surfactant administration lowered the NF-κB expression, therefore attenuating the acute lung injury. Our results corroborate with the previous literature, suggesting the prone position and the pre-treatment with exogenous surfactant reduces the activation of the NF-κB pathway.
Recently, our research group showed that the pre-treatment of exogenous surfactant reduced lung inflammation by decreasing pro-inflammatory cytokines, such as IL-1, IL-6, IL-17, and TNF-α. 24 In contrast, mouse models of ventilator-induced inflammation, pre-treatment with surfactant did not affect TNF-α and IL-6 levels. 52 Moreover, animal studies and limited human trials have shown that the prone position is associated with decreased levels of IL-6, IL-8, and TNF-α levels.53,54 Although in this study we evaluated the expression of mRNA for inflammatory markers, the association between pre-treatment with exogenous surfactant and prone position appears to modulate the expression of inflammatory markers during mechanical ventilation with high tidal volumes. The previous findings regarding the antioxidant capacity of both factors are conflicting; however, their association proved to be beneficial in minimizing the expression of inflammatory markers.
The influx of leukocytes prompted by mechanical ventilation induces ROS production, leading to the activation of the antioxidant defense system. 55 ROS production and the subsequent oxidative damage to the lung parenchyma are a common complication in VILI and are associated with the hyperinflation in the alveoli.11,12 Oxidative damage to the lungs reduces the surfactant production, therefore, impairing lung function. 56 Previous studies from our laboratory have indicated exogenous surfactant decreases the unwanted effects of MV, by decreasing oxidative damage to lipids and proteins in the lung parenchyma. 24 Also, prone positioning attenuated lung injury in an experimental model of acute lung injury in rabbits. 54 However, in this study, the prone position alone did not exert an effect on the activity of antioxidant enzymes and nor did it reduce oxidative damage in the lungs. Previous studies have shown that MV in a prone position decreased mortality rate in ARDS patients.16,57 This ventilation strategy appears to delay VILI’s development. 50 Our findings may differ from the previous studies indicating a protective effect of the prone position on oxidative damage, because we used animals without prior lung injury. The mechanism of VILI in a healthy model differs from the response to MV when lung injury is present. 6 We observed that exogenous surfactant administration reduced the oxidative damage in the lung parenchyma in animals submitted to MV in both supine and prone position. Our results corroborate previous findings demonstrating an antioxidant action of exogenous surfactant in different experimental models,24,58 thus reinforcing the effectiveness of exogenous surfactant pre-treatment.
MV causes cyclic stretching of the alveoli, which may cause cellular adjustments by changing actin filaments, microtubules, and other intermediate filaments. These cellular changes result in endothelial and epithelial dysfunction. 6 High tidal volumes causing the overstretching of the alveoli are associated with VILI by inducing permanent structural changes in the lung parenchyma. 4 The prone position homogenizes the mechanical forces and the aeration of the lungs, reducing alveolar overstretching in patients with ARDS, allowing the use of lower tidal volumes, 15 and thus preserving the histoarchitecture of the lung parenchyma. Previous studies have shown that the use of the prone positioning in experimental models prevents lung injury.54,59 The results of this study are in line with previous literature indicating both the prone positioning and exogenous surfactant pre-treatment during mechanical ventilation preserves the original lung histoarchitecture.
The pandemic caused by the coronavirus promoted the increase in the clinical use of the prone position in patients with moderate-to-severe respiratory distress syndrome undergoing invasive mechanical ventilation.18,41 The prone position favors the re-expansion of collapsed lung parenchyma in the dorsal lung regions and the reduction of aeration in the ventral regions, leading to more homogeneous lung aeration. 18 Despite these benefits, its use has some disadvantages. Positioning a patient in a prone position requires a dedicated and experienced team, but to perform this maneuver, it is often necessary to increase the dose of sedatives and muscle relaxants, which can lead to hemodynamic instability. In addition, the prone position is associated with increased risk of accidental extubation, displacement and obstruction of the endotracheal tube, loss of venous access, brachial plexus injury, and pressure ulcers. 41
Considering the risks of performing mechanical ventilation in a prone position, our results suggest the use of exogenous surfactant may represent an effective clinical strategy to replace the use of the prone position during MV to improve survival. First, surfactant is simple to execute and requires less expertise from the care team. Second, this therapy is already widely used in neonatology and represents a milestone in the treatment of neonatal respiratory distress syndrome. 60 In invasive mechanical ventilation, the cyclic stretch caused by mechanical ventilation may promote endothelial injury and consequent increase in vascular permeability, which may promote an inactivation of endogenous surfactant. 61 Thus, the lungs may respond to treatment with exogenous surfactant in patients undergoing mechanical ventilation by improving lung compliance, reducing plateau pressure, and improving gas exchange. 61
The prone position effectiveness is also due to its ability to preserve the lung parenchyma by reducing the tissue damage and the inflammatory response. Exogenous surfactant also had a protective effect on the lungs, minimizing tissue damage, redox imbalance, and inflammatory response. These results suggest that the administration of exogenous surfactant may represent a safe alternative to reduce the deleterious effects of mechanical ventilation, especially when positioning a patient in a prone position is contraindicated or difficult to perform.
Although the results found here suggest that the pre-treatment with surfactant has important protective effects during mechanical ventilation, the findings of this study have some limitations. Extrapolating our data for human use would be challenging, as the duration of mechanical ventilation in our study was very short when compared to the average duration of mechanical ventilation in humans. In addition, the use of exogenous surfactant in the treatment of respiratory distress syndrome in neonates is already well established; however, its viability in treating respiratory diseases in adults is poorly understood. Further studies are needed to determine the surfactant half-life and the number of doses necessary to cause an antioxidant and anti-inflammatory effects when mechanical ventilation lasts for a long period.
In conclusion, the results show that the pre-treatment with exogenous surfactant, regardless of the position adopted in mechanical ventilation, preserves the original lung histoarchitecture, reduces redox imbalance, and reduces acute inflammatory responses caused by mechanical ventilation in healthy adult Wistar rats.
Footnotes
Acknowledgements
The authors are thankful to Ana Luiza Copello and Michel Oliveira for their technical assistance during this study.
Authors’ Contributions
ABFS and FBS contributed to conceptualization and methodology. ABSF, YD, PAMJ, and TFC performed the investigation and formal analysis. JMOC performed formal analysis. ABFS and YD drafted manuscript. BMR contributed with equipment and laboratory. ABFS, SDC, RCAM, and FSB edited and revised manuscript. FSB contributed to supervision; project administration; and funding acquisition. All authors approved the last version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Federal University of Ouro Preto (UFOP). FSB, RCM, and BMR are in credit for the fellowship of research productivity the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq).