
Abstract
Introduction:
Sharps safety is critical in preventing injuries such as cuts, lacerations, and needlestick wounds, particularly in research environments where sharp instruments are frequently used and there is a risk of exposure to biological hazards. The aim of this study was to assess how effectively implemented control measures reduce sharp-related injuries in research environments. This study examines the implementation of best practices aimed at preventing sharp-related injuries in research settings through a combination of substitution, engineering controls, administrative controls, and employee education via workshops and training.
Methods:
The Abigail Wexner Research Institute (AWRI) adopted a multi-faceted safety program focused on equipment redesign, engineering controls, staff education, and engagement. Injury data from 2019 through 2025 were analyzed to evaluate the development and impact of targeted initiatives. Initiatives included implementation of a revised cryostat/microtome policy, hands-on workshops, and provision of safer engineering controls or alternatives.
Results:
A 35% reduction in overall sharps injuries was observed from 2022 to 2023 (from 20 to 13 incidents), alongside a 70% drop in Occupational Safety and Health Administration (OSHA)-recordable injuries (from 10 to 3 incidents). From 2024 to 2025, a 28% reduction in overall sharps injuries was observed (from 21 to 15 incidents), alongside a 67% reduction in OSHA-recordable injuries (from 3 to 1 incidents). Notably, injuries related to cryostats and microtomes dropped to zero in 2023.
Conclusion:
Implementation of targeted, comprehensive sharps safety initiatives led to significant injury reduction at AWRI. This demonstrates the effectiveness of combining administrative policy, training, and equipment improvements in fostering a culture of safety.
Keywords
Introduction
Percutaneous injuries involving sharps (needles, scalpels, blades, and broken glass) pose significant risks to research personnel, particularly in settings involving bloodborne pathogens like Hepatitis B, Hepatitis C, Human immunodeficiency virus (HIV), and other biological pathogens.1–3 These incidents can pose a risk of developing severe, and in some cases, life-threatening infections. Both in vitro procedures (e.g., blood processing, tissue sectioning, cell culture) and in vivo activities (e.g., animal or clinical studies) present substantial risks, particularly when appropriate precautions and safety devices are not employed.4–8 Administration of viral vector-based gene therapies to human participants also presents a significant safety risk, making institutional mitigation planning essential for protecting personnel. 5 In research organizations, conducting clinical trials involving these modalities further elevates the overall risk profile, underscoring the need for comprehensive oversight and robust risk-management practices.5–10
Sharp-related incidents are recognized internationally as a major contributor to laboratory exposures and laboratory-acquired infections. 11 In addition to the immediate risk of percutaneous inoculation, improper handling or disposal of sharps can also lead to secondary exposures among support staff, waste handlers, and environmental services personnel, extending the impact beyond the primary laboratory setting. Surveillance data from Laboratory Incident Notification Canada (LINC) program show that sharps are among the most frequently reported exposure types in licensed laboratories, underscoring their persistent risk across research and diagnostic settings. 11 These findings underscore the critical need for robust institutional programs and proactive prevention strategies aimed at reducing sharps-related injuries within organizations.
Beyond the inherent biological and occupational risks, sharps injuries impose a considerable financial burden on research institutions. 12 Studies have shown that the average cost of a single needlestick injury including diagnostic testing, treatment, and lost productivity ranges from $3,000 to $5,000 in the United States. 2 These figures do not account for long-term health care costs or the psychological impact on affected personnel, which can further compound institutional expenses. A systematic review of economic evaluations found that the median aggregate cost (direct and indirect) of sharps injuries was approximately $747, with some cases reaching up to $1,691, depending on the severity and postexposure protocols required. 3 These costs demonstrate the importance of proactive safety measures and justify investments in safety-engineered devices and training programs.10–16
The financial implications also extend to regulatory compliance and institutional liability. The Occupational Safety and Health Administration (OSHA) recordable injuries, which include sharps incidents resulting in medical treatment beyond first aid or work restrictions, can trigger audits, fines, and reputational damage. 4 By implementing targeted interventions such as establishing an injury tracking system and categorizing incidents by cause and severity, research institutions can not only reduce injury occurrence but also mitigate the associated economic impacts. The integration of cost-awareness into safety planning reinforces the dual imperative of protecting both human health and institutional resources.
Organizations such as the Centers for Disease Control and Prevention (CDC), 6 the OSHA, 7 and the National Institutes of Health (NIH), 8 all agencies within the United States of America, have outlined safety standards and best practices; however, many institutions still face challenges in preventing these injuries. OSHA mandates that all work-related needlestick and sharps injuries involving contaminated materials be recorded and addressed under its Bloodborne Pathogens Standard, emphasizing the importance of exposure control plans and postexposure protocols.1,4 The CDC and NIH reinforce these standards by promoting engineering controls, safe needle devices, and rigorous training programs.6–8 The European Union (EU) Directive 2010/32/EU, adopted on 10 May 2010, establishes legally binding requirements for the prevention of sharps injuries within hospital and healthcare settings across EU member states. This directive implements the Framework Agreement on the Prevention of Sharps Injuries developed by the European social partners in the health care sector, thereby providing a standardized regulatory structure aimed at reducing percutaneous exposures and enhancing worker safety. The directive mandates a comprehensive, multilayered approach to worker protection, including systematic risk assessment of sharps hazards; elimination or minimization of risks through substitution and engineering controls; the mandatory use of safety-engineered sharp devices where exposure cannot otherwise be prevented; implementation of safe work practices; restrictions on unsafe procedures such as recapping; establishment of robust reporting, follow-up, and investigation systems; and provision of training, information, and worker involvement regarding both risks and preventive technologies. By integrating engineering controls, organizational policies, and worker education, Directive 2010/32/EU creates a unified, enforceable standard intended to significantly reduce needlestick and sharp-related injuries within the European health care workforce. 12 Even with regulatory guidance, many institutions continue to struggle with implementation due to factors like inconsistent reporting, limited resources, and gaps in staff compliance. These challenges underscore the need for strengthened institutional commitment, sustained education and training efforts, and the cultivation of a safety culture that emphasizes proactive prevention rather than reactive response.
To contextualize the multilayered approach used in this study, the CDC National Institute for Occupational Safety and Health (NIOSH) Hierarchy of Controls provides a widely accepted framework for evaluating and implementing safety interventions. The Hierarchy of Controls is commonly depicted as an inverted pyramid illustrating five levels of hazard mitigation, listed from most to least effective: Elimination, Substitution, Engineering Controls, Administrative Controls, and Personal Protective Equipment (PPE). 13
In this study, Abigail Wexner Research Institute (AWRI) utilized multiple tiers of this hierarchy simultaneously to reduce sharp-related injuries. Although the complete elimination of sharps was not feasible due to research needs, several substitution strategies were implemented. These included replacing metal razor blades with polycarbonate alternatives and adopting safer sharp devices such as retractable syringes and guarded box openers. Engineering controls played a substantial role through redesigned equipment (e.g., needle recappers, magnetic-tip brushes, cryostat/microtome safety features). These controls were complemented by administrative controls, including updated policies, hands-on workshops, targeted training, and the institution-wide implementation of Zero Hero™ behavioral safety program. The Zero Hero™ program is Nationwide Children’s Hospital (NCH) comprehensive patient and staff safety initiative. Launched in 2009, it marked the institution as the first pediatric hospital to publicly commit to eliminating preventable harm. The hospital identifies Zero HeroTM as the foundational framework for its patient-safety culture, integrating quality-improvement practices and reinforcing a unified “One Team” approach. Although PPE represents the least effective tier under the hierarchy of controls, it remained an essential component of risk-mitigation efforts. In particular, cut-resistant gloves were routinely used during cryostat and microtome tissue sectioning to reduce the risk of laceration injuries. Incorporating the NIOSH hierarchy helps highlight that the reductions in sharps injuries were achieved not by relying on a single intervention, but through a strategic layering of controls across multiple tiers of the pyramid. Implementation of controls within this established mitigation framework led to improved sharps-handling practices and a reduction in overall injury occurrence.
The institution conducted a risk assessment informed by the distribution and severity of documented injuries. Although animal bites and needlestick injuries occurred more frequently, cryostat and microtome-related injuries were prioritized because they demonstrated a disproportionately higher severity regarding the consequences of these types of injuries. These injuries often required sutures and medical treatment beyond first aid, making them OSHA recordable events, whereas often animal bites and minor needlestick injuries did not meet this threshold. By evaluating both likelihood and consequence, the assessment identified microtome and cryostat use as high-impact hazards despite their lower frequency. This severity-based risk assessment informed the decision to focus early interventions on tissue-sectioning practices, resulting in revised policies, enhanced training requirements, implementation of safer tools and PPE specific to tissue sectioning.
Based on the categorized patterns of sharp injuries, the institution introduced safer sharp substitutions. Implementing these enhanced devices represents a critical advancement in laboratory and clinical safety, directly targeting the persistent risk associated with sharp-related injuries.14–23 These injuries ranging from needlesticks and scalpel cuts to animal bites and microtome blade contact, pose significant threats to health care and research personnel, including exposure to bloodborne pathogens and biological agents. By integrating devices such as retractable syringes, needle recappers, and scruff guards, institutions can dramatically reduce the likelihood of accidental harm.14–23 Moreover, innovations like cut-resistant gloves and guarded box openers extend protection beyond procedural settings to routine tasks, reinforcing a culture of safety. These tools, while modest in cost, offer substantial returns in injury prevention, reduced liability, and improved staff well-being. Their adoption reflects a proactive commitment to occupational health and underscores the importance of engineering controls in mitigating sharps hazards.17–23
Zero Hero™ tools function as institutional safety resources that reinforce Nationwide Children’s Hospital’s broader culture of safety. In this context, they were applied with specific emphasis on enhancing sharps-handling practices and reducing the incidence of sharps-related injuries. Sharps safety depends not only on the use of appropriate equipment but also on fostering a culture of personal accountability, proactive hazard recognition, and effective communication. Zero Hero™ tools like Pause to Predict, Stop–Think–Act–Review (STAR), and Stop and Resolve empower individuals to slow down, assess risks, and make informed decisions before engaging with potentially hazardous sharps. These techniques foster situational awareness and reduce the likelihood of injury during routine tasks. Teaching users to be accountable and act appropriately is a major factor in reducing preventable sharps injuries.9,10 Equally vital are communication strategies such as Situation–Background–Assessment–Recommendation (SBAR), Repeat Back and Verify, and Introduce–Discuss–Explain–Act (IDEA), which ensure clarity, accuracy, and inclusivity when discussing safety concerns or procedural uncertainties. By embracing a questioning mindset through tools like Qualify–Verify–Validate (QVV) and Ask–Request–Concern–Chain of Command (ARCC), teams are encouraged to challenge unsafe practices and escalate concerns respectfully. Together, these behavioral tools reinforce a shared commitment to safety, transforming sharp injury prevention from a checklist into a mindset woven into every action and interaction.
Fostering personal accountability and active engagement in a safety culture can be a constructive and even enjoyable experience for researchers. Incorporating creative, game-based approaches into training provides an effective way to transform safety education into interactive learning opportunities. Games can be energizing, creative, and fun to provide education. Safety professionals can transform learning opportunities into interactive games that foster sharps safety while building team camaraderie. Activities like Colored Jenga, Spinning Wheel, and Jeopardy turn trivia into dynamic learning moments, while Legos and Risk Assessment Matrix help visualize exposure and prioritize interventions. Games such as Spot the Problem and Scenario-Based Role Play encourage critical thinking and real-world application. These playful formats not only make safety training more memorable but also empower researchers to take ownership of their environment. By embedding safety into engaging formats, institutions cultivate a culture where vigilance and collaboration thrive, proving that safety can be both serious and fun.
Specific targeted initiatives such as tissue sectioning policies and guidelines were created to combat sharp injuries. Microtome and cryostat tissue sectioning policies are essential safeguards designed to prevent sharp injuries and ensure consistent, safe operation of precision instruments. These policies outline rigorous first-time operation requirements, including reading institutional guidelines, developing standard operating procedures (SOPs) tailored to specific equipment models, and completing supervised training with documentation uploaded to a centralized tracking system. Once trained, researchers must adhere to recurring operation protocols such as wearing appropriate PPE, securing blades, maintaining a clean workspace, and using mechanical tools to handle sharps.21–23 Cleaning procedures further reinforce safety by mandating disinfectant use and mechanical removal of debris and blades. Together, these structured safety practices not only reduce the risk of lacerations and needlestick injuries but also reinforce a culture of accountability and procedural rigor within the research environment. Targeted initiatives that highlight the importance of policy-driven safety, particularly in high-risk activities such as tissue sectioning, are essential for ensuring consistent adherence to best practices and sustaining a safe, high-reliability laboratory culture.
Materials and Methods
Adaptation of the CDC Sharps Injury Prevention Framework for Program Development at AWRI
The CDC Workbook for Designing, Implementing, and Evaluating a Sharps Injury Prevention Program served as the primary framework for developing the institutional sharps injury reduction initiative. The workbook provides a structured, evidence-informed approach for assessing existing sharps-related hazards, forming multidisciplinary safety teams, evaluating injury trends, and selecting engineered controls to mitigate risk. Although originally developed for healthcare systems, its core principles such as baseline assessment, hazard identification, engineering control evaluation, and program monitoring are readily transferable to research environments, including academic laboratories, vivarium, and other scientific facilities.
To align the methodology with a research setting, the workbook’s recommended organizational steps were adapted to laboratory-based equivalents. Processes such as forming a working group, reviewing reporting practices, and analyzing injury trends paralleled institutional mechanisms already in place for laboratory safety oversight. This allowed the research institution to maintain alignment to the workbook’s continuous-quality-improvement model while tailoring implementation to laboratory operations.
At AWRI, a multidisciplinary team was convened consisting of Safety leadership, departmental safety representatives, and research personnel. This team conducted a baseline assessment using sharps-related injury data from 2019 to 2025, consistent with the CDC’s emphasis on evaluating current program performance. The assessment included characterization of reporting practices, identification of high-risk procedures, and review of laboratory processes involving sharps. High-risk activities were identified in areas such as cryostat and microtome operation, animal-handling procedures, and manual manipulation of sharp devices.
Intervention strategies were selected based on the hazard assessment and in accordance with CDC recommendations for prioritizing engineering and substitution controls. AWRI implemented targeted substitutions (e.g., polycarbonate blades, retractable syringes) and introduced engineered controls such as needle-recapping devices and magnetic-tip brushes. Complementary administrative interventions included updated sectioning policies, hands-on training workshops, and integration of engagement tools such as the Zero Hero™ safety program.
Program implementation was accompanied by ongoing monitoring to evaluate reductions in injury numbers and improvements in reporting behavior. This cyclical evaluation approach reflects the continuous-quality-improvement framework central to the CDC workbook. Through this structured adaptation, AWRI effectively translated a health care-oriented safety model into a research-focused sharps-injury prevention program.
Injury Surveillance and Data Analysis Methods
A comprehensive review of institutional injury records was conducted to characterize the distribution, severity, and causes of sharp-related incidents among research personnel. Sharps injury surveillance was initiated by examining the frequency and type of injuries reported over time. Injuries were categorized into animal-related injuries, cryostat and microtome injuries, needlesticks, razorblade injuries, scalpel injuries, and other miscellaneous sharp events. Injury severity was classified into two groups: nonrecordable injuries and OSHA-recordable injuries. OSHA-recordable injuries were defined according to federal criteria requiring documentation when an event results in death, days away from work, restricted duty or job transfer, medical treatment beyond first aid, or loss of consciousness. For our organization, most of these injuries require treatment beyond first aid.
Sharps injury data from 2019 to the present were extracted from the institutional risk-management software (Riskonnect). Incident data were then organized and analyzed using Microsoft Excel. Analytical procedures included calculation of descriptive statistics, such as proportions and proportional changes over time, to identify trends and recurring injury patterns. This dataset served as the foundation for identifying high-risk tasks and informing the development of targeted injury-prevention interventions. The analysis revealed elevated injury frequencies in activities involving cryostat and microtome operation, needle recapping, animal handling, and the use of common utility tools such as box openers. These findings guided the implementation of administrative controls, updated institutional policies, the introduction of safer sharps devices, and enhanced hands-on training programs aimed at reducing both the frequency and severity of sharp-related injuries across the research enterprise.
Zero Hero™ safety tools and behavioral reinforcement
To strengthen institutional safety practices, the AWRI implemented the enterprise-wide Zero Hero™ program, an initiative designed to promote consistent daily safety behaviors and standardized communication. All AWRI personnel are required to complete Zero Hero™ training during onboarding and annually thereafter through a virtual 1-h module. The training emphasizes structured communication and behavioral safety tools, including SBAR, STAR, and Stop & Resolve.
These standardized tools were deliberately embedded into sharp injury prevention activities and related educational interventions to support real-time hazard recognition, improve clarity of communication, and ensure timely escalation of safety concerns. Personnel applied these strategies during routine and non-routine operations, particularly when facing ambiguous or potentially unsafe circumstances. For example, SBAR provided a structured framework for communicating changes during equipment modifications or procedural revisions, while Stop & Resolve empowered individuals to pause work and obtain clarification when uncertainty or potential hazards were identified. Integration of these behavioral safety tools served to reinforce an educational framework aligned with AWRI broader institutional safety culture and strategic commitment to achieving zero harm.
Training interventions: Workshops and engagement activities
Sharps-safety education and equipment distribution were delivered primarily through in-person workshops designed to increase accessibility and cross-departmental participation. Workshops were held in high-traffic, nonlaboratory areas and incorporated hands-on demonstrations, brief coaching, interactive quizzes, and game-based learning formats (e.g., safety trivia, biosafety bingo, etc.). Participation was encouraged through small incentives such as food coupons, branded items, and laboratory supplies. Safer sharp devices, including guarded box openers, retractable syringes, and magnetic-tip tools, were distributed during these sessions to reinforce proper technique and support immediate adoption.
Workshops were implemented in phases based on emerging needs and incident trends. The first sharps-focused event was held in September 2020, followed by a second workshop in June 2021. In response to an increase in OSHA-recordable cryostat and microtome injuries, a formal tissue-sectioning policy was introduced in March 2022, and an additional workshop was conducted in August 2022 to reinforce new procedural requirements. Since 2022, annual sharps-safety workshops have been maintained, supplemented by 8–12 general laboratory safety workshops per year.
Training modalities included in-person sessions, online modules, one-page flyers, and short instructional videos. Personnel were permitted to transition to safer sharp devices at their own pace, with legacy tools remaining available when required for specific procedures. Workshops were designed for brief participation (typically <15 min) and emphasized hands-on exposure to safer alternatives.
These sessions also served as opportunities for observational assessment and feedback. Safety culture surveys and preference assessments were administered using Microsoft Forms, and observations during workshops informed subsequent training modifications, particularly for high-risk groups such as vivarium personnel. Policies and SOPs were communicated broadly through quarterly meetings, institutional webpages, and direct email distribution to ensure consistent dissemination and uptake.
Ongoing Monitoring and Program Evaluation
Program effectiveness was evaluated continuously throughout the intervention period using institutional sharp injury surveillance data. Injury distribution, OSHA-recordable events, and trends in severity were monitored routinely to assess changes over time. Staff engagement metrics from workshops, along with observational findings and feedback from departmental safety teams, were incorporated to refine educational content, adjust supply distribution, and target high-risk areas.
This evaluation framework combined quantitative injury data with qualitative input from training sessions and departmental observations. The integration of injury surveillance, engineering controls, education, and behavioral-based training supported iterative program improvements and informed ongoing adjustments to maintain a proactive and sustainable sharps-injury prevention environment.
Results
Trends in Sharps Injury Distribution and Outcomes Following Safety Interventions
Figure 1 summarizes sharp injury data collected from 2019 through 2025, representing a 7-year evaluation period during which AWRI implemented multiple sharp-specific safety interventions. Across the study period, injury trends demonstrated notable variation in reporting patterns, injury severity, and workforce-adjusted risk. Sharp injury data showed fluctuations in both OSHA-recordable and non-OSHA-recordable incidents. OSHA-recordable cases reached a peak of 10 incidents in 2022, followed by a marked decline to 1 incident in 2025, the lowest value observed during the 7-year period. Non-OSHA-recordable injuries remained relatively stable from 2019 to 2023, averaging 10–11 incidents annually, before increasing to 18 incidents in 2024 and subsequently decreasing to 9 in 2025. Total annual sharp injury counts followed similar patterns, increasing to 21 incidents in 2024 and declining to 10 in 2025.
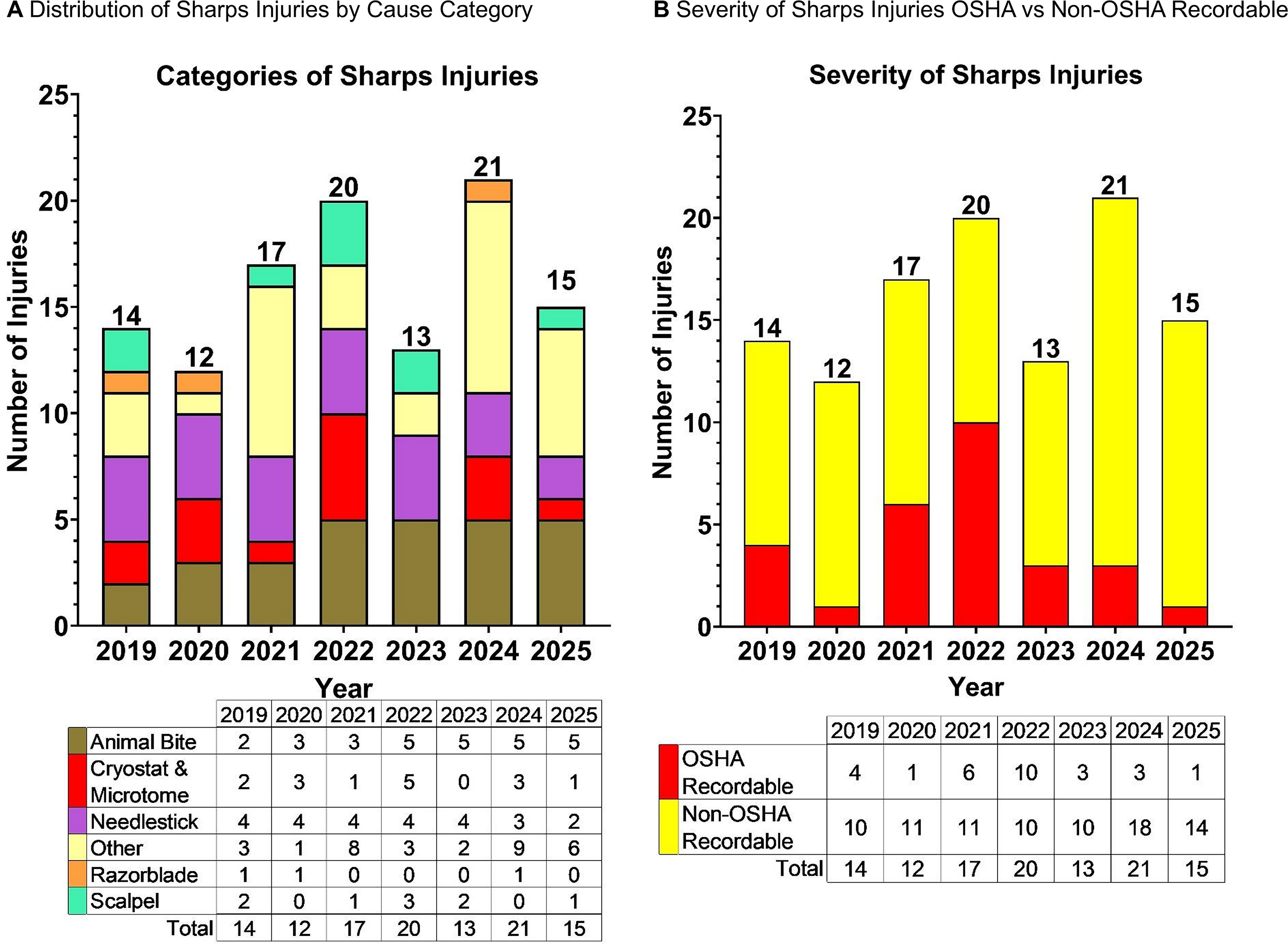
Between 2022 and 2023, sharp injury counts among research staff decreased by 35% (20–13 incidents), occurring concurrently with a substantial workforce expansion of 141 additional full-time employees during that period. OSHA-recordable incidents decreased by 70% during the same interval (10–3 incidents). These reductions occurred during the implementation of targeted interventions that included workshops, coaching, equipment-related policy revisions, and institutional emphasis on safe work practices. Following these improvements, a subsequent increase in non-OSHA-recordable injuries was observed in 2024.
From 2023 to 2024, overall sharps-injury counts increased by 62% (13–21 incidents), although OSHA-recordable cases remained unchanged at three incidents in both years. Between 2024 and 2025, overall sharps injuries decreased by 38% (21–15 incidents), and OSHA-recordable incidents declined by 67% (3–1 incidents).
Workforce hours varied considerably across the study period, increasing from 1,987,622 h in 2019 to 3,072,784 h in 2024, a 54.6% increase, before declining to 2,615,903 h in 2025 (31.6% above 2019 levels). Year-to-year changes were + 17.1% (2020), + 1.2% (2021), + 7.5% (2022), + 9.6% (2023), + 10.7% (2024), and –14.9% (2025). The analysis revealed notable fluctuations in incident counts over the study period, reflecting changes in workforce conditions. It is important to note that this study did not calculate incident rates. While rate-based measures are widely recognized as critical for evaluating injury trends, complete and consistent denominator data (e.g., workforce size or hours worked) were not available across all study periods. As a result, the findings are based on raw incident counts and corresponding percentage changes over time. Accordingly, the reported trends should be interpreted as changes in the number of reported incidents rather than definitive changes in sharps injury rates.
Analysis of injury categories revealed shifting patterns from 2019 to 2025. Total incidents peaked in 2024 (21) and declined to 15 in 2025. Animal-bite injuries remained consistently elevated from 2021 to 2025, representing a persistent risk category. Needlestick injuries showed a gradual decline over time, decreasing from four incidents annually in 2019–2023 to two incidents in 2025. Injuries associated with cryostat and microtome equipment increased in 2022 and subsequently fluctuated, while scalpel and razor blade injuries remained consistently low. The “other” category showed substantial variability, including marked increases in 2021 and 2024, which may reflect changing reporting practices or emerging hazards.
Several targeted safety initiatives occurred during the study period, corresponding with shifts in sharp injury trends. The first sharp safety workshop was conducted in September 2020, followed by a second workshop in June 2021. A formal cryostat/microtome tissue-sectioning policy was implemented in March 2022, and a third sharp-safety workshop reinforcing this policy was delivered in August 2022. Beginning in 2023, annual sharp-safety workshops were introduced and continue to the present. These initiatives were temporally aligned with subsequent reductions in OSHA-recordable incidents, including the 70% decrease observed from 2022 to 2023, and the sustained decline in severe injuries through 2025.
Sharps-Injury Mitigation Strategy and Intervention Methods
A structured risk-based assessment guided the development of the sharps-injury mitigation strategy. Variables evaluated included injury frequency, OSHA recordability, type of injury, and the associated laboratory or animal-care procedures. Severity was a primary consideration, with microtome and cryostat-related lacerations identified as high-impact events due to their frequent need for clinical treatment and OSHA recordability. These findings informed the selection of targeted engineering, administrative, and training interventions implemented across the study period.
Cryostat and microtome interventions
Injury surveillance in 2022 identified five tissue-sectioning injuries, several of which were OSHA-recordable. Contributing factors included manual manipulation of blades, failure to lock handwheels during use, and inconsistent adherence to cut-resistant glove requirements. In response, the institution implemented a revised tissue-sectioning policy requiring trainers to document ≥40 h of experience on each device, assignment of device-specific SOPs, and use of a standardized training checklist completed by trainers and users. Procedural updates emphasized cut-resistant gloves worn beneath nitrile gloves and the use of magnetic-tip brushes for blade removal and tissue retrieval. Following implementation, cryostat- and microtome-related injuries declined to zero in 2023 and remained low for the remainder of the evaluation period.
Needlestick injury prevention
Needlestick injuries were most frequently associated with syringe disposal, manual recapping, animal inoculation procedures, and transport of prepared injections. Because certain workflows required recapping, stabilized one-handed recapping devices were introduced to reduce hand-to-needle contact. Retractable syringes with automated needle-shielding mechanisms were also implemented to reduce disposal-related injury risk. These devices were distributed during safety workshops and placed in high-use areas of the Animal Resources Core to promote consistent adoption. Monitoring over subsequent years demonstrated a steady reduction in needlestick-related injuries.
Animal bite risk reduction
Animal bites represented a substantial proportion of sharps-related injuries, particularly during restraint, cage transfer, and procedural preparation involving mice, rats, and ferrets. To address these risks, focused animal-handling training reinforced proper restraint techniques, bite-resistant gloves were introduced for ferret-related activities, and scruff guards were deployed for procedures requiring stable immobilization. These measures corresponded with reductions in bite-related injury severity and increased consistency in safe-handling practices across the vivarium.
Utility-tool injury controls
Lacerations from utility tools including box cutters, scalpel blades, and razor blades were often associated with routine tasks such as unpacking supplies and gel preparation. To mitigate these injuries, traditional box cutters were replaced with guarded models, and metal razor blades were substituted with polycarbonate alternatives for gel manipulation. Demonstrations, instructional videos, and departmental training supported the correct use of the substituted tools. After these changes, utility-tool-related lacerations decreased and remained consistently low throughout the later years of the study period.
Figure 2 summarizes the engineered safer-sharp substitutions introduced across the evaluation period. These substitutions were intended to minimize direct contact with sharp edges, reduce manual handling, and incorporate passive or active safety features. For animal-bite injuries, scruff guards provided a reusable restraint option to reduce handling-related bite risk. For cryostat and microtome procedures, magnetic brushes facilitated hands-free blade handling and disposal. To address needlestick hazards, several devices were introduced, including one-handed needle recappers, retractable syringes, single-handed needle-safe devices, and needle boxes serving as secondary containment. Additional substitutions targeted other sharp-injury categories, such as plastic razor blades for gel manipulation, retractable disposable scalpels to reduce handling after use, and cut-resistant gloves and guarded box openers for general laboratory tasks. Collectively, these engineered substitutions were implemented alongside administrative and training measures described above. Their introduction aligned temporally with observed declines in OSHA-recordable injuries and overall sharp injury counts during the latter portion of the study period (Figure 1).
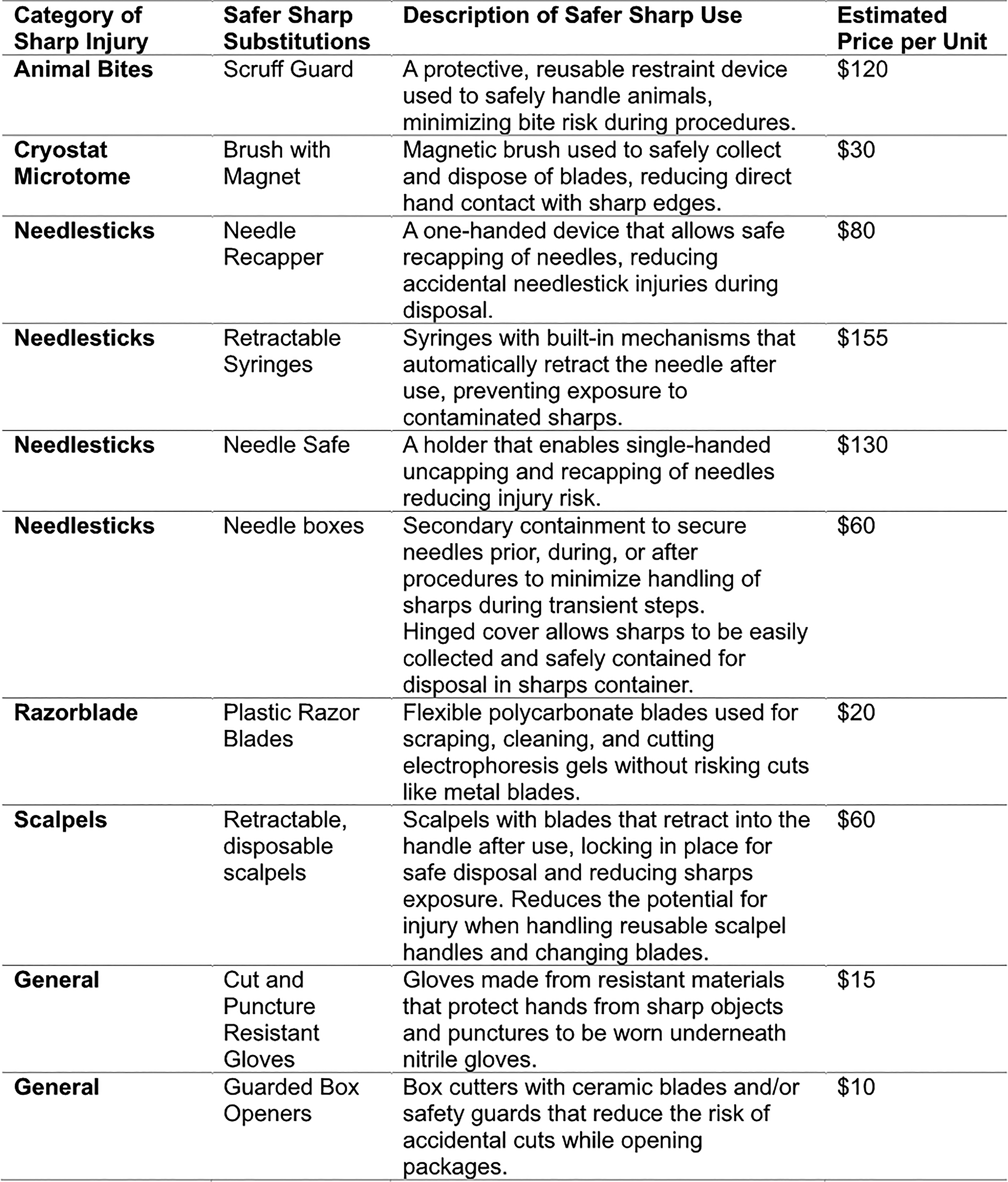
Safer Sharp Substitutions.
Integration of Behavioral-Safety Tools to Support Sharps-Injury Prevention
During the evaluation period, institutional Zero HeroTM tools were incorporated into sharps-related workflows to support hazard recognition, decision-making, and communication (Figure 3). These tools fell into three domains (i) personal safety behaviors, (ii) communication strategies, and (iii) a questioning mindset. These Zero Hero tools were applied across laboratory and animal-care operations.
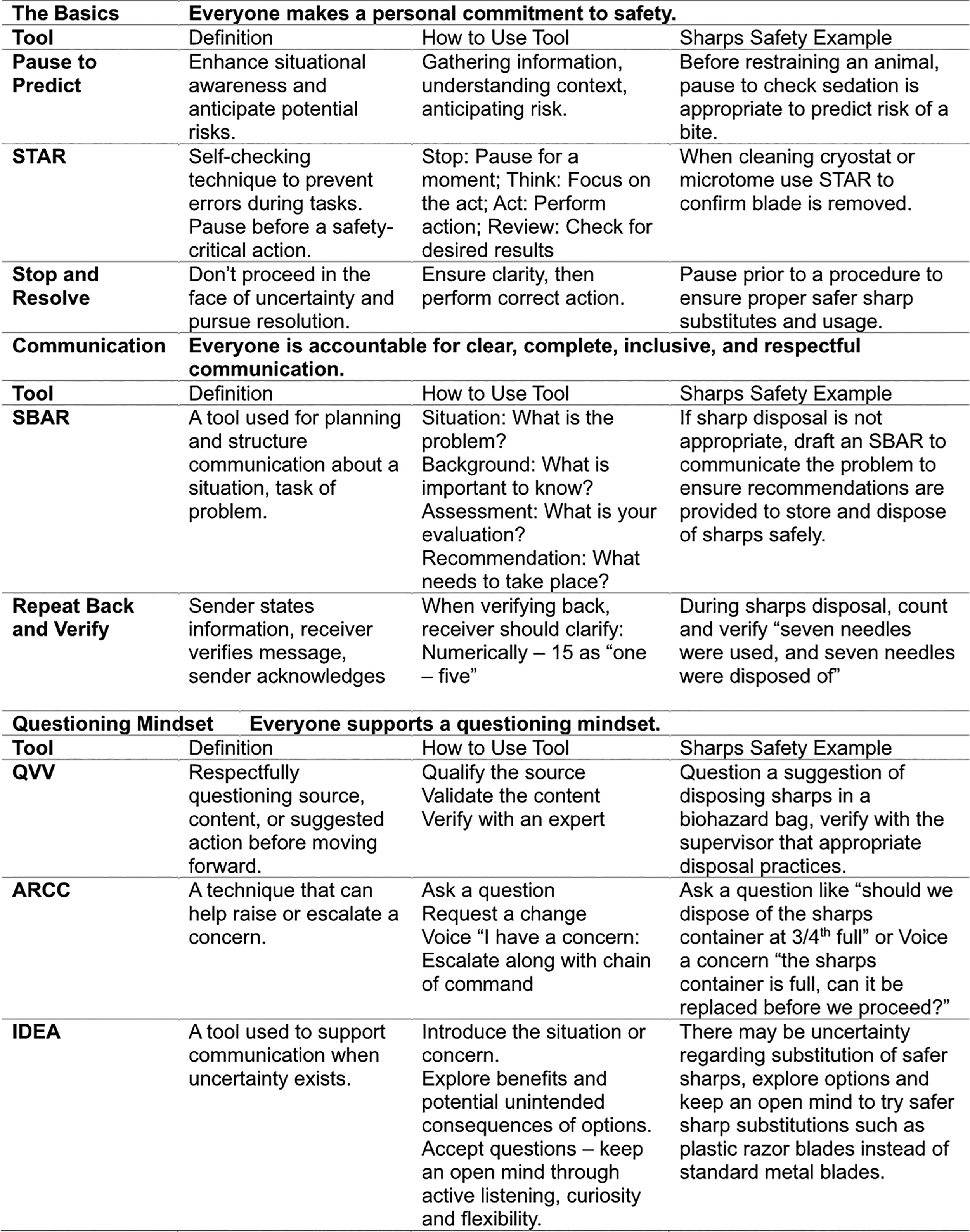
Zero HeroTM Tools for Situations with Sharp Risk.
Personal safety behaviors
Foundational practices were used to increase situational awareness and reduce risk before engaging in sharps tasks. Pause to Predict encouraged staff to assess hazards prior to procedures such as animal restraint or sharps handling. The STAR method provided a structured self-check for tasks like cryostat or microtome operation, including verification of locked handwheels and correct PPE. Stop and resolve allowed employees to pause when uncertain and confirm proper safer-sharp substitutions or equipment setup.
Communication tools
Communication-focused behaviors supported clarity during sharps-related activities. SBAR was used to communicate disposal concerns or recommend safer alternatives. Repeat Back and Verify ensured accurate information transfer during sharps disposal and inventory, reducing errors related to unsecured or miscounted sharps.
Questioning mindset
Inquiry-driven tools supported verification of safe practices. QVV helped confirm information related to disposal, equipment status, or procedural requirements. The ARCC technique (Ask a question, request a change, Voice a concern, Use the chain of command) enabled escalation of safety concerns, including identification of safer substitutions such as plastic razor blades or guarded box openers. The IDEA tool promoted structured discussion when uncertainty existed, allowing teams to evaluate options before proceeding (Figure 3).
Collectively, these behavioral and communication tools were integrated into daily operations to reinforce consistent sharps-safety practices. Their use aligned with the period in which reductions in total sharps injuries and OSHA-recordable incidents were observed across the institution.
Engagement Strategies to Promote Researcher Learning in Sharps Safety
During the evaluation period, a series of interactive educational activities were incorporated into safety programming to enhance researcher engagement with sharps-related procedures and risk-mitigation concepts (Figure 4). These activities consisted of structured games designed to reinforce key principles such as safe disposal, appropriate tool selection, hazard recognition, and use of safer sharps substitutions. The games were integrated into workshops and hands-on training events across laboratory and vivarium environments.
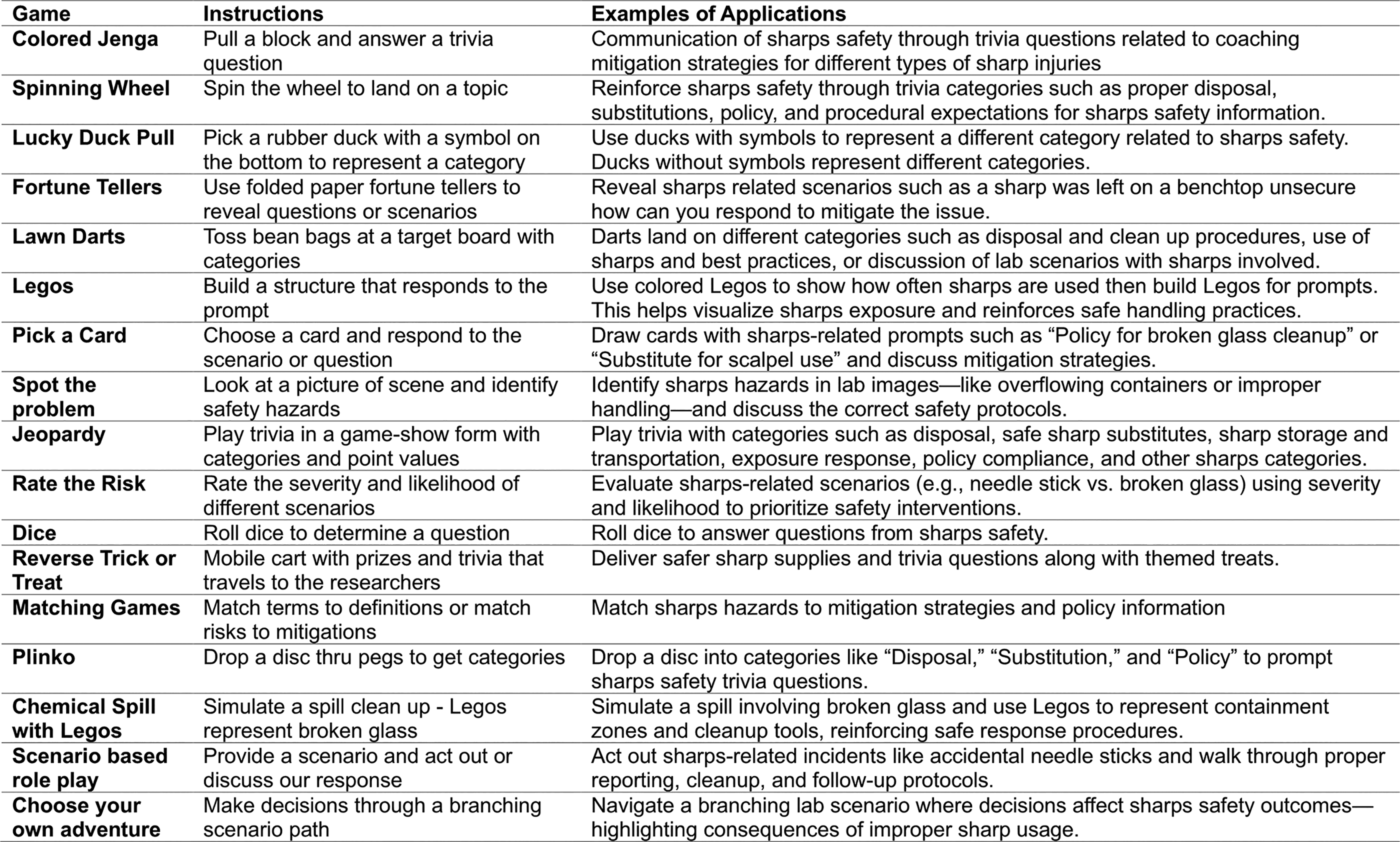
Games to Encourage Researcher Learning and Engagement with Research Safety.
Several activities focused on reinforcing sharps-safety knowledge through guided prompts or scenario-based decision-making. Trivia-style formats including Colored Jenga and Jeopardy were used to review institutional policies, disposal methods, and substitution strategies through randomized questions (Figure 4). Similarly, the Spinning Wheel and Lucky Duck Pull engaged participants in discussions aligned with the category selected, such as safer alternatives, storage and transport practices, or procedural risk-reduction steps. Other activities emphasized hazard identification and situational assessment. The Spot the Problem and Pick a Card exercises presented images or scenarios depicting sharps-related risks, prompting participants to identify unsafe behaviors such as improper containment, unsecured devices, or lack of proper PPE. Lawn-dart-style targeting games and fortune-teller prompts were used to guide discussion on best practices and corrective actions.
Hands-on activities were incorporated to strengthen understanding through physical representations of laboratory hazards. Legos were used to demonstrate sharp related processes, including how improper placement or transfer might increase exposure risk. Games such as Chemical Spill with Legos simulated cleanup workflows and safe use of containment tools. Matching-based activities, including Matching Games and Plinko, reinforced the alignment of hazards with appropriate mitigation strategies or institutional policies (Figure 4).
Several games supported applied decision-making in dynamic or branching scenarios. Rate the Risk, Reverse Trick or Treat, and Choose Your Own Adventure guided participants in evaluating the severity of sharps-related outcomes, choosing safer alternatives, and predicting consequences of improper sharps handling. Collectively, these interactive activities provided structured opportunities for researchers to practice hazard recognition, engage with safety policies, and apply safer sharp concepts in a controlled learning environment.
Tissue Sectioning Policy Development and Implementation of Safer Sharp Alternatives
Consistent with CDC prioritization principles, AWRI ranked risks primarily by severity particularly OSHA recordability rather than frequency alone. This approach aligned with the institution’s Zero Hero™ initiative, which promotes sustained progress toward zero harm regardless of event frequency. The prioritization process guided the selection of targeted controls. AWRI developed and implemented a comprehensive tissue-sectioning policy to address recurrent injuries associated with microtome and cryostat use. The policy, outlined in Figure 5, established standardized operational requirements and revised procedures for both trainers and instrument users. Key elements included mandatory credentialing for trainers, requiring a minimum of 40 documented operational hours on each instrument type, creation of user-specific SOPs, and completion of structured training checklists prior to independent operation. The policy also emphasized reading the instrument manual, receiving orientation from a qualified individual, and following detailed recurring-use guidelines related to safe blade handling, mechanical aid usage, equipment guards, and proper PPE.
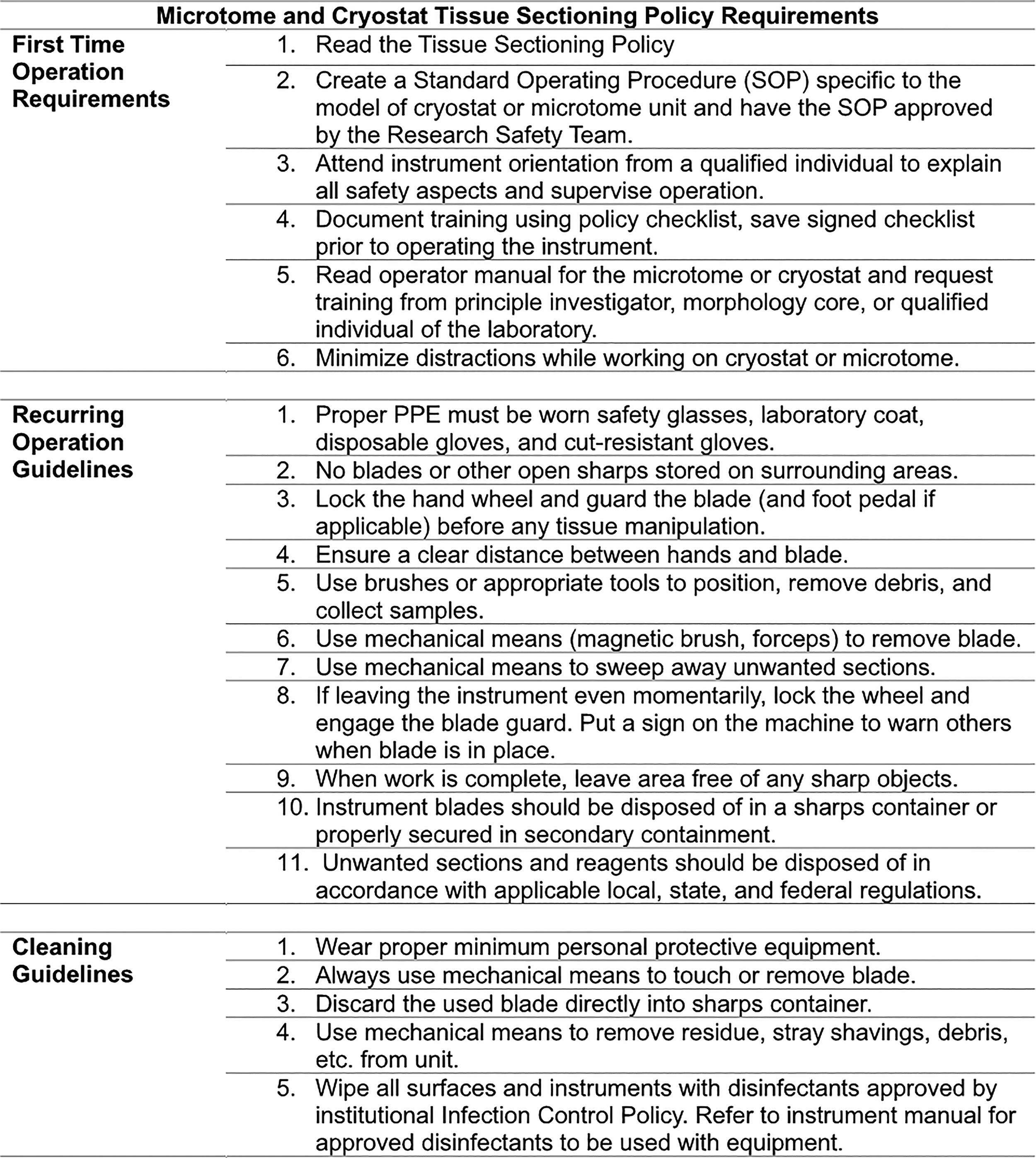
Cryostat and Microtome Policy Guidelines.
To minimize manual interaction with cryostat and microtome blades, the safety team distributed engineered safety devices such as cut-resistant gloves, magnetic-tip brushes, and forceps to facilitate hands-free removal of blade debris and tissue shavings. Additional procedural controls included explicit requirements for locking handwheels, guarding blades when equipment was unattended, maintaining clear work areas, and disposing of unwanted sections and blades in approved sharps containers. Cleaning guidelines further standardized post-use decontamination using approved disinfectants and noncontact methods to remove shavings and residual debris.
In parallel with policy development, AWRI introduced a range of safer-sharp alternatives across research laboratories, summarized in Figure 2. Safer-sharp alternatives were integrated through multiple communication channels, including online training modules, instructional videos, and printed guidance materials. These resources supported consistent adoption of substitution practices for syringes, scalpels, razor blades, and general laboratory utility tools. Collectively, the tissue-sectioning policy and the deployment of safer-sharp devices established uniform expectations for equipment handling and reduced opportunities for manual blade contact within high-risk workflows.
Discussion
Sharps injuries present a significant occupational risk for research personnel, particularly when working with bloodborne pathogens such as Hepatitis B, Hepatitis C, and HIV. 1 These injuries, which can occur through various sharp instruments such as needles, scalpels, and razors, carry the potential for serious health implications. Effective sharps safety practices are critical in minimizing these risks, and institutions such as NCH have implemented comprehensive safety initiatives to reduce sharp-related injuries.
The results from AWRI targeted interventions, including specialized workshops, training, and the introduction of safer equipment, show a marked reduction in sharps injuries. A 35% decrease in overall sharps injuries and a 70% reduction in OSHA recordable incidents in 2023 demonstrate the success of these initiatives. The institution’s approach, which combined engineering controls, administrative actions, and hands-on safety training, contributed to a safer research environment. This decrease in injuries is also attributed to specific policy changes and improvements in equipment handling, such as updates to cryostat and microtome policy, the introduction of safer needle recapping devices, and the provision of retractable syringes.
In addition, the involvement of research personnel in workshops, the use of engaging activities for education, and the incorporation of Zero Hero™ safety principles helped foster a culture of safety within the organization. As a result, AWRI not only reduced sharps injuries but also demonstrated the effectiveness of a multifaceted safety program that prioritizes prevention, education, and continuous monitoring. Moving forward, ongoing education and the adoption of safer technologies will continue to play a key role in reducing the risk of sharps injuries in research settings.
While the outcomes of this initiative were positive, several limitations and confounding factors should be acknowledged. First, the increase in non-OSHA-recordable reports in 2024 may reflect improved reporting culture rather than a true rise in incidents, making year-to-year comparisons complex. Second, the voluntary nature of adopting safer sharp substitutes means that user preference may have influenced injury patterns, potentially confounding the measured impact of specific engineering controls. Third, no formal follow-up surveys were conducted to quantify long-term behavioral change, and user adherence to safer devices was assessed indirectly through injury trends and observational feedback rather than direct measurement. In addition, a key limitation of this study is the absence of calculated incident rates. Although rate-based comparisons are essential for accurately assessing injury trends, the analysis relied on raw incident counts and percentage changes over time due to incomplete denominator data across study periods. Consequently, the observed trends should be interpreted as changes in reported incident counts rather than definitive changes in true incident rates.
With regard to comparison to existing literature, few published studies have described a multi-pronged, institution-wide injury-reduction strategy tailored specifically to research environments. Many sharp prevention frameworks originate from health care settings, whereas AWRI approach adapts these models for laboratory use by integrating engineering changes, policy updates, behavioral training, and equipment substitution. As a result, this work contributes to a relatively limited body of evidence demonstrating how layered controls can be effectively applied in nonclinical research institutions.
Implementing these interventions also presented operational challenges. Staff worked across diverse research programs with varying risk profiles, requiring custom approaches rather than a single standardized system. Ensuring consistent adoption of new devices was difficult, as some workflows required legacy tools or unique handling techniques. Time and resource constraints limit the ability to conduct formal evaluations of behavior change, and distributing equipment across a large institution requires sustained coordination with laboratories. A further challenge included balancing safety improvements with workflow disruption, particularly in the vivarium and high-output laboratories.
The timeline for implementation spanned several years, with most new controls and training components rolled out between 2022 and 2024. Revising the tissue-sectioning policy alone required significant planning time, including development of SOPs, training checklists, and trainer credentialing requirements as well as working with the laboratories to appropriately enroll in the new policy. Workshops and equipment distribution occurred 8–12 times each year over 12–24 months, and program refinement continued as injury data and staff feedback became available. This extended implementation period allowed the institution to phase in improvements while ensuring user understanding and operational continuity.
It is evident that behavioral interventions and organizational culture play a pivotal role in reducing needle stick injuries. 9 Research highlights that compliance with safety protocols is often influenced by individual attitudes, perceived behavioral control, and the presence of supportive leadership. At AWRI, the integration of Zero Hero™ safety principles aligns with these findings by reinforcing positive safety behaviors and encouraging accountability. When personnel feel empowered and supported in their safety practices, adherence to protocols becomes more consistent, leading to sustained reductions in injury numbers.
The importance of continuous feedback and incident reporting systems as part of an effective injury prevention strategy is evident. AWRI’s success can be partially attributed to its commitment to ongoing monitoring and transparent reporting mechanisms, which allow for the timely identification of risk patterns and targeted interventions. This proactive approach mirrors the review’s recommendation for dynamic safety systems that evolve based on real-time data and employee input. By fostering open communication and integrating frontline feedback into policy development, institutions can create adaptive safety environments that respond to emerging challenges and reinforce a culture of vigilance.
In addition, all these initiatives show the value of multidisciplinary collaboration in designing and implementing sharps injury prevention programs. AWRI’s initiatives reflect this by involving researchers, safety officers, and leaders in the development of training modules and equipment upgrades. Such cross-functional engagement ensures that safety measures are both practical and contextually relevant, enhancing their effectiveness. As research settings continue to diversify and evolve, maintaining this collaborative model will be essential in addressing the complex factors that contribute to sharps injuries and ensuring the long-term success of prevention efforts.
Conclusion
Through strategic, data-informed interventions, AWRI successfully reduced sharps injuries and improved lab safety culture. This model demonstrates how institutional commitment, employee engagement, and continuous improvement can work synergistically to achieve tangible safety outcomes in high-risk research environments. The importance of tailoring interventions to address both behavioral and systemic factors contributing to sharps injuries is a recurring theme. Findings suggest that effective prevention requires more than just equipment upgrades, it demands a holistic approach that includes behavioral training, leadership support, and a culture of accountability. AWRI’s success exemplifies this principle, as its initiatives not only introduced safer technologies but also cultivated a proactive mindset among staff. By aligning institutional goals with individual responsibility and fostering a shared commitment to safety, AWRI created an environment where best practices are consistently reinforced and sustained.
Authors’ Contributions
S.G. and K.C.: Conceptualization (ideas; formulation or evolution of overarching goals). J.C. and S.P.: Methodology and project administration (Implementation of the safer sharp mitigation practices). J.M. and M.B.: Developing the Zero Hero tools described throughout the article. H.M. and K.B.: Implementation of Safety initiatives and Zero HeroTM tools utilized for safer operations; S.G.: Formal analysis. S.P. and S.G.: Writing—original draft (preparation, creation, and/or presentation of the published work, explicitly writing the initial draft. S.G.: Supervision (oversight and leadership responsibility for the research activity planning and execution, including mentorship external to the core team).
Disclaimer
The views presented in this publication are those of the authors and do not necessarily reflect the position of the associated institutions.
Authors Disclosure Statement
No competing financial interests exist.
Footnotes
Acknowledgment
The authors thank leadership at the Abigail Wexner Research Institute at Nationwide Children’s Hospital for supporting the safety initiatives and publication of this article.
Funding Information
The authors received no financial support for this article’s research, authorship, and publication.