
Abstract

Electricity and chemicals enable neurons to communicate. Adding either to the brain can change how it functions. The mainstay of treating epilepsy is antiseizure medications—essentially, chemicals—but medications do not control seizures in many patients. For decades, clinicians and scientists have explored whether electricity can reduce seizures when medications cannot, potentially with fewer systemic side effects. The National Institute of Neurological Disorders and Stroke (NINDS) recognized the potential in this idea early, partnering with investigators, hospitals, and people with epilepsy nationwide to establish how electrical stimulation can be delivered to the brain safely and effectively. Both currently approved intracranial stimulation therapies for epilepsy—deep brain stimulation (DBS) and responsive neurostimulation (RNS)—trace essential parts of their development to NINDS-funded research.
Not all stimulation strategies ultimately proved effective, and here too the NINDS played a decisive role: the institute funded not only early innovation, but also the key replication and validation studies that distinguished promising ideas from those unable to withstand rigorous testing. These efforts, beginning as early as the 1960s, steered the field away from ineffective approaches and toward the therapies that benefit patients today, all while leaving open compelling hypotheses that may yet merit reexamination with modern tools.
Early Work: The Cerebellum
Interest in cerebellar involvement in epilepsy emerged from observations of cerebellar atrophy in some patients with seizures and early experiments showing that cerebellar manipulation could alter seizure expression in animal models. For example, in the 19th century, Risien Russell found that motor manifestations of seizures, induced by injecting absinthe into the jugular vein of dogs, were exaggerated ipsilateral to cerebellar resections. 1
These results led Robert Dow and colleagues at the Good Samaritan Hospital in Portland, with support from the NINDS, to address this more completely in the early 1960s. 2 Their experiments involved 100 rats, a cobalt model of epilepsy, and numerous cerebellar manipulation techniques, such as ablation, electrical stimulation, and focal cooling (accomplished by fixing atop the cerebellum a piece of metal foil that was in contact with dry ice outside the closed incision). Both ablation and cooling worsened seizures, suggesting an inhibitory role of the cerebellum in epilepsy, and the effects of electrical stimulation were mixed, with some testing worsening and some testing improving seizures.
Enthusiasm for cerebellar stimulation grew, and Irving Cooper in New York performed such procedures in 100 patients. The open-label results were promising for these patients who had few other options, but the procedure remained controversial. The NINDS recognized the need for validation and funded a randomized controlled trial led by John van Buren and colleagues at the National Institutes of Health in Bethesda. 3 They implanted the cerebellar hemispheres of 5 patients with 4-contact Avery electrodes (Figure 1), which, in turn, were connected to implanted pacemakers. Seizures did not improve, but families were reportedly pleased with the results, perhaps due to patients’ increased arousal.
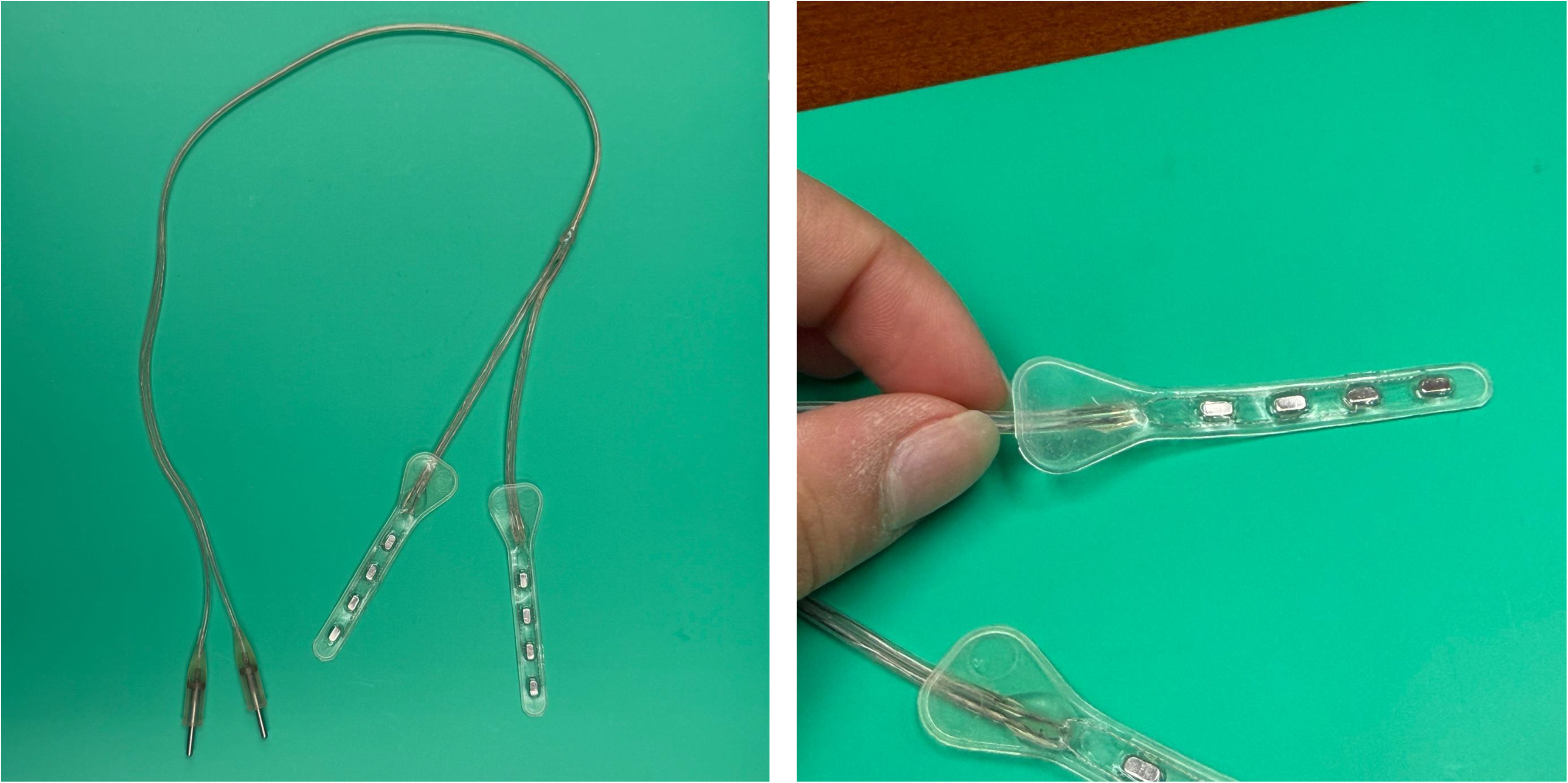
Avery model E333 electrode arrays, used in pioneering early work of cerebellar stimulation for epilepsy in the 1970s. 3 This photo was graciously provided by Gabriela Martins and Linda Towler of Avery Biomedical Devices, which continues today as a leader in diaphragmatic pacemaker stimulation.
Follow-up studies in nonhuman primates confirmed the absence of seizure reduction but replicated the arousal effect. 4 In hindsight, the cerebellum's complex and heterogeneous connectivity makes such divergent findings unsurprising. With modern neuroimaging, tractography, and a deeper understanding of cerebellar functional organization, renewed interest in cerebellar neuromodulation is emerging.
Shifting Focus: The Thalamus
The notion of stimulating structures outside the cortex to treat seizures proved tenacious, with particularly fruitful attention directed toward the thalamus. Marek Mirski and James Ferrendelli, in elegant NINDS-funded research performed at Washington University in St. Louis and published in Science, showed that ablation of the mammillothalamic tract (MMT) abolished seizures in the pentylenetetrazol (PTZ) model of epilepsy in guinea pigs. 5 While this would eventually motivate study of the anterior nucleus of the thalamus (ANT) as a target for DBS, it is prescient that the optimal target for ANT–DBS today seems defined by the entry of the MMT to the ANT or, in some studies, the MMT itself.
The same duo, with sustained support from the NINDS, moved on to experiments directly assessing the role of ANT in acute PTZ-induced seizures in the same model. 6 Seizures were abolished by ANT injections of muscimol, a GABA agonist that putatively silenced the nucleus. This effect was stronger in the ANT than in the nearby mediodorsal or ventral anterior nuclei, illustrating the specificity of this nucleus. Notably, these seizures were the acute generalized seizures of PTZ, not the kindled seizures that occur spontaneously after PTZ-induced kindling. While ANT–DBS has its strongest evidence of effectiveness in temporal lobe epilepsy, there are some reports of using ANT for generalized epilepsy, and early observations of NINDS-funded investigators may support that indication.
Building on this foundational animal work, the NINDS directly supported its clinical translation: DBS of the ANT to treat drug-resistant focal seizures. A small study of 5 patients led by investigators at the Barrow Neurological Institute, University of Pennsylvania, and Stanford University, showed improvement in generalized tonic–clonic seizures and focal seizures that would lead to falls, though DBS did not improve overall seizure counts. 7 This initial success helped justify the larger SANTE pivotal trial, for which the NINDS helped fund the planning. SANTE included 110 patients and was essential for securing Food and Drug Administration approval of this therapy. ANT–DBS is now a standard treatment for drug-resistant focal epilepsy when resection or ablation is not an option.
Closed-Loop Stimulation
The only other approved intracranial stimulation therapy for epilepsy is RNS, and critical work that drove its development was funded by NINDS. During extraoperative mapping using electrocorticography electrodes, Ron Lesser and colleagues found that electrical stimulation could abort runs of after-discharges. 8 Their pivotal paper was exceptionally forward thinking, anticipating lines of inquiry still pursued by RNS researchers today, such as how antiseizure medications might alter the response to stimulation and whether electrographic biomarkers might predict response (intriguingly, they noted that areas with more interictal discharges were less likely to respond). They close their paper with prescient speculation: “In theory, a treatment such as ours could be linked to a detection method.” Indeed!
A real-time detection method was being developed in parallel by other groups, again supported by the NINDS. Ivan Osorio, for instance, developed a wavelet-based seizure detector and showed it could reliably detect seizures with a small number of intracranial electrode contacts in play, anticipating the devices that would soon be employed for closed-loop neuromodulation. 9 And it was with NINDS support that one of the first closed-loop bedside neurostimulation systems was developed, confirming the feasibility of this approach. 10 This work culminated in the fully implantable RNS system, now used in over 8000 patients, with ongoing active research into stimulation optimization, biomarkers of response, and long-term plasticity.
In summary, the field of neurostimulation for epilepsy did not advance linearly. Instead, it progressed through bold exploration, careful validation, and strategic redirection—processes consistently guided and supported by NINDS. The result is that today, patients who previously had no viable treatment options now have multiple evidence-based neuromodulation therapies that meaningfully reduce seizures and improve quality of life. Those therapies, and many more that will follow in the years ahead, are the enduring legacy of the NINDS in neuromodulation.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.D.R. and V.R.R. have served as paid consultants for NeuroPace but declare no targeted funding from NeuroPace for this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.