
Abstract
Mental health equity is a critical issue for people with epilepsy (PWE), who bear a disproportionate burden of psychiatric and cognitive comorbidities. Conditions such as depression, anxiety, attention-deficit/hyperactivity disorder, autism spectrum disorder, functional/dissociative seizures, and cognitive impairment occur more frequently in PWE, contributing to elevated morbidity, mortality, and reduced quality of life. Many of these disorders have bidirectional relationships with epilepsy, reflecting overlapping biological, psychological, and social mechanisms. Social Determinants of Health (SDoH), including educational opportunities, access to health care, neighborhood and environmental exposures, social and community context, and economic stability, further shape risk, presentation, and outcomes across the lifespan. Children with epilepsy and neurodevelopmental disorders face academic and service inequities, while adults encounter barriers in mental health access and stigma that may worsen depression and anxiety. Older adults with epilepsy and dementia experience additional disparities driven by socioeconomic status and minority status. This narrative review synthesizes current evidence on the epidemiology, risk factors, and mechanisms linking epilepsy with psychiatric, neurodevelopmental, and neurodegenerative conditions, with an emphasis on how SDoH exacerbates inequities. We identify gaps in mechanistic research and highlight the underrepresentation of vulnerable populations. To advance equity, strategies must include routine SDoH screening, integration of psychosocial and neurologic care, stigma-reduction efforts, and development of culturally competent, patient-centered interventions. Policy initiatives that address structural barriers to care are also essential. Together, these approaches can improve outcomes and promote health equity for PWE.
Keywords
Introduction
People with epilepsy (PWE) experience a disproportionate burden of psychiatric, neurodevelopmental, and neurodegenerative comorbidities, contributing to excess morbidity, premature mortality, and reduced quality of life.1–5 Depression, anxiety, attention-deficit/hyperactivity disorder (ADHD), autism spectrum disorder (ASD), functional/dissociative seizures, cognitive impairment, and dementia occur more frequently in PWE than in the general population. Social determinants of health (SDoH)—defined as the conditions in which people are born, grow, live, work, and age—shape vulnerability to these comorbidities and their outcomes. 6 Educational opportunities, access to health care, neighborhood and environmental exposures, social and community context, and economic stability are all relevant to mental health equity in epilepsy. 7 Recent studies highlight that adverse SDoH increase the likelihood of psychiatric comorbidity, reduce treatment access, and exacerbate disparities across the lifespan. 5 The impact of these factors differs across developmental stages. In childhood and adolescence, SDoH influences educational attainment, service use, and long-term cognitive outcomes.8–10 In adulthood, stigma, employment instability, and healthcare access barriers contribute to a heightened risk of depression and anxiety. In older adulthood, the combined effects of limited financial resources, social inequities, and underrepresentation amplify the likelihood of cognitive decline and other negative health outcomes in PWE.11,12 This narrative review examines the intersection of epilepsy and psychiatric/cognitive comorbidities, and SDoH across the lifespan. We synthesize epidemiology, risk factors, and mechanisms; identify gaps in knowledge; and propose clinical, research, and policy strategies to advance mental health equity for PWE.
Conceptual Framework
Healthy People 2030 defines 5 domains of SDoH: education access and quality, health care access and quality, neighborhood and built environment, social and community context, and economic stability. 13 These domains provide a structured lens for examining disparities in epilepsy care. A lifespan perspective highlights how these domains impact mental health equity differently across various developmental stages. During childhood and adolescence, educational resources and neighborhood factors significantly impact neurodevelopment, learning, and access to supportive services. In adulthood, healthcare barriers, stigma, and employment instability drive risk for depression and anxiety. In later life, socioeconomic disadvantage and minority status intersect with neighborhood deprivation to compound risks of epilepsy-associated dementia. Systemic barriers, including fragmented care, underinsurance, stigma, and inequitable access to mental health services, undermine outcomes. In contrast, facilitators such as integrated care models, patient navigation programs, and culturally competent practice can promote equity. Together, this framework underscores the need to address SDoH systematically across the lifespan to improve mental health outcomes in epilepsy (Figure 1). Key SDoH domains and their relevance across major neuropsychiatric comorbidity groups are further summarized in Table 1.
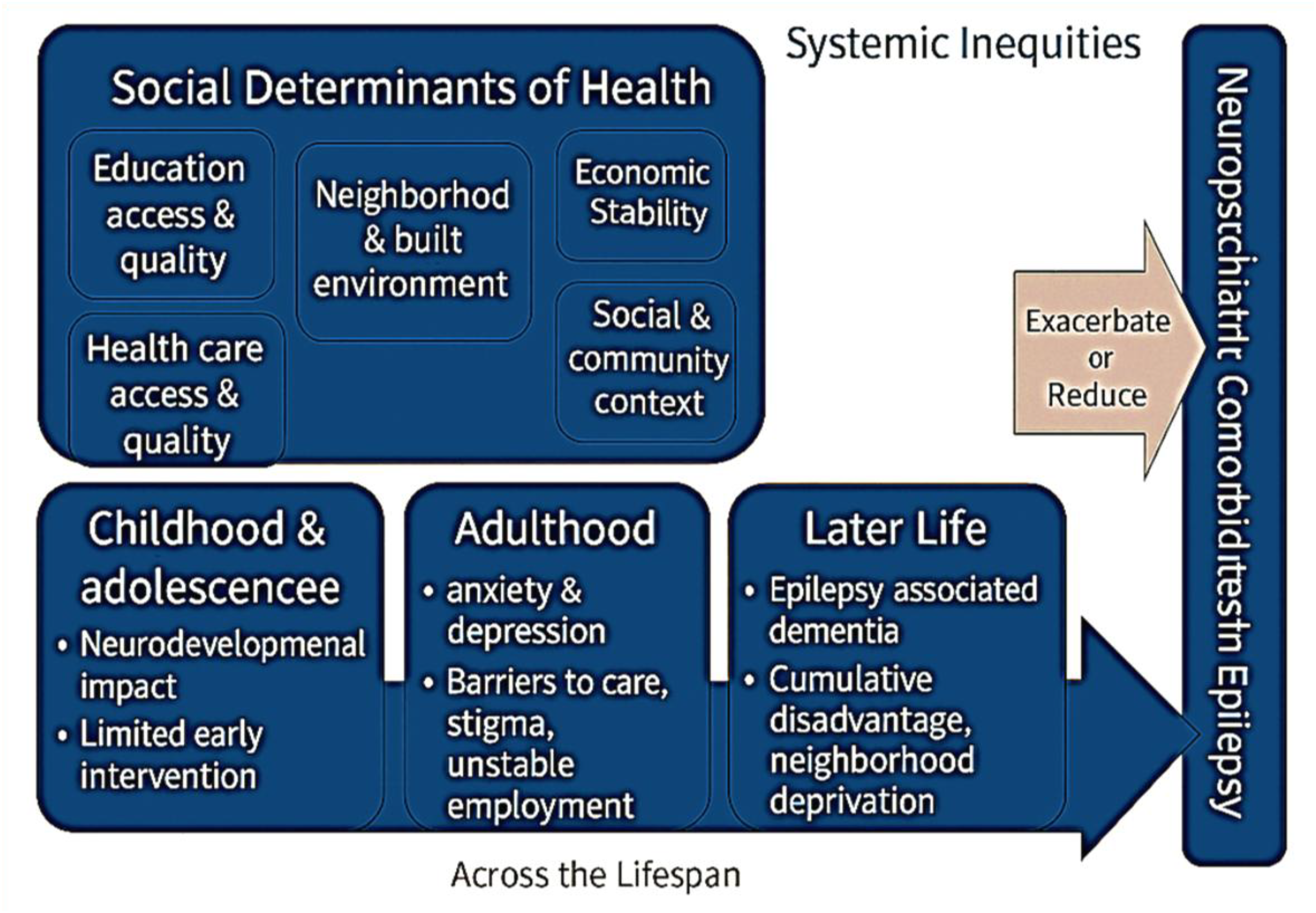
Social Determinants of Health Framework for Neuropsychiatric Comorbidities in Epilepsy.
Summary of Social Determinants of Health Across Comorbidities in Epilepsy.
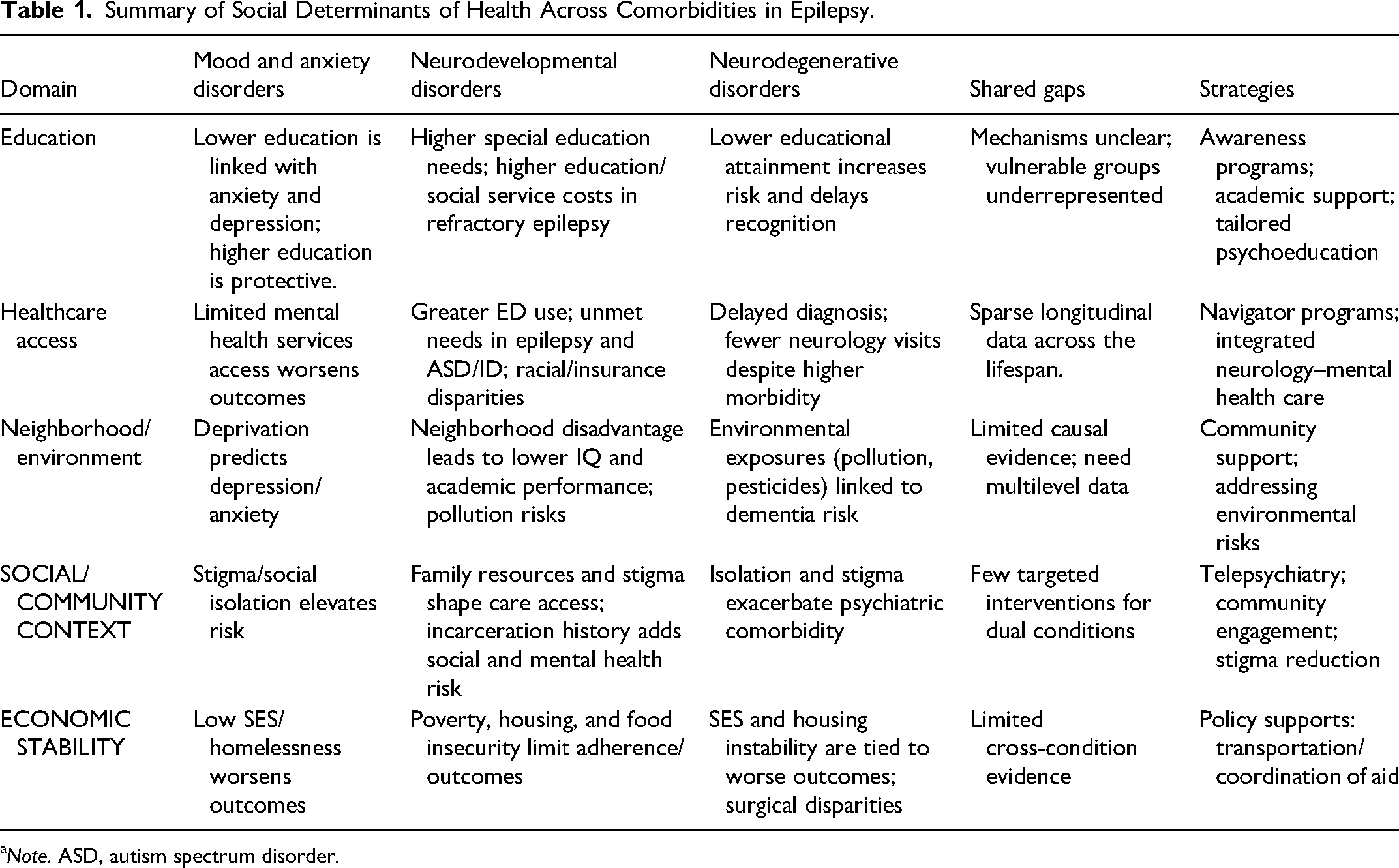
Note. ASD, autism spectrum disorder.
Methods
This narrative review was conducted to synthesize key evidence on the SDoH influencing psychiatric and cognitive comorbidities in epilepsy. Unlike a systematic review, it was not intended to be exhaustive but to integrate findings across developmental stages and clinical contexts. Searches were performed in PubMed, PsycINFO, and Scopus using terms related to epilepsy, mental health, cognition, disparities, and social determinants. Relevant peer-reviewed articles, reviews, and conceptual papers were included if they addressed the relationships between SDoH domains, education, healthcare access, neighborhood and environment, social and community context, or economic stability, and outcomes in pediatric or adult epilepsy populations. Evidence was synthesized thematically to highlight mechanisms, disparities, and key gaps for future research and clinical application.
Epilepsy, Mood Disorders, and Anxiety Disorders
Major depressive disorder and anxiety disorders are the most common psychiatric conditions in PWE, affecting approximately 1 in 3 individuals over the lifetime.14–16 Bipolar disorder is less prevalent, but also seems to have a higher prevalence in PWE, though it is less well studied. 17 Epilepsy and depression appear to have a bidirectional relationship, but this has not been clearly shown for anxiety disorders. 18 Clinical predictors of mood disorders and anxiety disorders include factors that can be associated with SDOH and others that are not. One non-SDoH-related predictor of depression and anxiety disorders is polytherapy. However, other clinical factors, such as poor seizure control or seizure severity, have not been consistently associated with mood or anxiety disorders. 19
SDoH in Mood and Anxiety Disorders
SDoH-related factors that have been associated with depression in PWE include older age, female sex, low education level, unemployment, and stigma. 20 In comparison, anxiety disorders have been associated with female sex, unmarried/divorced/widowed status, low socioeconomic status, poor educational attainment, and illness-related shame. 19 Poor educational attainment may be associated with depression and anxiety because it is linked to diminished access to protective socioeconomic resources, including social support networks and psychological treatments.21,10,12,13 Neighborhood deprivation can independently predict depressive and anxiety symptoms beyond seizure-related factors in PWE due to poorer health care and education access, as well as food insecurity.7,22 Economic instability, including low socioeconomic status and homelessness, further worsens outcomes, and stigma remains a pervasive determinant across settings.23,24
Gaps and Strategies—Mood and Anxiety Disorders
Key gaps include a mechanistic understanding of how SDoH drives psychiatric risk in PWE and understudying of less common conditions, such as bipolar disorder.23,25 Priority strategies include routine psychosocial screening; stigma-reduction interventions; culturally competent, patient-centered care; patient-facing tools to elicit priorities; and navigator programs addressing transportation and coordination barriers.24,26
Epilepsy and Neurodevelopmental Disorders
Approximately 35% of children and adolescents with epilepsy have co-occurring neurodevelopmental diagnoses such as ASD, intellectual disability, or ADHD; conversely, about 30% of individuals with ASD have epilepsy.27,28 Shared risk factors include genetic predisposition and environmental factors—such as exposure to air pollution, which one study reported as associated with increased neurodevelopmental risk (Volk et al, 2013)—within a differential susceptibility model, in which contextual adversity may heighten underlying vulnerability.29–32
SDoH in Neurodevelopmental Disorders
Neurodevelopmental comorbidities in epilepsy reflect the combined effects of biological vulnerability and SDoH. Children and youth with epilepsy (CWE) and comorbid neurodevelopmental disorders experience inequitable access to both health and special education services, including higher healthcare and social service costs, suboptimal access to healthcare services, and are less likely to have health services that meet their needs. 33 CWE with cognitive impairment and refractory epilepsy experience the highest need for special education services, while CWE with ASD and ID felt that available health services failed to meet their needs. 33 Adults with developmental disorders and epilepsy are more likely to depend upon public health insurance, 34 which can limit the availability of providers and access to certain treatments. In pediatric populations, children with comorbid epilepsy and cognitive impairment experience greater health care costs. In clinical settings, caregivers of CWE and ASD and ID reported more frustration with accessing care for their child compared to families of children with only ASD or epilepsy. 33 They felt that available health services failed to meet their needs. Further, of children with epilepsy and ASD, 36% also had an intellectual disorder. Children with epilepsy, ASD, and ID were less likely to have health services that met their needs. 33
Neighborhood disadvantage predicts lower cognitive and academic performance in children with epilepsy, which persists over time and has a greater impact than other clinical variables.35,36 Exposure to environmental hazards (eg, fine particulate matter, nitrogen oxides) is linked to increased risks for neonatal encephalopathy and febrile seizures, which are associated with later ADHD and ASD.31,32,37,38 Family stress, poverty, housing instability, food insecurity, parental incarceration exposure, and stigma shape developmental trajectories, limited access to services, and negatively impact medication adherence.24,26,39
Gaps and Strategies—Neurodevelopmental Disorders
While high prevalence of neurodevelopmental disorders has been well-established in epilepsy, primary gaps include the limited research on effective interventions to reduce the negative impacts of SDoH in neurodevelopmental disorders in epilepsy. Due to the ongoing caregiver needs for some people with neurodevelopmental disorders, more strategies for supporting caregivers in this population are needed. Key strategy includes timely referrals to assessment/therapies for young children with epilepsy who may have a neurodevelopmental comorbidity and increased training in both adult-focused epileptologists (for neurodevelopmental disorders) and ASD specialists (to treat patients with epilepsy).
Epilepsy and Neurodegenerative Disorders
Seizure risk is elevated across dementias—including Alzheimer's disease, vascular dementia, dementia with Lewy bodies, frontotemporal dementia, and Down syndrome–associated dementia.40–43 Epilepsy and dementia exhibit a bidirectional association: each confers at least a twofold increase in risk for the other in population-based cohorts. Shared risk factors include age, ApoE4 status, proteinopathies (amyloid, tau, alpha-synuclein), cerebrovascular disease, traumatic brain injury, smoking, and lower educational attainment. 44
SDoH in Epilepsy–Neurodegenerative Disorders Overlap
Patients with comorbid epilepsy and dementia may be at an elevated risk for accidents and injuries due to frailty, cognitive impairment, polypharmacy, and deconditioning, which may result in elevated morbidity and mortality.45–47 SDOH factors, such as lower socioeconomic status, isolation, stigma, and limited transportation access, may exacerbate these risks by delaying and limiting access to healthcare resources. Greater SDOH needs have been associated with increased emergency department resource utilization and lower likelihood of survival. In contrast, patients with a poorer educational attainment at baseline may be at risk for worse cognitive outcomes. 48 Environmental exposures, including air pollution, pesticides, metals, solvents, and residential deprivation have been explored as possible contributors to dementia risk, although the evidence for many factors (such as electromagnetic fields, pesticides, SO₂ levels, neighborhood socioeconomic status, and rural living) is considered low-to-very-low quality discrimination may indirectly increase risk via cardiovascular and psychiatric pathways.49,50
Gaps and Strategies—Neurodegenerative Disorders
There is sparse research specifically addressing SDoH in patients with both epilepsy and dementia. Longitudinal, standardized cohorts are necessary to clarify the timing and mechanisms involved, as well as to test interventions.26,39 Although often challenging to implement, brief SDoH screening within epilepsy clinics, integrating telepsychiatry and community programs to reduce isolation, and prioritizing tailored interventions for minority and low-resource populations remain practical, near-term steps.26,39
Table 1 summarizes the major SDoH domains, how they influence mood, neurodevelopmental, and neurodegenerative comorbidities in epilepsy, and the cross-cutting gaps and strategies identified in this review.
Future Directions
Mechanistic studies linking social context to neurobiological change in epilepsy and its comorbidities remain scarce. To advance understanding, multilevel, longitudinal research designs are needed that incorporate neighborhood-level data, patient-reported outcomes, and standardized SDoH screening. Such approaches can illuminate how environmental and social exposures intersect with genetic and neurobiological vulnerabilities to shape psychiatric and cognitive trajectories across the lifespan. In addition, pragmatic implementation trials should evaluate the effectiveness of patient navigation models, stigma-reduction programs, and integrated neurology–behavioral health interventions in real-world settings. Special emphasis should be placed on culturally competent and equity-focused strategies, as well as inclusion of historically underrepresented groups, to ensure findings are generalizable and relevant to diverse populations. Expanding partnerships across health systems, schools, and community organizations will also be essential to identify and address structural barriers that perpetuate disparities in epilepsy care.
Conclusions
Epilepsy's intersections with mood, neurodevelopmental, and neurodegenerative disorders are shaped as much by social and environmental context as by underlying neurobiology. Recognition of SDoH as key drivers of psychiatric and cognitive outcomes reframes comorbidities not only as clinical challenges but also as health equity priorities. Advancing mental health equity will require embedding SDoH assessment and culturally competent psychosocial care into routine epilepsy practice, while ensuring care pathways are accessible, coordinated, and patient-centered. Policy-level initiatives that address insurance gaps, socioeconomic inequities, and community-level resources are equally critical. Finally, future research must prioritize diverse and underserved populations, with attention to lifespan-specific risks and protective factors, in order to generate solutions that are both scientifically rigorous and socially just.
Statements and Declarations
Margaret Gopaul has received research support at Yale University for an investigator-initiated study from Patient-Centered Outcomes Research Institute.
Kelly Conner has received research support from the American Association of Physician Associates for an investigator-initiated study for the All of Us Database.
Mary Wojnaroski was a one-time consultant for BVF partners.
Heidi Munger-Clary receives research support related to mental health comorbidities of epilepsy or other mental health conditions from the Department of Defense, Duke Endowment, National Science Foundation via Eysz, Inc., and Susanne Marcus Collins Foundation. She serves as a consultant for Xenon Pharmaceuticals, including as a content expert on anxiety and depression in epilepsy. She receives payment as associate editor of Epilepsia Open.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.