
Abstract
Nearly 1% of the global population suffers from epilepsy. There are over 65 million people worldwide with epilepsy and approximately 10.5 million of those are children. One third of these people have drug-resistant epilepsy (DRE). Neuromodulation is an adjunct treatment option for these patients. This manuscript aims to describe the history, patient/parent perspective, current use, and future directions of neuromodulation in the management of pediatric DRE. We conducted a nonsystematic search of the literature through different databases as part of the Pediatric State of The Art Symposium at the 2025 American Epilepsy Society meeting in Atlanta. Three neuromodulation therapies, all using implanted devices and electrodes, have been approved by the Food and Drug Administration (FDA) to treat DRE, namely, vagus nerve stimulation (VNS) (1997 and lately 2017), deep brain stimulation of the anterior nucleus of the thalamus (ANT-DBS) in 2018 (2010 in Europe), and responsive neurostimulation (RNS) in 2013. Only VNS is approved in pediatric patients. Emerging noninvasive neuromodulation modalities such as noninvasive VNS and transcranial magnetic stimulation showed mild adverse effects and exhibit the most encouraging seizure and neurocognitive outcomes to date, but larger multicenter studies are essential before these modalities can be offered and integrated into standard pediatric epilepsy care.
Keywords
Introduction
Nearly 1% of the global population suffers from epilepsy. There are over 65 million people worldwide who are estimated to have epilepsy, including approximately 10.5 million children.1,2 One third of these people have drug-resistant epilepsy (DRE). 3 Neuromodulation is an adjunct treatment option for these patients. This therapy produces electrical or magnetic stimulation to modify the nerve activity through targeted delivery of stimuli, involving direct or induced electrical current, with the goal of decreasing seizure frequency, severity, and/or duration. 4 Three neuromodulation therapies, all using implanted devices and electrodes, have been approved by the Food and Drug Administration (FDA) to treat DRE, namely, vagus nerve stimulation (VNS) (1997 and lately 2017), deep brain stimulation of the anterior nucleus of the thalamus (ANT-DBS) in 2018 (2010 in Europe), and responsive neurostimulation (RNS) in 2013. 5 VNS is currently the only one of these treatment approved by the FDA to pediatric patients with a DRE indication.
At the 2025 American Epilepsy Society Meeting the Pediatric State of the Art Symposium addressed the history, patient/parent perspective, current use, and future directions of neuromodulation in the management of pediatric DRE. This manuscript serves to highlight the up-to-date information presented on this topic.
Methods
A nonsystematic search of the bibliography was done through different databases including PubMed, Medline, Scopus, and Lillacs as part of the Pediatric State of The Art Symposium at the 2025 American Epilepsy Society meeting in Atlanta.
History of Neuromodulation in Epilepsy
Neuromodulation first entered the literature in 1884 with the publication of “the galvanic current effect in the pneumogastric nerve” by Leonard Corning using insulated sponge electrodes; he posited that the device reduced blood flow into the central nervous system to create its effect. 6 Fifty years later, a report stated that stimulation of the vagus nerve (VN) increased the potential of the orbitofrontal cortex (based on cortical electrograms) and decreased blood pressure due to anoxemia. 7 Subsequently, studies in cats (Encéphale isolé) demonstrated it was possible to reduce or eliminate spontaneous cortical spindles and strychnine induced spikes through repetitive central vagal stimulation. 8 In the 1990s, human studies with a VNS implantable device demonstrated seizure reduction of more than 50% in patients with focal epilepsy.9,10 Other studies done only in the pediatric population reported similar outcomes.11–13 Recently, VNS was found to be effective in generalized tonic clonic seizures with 77% seizure reduction in adult and pediatric patients. 14
Subsequently, Penfield studied neurostimulation by using cortical electrical probes. This formed the foundation for the development of a stereotactic apparatus improving the accuracy of neurosurgical procedures and electrical stimulation (later becoming the deep brain stimulator (DBS)).15,16 Initial targets included the brainstem, frontopolar cortex, spinal cord, and thalamus based on the localization of Parkinson disease, psychiatric disorders, and chronic pain.16–18 Advances during the 1980s and 1990s led to decreased size of the devices, the addition of lithium batteries increasing longevity. 19 More recently, a randomized clinical trial (SANTE) demonstrated the efficacy and tolerability of DBS in people with epilepsy (PWE). 20 This technology has advanced to include real time monitoring of electrical activity and stimulation and subsequently the development of external responsive neurostimulators.21,22 Researchers found the electrographic seizures were suppressed by direct brain stimulation.21,22 Later advances in automated seizure detection led to the development of RNS. 23
Expectations of PWE and Their Families Regarding Neuromodulation
The landscape of pediatric epilepsy surgery today encompasses a growing menu of surgical treatments for pediatric DRE, including neuromodulation. This treatment should be framed as a meaningful and proactive option rather than as a fallback when resective surgery is not recommended. Families and clinicians could discuss minimally invasive procedures as focused ultrasound, endovascular embolic, or robotic thermocoagulative approaches, in addition to VNS, RNS, and DBS neuromodulation technologies.24,25
Parent decision-making studies in neuromodulation technologies for DRE identified three branches: features of the intervention; decision drivers shaped by relational trust and contextual barriers; and the sources/quality of information parents use. 26 Parents are most concerned about the direct risks and benefits of surgical and device-based interventions. There is a general aversion to open or highly invasive surgical procedures, and parents often prefer to try less invasive neurotechnologies first. In doing so they underappreciate the risks of ongoing seizures, instead focusing on the risks of new procedures and technologies. Parents weigh their child's overall quality of life improvements (including cognition, behavior, and independence) at least as heavily as seizure freedom. Barriers such as access to treatment, financial challenges, insurance limitations, and family considerations are equally influential. Parents obtain decision-making information from a variety of sources, including clinical teams, online materials, peer networks, and social media.27,28
The term “palliative” is commonly used to describe neuromodulation technologies, yet as Englot notes “… we rarely refer to anti-seizure medications (ASM) as ‘palliative,’ even though they may be considered such. So, why would we use the word when referring to epilepsy surgery?”. 29 This terminology undervalues significant life-changing benefits to cognition, safety, and daily function even when seizures do not fully resolve. Curative surgeries do not guarantee seizure freedom forever. 30 For many in the general public, “palliative” connotes pain management, end-of-life care, and the notion of “giving up.” 31 Recent commentary supports retiring “palliative” from epilepsy surgery altogether, in favor of language that reflects the comprehensive improvements these interventions – including neuromodulation technologies – can offer. 32
Parents of children with DRE experience significantly elevated levels of stress even before surgery, driven by uncertainty, constant vigilance, and the demanding nature of care. 33 Pediatric neurosurgery adds an undeniable layer of stress for families, with evidence showing that almost half of parents display enough symptoms to warrant a diagnosis of post-traumatic stress disorder (PTSD) following the child's neurosurgical procedure. 34 Studies demonstrate that while stress may decrease postsurgery, levels remain elevated compared to controls. 35 Because neuromodulation does not promise seizure freedom, clinicians should presume high parental stress will persist, regardless of the intervention's invasiveness. 34 Notably, mothers suffer disproportionately high rates of depression and anxiety for years after a child's epilepsy surgery. 36 The pediatric epilepsy surgery journey must be recognized as a source of trauma affecting the entire family that demands a trauma-informed approach throughout both the pre- and postsurgical care of these families to address this persistent psychological burden.
Choosing the Appropriate Device in Children with DRE Not Amenable to Surgical Resection
Role of the Vagus Nerve Stimulator
VNS is an FDA-approved as adjunctive therapy for pediatric patients with DRE who are > 4-years-old. This device involves unique multi-level mechanisms including modulation of neurotransmitter expression, cerebral blood flow, and EEG desynchronization. VNS increases acetyl choline, 37 norepinephrine, 38 dopamine and GABA, 39 reduces aspartate and modulates glutamate 39 balancing inhibition/excitation, influencing synapsis and brain-gut communication.40–42 It also reduces inflammation, 37 increases serotonin and thalamo-cortical blood flow, 43 as well as desynchronizing EEG rhythms through the amygdala into the limbic system. 44
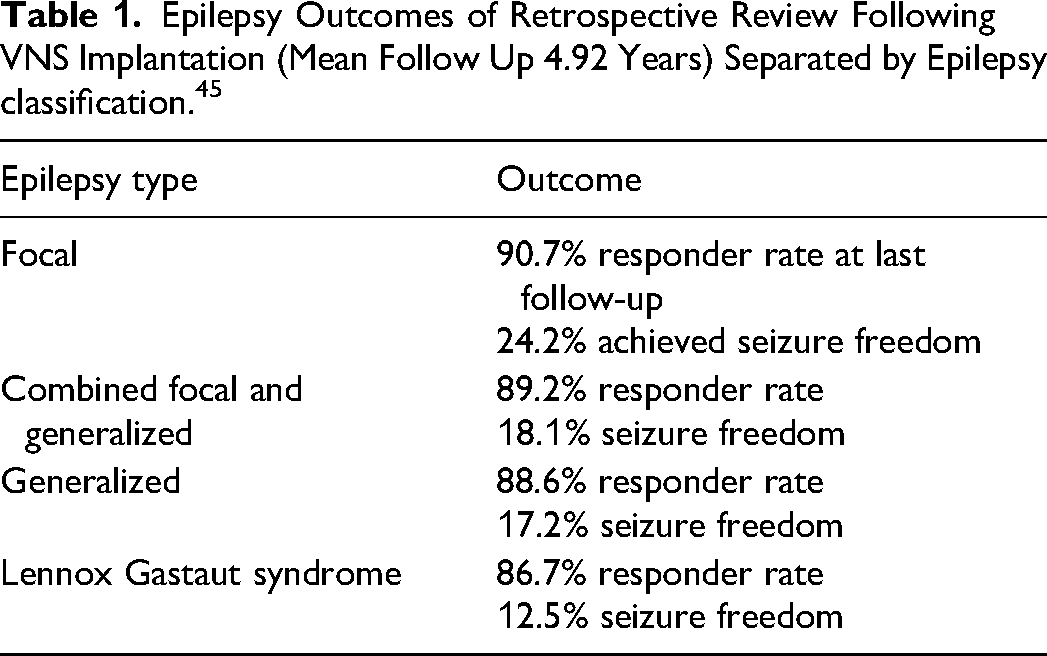
In a retrospective cohort of 400 pediatric patients followed over 20 years, VNS demonstrated robust overall responder rates: 44.9% at 3 months, 68.8% at 6 months, 80.9% at 12 months, 85.3% at 24 months, and 90.5% at last follow-up, with 20.5% of patients achieving complete seizure freedom at their final assessment. Early VNS implantation and individualized adjustment of parameters were critical predictors of optimal outcomes. Increasingly higher output and duty cycle parameters are used sooner to improve outcome. 45 Most adverse events were manageable with protocol adjustments, and quality of life measures improved significantly across multiple domains. Outcomes varied by epilepsy type as seen in Table 1. 45
Epilepsy Outcomes of Retrospective Review Following VNS Implantation (Mean Follow Up 4.92 Years) Separated by Epilepsy classification. 45
Role of the Deep Brain Stimulator
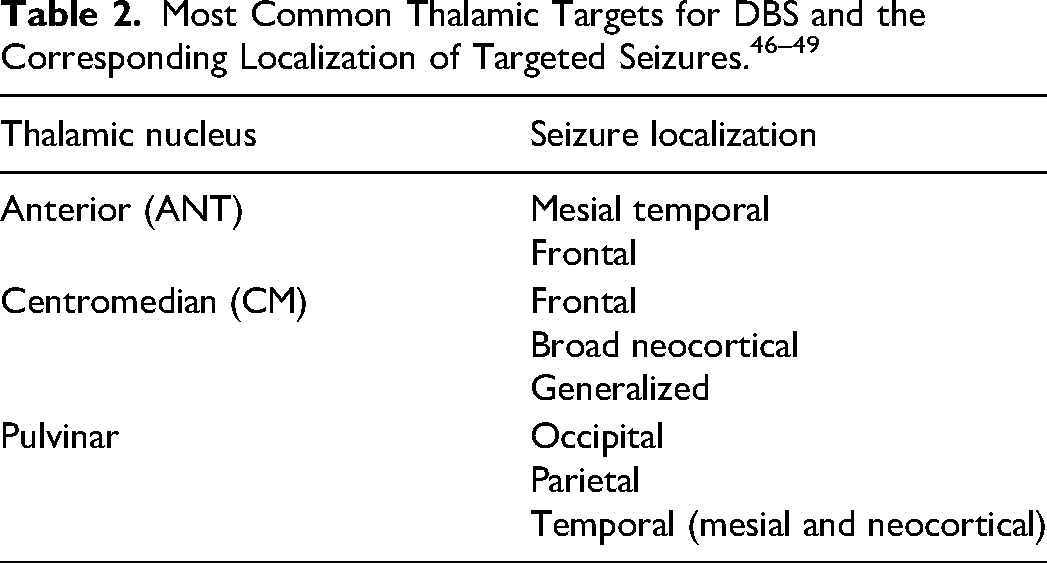
DBS-ANT is FDA-approved as adjunctive therapy in adults (≥18 years-old) with drug-resistant focal epilepsy. Through off-label use for pediatric epilepsy, DBS has been shown to be safe and effective in pediatric patients with DRE, regardless of epilepsy type or targeted thalamic nuclei, with responder rates varying from 60% to 75% in observational studies.46–49 The most common thalamic targets and corresponding epilepsy types based on thalamo-cortical connectivity are included in Table 2.
In young adults with Lennox-Gastaut Syndrome (LGS), class 1 evidence for centromedian DBS (DBS-CM) has shown 50%–59% relative risk in clinical and electrographic seizures, respectively. 50 In addition to seizure improvements, other benefits of DBS in children include improvements in quality of life and functional outcomes, such as increased school attendance.51,52 Long-term studies in adults demonstrate decreased SUDEP risk. 20 Surgical complications are low in children, comparable to adult populations, and stimulation is well tolerated. 53
Role of Responsive Neurostimulation
Although the RNS System is FDA-approved for adult drug-resistant focal epilepsy, its utilization in the pediatric population has expanded as an off-label therapeutic avenue for children as young as three years of age. The system operates on a dual-mechanism hypothesis: acutely delivering abortive stimulation to disrupt ictal patterns and chronically inducing long-term depression of network excitability to suppress cortical synchronization globally. Real-world preliminary experiences, with combined prospective and retrospective data, indicate that RNS is well tolerated in children, with efficacy profiles matching adult literature; approximately 65% of pediatric patients achieve a ≥50% reduction in seizure frequency over short-term follow-up.54,55
A significant evolution in pediatric neuromodulation is the application of corticothalamic and bi-thalamic stimulation to address multifocal or generalized epilepsies that are amenable to neither resection nor ablation. By targeting thalamic hubs, specifically the Anterior Nucleus (ANT) for limbic networks, the Centromedian (CM) nucleus for frontal/generalized networks, and the Pulvinar for posterior quadrant onsets, surgeons can modulate large-scale epileptic networks. Recent small single-center data regarding bilateral CM stimulation has demonstrated robust outcomes, with 60% of patients with LGS and 100% of patients with generalized epilepsy achieving ≥50% seizure reduction in retrospective review. 54 Notably, early intervention in these developmental epileptic encephalopathies may mitigate maladaptive network reorganization and subsequent cognitive regression. 55
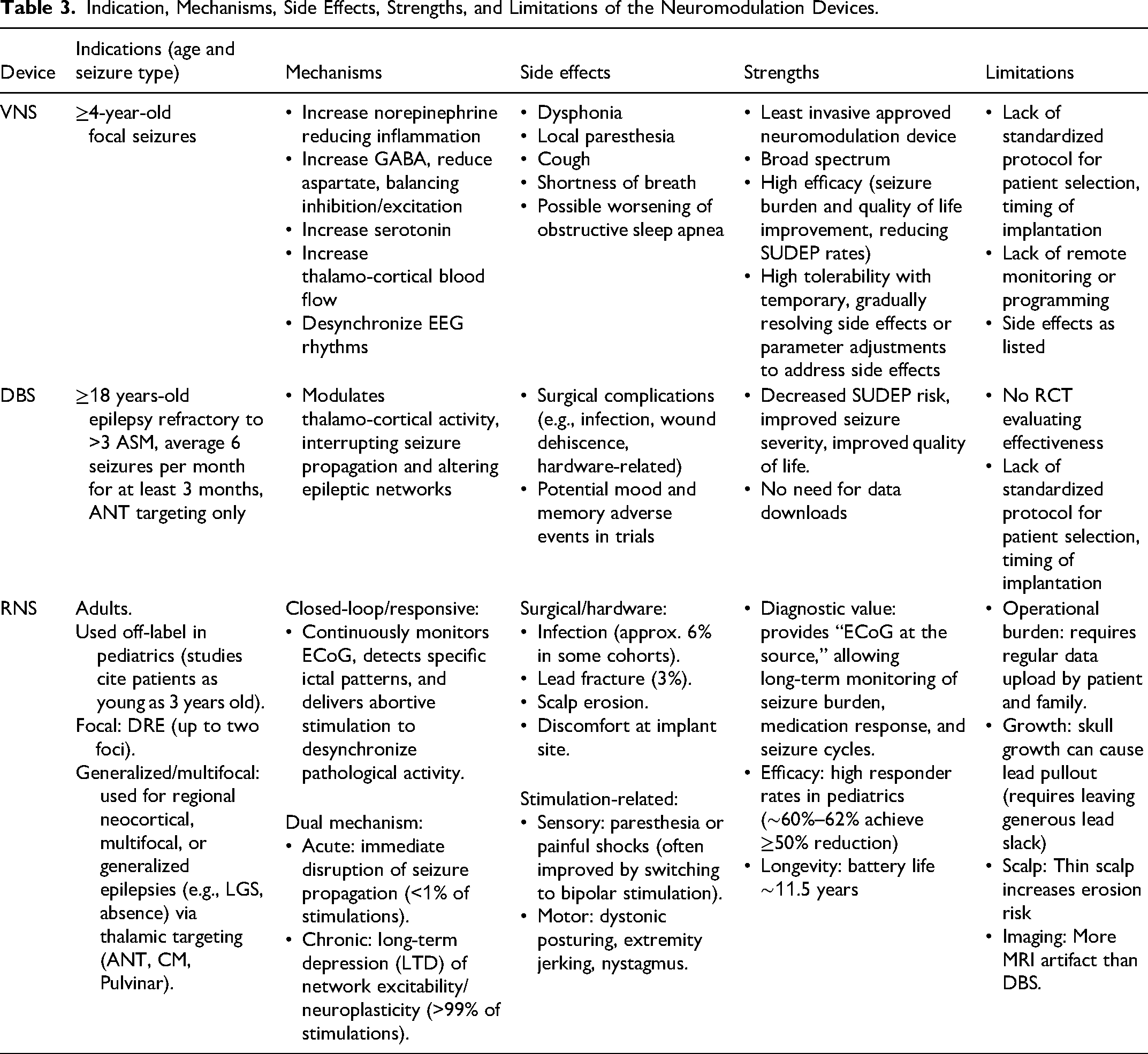
Surgical implantation in the pediatric cohort requires distinct technical modifications to address anatomical constraints. Adverse effects were predominantly associated with high charge density in monopolar-cathodal configurations and were largely resolved by adjusting stimulation parameters or transitioning to bipolar configurations. 56 Main characteristics of the neuromodulation devices described above are summarized in Table 3.
Indication, Mechanisms, Side Effects, Strengths, and Limitations of the Neuromodulation Devices.
Artificial Intelligence (AI) and Machine Learning for sEEG Seizure Detection, Localization, and to Predict Seizure Freedom
AI, particularly through graph-based deep learning frameworks, has the potential to significantly impact neuromodulation and epilepsy surgery by decoding complex neural network interactions that underline seizure generation and propagation. Graph Neural Networks (GNNs) model the intricate thalamo-cortical connectivity responsible for epileptic activity. Utilizing stereo electroencephalography (sEEG) to represent each electrode channel as a node and inter channel connectivity as weighted edges, GNN captures both spatial and temporal dependencies of brain dynamics. 57 Spatiotemporal GNNs models and dual task architectures integrate high resolution electrophysiological recordings with imaging modalities like MRI to attempt to predict surgical outcomes and localize seizure onset zones with high accuracy (> 90% in seizure wise validation). They may also reveal key biomarkers of poor outcomes, including excessive thalamo-cortical synchronization and dense network topologies at seizure onset. 58
Combining multimodal neuroimaging and electrophysiological data, AI is emerging as a potential tool capable of better identifying patients and cerebral targets for neuromodulation using precision neuronal network mapping.57,58
Global Perspectives: Epilepsy Surgery in Limited Resource Settings
Of the 65 million individuals worldwide with active epilepsy, close to 80% are in low-middle income countries (LMIC), where the burden is disproportionately higher. Yet, specialized treatment services remain scarce, and much of the population has no access to advanced diagnostics or surgical intervention.59–62
There is a large gap in access to epilepsy surgery, which is complex, resource-intensive, and dependent on advanced diagnostic tools such as video-EEG monitoring, MRI, PET, MEG in addition to neurosurgical tools which include navigation systems, microscopes, robotic systems, ablation systems, and neuromodulatory implants. In addition to technology, successful epilepsy surgery requires a coordinated multidisciplinary team including epileptologists, neurosurgeons, neurophysiologists, anesthesiologists, and specialized nursing support. These capacities are the exception in LMICs, where even basic EEG, cross sectional imaging, trained personnel, and infrastructure may be limited which reinforces global inequities in epilepsy outcomes. 60
Ukraine is discussed as a detailed example of how a middle-income country can progressively build epilepsy surgery capability. A bidirectional collaborative partnership between the Hospital for Sick Children in Toronto and multiple Ukrainian centers began in 2012, with the goal of expanding pediatric surgical and clinical expertise through hands-on observerships, clinical fellowships, and advisory training.63,64
More than 60 Ukrainian physicians and surgeons have travelled to Toronto for month-long observerships through this initiative, participating in clinical duties and integration of research into clinical activity. These experiences had previously been inaccessible in Ukraine. Conversely, Canadian specialists travel to Ukraine to provide clinical and surgical guidance in areas such as pediatric neurosurgery, neonatology, and neurology. 64
With ongoing efforts, they are achieving outcomes comparable to high-income countries in selected epilepsy disorders and moving toward advanced techniques such as sEEG and ablation. The Ukrainian model underscores the value of long term, stepwise capacity building supported by international collaboration. It demonstrates that meaningful progress toward specialized epilepsy surgery is possible even where initial resources are limited.65–68
Future of Neuromodulation: Emerging Technologies in Neuromodulation
Emerging noninvasive and minimally invasive neuromodulation management options are expanding in pediatric epilepsy, offering alternatives to pharmacologic, dietary, and current surgical approaches. Several novel stimulation modalities including transcranial magnetic stimulation (TMS), tDCS, noninvasive vagus nerve stimulation (nVNS), electroconvulsive therapy (ECT), focused ultrasound stimulation (FUS), and chronic subthreshold cortical stimulation (CSCS) are discussed below regarding current evidence, mechanisms, and limitations.
Role of the Cathodal Transcranial Direct Current Stimulation in Pediatric Epilepsy
Transcranial direct current stimulation (tDCS) is a noninvasive, safe, cost-effective, and easy to apply technique, that modulates cortical excitability through subthreshold membrane depolarization or hyperpolarization.69,70 The effects of a single 20–30-min session in humans can persist for up to 90 min. 71 This device remains investigational and is not yet approved by the FDA for clinical use.
The mechanism of tDCS is partially understood. Cathodal tDCs (c-tDCs) decrease the neuronal hyperexcitability associated with epilepsy. 72 The c-tDCs mechanisms include shifting neuronal membrane potential towards hyperpolarization, reducing synaptic transmission particularly mediated by N-methyl-D-aspartate receptors and potentially inducing long-term depression (LTD)-like effects with transmembrane protein migraine, cell migration of neurons and glial cells, and anti-inflammatory effects.72,73
Cathodal tDCS has been used in heterogeneous pediatric and adult clinical patients suffering focal refractory epilepsy such as Rasmussen Syndrome or Infantile Epileptic Spasms with promising results.72,74 Recent randomized clinical trials have demonstrated frequency seizure reduction of 40%–50%, with only minor, self-limited adverse effects.75–77
This emerging technique appears feasible for implementation in pediatric patients with limited resources and may serve as an adjunctive, home-based therapy. 78 Moreover, it carries the potential to enhance cognitive functions frequently compromised by epilepsy and its associated neuropsychiatric comorbidities. 79
Role of the Noninvasive VNS in Pediatric Epilepsy
Noninvasive VNS is represented by transcutaneous VNS, transcutaneous cervical VNS (tcVNS), percutaneous auricular VNS (paVNS), and transcutaneous auricular VNS (taVNS). These therapies target the afferent vagus nerve fibers beyond the nucleus of the solitary tract which integrates not only visceral but also somatic afferents. 80 These devices have shown responder rates (> 50% seizure reduction) ranging from 40% to 57% with safety profiles superior to implanted VNS. Adverse side effects were mostly headache, ear pain, and skin alteration and rated as mild to moderate. 81
A prospective pilot trial in 14 children with epilepsy demonstrated efficacy with seven of 13 children being responders and four of 13 children being seizure free after 4 months and persisting after 6 months of stimulation. Reduction of seizure frequency was significant compared to baseline after 4 and 6 months of stimulation (p < 0.05). Tolerability was generally good, two children experienced mild skin ulceration.82,83
Role of the Electroconvulsive Therapy
ECT, traditionally reserved for psychiatric conditions, has demonstrated efficacy in refractory status epilepticus as described in case reports, though relapse rates were high and standardized pediatric protocols are lacking.83,84
Role of the Focused Ultrasound Stimulation
FUS represents a preclinical modality capable of focal, nonthermal neuromodulation, with early human studies suggesting variable seizure outcomes but highlighting safety concerns including transient cognitive effects. Low intensity focused ultrasound (LIFU) can modulate neuronal activity and could be used to lower cortical neuronal hyper-excitability in epilepsy patients in a noninvasive manner.83,85
Role of the Chronic Subthreshold Cortical Stimulation
CSCS, an open-loop stimulation via subdural electrodes, targets the location of multifocal or eloquent seizure onset, has shown >90% responder rates and sustained seizure reduction in small cohorts, suggesting promise for multifocal epilepsies or for epileptogenic foci in eloquent cortex.83,86
Making the Neuromodulation Modality Decision in Pediatric Epilepsy
A patient with DRE, who is not a candidate for resection/ablation or disconnection, should be considered for neuromodulation. Typical examples are patients with generalized DRE, focal DRE with a nonlocalized epileptogenic zone, focal DRE with localized epileptogenic zone in an eloquent region, or focal DRE with two or more epileptogenic foci.87,88 At present, there is limited evidence comparing different modalities of neurostimulation to guide formation of a formal algorithm. A meta-analysis conducted in 2022 looked at 30 studies, only six of which were randomized controlled trials and none of which included head to head comparisons of different modalities. 89 When long-term outcomes data were pooled from all studies of each device the results overall suggested that RNS and DBS are more effective at decreasing seizure frequency than VNS. However, length of follow up was shorter in the VNS studies and patient selection varied.
Given the lack of direct comparison trials and difficulties in comparing studies of individual devices, at this time providers should approach consideration of neurostimulation with a patient and family-centered approach. Known potential risks and benefits for each device can be discussed in relation to an individual patient's presentation, keeping in mind specific epilepsy type, socio-economic and geographic factors, and comorbidities. For example, VNS requires the least amount of maintenance and is typically the lowest cost option with RNS currently requiring the most in-person programming and maintenance. For people living far from surgical epilepsy centers or have higher cost sharing insurance plans, these factors may weigh more heavily in the decision making process. Alternatively, VNS may also pose higher risk for irritation from the sensation of stimulation and/or device placement location for certain young people and also has less data regarding long-term seizure reduction. 87 For PWE who have a high burden of epilepsy and may have comorbidities such as autism with high sensory sensitivity, other modalities may be considered as a first option.
Because RCTs may be difficult or even impossible to conduct to directly compare these neuromodulation modalities, an emphasis should be placed on comprehensive registries, including outcome data, so that cohorts of similar patients can be more directly compared.
Conclusion
As demonstrated at the 2025 American Epilepsy Society Meeting the Pediatric State of the Art Symposium, neurostimulation is a viable, active treatment that should be considered early on in the pediatric population with DRE. It has real potential to make impactful changes on the burden of epilepsy. In addition to reducing seizure frequency and severity, these therapies have the potential to positively affect quality of life and cognition as these therapies improve seizures and allow for decreased medication burden and side effects. More data needs to be gathered to help guide clinician teams and families making timing and modality decisions regarding neurostimulation. Until then, providers should have an informed discussion regarding potential benefits and risks for each individual patient to help determine recommendations and the ultimate decision to move forward with a specific therapy.
Footnotes
Acknowledgments
We would like to recognize the effort and contribution of all the speaker at the 2025 American Epilepsy Society Meeting the Pediatric State of the Art Symposium as well as in the preparation of this manuscript which represent a summary of all the updated information presented.
Author Contributions Statement
Juan Toro Perez (co-first author) and Kathryn Lalor (co-first author) contributed equally with the organization of the 2025 American Epilepsy Society Meeting the Pediatric State of the Art Symposium, data collection, writing and final edition of manuscript. In addition, Juan Toro Perez wrote about the topic history of neuromodulation in epilepsy; and Kathryn Lalor wrote the topic neuromodulation modality decision in pediatric epilepsy and conclusion.
Inna Hughes contributed with the final edition of the manuscript.
Monika Jones contributed with the topic expectations of PWE and their families regarding neuromodulation.
Ahmed Abdelmoity contributed with choosing the appropriate device in children with DRE not amenable to surgical resection: Role of the Vagus Nerve stimulator (VNS) and building of ![]() .
.
Kimberly Houck contributed with choosing the appropriate device in children with DRE not amenable to surgical resection: Role of the Deep Brain Stimulator (DBS) and building of ![]() .
.
Aria Fallah contributed with choosing the appropriate device in children with DRE not amenable to surgical resection: Role of Responsive Neurostimulation (RNS) and building of ![]() .
.
Saadi Ghatan and Syed Anwar contributed with Artificial Intelligence (AI) and machine learning for sEEG seizure detection, localization, and to predict seizure freedom.
Eisha Christian contributed with Global perspectives: Epilepsy Surgery in Limited Resource Settings.
Daniel San Juan Orta and Shilpa Reddy contributed with future of neuromodulation: emerging technologies in neuromodulation.
Sarah Kelley contributed with the organization of the 2025 American Epilepsy Society Meeting the Pediatric State of the Art Symposium, selection of content and speakers, conclusions and the editing of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.