
Abstract
Because there are many effective treatments for epileptic seizures, there is a great need for optimal diagnostic and treatment pathways. We present national strategies to address gaps and health equity in patients with epileptic seizures, focusing on efforts in China and the USA. We outline the delay in diagnosis and treatment caused by the “treatment gap.” Efforts in China to address the “treatment gap” include the National Rural Epilepsy Management Project, the establishment of the national epilepsy quality control system, and standardized tertiary epilepsy center development. In the USA, Project Extension for Community Healthcare Outcomes (ECHO) epilepsy enables specialists to partner with primary care clinicians to deliver care. The National Association of Epilepsy Centers facilitates care and contributes to the standardization of presurgical epilepsy evaluation. A major recent and ongoing development is the Epilepsy National Plan in the USA, coordinated through the American Epilepsy Society (AES) with 120 epilepsy-related organizations, to advance a comprehensive national plan that reflects the needs of the entire epilepsy community.
Introduction
Despite many effective treatments, many epilepsy patients have prolonged delays in both diagnosis and treatment. We present national strategies to address gaps and health equity, focusing on efforts in China and the USA.
The “treatment gap”
The “treatment gap” (the difference between people with active epilepsy and people who receive appropriate treatment) in epileptic seizures presents challenges on several levels. Establishing diagnosis, access to healthcare, and treatment are all major factors that contribute to the “treatment gap.”
Delay in diagnosis of epileptic seizures often delays initiation of appropriate treatment, especially when presentation is with nondistruptive, 1 nonconvulsive, or nonmotor seizures. 2 In the Human Epilepsy Project, including 34 sites in the USA, Canada, Europe, and Australia, an analysis involving 447 participants compared subjects with focal nonmotor or focal with motor involvement for time to diagnosis and prediagnostic injuries, including motor vehicle accidents (MVAs). The median time for diagnosis for patients with focal epilepsy was 219 days. Diagnosis from the first seizure was 10 times longer in patients with nonmotor seizures compared to motor seizures at onset. For MVAs, 82.6% occurred in patients with undiagnosed nonmotor seizures.
Access to care plays a role in the “treatment gap.” Past studies document that limited access to health care and a lack of public education about epilepsy limits diagnosis and treatment of epilepsy, especially in less socioeconomically developed regions. Approximately 2.4% of people in eastern China have active epilepsy, with approximately half of them receiving inappropriate treatment or no treatment at all, with no health insurance as a significant factor in the lack of appropriate treatment. 3 In a “first world” urban environment with the availability of free basic medical care (Melbourne, Australia), socioeconomic factors are also associated with delay to presentation. 1
Patients may experience treatment delays after the diagnosis of epilepsy. Using standardized diagnosis codes (ICD-9-CM) as a primary diagnosis definition, a study including 59,970 patients found 36.7% remained untreated up to 3 years after diagnosis of an initial seizure. 4 A more stringent definition, including cases with more follow-up visits after diagnosis, showed 4% were untreated within 3 years. The study illustrates the importance of prioritizing the epilepsy diagnosis, communicating with patients about the diagnosis and its implications, and addressing barriers to treatment.
Studies on the “treatment gap” illustrate the need for strategies to bridge gaps and advance health equity.
The World Health Organization (WHO) Intersectoral Global Action Plan (IGAP)
In November 2020, WHO member states passed a resolution to create and implement a global action plan on epilepsy. 5 IGAP has 90–80–70 targets by 2031, with goals of 90% of people with epilepsy (PWE) becoming aware of their condition as a treatable brain disorder, 80% of diagnosed individuals with access to safe, effective, and affordable antiseizure medicines, through sustainable supply chains, financing reforms, and regulatory support, and 70% of treated individuals achieving sustained seizure control. Efforts in China and the USA strive to obtain IGAP goals.
China's National Rural Epilepsy Management Project: A Model of Integrated Governance
Despite advancements in tertiary epilepsy care, healthcare in China remains imbalanced, with uneven distribution of scarce medical resources. There is a significant treatment gap in the over 10 million PWE. 6 Prior to the launch of the China Rural Epilepsy Management Project (CREMP), epidemiology surveys revealed that over 60% of PWE in rural regions never received appropriate treatment.7,8 This situation positioned China as an epitome of the global epilepsy governance challenge.
The WHO/International League Against Epilepsy/International Bureau of Epilepsy Global Campaign Against Epilepsy laid the foundation for a national solution in China with a demonstration project from 2000 to 2004, 9 providing a practical and effective strategy for resource-limited settings. Building on these lessons, China officially launched CREMP in 2005, scaling a successful pilot into a sustainable national program.
CREMP established an integrated, national operational model for epilepsy management in resource-limited rural areas. 10 Sustained investment from the National Health Commission formed the program's bedrock, ensuring consistent funding and top-down administrative support. By leveraging the existing public health infrastructure, funding enabled primary care practitioners at the county and township levels to screen and treat PWE during routine clinical visits, providing free phenobarbital and valproate according to standardized protocols. Specialist physicians from tertiary centers provided crucial professional empowerment through direct training and supervision of primary care providers (PCPs), reinforced by regular on-site visits. This system empowered township health workers to perform frontline duties—including screening, follow-up, and management of common side effects—ensuring the direct delivery of free antiseizure medication and continuous care within patients’ communities. 11
This integrated model has yielded substantial and verifiable impacts on a national scale. By 2021, CREMP achieved full nationwide coverage, operating in 310 counties across all 32 provincial-level regions. The program screened over 300,000 individuals and provided long-term follow-up for 66,607 patients with convulsive epilepsy, demonstrating remarkable sustainability with a median follow-up of 63.6 months. 12 Data from 63,223 patients demonstrated that after 6 months of management, 54% (N = 34,148) achieved seizure freedom, and the overall treatment response rate (≥50% seizure reduction) reached 70.5%. This clinical success was matched by an outstanding safety profile; over 2 decades of operation, only 0.45% of patients reported moderate adverse reactions and 0.08% reported severe reactions, with no mortality directly attributed to drug management. 13
CREMP also generated profound socioeconomic benefits. 14 The program addressed the human resource gap by cumulatively training 23,892 primary care doctors through an average of 89 specialized training sessions annually, establishing a permanent epilepsy care network in rural China. It also improved critical social outcomes: during the project's peak implementation, baseline school dropout rates among pediatric PWE fell from 20.81% to 17.24%, and unemployment rates among PWE dropped from 11.62% to 9.78%. Furthermore, over 56% of patients across all baseline seizure-frequency groups reported improved quality of life, with only about 2.3% experiencing deterioration.
The CREMP model demonstrates that the epilepsy management goals in resource-limited settings were achievable. Aligned with the objectives of IGAP, it provides a replicable operational guide to improve epilepsy and other neurological diseases care. This project was adapted for urban communities in China. While it aimed to guarantee fundamental epilepsy care access, the next critical step was to ensure the quality and standardization of epilepsy services across the entire healthcare system.
Establishment of the National Epilepsy Quality Control System in China
To implement the “Healthy China 2030” initiative in epilepsy care, it was imperative to ensure not only nationwide access but also homogenized, standardized care quality for all PWE. In response, the National Health Commission, through the National Center for Quality Control of Nervous System Diseases, mandated a comprehensive epilepsy quality control system in 2017. This system, aligned with international standards yet tailored to China's context, is obligatory for all secondary and tertiary hospitals.
This system employs a dual-track national surveillance approach. “Cold Tracking” utilizes the national Hospital Quality Monitoring System to automatically extract and monitor epilepsy case data from medical records across the country. This is complemented by “Hot Tracking,” which involves active, real-time data reporting from a network of sentinel hospitals and a specialized epilepsy database across all 31 provincial-level regions. This combination enables comprehensive, longitudinal assessment of national epilepsy care quality, pinpointing areas for improvement to systematically reduce the “treatment gap.”
The measurement kit consists of 10 key epilepsy indicators, including 6 medical and 4 surgical indicators: these indicators comprehensively cover treatment, setting a measurable standard for every level of healthcare institution. 15 The care quality indicators are as the followings: (1) recording rate of seizure type and frequency; (2) regularity rate of anti-seizure medications (ASMs) in people with uncontrolled seizure; (3) epilepsy etiology screening rate; (4) screening rate for psychiatric or behavioral comorbidities; (5) counseling rate for women with epilepsy of childbearing potential; and (6) serious adverse event rate by ASMs.
Figure 1 compares the epilepsy internal medicine quality data over 4 years from 2019 to 2022.16,17 A total of 17,144 PWE were investigated. Clearly, there was improvement in providing pregnancy health education for women with epilepsy of childbearing age and screening/management of psychiatric and behavioral comorbidities. Meanwhile, indicators such as the recording rate of epilepsy seizure frequency, the completion rate of etiological examinations for epilepsy, and the standardized medication adherence rate for ASMs maintained a high completion rate.
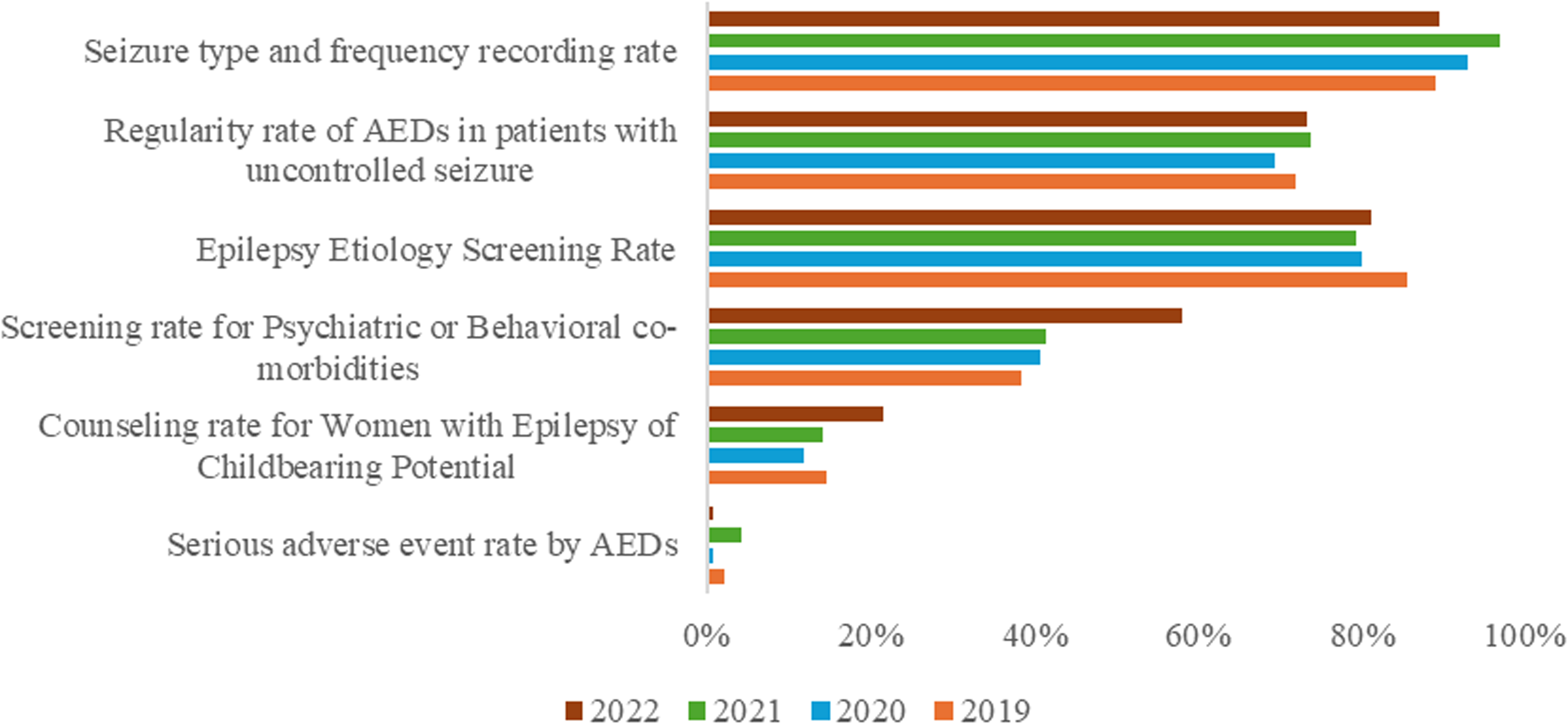
The implementation of the Chinese national quality indicators for epilepsy medical treatment. Among 17,144 people with epilepsy, there was a clear improvement in providing pregnancy health education for women with epilepsy of childbearing age and screening/management of psychiatric and behavioral comorbidities. Other indicators, such as the recording rate of epilepsy seizure frequency, the completion rate of etiological examinations for epilepsy, and the standardized medication adherence rate for anti-seizure medications (ASMs), maintained a high completion rate.
After the stable operation of medical quality control indicators for epilepsy internal medicine for nearly 2 years, 4 surgical indicators were launched at the end of 2018: (1) in-hospital mortality rate of elective surgery for epilepsy patients; (2) rate of postoperative complications in epilepsy patients; (3) rate of definite postoperative pathological diagnosis in epilepsy patients; and (4) rate of continued ASMs after discharge.
Figure 2 presents the surgical indicators over 4 years from 2019 to 2022, showing a total of 1124 PWE who underwent surgical treatment. The indicators show that surgical complications remain relatively common, while most patients can obtain a definite pathological diagnosis and continue to receive antiseizure drug treatment after discharge.
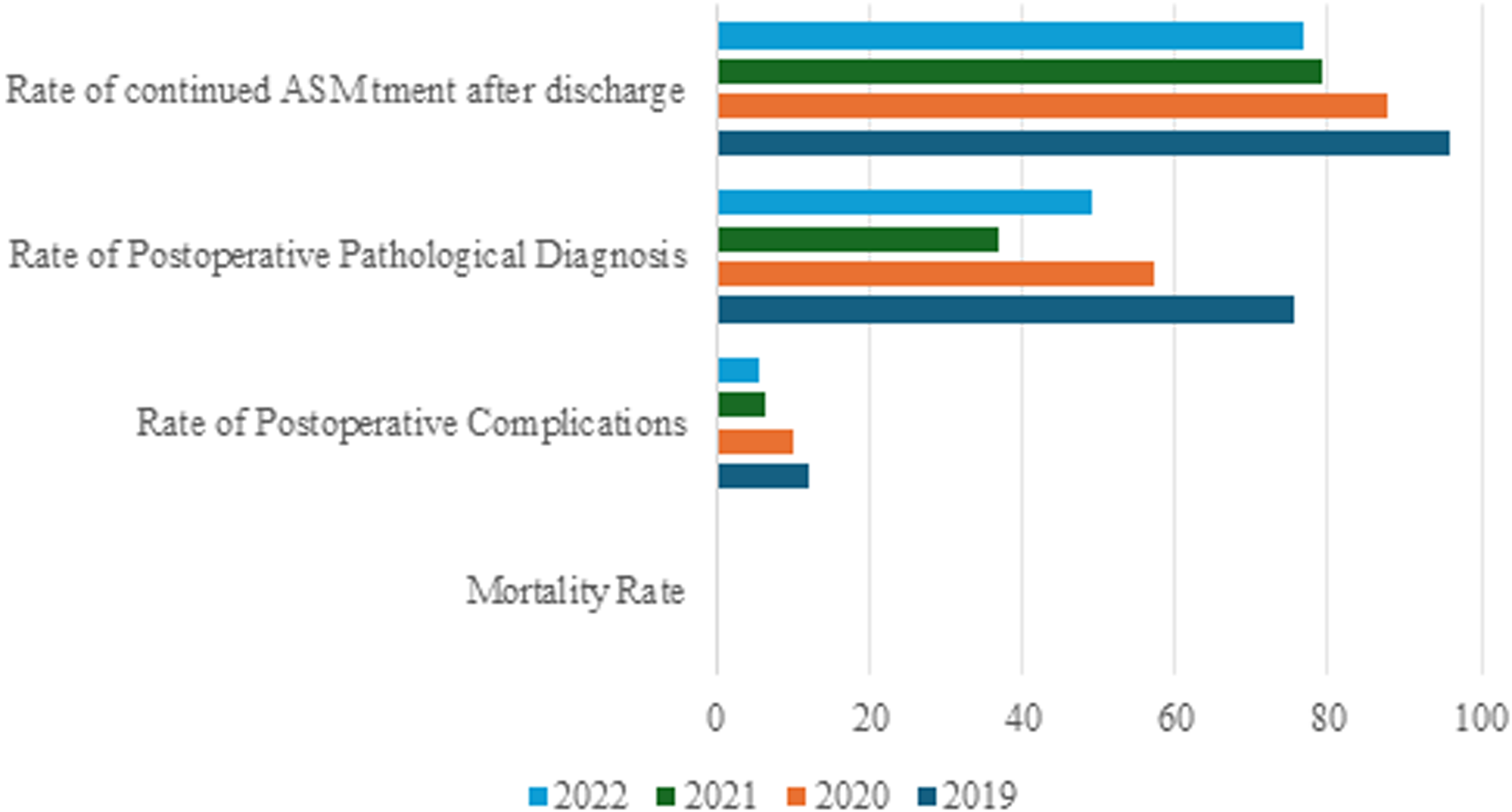
The implementation of the Chinese national quality indicators for epilepsy surgery. The figure presents the surgical indicators over 4 years from 2019 to 2022, showing a total of 1124 people with epilepsy who underwent surgical treatment. The indicators show that surgical complications remain relatively common, while most patients can obtain a definite pathological diagnosis. The rate of anti-seizure medication (ASM) continuation after discharge shows an increasing percentage.
Standardized Tertiary Epilepsy Center Development in China
Complementing the government-led quality control system, the professional community launched a parallel initiative to elevate specialized epilepsy care. Spearheaded by the China Association Against Epilepsy (CAAE), this program was designed as a profession-driven effort to systematically build expertise and address critical gaps. This monumental reform was forged in response to a critical need uncovered by a foundational 2016 national survey, 18 which revealed severe systemic gaps: a scarcity of trained professionals, a lack of primary-care institutions, and surgical volumes far below the actual need. The strategic response was not merely to establish individual centers, but to build an integrated, 3-tiered national network from the ground up.
The journey began with foundational work in 2013, culminating in the pivotal publication of China's Epilepsy Center Grading Standards in 2017–2018. 19 This framework created a clear classification system: Tertiary Comprehensive Epilepsy Centers for complex care and surgery; Secondary Centers for advanced medical management and referral; and Primary Service Facilities for essential diagnosis and treatment at the grassroots level. The implementation of this structure is supported by 4 robust pillars: a rigorous, multistage accreditation process ensuring quality control; a tiered education and training system that has expanded the specialized workforce by up to 40-fold since 2019; mechanisms for collaboration through case discussions and a national Remote Consultation Platform to bridge regional disparities; and active international exchange to integrate global best practices.
The outcomes of this systematic, decade-long effort are transformative. From a single center in the 1990s, China has now accredited a remarkable 578 epilepsy centers, creating a truly collaborative national network. This expansion is underpinned by phenomenal growth in specialized human resources and clinical capacity. By 2024, key service metrics, including outpatient visits, long-term electroencephalogram (EEG) monitoring, neuropsychological assessments, ketogenic diet therapies, and inpatient admissions, have increased by 9 to 33 times. Surgical capabilities have advanced significantly, with growing volumes and an evolving procedural mix indicating greater maturity. For geographical coverage, disparities remain, with 9 provinces still lacking a top-tier center, illustrating the need for future expansion and equity.
Looking forward, the strategic vision is clearly defined by the principles of standardization, collaboration, development, and advancement. Future efforts will focus on continuously enhancing the certification process, empowering tertiary centers to lead grassroots development, deepening research, and strengthening global partnerships. Guided by the core mission of building a high-quality, accessible, and efficient care system, CAAE is committed to providing effective solutions for China and meaningfully contributing to the global fight against epilepsy. This journey from a fragmented landscape to a standardized, collaborative network offers a model for health system strengthening worldwide. 20
As a coordinated national action aligned with IGAP objectives, the 3 Chinese approaches offer valuable experiential evidence and a potential replicable framework for global epilepsy governance.
Project Extension for Community Healthcare Outcomes (ECHO) in North America
Project ECHO provides an important avenue for addressing the “treatment gap” by enabling specialists to partner with primary care clinicians in underserved areas to deliver complex specialty care to patients. 21 Typical Project ECHO models include a TeleECHO clinic comprising an expert hub team. The TeleECHO team supports community-based primary care teams for training and facilitating care, better enabling primary care teams to reach patients with specialty knowledge and expertise. There are several programs implementing ECHO for patients with epilepsy.
The University of Cincinnati implements a successful Project ECHO Epilepsy/Neurology program for educating PCPs about epilepsy treatment. They combine epilepsy and other neurology topics for regular educational programs, which attract more interest among PCPs. Most participants report greater interest in caring for, as well as greater comfort in treating, patients with neurological disorders. The program improves PCP knowledge and confidence in managing issues on a primary care level, and at the same time identifies those patients who need a referral to a specialist. 21
ECHO Ontario: Epilepsy across the lifespan interdisciplinary teams are based in 10 sites across Ontario, Canada. Each team includes an epileptologist, nurse practitioner, pharmacist, social worker, neuropsychologist, and community agency representative connected with the provinces regional Comprehensive Epilepsy Programs. 22 Using the Project ECHO model, The Epilepsy Foundation of America provides an e-learning platform with the program “The (Not So Rare) Epilepsies Series: Bridging Genetic Diagnosis with Complex Care,” providing 6 sessions covering aspects of diagnosis, treatment, and management of patients with rare epilepsies. 23
Standardization of Presurgical Epilepsy Evaluation in the USA: Progress and Future Direction
For many individuals with drug-resistant epilepsy (DRE), epilepsy surgery offers the greatest opportunity for achieving seizure freedom. However, surgical treatment remains significantly underutilized. 24 Between 1990 and 2008, high-volume epilepsy centers – defined as those performing more than 15 lobectomies annually – experienced a marked decline in the total number of lobectomies performed. 25 Improving both access to and standardization of presurgical evaluation for DRE is therefore essential: it promotes consistency of care across centers, validates appropriate patient selection, expands access to surgical therapies, and enables the development of meaningful national quality metrics and benchmarking.
The movement toward a harmonized diagnostic pipeline in the United States began in the early 1990s, evolving from highly heterogeneous, center-specific practices to the more structured framework in place today. A pivotal milestone was the establishment of the National Association of Epilepsy Centers standards, including explicit criteria for Level 3 and Level 4 comprehensive epilepsy centers. These accreditation requirements mandate defined capabilities—such as expertise in video-EEG monitoring, epilepsy-specific magnetic resonance imaging (MRI) protocols, and advanced functional imaging (positron emission tomography (PET), single-photon emission computed tomography (SPECT), and magnetoencephalography (MEG))—as well as multidisciplinary case review, thereby establishing a baseline level of uniformity and care nationwide.
The cornerstone of the presurgical evaluation is the Phase I workup, aimed at noninvasively identifying the seizure-onset zone. This comprehensive assessment includes detailed seizure semiology, a thorough clinical history, and a high-resolution MRI performed with epilepsy-specific protocols. Prolonged video-EEG monitoring remains indispensable. Functional studies such as interictal PET, ictal SPECT, and MEG are applied judiciously, particularly when MRI findings are nonlocalizing. A comprehensive cognitive and psychological evaluation—required for all surgical candidates—is an essential component of this phase. All findings are subsequently synthesized and reviewed during a multidisciplinary Epilepsy Surgery Conference. If noninvasive data remain discordant or insufficient, the evaluation proceeds to Phase II invasive monitoring.
Over the past decade, a substantial consensus has emerged. There are now routine, standardized MRI protocols and neuropsychological testing performed by epilepsy-trained specialists. Multidisciplinary case conferences ensure that treatment decisions benefit from diverse expertise. PET and SPECT are now commonly used for MRI-negative cases, while functional MRI has largely supplanted the Wada test for language and memory lateralization. Technological advances have further transformed the field: stereoelectroencephalography has largely replaced subdural grids; machine learning approaches are increasingly used for seizure localization; automated MRI postprocessing is improving detection of subtle abnormalities; and network-based connectomic analyses are enabling a more holistic understanding of the epileptogenic zone. These innovations are paralleled by expanded use of minimally invasive surgical approaches, including Laser Interstitial Thermal Therapy and resections guided by Responsive Neurostimulation data.
Despite this progress, challenges remain. Notable issues include variability in standards between Level 3 and Level 4 centers and inconsistent access to advanced diagnostic tools, among others. Although both MEG 26 and 7-Tesla MRI 27 have demonstrated value in refining presurgical hypotheses, they are available at only a minority of U.S. epilepsy centers—for example, MEG is available at just 17% of centers. 28
Looking ahead, the field is moving toward a fully standardized national pathway, leveraging the development of large-scale datasets, predictive modeling of seizure freedom, and automated algorithms for seizure-onset zone localization. Innovative therapeutic strategies will also be essential as the field shifts from targeting a single epileptogenic focus to addressing the broader pathological seizure network. 29 By continually refining the foundations of presurgical evaluation and embracing emerging technologies, the effectiveness, reach, and impact of curative epilepsy surgery can continue to expand.
The Epilepsy National Plan in the USA
The United States has national plans for many neurological disorders (including Alzheimer's, Parkinson’s, Amyotrophic Lateral Sclerosis, Multiple Sclerosis, and Autism), but not for epilepsy (<0.5% of National Institutes of Health funding goes to epilepsy). There is a need for a national plan on multiple levels, including people and caregivers living with epilepsy, researchers and clinicians, and the economy. 30
In July 2024, the American Epilepsy Society (AES), joining with more than 120 epilepsy-related organizations, initiated a National Plan for Epilepsy. Goals include advocacy to advance a comprehensive national plan that reflects the needs of the entire epilepsy community. Efforts include defining objectives for improving health outcomes, fostering research and innovation for treatments, and increasing access to care and public awareness. Accomplishments thus far include the National Plan for Epilepsy Act (H.R. 1189), which was reintroduced to Congress by the Congressional Epilepsy Caucus. Next steps include the formulation of strategies from the involved stakeholders.
Conclusion
Despite the many advances in the diagnosis and treatment of epilepsy, challenges remain in addressing the “treatment gap.” Because of the many viable medical and surgical treatment options, there is a critical need for national strategies to bridge gaps and achieve health equity in epilepsy care. We demonstrate achievements, as well as future goals in addressing epilepsy on a national level in both China and the USA, emphasizing the need for ongoing diligence in providing optimal care for patients with epilepsy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.