
Abstract
Epilepsy-related mortality, including Sudden Unexpected Death in Epilepsy and suicide, is a crucial topic within the interdisciplinary scope of caring for people with epilepsy (PWE). This review highlights best practices that emphasize proactive education for patients, caregivers, and communities, as well as evidence-based strategies and interventions for seizure management aimed at reducing mortality risk. It further underscores the essential contribution of the multidisciplinary care team in managing epilepsy-related mortality, highlighting considerations such as comorbid behavioral health conditions, challenges with treatment adherence, the use of the ketogenic diet, and the impact of social determinants of health and health disparities on historically marginalized populations. The authors provide actionable insights to address these challenges and barriers and enhance the outcomes and quality of life for PWE and their loved ones.
Keywords
Introduction
Epilepsy-related mortality remains an inadequately discussed yet critical component of comprehensive epilepsy care. 1 Topics such as Sudden Unexpected Death in Epilepsy (SUDEP), suicide risk, and seizure-related injuries can be uncomfortable or difficult for healthcare professionals, people with epilepsy (PWE), and caregivers to discuss.2,3 However, addressing them directly is essential to reduce preventable harm, improve clinical outcomes, and enhance quality of life for PWE.4,5 This is particularly important as PWE and their families have endorsed a desire to know about their condition, including related to mortality risk and SUDEP.2,5,6 Mortality risk in PWE is shaped not only by neurological and behavioral health factors, but also by broader health disparities and social determinants of health (SDOH), such as socioeconomic status, cultural and spiritual factors, access to specialty care, health literacy, among others.1,7
Given the complexity of these intersecting influences, multidisciplinary care teams play an indispensable role in identifying, mitigating, and communicating mortality risks for PWE. Education for PWE, their caregivers, and the community needs to be centered on effective seizure management, safety, and support for comorbidities such as behavioral health and psychosocial needs. Despite general understanding around the importance of epilepsy-related mortality, significant gaps remain in knowledge, communication, and access to appropriate resources for many patients, caregivers, and the community.
This review offers insights regarding barriers to managing epilepsy-related mortality risk as well population SDOH considerations, strategies, and resources for multidisciplinary healthcare teams to improve care for PWE. Pediatric and adult practitioners representing roles including doctors, advanced practice providers, social workers, dieticians, and neuropsychologists lend their expertise and explore topics including health disparities and SDOH considerations, proactive screening, education and engagement, navigating difficult conversations, the role of the ketogenic diet, and adherence considerations.
Health Disparities in the Prevention of Epilepsy-Related Mortality
PWE experience a higher risk of premature mortality than the general population. This increased mortality is mostly related to potentially preventable factors, including uncontrolled seizures, medication non-adherence, and gaps in safety education. 8
Epilepsy-related mortality can be classified into four types: 1) direct: SUDEP, status epilepticus, or seizure-related accidents; 2) acute symptomatic: directly related to acute injury, infection, or insult such as, brain injuries; 3) indirect: complications such as pneumonia, suicide, cardiovascular disease; 4) due to underlying neurological disease and conditions: such as tumors and stroke. 1
Health disparities are measurable differences in health outcomes that stem from SDOH. 9 SDOH is defined by the World Health Organization (WHO) as the social, economic, and environmental conditions in which people are born, live, work, and age. Globally, epilepsy affects more than 50 million people, and PWE experience a mortality rate two to three times higher than that of the general population, 10 highlighting epilepsy as both a neurological disorder and a major public health concern. However, this excess in epilepsy-related mortality is not evenly distributed. Factors such as poverty, low educational attainment, unstable housing, limited health literacy, geographic isolation, lack of health insurance, and minority group status significantly shape access to diagnosis, evidence-based treatment, antiseizure medications, specialty epilepsy care, and safety counseling. Even within well-resourced health systems, racial and ethnic minority groups and individuals of lower socioeconomic status continue to experience delayed diagnosis, reduced access to epilepsy specialists and surgical evaluation, poorer medication adherence, and higher mortality risk. 1 As a result, marginalized populations face a disproportionately higher risk of preventable epilepsy-related deaths.
From a global health lens, these inequities are especially pronounced in low- and middle-income countries, where treatment gaps remain large and where accidents, drowning, burns, and untreated seizures are among the leading causes of death. However, in high-income countries, indirect causes such as cardiovascular disease, malignancy, and suicide contribute more substantially. 7
Addressing epilepsy-related mortality, therefore, requires interventions that extend beyond individual-level medical management to confront the upstream social and structural drivers of risk. Adapted public health frameworks grounded in the WHO SDOH model 11 emphasize the need for coordinated, multisector strategies that strengthen health systems, reduce financial and geographic barriers, expand education and community capacity, and improve continuity of care across the lifespan. In parallel, professional society-led initiatives such as the American Epilepsy Society (AES) and International League Against Epilepsy North America Task Force articulate principles for equity-driven epilepsy care, emphasizing patient-centeredness, cultural responsiveness, workforce training, data-driven quality improvement, and advocacy to reduce persistent gaps in outcomes. 12 Together, these frameworks shift the focus from isolated clinical risk toward systemic accountability and population-level impact. Practical resources aligned with these models further support implementation in real-world settings, including the Partners Against Mortality in Epilepsy Clinician Toolkit for SUDEP risk screening and patient education, the Managing Epilepsy Well Network (MEW) for community-based self-management programs, and culturally sensitive patient and provider resources from the Epilepsy Foundation. Collectively, these tools operationalize equity-focused strategies by empowering clinicians, PWE, families, and communities with actionable knowledge, safety planning, and supportive services.
Taken together, epilepsy-related mortality remains unacceptably high, and a substantial proportion of these deaths are preventable. Growing evidence demonstrates that meaningful reductions in mortality depend on addressing the social and structural conditions that shape risk. Integrating clinical care with community resources, public health infrastructure, and policy-level interventions is essential to narrowing disparities, improving survival, and advancing health equity for PWE.
Patient, Caregiver, and Community Education and Engagement
Patient, caregiver, and community education are foundational components of strategies aimed at reducing epilepsy-related mortality, particularly SUDEP. SUDEP remains a leading cause of death among PWE and occurs across the epilepsy spectrum, including in individuals considered to be at relatively lower risk. 13 Despite growing professional awareness, knowledge among patients and caregivers remains limited, and many families report learning about SUDEP only after a fatal event. 14 Early, transparent, and proactive education on epilepsy-related mortality is needed and beneficial for PWE and their caregivers. Clinical guidelines from the American Academy of Neurology and the AES advocate for routine SUDEP counseling as a component of comprehensive epilepsy care. 13 However, many child neurologists report hesitance in discussing SUDEP due to time constraints or discomfort with the topic. 15 Framing epilepsy-related mortality education as a longitudinal, integrated component of routine epilepsy management, rather than a single disclosure, may increase healthcare professionals’ confidence and support more consistent, patient-centered communication.
Effective education begins with individualized seizure risk assessment that considers seizure type and frequency, nocturnal seizures, antiseizure medication adherence, comorbidities, and psychosocial context. Advanced practitioners play a vital role in this process, particularly in a pediatric setting. Tailoring discussions to a patient's clinical profile and caregiver concerns allows healthcare professionals to address modifiable risk factors without provoking undue alarm. Clear, nontechnical language and developmentally appropriate framing are essential, as is ensuring that written and verbal materials are accessible in patients’ and caregivers’ preferred languages. Such approaches support comprehension, adherence, and shared decision-making.
Seizure action plan (SAP) is an important tool for PWE and their caregivers (https://www.epilepsy.com/preparedness-safety/action-plans). Personalized SAPs outline seizure recognition, first aid, rescue medication use, and criteria for seeking emergency care, thereby empowering caregivers and community members to respond confidently and consistently. Education on rescue therapies, including indications, routes of administration (rectal, oral, or intranasal), and safety considerations, is a critical component of mortality risk reduction. 16 Extending SAP implementation to schools, workplaces, and other community settings further promotes continuity of care and supports medical and educational accommodations for children, youth, and adults with epilepsy.
Patient and caregiver education must also be understood within a broader framework of SDOH. Barriers related to insurance coverage, medication access, health literacy, and care fragmentation can exacerbate seizure burden and increase mortality risk. Coordinated care that includes collaboration with primary care providers, use of safety-net pharmacy programs, and shared communication across care teams can mitigate these challenges. Addressing SDOH alongside clinical education reinforces that SUDEP prevention is not solely a medical issue but one that is shaped by structural and social contexts.
Overall, patient, caregiver, and community-centered education represent a critical, modifiable intervention for reducing epilepsy-related mortality. Individualized, culturally sensitive education integrated with SAP, community collaboration, and attention to SDOH impacts enables meaningful conversations on epilepsy-related mortality to be integrated into routine practice.
Suicide Risk Assessment, Coping Support, and Difficult Conversations
In addition to advanced practitioners, social workers are integral members of the care team and can play a key role in conducting suicide risk assessments, providing coping and psychosocial support, and facilitating difficult conversations with PWE and their caregivers. Suicide risk assessment is a key aspect of caring for PWE. PWE experience significantly higher rates of psychiatric comorbidities compared to the general population, including ADHD, anxiety, autism spectrum disorder, psychosis, depression, and suicidal ideation. 17 Although epilepsy affects about 1-1.2% of the population, mood disorders occur in 25%-50% of individuals with epilepsy, with depression alone reported in 23%-50%. 17 Contributing factors include antiepileptic drugs, lifestyle stressors, seizure activity—particularly from the temporal lobe—and a bidirectional relationship between epilepsy and depression. Psychosocial and biological influences such as stigma, social restrictions, altered brain networks, and treatment effects also play roles.17,18 While having a mood disorder does not guarantee suicidal ideation, PWE show elevated rates of suicide attempts. Key risk factors include family history, health burdens, severe anxiety, life stress, access to lethal means, drug-resistant epilepsy, frequent seizures, and the period following diagnosis.19,20
The National Institute of Mental Health has developed evidence-based tools for suicide risk assessment, specifically the Ask Suicide-Screening Questions (ASQ) and the Brief Suicide Safety Assessment (BSSA). The ASQ is the first step in a three-tiered clinical pathway and consists of four yes/no questions, with a follow-up question if needed. The screen takes about 20 seconds and is designed to quickly identify individuals who may be at risk. If a person answers “yes” to any question, the clinician proceeds to the BSSA. The BSSA takes approximately 10 minutes and provides a deeper evaluation of the patient's current emotional state, protective factors, and overall suicide risk. It assesses the frequency, intensity, and duration of suicidal thoughts, the presence of a plan, access to lethal means, past suicide attempts or self-harm, mental health comorbidities, current stressors, and available social supports. 21
Based on the assessment, clinicians categorize risk as low, intermediate, or imminent. Low-risk individuals receive follow-up care, crisis resources, and a collaborative safety plan. Moderate-risk individuals require evaluation by a mental health specialist, safety planning, and lethal-means counseling. Imminent-risk individuals need immediate emergency psychiatric evaluation, constant monitoring, and removal of access to lethal means. Safety plans highlight personalized coping strategies, warning signs, supportive contacts, and crisis resources. 21
It is critical to identify protective factors and support resources for PWE and their caregivers to improve mental health and prevent crises. Both general and epilepsy-specific supports can be helpful, including national and local Epilepsy Foundation programs, psychotherapy, psychiatry, and social workers in medical and school settings. Additional coping resources include caregiver, sibling, and PWE support groups, faith-based communities, peer-matching programs, and self-management programs such as MEW and Home-Based Self-Management and Cognitive Training Changes Lives (HOBSCOTCH) Program. Legal aid, disability rights groups, educational advocacy, emotional support animals, safety plans, and suicide hotlines also contribute to resilience and improved quality of life.
Discussions between providers and PWE and their caregivers regarding mortality risk are often difficult, and all parties may experience certain barriers that impede meaningful engagement in these important conversations. Providers may hesitate to discuss suicide risk when a patient appears well or has not disclosed suicidal ideation, and time constraints during appointments make thorough assessments difficult. Some clinicians feel suicide screening or discussing SUDEP is outside their role, while others lack confidence in responding to positive screens. Discomfort with emotionally heavy topics also contributes to avoidance. 22 For PWE, additional barriers include shame, fear, stigma, trauma histories, power imbalances, and cultural norms that discourage vulnerability. 23 To overcome these challenges, providers must develop comfort and skill in navigating difficult conversations. Key competencies include cultural humility and cultural competence, motivational interviewing, active listening, empathic and nonjudgmental inquiry, asset-based approaches that highlight strengths, and trauma-informed communication. These skills help create safer, more effective discussions with PWE and their families. 24 Resources including the “Empowering Conversations Guide” from Preventing Epilepsy Deaths 25 and the Center to Advance Palliative Care's “Trauma-Informed Care” toolkit 26 can aid in the development of these skills.
Together, these insights underscore the need for proactive, compassionate care that prioritizes mental health, open communication, and strong support systems for PWE. By building skill, confidence, and connection, providers can foster safer conversations, reduce risk, and meaningfully improve the well-being of PWE and their caregivers.
Diet Therapy in Reduction of Epilepsy-Related Mortality
Poorly controlled epilepsy is associated with an increased risk of SUDEP. Approximately one-third of PWE do not achieve adequate seizure control with antiseizure medications alone. Therefore, it is critical to explore additional treatments that can reduce the risk of SUDEP. Dietary therapy is one such option. For example, the Ketogenic Diet has been shown to decrease mortality in mouse models, extending longevity by up to 47%.25,26
The Ketogenic Diet is a highly precise, high-fat, low-protein, and very low-carbohydrate dietary regimen used to treat epilepsy and certain metabolic disorders. All seizure types may respond to dietary therapy. Treatment is highly individualized, and a range of dietary options exist, from the strict classic Ketogenic Diet to the more flexible Modified Atkins Diet, among others. 27
Overall, the Ketogenic Diet shifts metabolism to favor fat as the primary fuel source for the brain. The mechanism by which it reduces seizure burden is likely multifactorial, including increased beta-oxidation of fatty acids, production of ketone bodies, activation of ATP-sensitive potassium channels, and enhanced GABA synthesis. 27
In general, about 10% of children on diet therapy become seizure-free, approximately 30% experience more than a 90% reduction in seizures, and 2% achieve a 50%-90% reduction. Additional benefits beyond seizure control may include reduced medication requirements, increased alertness, and improved behavior. 27
Although many patients perceive dietary therapy as a natural approach to seizure management, it is important to recognize that the Ketogenic Diet can have side effects, such as constipation and acidosis. Therefore, it should be closely monitored by a specialized team, including a neurologist and a dietitian. Dietary therapy is not a cure-all and is typically used in conjunction with antiseizure medications. It may take up to 3 months to observe the full benefits.
While any seizure type may respond to therapy, the diet is not suitable for every patient. Conversely, practitioners should not assume that a patient will be unsuccessful with diet therapy. Considerations regarding a patient's culture and values, along with aspects related to SDOH which may impact access to care should be assessed. Dietary therapy can be an important tool in epilepsy management. Because SUDEP risk increases with uncontrolled seizures, any treatment that reduces seizure frequency should be considered.
Adherence to Medications and Care and Its Impact on Outcomes
Adherence and self-management are critical for successful health and patient-reported outcomes in epilepsy. Unfortunately, non-adherence to antiseizure medications range from 25 to 50% in adults28–31 and 27-42% in children 32 with epilepsy. Suboptimal adherence can lead to significant negative consequences, including continued seizures,33–35 unnecessary antiepileptic drug changes, 36 higher healthcare costs and utilization,37–39 pharmacoresistence, 40 and SUDEP in PWE.41,42
SDOH, including lower socioeconomic status,43–46 low parental health literacy, 47 parental income, 43 rural residency status,45,46 and Black race,45,46,48 play a critical role in predicting non-adherence and early death. Additional patient and family-identified adherence barriers include forgetting, side effects, running out of medication, competing activities, difficulty swallowing pills, child refusal, and unpleasant taste.49–51
These adherence barriers are amenable to behavioral interventions. A 2020 Cochrane review of adherence interventions in epilepsy identified 20 studies, with 13 focused on adults, five focused on children and/or caregivers, one focused on adolescents, and one focused on all ages. 52 The review indicated that intensive reminders and multi-component interventions (eg, education, problem-solving) demonstrate positive results. However, more evidence-based interventions to improve adherence are still needed. One recent clinical trial demonstrated the importance of microlearning education sessions, automated reminders, and individualized feedback in a large multi-site sample of youth with epilepsy and their caregivers. 53 Translating strategies to address adherence barriers in clinical practice is imperative if we are to bring bench science to the bedside. As such, the Epilepsy Learning Health System, in conjunction with the Epilepsy Foundation, has created shared decision-making and patient handouts to address common adherence barriers (https://www.epilepsy.com/tools-resources/forms-resources/medication-tools). These can be useful for caregivers of children and the elderly, as well as pediatric and adult patients.
Conclusion
Reducing epilepsy-related mortality requires a deliberate and coordinated effort across clinical, social, and community domains. As highlighted throughout this review, proactive education, open communication, and culturally sensitive engagement empower PWE, their caregivers, and their broader support networks to better understand the risks and participate in shared decision-making.
Multidisciplinary teams are uniquely positioned to address the medical, behavioral, psychosocial, and structural factors that contribute to mortality risk among PWE. Evidence-based approaches such as standardized suicide risk assessment, trauma-informed communication, seizure safety counseling, adherence interventions, and ketogenic diet management can meaningfully reduce preventable harms. Equally important is recognizing the impacts of SDOH, which shape health disparities in access to diagnosis, treatment, education, and long-term outcomes.
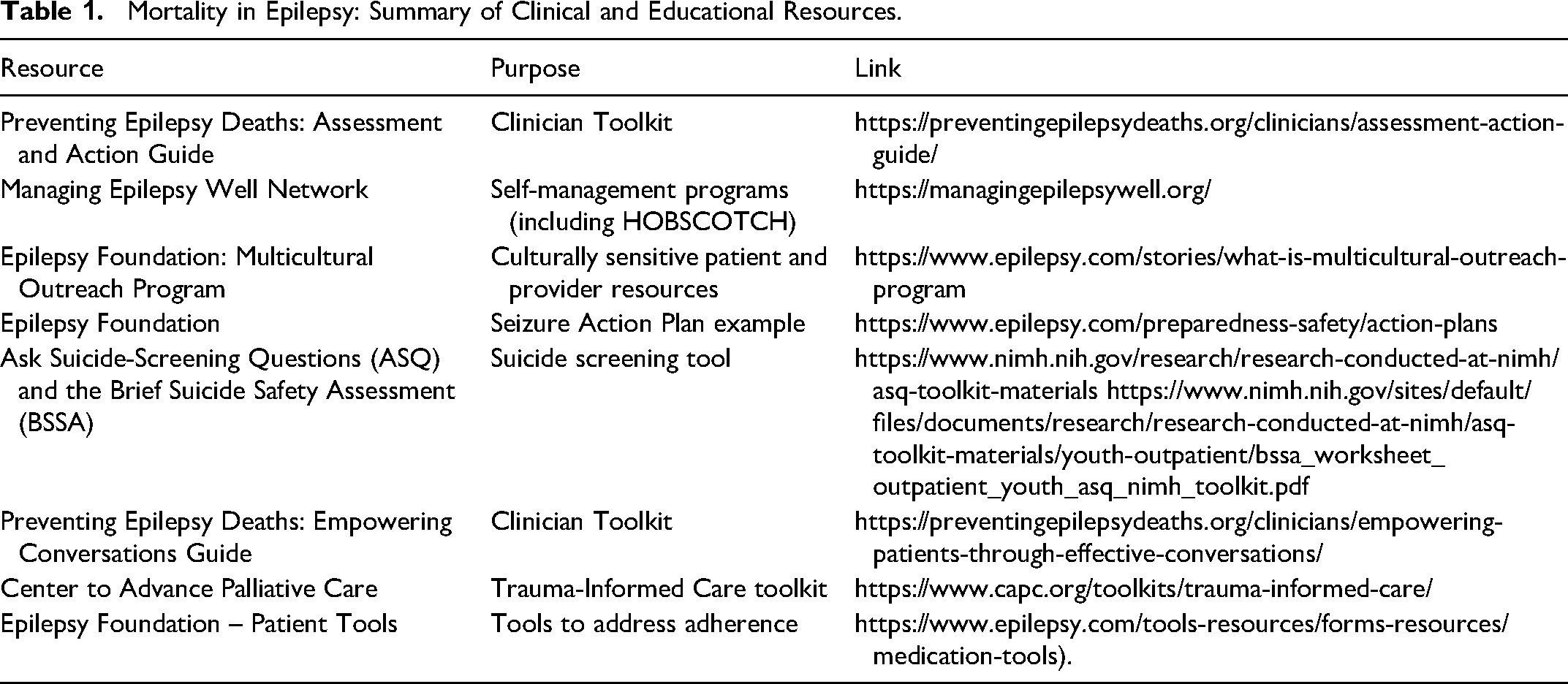
By integrating clinical best practices with SDOH frameworks and community resources (Table 1), healthcare professionals can strengthen patient safety, mitigate gaps in knowledge and care, and advance a more comprehensive model of epilepsy management. Empowering clinicians, families, and communities with tools, language, and strategies for these difficult but necessary conversations is central to improving survival and quality of life for PWE.
Mortality in Epilepsy: Summary of Clinical and Educational Resources.
We also acknowledge that additional interventional approaches to reducing SUDEP risk were not addressed in this symposium due to time constraints. Emerging technologies, such as smartwatches equipped with seizure-detection sensors, can identify convulsive seizures and promptly alert caregivers, potentially enabling timely intervention. 54 In addition, neuromodulation therapies, including vagus nerve stimulation, have been associated with a reduced risk of SUDEP. 55 Ongoing advances in technology and device-based interventions continue to expand the landscape of strategies aimed at improving safety and outcomes for PWE. Their broader implementation will depend on addressing key barriers, including health literacy, cost, and equitable access, to ensure these innovations benefit a wider population of PWE.
Footnotes
Acknowledgements
The authors would like to thank JoLynn Amsden and Paige Romanello for their invaluable support in facilitating the planning and coordination of the meeting. We also extend our sincere appreciation to the AES Interprofessional Education Committee members for their contributions in designing and organizing the symposium.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.