
Abstract
Krall RL, Penry JK, White BG, Kupferberg HJ, Swinyard EA. Epilepsia. 1978 Aug;19(4):409-28. doi:10.1111/j.1528-1157.1978.tb04507.x. PMID: 699894 By means of the maximal electroshock seizure test, the subcutaneous pentylenetetrazol seizure threshold test, and the Rotorod minimal neurotoxicity test, the Anticonvulsant Screening Project has evaluated the activity of 1,495 experimental compounds accessioned in the first 2 years. A three-screen protocol for appraising these compounds has proved reliable, fast, and inexpensive. Preliminary data show that 430 of these compounds have good anticonvulsant activity. Completed evaluations of 352 identified 16 that have anticonvulsant activity at doses less than 75 mg/kg and protective indices greater than 5.0.
Commentary
In the early 1970s, there were 16 marketed drugs for the symptomatic treatment of epilepsy, and it was recognized then that many patients did not experience adequate seizure control. There was also a great need to discover new anti-seizure medications (ASMs) with improved tolerability and safety profiles. Pharmaceutical companies at the time were not actively pursuing the development of new ASMs due to the increasing cost of development compared to the perceived market size for epilepsy. Another contributing factor was the lack of collaborating laboratories utilizing validated screening models that were able to support medicinal chemists who were developing novel compounds. The Epilepsy Branch of the then NINCDS (National Institute of Neurological and Communicative Disorders and Stroke) at the National Institutes of Health (NIH) was therefore tasked to link academic and private sector research in epilepsy therapy development to identify and further develop compounds with improved efficacy and reduced toxicity. Starting in January of 1975, the Anticonvulsant Screening Program (ASP) of the NINDS began receiving and submitting for screening novel compounds at the Program's University of Utah Contract Site. 1
Over the past 50 years, the ongoing work of the National Institute of Neurological Disorders and Stroke (NINDS) ASP, now named the Epilepsy Therapy Screening Program (ETSP), has screened more than 32,000 compounds and significantly contributed to the development of 11 current ASMs (vigabatrin, lamotrigine, oxcarbazepine, felbamate, gabapentin, topiramate, rufinamide, lacosamide, ezogabine, cannabidiol, and most recently, cenobamate). Further, program participants have communicated screening results in numerous publications, greatly adding to the knowledge base for epilepsy drug development. This work could not have been performed as successfully without the critical elements of inexpensive and rapid in vivo screening models for identification of antiseizure activity, clear endpoints for efficacy and tolerability in assays performed by skilled experimenters, and advocacy for new drugs (from NIH, pharmaceutical industry, academic researchers, and patient-caregiver organizations).
Maximal Electroshock (MES) and Subcutaneous Pentylenetetrazole (scPTZ) Screening Models: Workhorses of ASM Screening
In the first 2 years of the ASP, 1495 compounds were screened using the MES and scPTZ screening assays for efficacy and the rotarod motor impairment assay for tolerability. These initial efforts yielded several hundred compounds with antiseizure activity in these assays, and sixteen novel compounds with potent activity and optimal therapeutic indices. 1 A key element in this intial screening success was the availability of mouse models that were both inexpensive (low cost of animals and equipment) and relatively high throughput (short assay times, clear endpoints). Merritt and Putnam first used an animal model of electrically induced seizures to identify phenytoin (Dilantin) in the 1930s. 2 This pioneering work is thought of as a “monumental landmark in the history of epilepsy, pharmacology, and neurology.”3–5 Shortly afterward in the 1950s, similar methods were adopted by Swinyard, Brown, and Goodman at the University of Utah to begin identifying ASMs in mice and rats.6–8 Assay validation efforts were initially performed using standardized formulation procedures (0.9% saline or 30% polyethylene glycol solutions or suspension), time course evaluation to identify time-to-peak effect (TPE), median effective dose (ED50) determination, and median toxic dose (TD50) determination via the rotarod assay. A reference library of compounds was also evaluated to demonstrate efficacy in FDA-approved marketed ASMs and comparison to previously published in vivo data. This initial screening paradigm established two key principles that continue to inform drug screening efforts: standardized assays with reproducible endpoints and assay validation (comparison to established ASMs).
Establishment of Standard Operating Procedures and Reproducible Endpoints to Demonstrate Rigor and Reproducibility
Krall et al provides insights into the initial efforts performed to ensure rigorous standards for screening at the establishment of the ASP. 1 Blinded screening was performed for all novel compounds and, using an initial set of randomly selected compounds, internal assay validity was evaluated. The degree of variability of screening results was determined to be acceptable, as well as a low rate of false positive and false negative results. 1 This, in combination with an expanding reference compound library, demonstrated a strong rationale to continue screening and evaluating novel ASMs. The ASP's early successful establishment of assay parameters for drug screening directly lead to an ongoing success in epilepsy therapeutics that continues to the present day. Indeed, epilepsy therapy development continues to have an active pipeline. Today, as part of a large effort to improve rigor and reproducibility, the epilepsy research community, led by the International League Against Epilepsy (ILAE) and the American Epilepsy Society (AES) working groups, has fostered the incorporation of Common Data Elements (CDEs) captured in Case Report Forms (CRFs) to aid in standardization of assay conditions.9,10 Correspondingly, the Contract Site for the ETSP initiated several key practices in recent years to adhere to these standards and improve rigor and reproducibility. This includes an internal review and modernization of Standard Operating Procedures, with corresponding CDEs identified and captured in CRFs. 10 This demonstrates that the ETSP continues to focus on data rigor and reproducibility.
Paradigm Shifts: Responding to the Active and Supportive Epilepsy Research Community
The program has also adapted in several ways over the course of 50 years of screening. Where initial efforts were driven by screening of a large quantity of compounds (e.g., multiple analogs for structure-activity studies), the emphasis now is centered around key areas informed by recommendations from the 2015 and 2020 Working Group Reports of the National Advisory Neurological Disorders and Stroke Council.11,12 This exemplifies the responsiveness of the program to the needs of the clinical epilepsy population and the latest research. After the approval and widespread use of levetiracetam (Keppra, FDA approval in 1999), it was observed that the compound had been screened by the ETSP and was shown to be inactive in mouse MES and scPTZ models, and was only efficacious in the 6 Hz assay at the lower (32 mA) stimulus intensity. However, its eventual clinical development leveraged data in kindling and other models. Therefore, hippocampal kindling in rat, followed a few years later with corneal kindling in mouse, were introduced into the program and have been utilized in screening by the ETSP since that time. 13
The proportion of epilepsy patients that exhibit pharmacoresistance to the existing armamentarium of ASMs is essentially unchanged from that initially observed decades ago. Although newer ASMs address a key need for epilepsy therapy—improved safety profiles—no treatment has emerged that is effective for patients deemed pharmacoresistant (though notably cenobamate may make improvements in pharmacoresistance14,15). In response to this ongoing unmet need, the ETSP revised the program's approach to utilize more pharmacoresistant screening models. For instance, although the 6 Hz seizure model is used by the program, the current screening paradigm uses the more pharmacoresistant 44 mA stimulus intensity. Notably, while the 6 Hz 32 mA assay is sensitive to most ASMs, few ASMs are effective at the higher 44 mA stimulus intensity. The current screening paradigm for pharmacoresistant epilepsy is shown in Figure 1.12,16 This approach continues to use acute screening models (e.g., single administration and evoked seizures in naïve animals, 6 Hz 44 mA and MES assays), corneal kindling, and spontaneous seizure models (e.g., intrahippocampal, intra-amygdala, and systemic kainic acid administration to produce rodents with spontaneous recurrent seizures). 17 The program also addresses special populations of epilepsy by incorporating screens for status epilepticus, infection-induced epilepsy, and Dravet Syndrome.
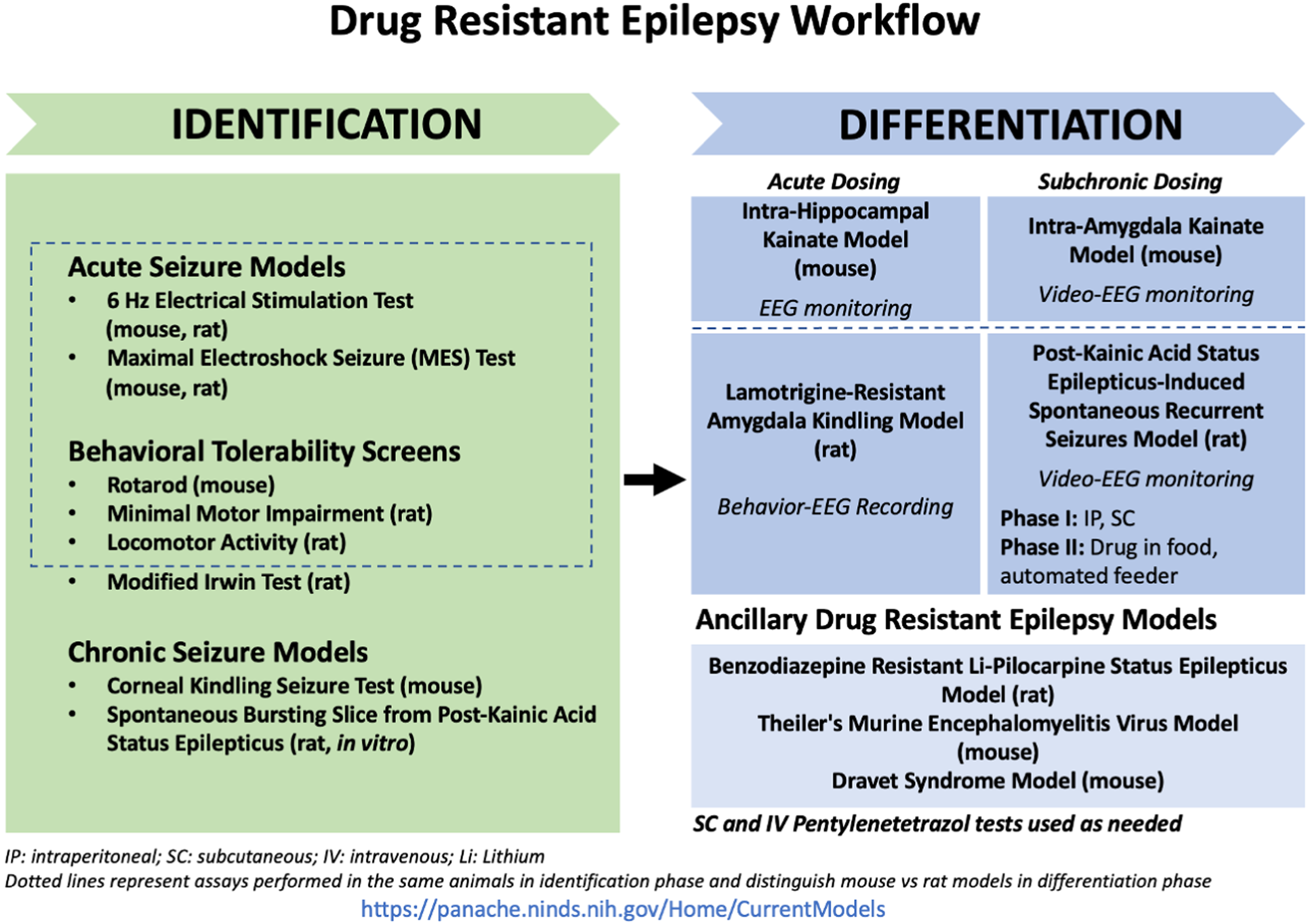
The current ETSP work flow (2025) (see also https://panache.ninds.nih.gov/).
Epilepsy Therapy Screening Beyond 2026 Merging Established and New Approaches to Develop Novel Therapies
The ASP/ETSP contract with the University of Utah constitutes one of the longest-standing NIH-funded contracts since the inception of NIH and NINDS. Other screening programs have been developed using the ETSP as an example (i.e., the Preclinical Screening Platform for Pain (PSPP)), and the program's successes have been well recognized.18–20 This successful development of novel ASMs over the past 50 years has relied heavily on the use of well-validated translational animal models of seizures and epilepsy, and the judicious use of these models is expected to continue beyond 2026. In recent years, the Program has incorporated new models of pharmacoresistance in response to the evolving needs of the epilepsy community. When new models are evaluated for potential incorporation into screening, they are rigorously evaluated and validated.21–26 Additionally, the ETSP is actively developing new translational models of acquired epilepsies (e.g., post-traumatic epilepsy resulting from brain injuries), establishing additional models suitable for evaluating disease-modifying and/or anti-epileptogenic compounds, and pharmacokinetics/bioanalytical testing to support the determination of compound levels in plasma and brain. While this work continues, the Program is also evolving to incorporate additional Novel Alternative Methodologies (NAMs) and breakthroughs in artificial intelligence that will no doubt impact workflow to increase the speed at which novel ASMs can be tested in the clinic.
Conclusion
Patients with epilepsy, caregivers, providers, and epilepsy researchers have benefited from the work of the ETSP. The program provides a clear example of the benefits of in vitro, ex vivo, and in vivo screening to provide early efficacy and tolerability data for clinical development candidate compounds. In addition to a key contribution to several FDA-approved therapies, the program has contributed to translational and basic science in epilepsy. Many of its previous and current program participants and staff are key opinion leaders in epilepsy, contributing to a wide span of research and development projects in the field. The program also continues to evolve, addressing unmet needs of the epilepsy community. The work of screening and evaluation of novel drugs is challenging, requiring an extensive understanding of current practices in translational and basic science. Not uncommonly, the ongoing needs and challenges of the program also require occasional paradigm shifts, taking into account novel approaches or practices. The goals of the program from its inception, however, remain the same: to further the development of novel compounds for epilepsy therapy for the betterment of patient care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Neurological Disorders and Stroke (grant number 75N95022C00007).