
Abstract
Posttraumatic stress disorder (PTSD) significantly influences individuals’ daily life, yet little is known about their experiences of occupational participation and the supporting resources they use. To explore the lived experiences of occupational participation among adults with PTSD and identify resources that support their participation in everyday life. Employing a qualitative design grounded in descriptive phenomenology, remote semi-structured interviews were conducted with 10 community-dwelling adults diagnosed with PTSD. Data were processed through reflexive thematic analysis. Analysis revealed three primary themes: (a) the occupational experience of living with PTSD including effort, motivational challenges, and dysregulation; (b) temporal dynamics of participation; and (c) resources supporting participation, such as balance, processing trauma through occupation and doing for others. The findings elucidate the ways in which trauma influences occupational experiences and highlight key resources that can facilitate participation, offering valuable insights to advance occupational therapy practice for individuals with PTSD.
Plain Language Summary
Living with posttraumatic stress disorder (PTSD) can affect how people experience everyday occupations such as work, relationships, and self-care. This study explored how adults with PTSD experience their daily participation and which resources support their participation in occupations. Ten adults were interviewed about their everyday lives. Participants described that daily occupations often require high effort, feel less enjoyable, and are frequently driven by necessity rather than personal choice. Participation was also described as fluctuating over time, with days or periods of greater and lower participation. Participants identified several resources that helped them participate, including having routines, balancing activity and rest, caring for others, using occupations to cope with and process trauma, and receiving social support. These findings show that everyday occupations play an important role in recovery from PTSD and that supporting participation can improve quality of life.
Introduction
Posttraumatic stress disorder (PTSD) has a significant and far-reaching impact on individuals’ participation in daily occupations – a central component of health and quality of life (QoL). While much attention has been given to PTSD’s observable participation limitations, subjective dimensions associated with participation remain underexplored. In addition, the internal and external resources individuals use to carry and sustain participation are scarcely addressed. To address this gap, the present study explores the subjective experience of participation and questing after resources that support positive occupational experiences.
PTSD is a prolonged health condition that develops following direct or indirect exposure to events involving actual or threatened death of the individual or a close other (American Psychiatric Association (APA), 2013). PTSD formation reflects not only the objective threat but also the individual’s subjective experience of the situation and may involve persistent dysregulation across emotional, cognitive, and physiological domains (Van der Kolk, 2003). Core PTSD symptoms include reexperiencing the initial traumatic event(s) through intrusive thoughts and memories, avoidance, arousal fluctuations, and negative cognitions and mood changes, often triggered by internal or external cues associated with the traumatic event, which may significantly affect individuals’ daily functioning (APA, 2013). PTSD is associated with diminishing QoL, psychiatric comorbidities, chronic disease, high suicide risk, and premature mortality (Koenen et al., 2017; Substance Abuse and Mental Health Services Administration [SAMHSA], 2014). Approximately 6% of those exposed to traumatic events develop PTSD (APA, 2013; Koenen et al., 2017), with a global lifetime prevalence estimate of 3% to 7% (World Health Organization [WHO], 2024).
Participation in daily occupations is central to health and QoL, and involves both objective and subjective dimensions (Alter, 2015; American Occupational Therapy Association [AOTA], 2020; Kuo, 2011; WHO, 2008). The objective dimension includes observable aspects such as frequency and diversity of activities, location, and assistance provided (e.g., infrequent showering, or needing assistance to attend medical appointments) (AOTA, 2020). The subjective dimension, also known as occupational experience, addresses intrinsic needs of meaning, purpose, connectedness, choice, and control, and includes a wide range of experiences like pleasure, competence, balance, and restoration (e.g., experiencing satisfaction at work, or lacking enjoyment in leisure activities; Hammell, 2009; Pierce, 2003).
A substantial body of evidence highlights the negative impact of PTSD on objective participation across various occupational domains and life roles (Edgelow et al., 2019; Jellestad et al., 2021). Individuals with PTSD experience significant limitations in basic and instrumental activities of daily living (IADL), reporting specific challenges in health management, sleep, meal planning, managing finances, and driving (Clapp et al., 2014; Edgelow et al., 2019; Jellestad et al., 2021; Punski-Hoogervorst et al., 2023; Shapira et al., 2024). In addition, PTSD is linked to work and educational-related performance challenges (Edgelow et al., 2019), along with a decline in participation in leisure activities (Shapira et al., 2024; Stewart et al., 2020). Furthermore, challenges in occupations of parenting and social participation, including social isolation, are well documented (Dutra et al., 2016; Plach & Sells, 2013). Even though profound difficulty in the subjective participation dimension was suggested in PTSD (Shapira et al., 2024), understanding of this dimension of participation is limited.
This study addresses this gap by exploring (a) occupational experiences while living with PTSD and (b) internal and external resources supporting positive occupational experiences and participation, with the ultimate goal to inform theory on PTSD’s impact on participation and advance practices supporting health and QoL through everyday occupations.
Method
Design
This qualitative study adopted a descriptive phenomenological orientation and used reflexive thematic analysis to explore how adults with PTSD experience occupational participation (Braun & Clarke, 2006, 2019; Creswell & Poth, 2018). The study was approved by an institutional review board and reported in line with COREQ (Tong et al., 2007).
Participants
Participants were recruited through convenience sampling via social media platforms for PTSD, using targeted posts. Eligibility was confirmed through a brief telephone screening interview. Ten adults were included based on the following criteria: (a) self-reported formal diagnosis of PTSD; (b) current community residence; and (c) age ≥ 18 years. Exclusion criteria were: (a) current hospitalization and (b) any major health condition (other than PTSD) that produced significant participation limitations at the time of the study. Efforts were made during recruitment to enhance heterogeneity in participants’ experiences by disseminating study invitations across a range of online communities and forums for individuals with PTSD, including platforms representing diverse trauma backgrounds and demographic characteristics. These recruitment channels were selected to reach individuals with variation in trauma type, age, life roles, and gender. Although participants were not excluded to achieve sample diversity, these recruitment strategies were intentionally designed to enhance variability across these characteristics. All participants provided written informed consent prior to participation.
Data Collection
Research procedures included completion of a brief demographic questionnaire (age, family status, education, trauma type, and age at the traumatic event[s]) and 2-hr interviews conducted by a trained occupational therapist with experience in PTSD. Participants were offered the option of either an in-person interview at the university research site or a remote interview. All participants chose the remote option, and interviews were therefore conducted via Zoom. Data collection lasted over a 6-month period. No participants withdrew after consent. All interviews were conducted in Hebrew with native Hebrew-speaking participants. Interview quotes presented in the manuscript were translated into English collaboratively by the authors to ensure that the original meaning and nuance of participants’ expressions were preserved.
Interview Guide
A semi-structured interview guide was developed specifically for this study to explore participants’ experiences of occupational participation with PTSD. (For full interview guide, see Supplementary File 3.) The interview followed trauma-informed principles, emphasizing participants’ sense of safety and control over the setting and pace.
Data Analysis
Qualitative interviews were audio-recorded, transcribed verbatim, and analyzed with ATLAS.ti software (version 9; Scientific Software Development GmbH). All three authors independently reviewed the transcripts, identified significant statements, and organized them into meaning units, which were coded and consolidated into broader categories from which overarching themes were derived. Ongoing analytic discussions supported trustworthiness and comprehensive data coverage.
Rigor and Reflexivity
Data were analyzed iteratively, with themes developed inductively and refined through repeated comparison with the original data to enhance credibility. Rigor was further supported through peer debriefing, multi-perspective review, and ongoing reflective dialogue among the research team throughout the analysis process. Themes were refined collaboratively to remain grounded in participants’ language and meanings. To support comfort and privacy in the remote interview context, participants were asked to select a quiet and private location for the Zoom interview, where only the participant and the occupational therapist were present. Data were analyzed in Hebrew, and selected quotations were translated into English with careful attention to preserving their intended meaning.
Researcher Positionality
All authors are occupational therapists with professional backgrounds in mental health and trauma-informed practice. Their clinical and academic engagement with adults living with PTSD informed the study’s focus on participation and everyday occupations as central to health and recovery. The authors approach trauma as an individual experience rather than solely as a diagnostic category. They remained attentive to how these perspectives might shape the research process and interpretation and sought to foreground participants’ voices and lived meanings throughout the analysis.
Results
Participant Description
Ten adults with PTSD (six women, three men, one transgender) participated in this study. The sample represented diversity in gender identities, life roles, and trauma types. Participants described experiences encompassing individual, developmental, and collective forms of trauma (see Table 1). Their ages ranged from 33 to 55 years (M = 41.3, SD = 6.18). Participants experienced trauma at different life stages: childhood, adulthood, or both, and reported varying trajectories in their use of supportive services, ranging from recent engagement in therapy to long-term use of mental health and rehabilitation services.
Participants’ Characteristics (N = 10).
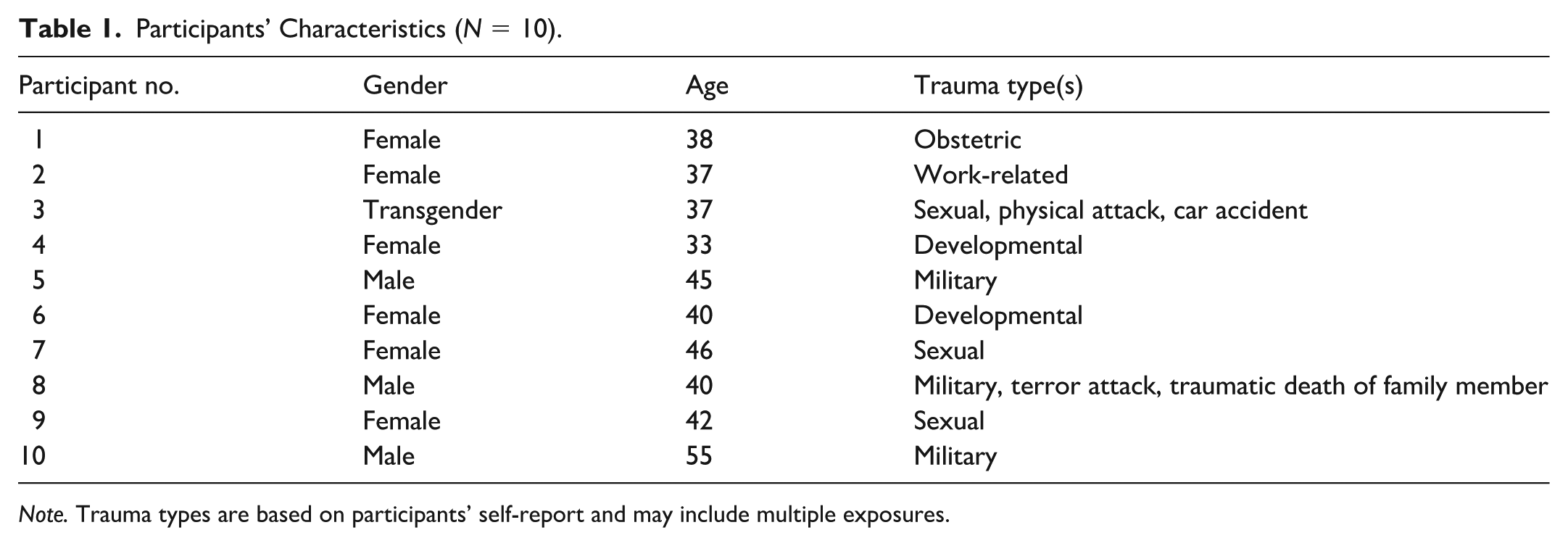
Note. Trauma types are based on participants’ self-report and may include multiple exposures.
The analysis identified three interrelated themes: (a) the occupational experience of living with PTSD, (b) temporal dynamics of participation, and (c) resources to support participation (Table 2).
Overview of Themes, Subthemes, and Their Descriptions.
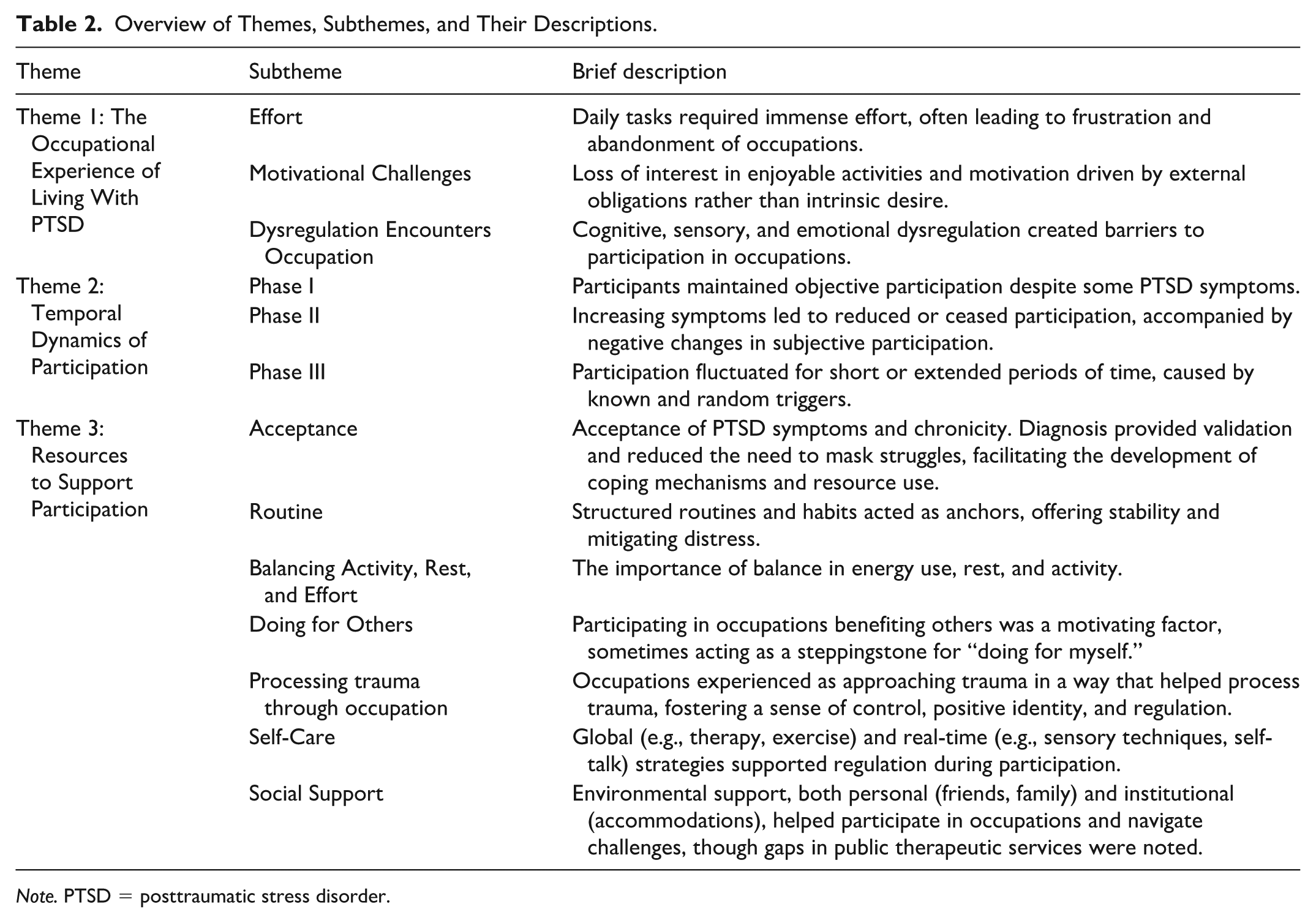
Note. PTSD = posttraumatic stress disorder.
Theme 1: The Occupational Experience of Living With PTSD
This theme highlights the impact of PTSD on occupational experiences, with three subthemes: (a) effort, (b) motivational challenges, and (c) dysregulation encounters occupation.
Effort: “Everything Is Like Climbing Mount Everest”
Participants described the immense effort required to perform everyday activities – even simple tasks that were previously performed automatically, such as bathing or preparing food: “You look at everything and think it’s like climbing Mount Everest . . . I used to do these things easily . . .” (P1).
This constant effort often led participants to withdraw from activities or abandon them in advance due to anticipated exhaustion.
Motivational Challenges: “Driven by Necessity”
Participants described difficulty in identifying preferences, loss of interest in previously enjoyable activities, and a lack of drive to participate in new ones: “I used to have a clear sense of my interests . . . These days, I’ve lost interest in all of these activities, I find myself in a state of uncertainty about what truly interests me” (P3).
Participants commonly described their participation as stemming from a sense of obligation rather than personal desire: “The activities I engage in are primarily driven by necessity. There’s a sense of obligation and external expectations to perform these tasks, even if I don’t necessarily have a personal desire to do them” (P6).
Dysregulation Encounters Occupation: “I Missed My Bus Stop”
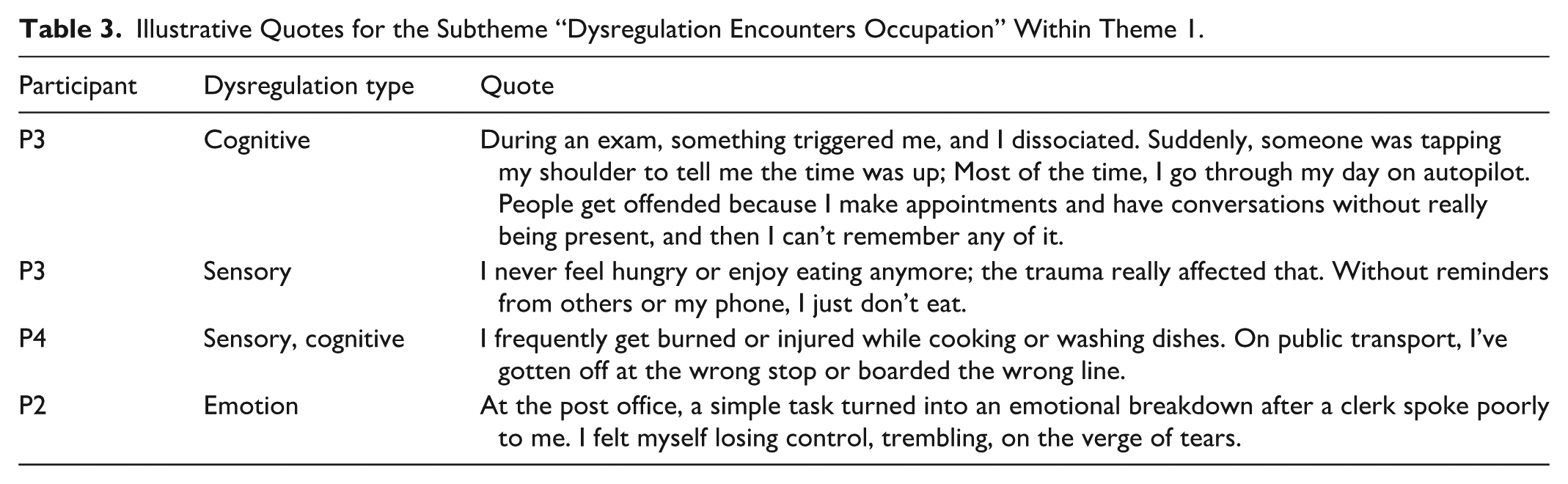
Participants experienced cognitive, sensory, and emotion dysregulation as significant barriers to effective occupational-based participation. Dysregulation experiences were described on a continuum from dissociation to hyper-responsiveness. Table 3 provides illustrative quotes demonstrating the variability of dysregulation in real-world occupational contexts.
Illustrative Quotes for the Subtheme “Dysregulation Encounters Occupation” Within Theme 1.
Theme 2: Temporal Dynamics of Participation
This theme outlines a temporal trajectory of participation after trauma, highlighting changes in both subjective and objective dimensions over time. Three phases portray a preliminary roadmap of participation across different stages of living with PTSD, though they do not represent a strict or uniform progression.
Phase I: “I Lived a Normal Life”; “I Was Fully Functional”
Participants recalled experiencing manageable routines and participation for extended periods, often lasting several years, as exemplified by a man coping with PTSD from military events, described his life after his service: “I lived a normal life of a student, engaging in various activities, working . . . I was functioning at a high level, maintaining a routine, and everything seemed good” (P5).
For some participants, high levels of objective participation served as a coping mechanism following the trauma: “I was consistently overdoing both at work and at home. Later, I recognize that this behavior is my coping mechanism, a way to avoid facing my emotions and feelings” (P9); “I repressed the terrible, scary birth, I believed I could overcome it. For the next four years, this coping mechanism seemed to work well for me. I was fully functional, fulfilling my role as a mother” (P1).
Phase II: “I Stopped Functioning, Stopped Enjoying Activities”
During this phase, participants described a gradual intensification of symptoms that severely impacted their participation, ranging from reduced participation in daily activities to complete cessation of participation: “I’ve had to significantly reduce my involvement in work and volunteer activities. I now work considerably less, and function less at home” (P8); “I quit my job, and from then on, the situation spiraled downward rapidly . . . I couldn’t function and was admitted to a psychiatric hospital” (P9).
Participants also reported a loss of enjoyment in activities they once found pleasurable, reflecting significant changes in subjective participation: “I stopped enjoying activities that I used to enjoy” (P1).
Phase III: Ongoing Fluctuations
Participants described fluctuations in participation, both subjective and objective, occurring over varying time frames and with varied levels of predictability: “Before I started taking medication, it was like alternating between good days and bad days, almost all the time” (P6); “Starting from the Israeli Memorial Day until my brother’s memorial day . . . I’m completely dysfunctional. Even something as simple as a patient’s date of birth at work matching my brother’s is enough to halt my day completely” (P8).
Unexpected triggers further disrupted plans and participation, creating unpredictability: “You can’t expect anything and can’t make any plans . . . I missed my son’s graduation party because of a panic attack. I was dazed from sedatives, and my mother and sister went in my place” (P1).
Theme 3: Resources to Support Participation
This theme highlights internal and external resources participants identified as key to enhancing their participation in occupations including acceptance, routine, balance, doing for others, processing trauma through occupation, and social support.
Acceptance
Acceptance was described as a lengthy process, involving recognizing PTSD symptoms, obtaining a formal diagnosis, and gaining validation for participation challenges: “This concept of PTSD gave me internal clarity and matched my experience . . . It is a kind of shield that says: look, I’m not as capable as you, I have official recognition” (P2).
For many, this recognition marked a turning point, enabling them to share their struggles and reduce the effort of masking their challenges: I used to hide everything. I could come to work in a terrible state and pretend everything was fine. In recent years, I decided to be open about the fact that I’m struggling. This shift led to positive changes . . . I started participating in a support group and started sharing my experience with colleagues at work. (P7)
Participants also described an internal process of acknowledging PTSD’s chronic nature: It wasn’t until this year that I truly grasped the chronicity of PTSD . . . The realization that it applies to me . . . I used to tell myself, “I’ll bounce back in a year.” But then it hit me – it’s chronic, something I must learn to coexist with, to navigate ongoing situation. (P3)
Acceptance emerged as a pivotal internal resource, laying the groundwork for participants to develop and utilize additional internal and external resources to support participation. The following subsections reflect these resources.
Routine
Participants emphasized the importance of routine in mitigating psychological distress: “For survival, I find it necessary to establish more permanent activities daily. Currently, I lack sufficient inner strength to self-motivate, so I look for external activities to motivate me” (P2). Fixed activities served as anchors, providing structure and stability. Participants described small, regular habits as instrumental in maintaining these routines: I go jogging every morning . . . I drink a cup of black coffee as soon as I wake up, put my running shoes next to the kettle beforehand, and when it boils, I put them on. It is not easy, requires a lot of discipline, but it works better than the psychiatrist. (P5)
The intensity of routines varied, ranging from one central daily activity to multiple structured activities throughout the week: “I now work three days a week for four hours each day. This arrangement provides structure to my days and gives me a purpose to get up in the morning” (P2).
Although establishing and maintaining routines often required considerable effort, as described in Theme 1, participants emphasized their value as stabilizing structures that supported occupational participation.
Balancing Activity, Rest, and Effort
Participants emphasized the need for balance across activity, rest, and effort to support participation. Balancing activity levels often involved being cautious about over-activity: “I’m striving for balance, I want to avoid extremes, whether it’s working all the time or having those occasional super-productive days. I have such a tendency, and I am aware not to let it become a daily matter” (P9).
In addition, setting aside time for rest was mentioned: I came to realize that it’s much more effective to pause and declare a day off when I’m not feeling well. This wave of difficulty passes more swiftly when I take a step back, attend to self-care and rest, rather than expend significant energy insisting that everything is fine, that I’m fully functional . . . Today, it’s no longer about maintaining functionality, my well-being is above all. (P7)
Another key component of balance was effort, which also emerged in Theme 1 as a central occupational experience among individuals with PTSD. In this context, participants described learning to balance effort by occasionally avoiding overly demanding environments or tasks: “In the process of my recovery, I learned that sometimes it’s good to avoid. Let’s say going to the mall, it’s a hectic place, I learned to avoid it” (P4).
Doing for Others
“Doing for others” included caring roles such as parenting, as well as supporting others in social, educational, or therapeutic contexts. Regardless of the specific role, participants described doing for others as more motivating than engaging in activities solely for themselves. Sometimes doing for others served as a kind of a steppingstone to participate in self-focused occupations: I bring myself back to reality and say to myself: “You have children, many obligations as a mother . . . I get up, prepare lunch for the children, and then I attend to my own needs. I take a shower, get dressed, and then I can just go out.” (P1)
Processing Trauma Through Occupation
Some participants engaged in occupations that helped them approach and process their traumatic experiences: “Writing is a place of refuge, a place to express a moment, to process what I experience” (P1). These occupations served as a resource for expressing and processing their traumatic experiences, offering them a positive sense of presence, regulation, control, and positive identity: Due to numerous physical scars, I dealt with body insecurity for many years, constantly concerned about how my body appeared and how it deviated from the norm. However, through drawing these imperfections, I found a sense of liberation, I can tell myself that I’m fine, I’m not like everyone else, but fine. (P9)
Some participants highlighted that assuming roles, like being a mother or working as a therapist, offered a way to repair traumatic experiences. This process occurred through routine actions and occupations that were part of that role: Because I was treated poorly as a child, when I became a mother, I recognized the power that comes with the role. I exert authority . . . If I decide it’s time for a shower, then it’s shower time. However, when doing it I’m committed to not being forceful, humiliating, or aggressive. (P4)
Self-Care
Participants described self-care as essential for managing PTSD. General self-care strategies included therapeutic support, medication, physical exercise, and sufficient sleep. Real-time self-care strategies focused on managing immediate challenges through cognitive (self-talk, guided imagery), emotional (meditation), sensory (temperature control, ice, music), and physical techniques (breathing exercises): “Cold has a significant regulatory effect on me. I might close the door and turn on the air conditioner to its coldest setting for a few minutes to regain a sense of regulation” (P7).
A real-time self-monitoring strategy was identified: “I call it ‘my traffic light’. When it’s green, I’m in a state of awareness and effectively managing the situation. Yellow indicates my recognition of warning signs; red means stop everything no matter what” (P7). Real-time self-regulation was also achieved by communicating positively with others: “In a crowded elevator I felt threatened and started to feel like I would explode. Instead, I greeted everyone cheerfully, turning anxiety into laughter. It was my way of grounding myself in the moment” (P5).
Social Support: “Doing It Together, Try to Ease the Burden”
Participants highlighted the vital role of social support in facilitating participation, both at a personal level and through broader social systems. Personal support often involved assistance with tasks: “I had to go to the dentist. My friend researched and booked the appointment for me. After that, I could handle it on my own” (P2).
Support extended to shared activities with groups, such as running errands or attending events together. On an institutional level, accommodations in educational and workplace settings provided accessible pathways for participation. “On difficult days, I ask others to come over instead of going out. We spend time or even work together, making things more manageable” (P3).
Participants also emphasized the value of therapeutic groups in which members shared similar challenges: “We’ve organized outings where everyone understands each other’s triggers and doing it together helps ease the burden and normalize the experience” (P2).
However, some participants expressed concerns about the lack of adequate therapeutic services and a general sense of being unsupported by the health system. These concerns included long delays in receiving care, limited availability of trauma-informed professionals, and difficulties accessing services that were responsive to the specific needs and characteristics of individuals with PTSD.
Discussion
This study aimed to explore the lived experiences of occupational participation among individuals with PTSD and to identify the internal and external resources that support participation. The findings also highlight temporal patterns, reflecting the dynamic nature of participation over time. Findings are discussed in light of contemporary frameworks that conceptualize trauma as multifaceted phenomenon, encompassing individual, developmental, and collective dimensions with potential negative impacts on participation and well-being (Ashcraft & Lynch, 2025; SAMHSA, 2014). A recent scoping review of occupation-based trauma research highlights the growing but still fragmented nature of trauma-related research within occupational therapy, underscoring the need for integrative perspectives that connect participation, experience, and recovery processes (Costas-Franco et al., 2025). Drawing on the findings of this study, we propose a preliminary conceptual framework to advance understanding of PTSD and its role in shaping participation (Figure 1). The framework integrates three central components of participation identified in this study: the lived occupational experiences of individuals with PTSD, the temporal dynamics through which participation unfolds over time, and the internal and external resources that support participation. Together, these elements illustrate how occupational participation in individuals with PTSD emerges through the ongoing interaction between occupational experience, change over time, and the resources individuals mobilize in everyday life.
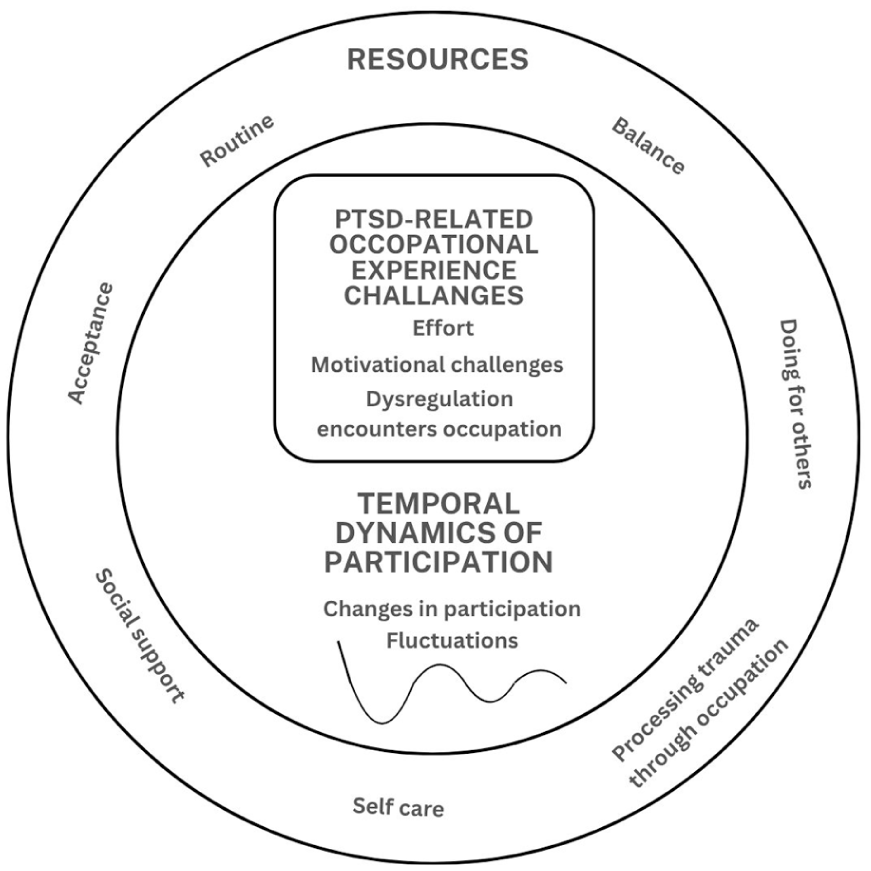
Preliminary conceptual framework: Occupational participation in individuals with PTSD.
The Occupational Experiences of Living With PTSD
The occupational experiences identified in this study were characterized by high effort, reduced interest, and obligation-driven participation. These patterns reflect limited autonomous motivation, which is considered essential for psychological health according to Self-Determination Theory (Ryan & Deci, 2000), and is consistent with recent qualitative findings on motivation and participation among individuals with PTSD (Lu et al., 2024). These findings are consistent with previous research describing occupational challenges among individuals with PTSD (Shapira et al., 2024; Stewart et al., 2020), while also extending existing knowledge by illuminating additional impaired aspects of personal experience as manifested in everyday participation. Diminished volition resonates with the Model of Human Occupation (MOHO; Kielhofner, 2008), which emphasizes role of personal agency in fostering occupational adaptation. As such, these experiences may hinder occupational adaptation and participation and may negatively affect long-term psychological health of individuals with PTSD.
Another central characteristic of occupational experiences emerging from this study is that of dysregulation, aligning with PTSD symptoms (APA, 2013; Aupperle et al., 2012; Engel-Yeger et al., 2013; Freichel et al., 2024; McMahon, 2024). The current findings provide insights into experiences of cognitive, emotional, and sensory dysregulation in the context of daily occupations. A few examples of such dysregulation are performing tasks on “autopilot,” difficulties recalling social interactions (leading to strained relationships), injury during routine tasks, forgetting basic needs, and experiencing intense emotional responses to seemingly simple events (e.g., a post office visit). These findings underscore the pervasive and complex ways in which dysregulation disrupts effective and satisfying participation in occupations, highlighting its significant daily costs in PTSD.
Beyond that, the findings highlight the dynamic interplay between motivational constraints and regulatory challenges as shaping occupational experiences in PTSD. This integrative perspective extends existing knowledge, aligning with the ICF framework (WHO, 2008), which conceptualizes participation as emerging from interactions between body functions and participation, while specifying the interdependence of motivation and regulation within lived occupational experience.
Temporal Dynamics of Participation
The temporal patterns identified in this study suggest that occupational participation in individuals with PTSD unfolds through a dynamic, non-linear process of change, marked by sustained fluctuations in both objective and subjective dimensions over time. This perspective aligns with Doroud et al.’s (2015) description of recovery from mental illness as an “occupational journey,” which emphasizes the importance of occupational engagement in regaining a meaningful and contributive life. Recent longitudinal research further demonstrates the dynamic nature of PTSD-related functional impairments over time (Freichel et al., 2024). While previous studies primarily focused on short-term occupational changes following trauma and fluctuations in symptoms and functional impairments, the contribution of this study lies in its longitudinal exploration of occupational experience, offering insights from individuals who have been coping with PTSD for years and striving toward recovery. These findings also resonate with broader recovery models, such as the CHIME framework (Leamy et al., 2011) and Herman’s (1998) trauma recovery model, both of which conceptualize recovery as a cyclical and evolving process. From an occupational perspective, current findings underscore the importance of addressing both objective and subjective dimensions of participation to foster sustainable recovery.
Resources to Support Participation
This study highlights a constellation of internal and external resources that individuals with PTSD actively use to support their participation. These resources include acceptance, routines, balancing activity, rest and effort, doing for others, processing trauma through occupation, self-care, and social support. Together, they illustrate how individuals adapt to and navigate their occupational lives while living with PTSD. While several of these resources align with prior trauma and occupational therapy literature (Edgelow, 2025; Gill, 2021; Torchalla et al., 2019), the present findings extend existing knowledge by illuminating how these resources are enacted in everyday life.
Notably, acceptance emerged as a foundational internal resource that reduced masking and supported the mobilization of additional resources. Routines and balance functioned as stabilizing structures that anchored participation, even when motivation and regulation were compromised. Doing for others often served as a gateway to self-focused participation. Occupations were also used as resources for trauma processing and identity repair, positioning participation as part of the ongoing recovery process. Self-care and social support further operated as real-time regulatory and participation-enabling resources.
These findings align with models of occupational experience that emphasize the potential of positive occupational experiences to enhance health and QoL across diverse populations (Hammell, 2009; Moll et al., 2015; Pierce, 2003). More specifically, participation in meaningful occupations has been shown to mediate the relationship between stressful life events and resilience (Sherman et al., 2024). In this context, the present findings further suggest that participation may be actively involved in recovery processes in PTSD through the cultivation of resources that promote positive occupational experiences in everyday life.
These findings resonate post-traumatic growth (PTG), which describes positive changes emerging through continued struggle with trauma (Tedeschi et al., 2018). The co-existence of ongoing occupational challenges alongside the development of supportive resources reflects adaptive processes consistent with PTG. Importantly, the present findings situate PTG within the context of everyday participation, demonstrating how growth is enacted not only through cognitive reframing but also through concrete patterns of participation.
Together, these findings help illuminate the relationships represented in the proposed conceptual framework, highlighting how occupational experiences, temporal participation patterns, and participation-supporting resources interact to shape occupational participation among individuals with PTSD.
Limitations and Recommendations for Future Studies
The relatively small sample size may have limited the breadth of occupational perspectives represented. Most participants had been living with PTSD for several years; therefore, future studies should examine occupational experiences across different stages of living with PTSD. While the inclusion of participants exposed to diverse trauma contexts enabled exploration of varied occupational experiences, different trauma types may shape participation in distinct ways. For example, prolonged or interpersonal trauma, often associated with complex PTSD, may generate participation patterns that differ from those following single-incident events. Examining subgroups separately may clarify variation in participation patterns and resource needs, thereby strengthening the depth and applicability of occupational perspectives on PTSD.
In addition, several procedures commonly used to enhance qualitative rigor were not implemented in this study. Repeated interviews were not conducted, field notes were not taken during or after the interviews, and transcripts were not returned to participants for comment or correction. Participants also did not provide formal feedback on the findings. Future studies may consider incorporating these strategies to further strengthen the trustworthiness of qualitative inquiry.
Implications for Practice and Research
The preliminary conceptual framework proposed in this study provides an occupation-centered lens for understanding participation among individuals living with PTSD and may guide clinical reasoning in occupational therapy practice. Individuals living with PTSD often experience participation challenges that are insufficiently addressed within standard trauma-care services. The present findings highlight challenges in occupational experience and fluctuating participation patterns having a potential to affect substantially health and QoL. These findings underscore the role of occupational therapy in identifying trauma-related occupational needs and supporting recovery through participation-centered strategies. More specifically, it is recommended to (a) collaborate with interdisciplinary teams advocating for the inclusion of occupational therapy within trauma-focused services and ensure that participation is addressed as a central component of recovery and sustained QoL; (b) within OT practice integrate participation-centered reasoning into assessment and intervention, with an emphasis on supporting the development of internal and external resources that promote positive occupational experiences.
Conclusion
This study explored the lived experiences of occupational participation among individuals with PTSD, alongside temporal patterns of participation and the resources that support participation in daily life. The findings highlight that participation is shaped by complex occupational experiences characterized by effort, motivational challenges, and dysregulation, unfolds dynamically over time, and is supported by a range of internal and external resources.
By outlining these core aspects, the study emphasizes the substantial toll PTSD may take on individuals’ occupational participation and QoL. The findings offer a preliminary conceptual framework for understanding PTSD from an occupational perspective (Figure 1), which may inform the development of occupation-centered practices aimed at fostering health and participation in this population.
Supplemental Material
sj-docx-1-otj-10.1177_15394492261459956 – Supplemental material for Beyond Observable Participation: Occupational Experiences, Temporal Dynamics, and Resources Used in Posttraumatic Stress Disorder
Supplemental material, sj-docx-1-otj-10.1177_15394492261459956 for Beyond Observable Participation: Occupational Experiences, Temporal Dynamics, and Resources Used in Posttraumatic Stress Disorder by Stav Levy–Smith, Adina Maeir and Lena Lipskaya-Velikovsky in OTJR: Occupational Therapy Journal of Research
Supplemental Material
sj-docx-2-otj-10.1177_15394492261459956 – Supplemental material for Beyond Observable Participation: Occupational Experiences, Temporal Dynamics, and Resources Used in Posttraumatic Stress Disorder
Supplemental material, sj-docx-2-otj-10.1177_15394492261459956 for Beyond Observable Participation: Occupational Experiences, Temporal Dynamics, and Resources Used in Posttraumatic Stress Disorder by Stav Levy–Smith, Adina Maeir and Lena Lipskaya-Velikovsky in OTJR: Occupational Therapy Journal of Research
Supplemental Material
sj-docx-3-otj-10.1177_15394492261459956 – Supplemental material for Beyond Observable Participation: Occupational Experiences, Temporal Dynamics, and Resources Used in Posttraumatic Stress Disorder
Supplemental material, sj-docx-3-otj-10.1177_15394492261459956 for Beyond Observable Participation: Occupational Experiences, Temporal Dynamics, and Resources Used in Posttraumatic Stress Disorder by Stav Levy–Smith, Adina Maeir and Lena Lipskaya-Velikovsky in OTJR: Occupational Therapy Journal of Research
Footnotes
Acknowledgements
The authors wish to thank the study participants for sharing their experiences.
Ethical Considerations
This study was approved by the Ethics Committee of the Faculty of Medicine, Hebrew University of Jerusalem (Reference ID: 31082021).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was written as part of a doctoral dissertation, which is supported by the President of Israel Scholarship for Excellence and Scientific Innovation. The specific study reported in this manuscript was conducted prior to receiving this funding.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during the current study are not publicly available due to ethical and privacy considerations related to sensitive trauma-related information, but are available from the corresponding author on reasonable request.
AI Statement
Generative artificial intelligence tools were used for language editing only. All intellectual content, analysis, and interpretation were conducted by the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.