
Abstract
This study examined parents’ perceptions of constraints that impact the attainment of independent walking in children with CHARGE syndrome. This syndrome is a multifaceted syndrome including a degree of vision and hearing loss at birth. The Dynamic Systems Theory (DST) was used as an ecological lens to provide insight into the complexity of issues impacting independent walking from the parents’ perceptions. Semi-structured interviews were administrated to 23 parents of children with CHARGE syndrome to ascertain the degree to which individual, environmental, or task constraints impacted their child’s development of independent walking. Data analysis was conducted through direct content analysis based on the DST. Parents reported that the task of walking was impacted by individual constraints, both structural and functional, and environmental constraints, such as space, surface area, and the use of furniture. Recommended interventions for professionals who work with children who are deafblind include manipulation and adaptation of environmental and task constraints.
CHARGE syndrome is multifaceted with complex anomalies, which may include a degree of vision and hearing loss at birth. Historically, six criteria were used to diagnose an individual with CHARGE syndrome: coloboma (i.e., hole in the structure of the eye), heart defects, atresia of the choanae (i.e., narrowing or closure of the nasal cavity), retardation 1 or delay of growth and/or development, genital and/or urinary abnormalities, and ear abnormalities and deafness (Pagon et al., 1981). In 2004, the mutation of chromodomain helicase DNA binding protein 7 (CHD7) gene was reported as a cause for CHARGE syndrome (Vissers et al., 2004). As a result, CHARGE syndrome is now considered a congenital autosomal dominant genetic disorder and the diagnostic criteria have been broadened (Hale et al., 2016). In 2017, the prevalence of children with CHARGE syndrome receiving special education services within the Unites States was 933; therefore, CHARGE syndrome is currently the leading hereditary syndrome causing childhood deafblindness (National Center on Deaf-Blindness [NCDB], 2017).
The majority of children with CHARGE syndrome are delayed in the development of motor milestones such as crawling, standing, and walking (Hartshorne et al., 2007). Because these motor milestones are relatively sequential and provide a progressive pattern, any delay in their attainment may impede further motor development (Johnson & Blasco, 1997). Furthermore, research has reported the age at which children with CHARGE syndrome independently walked was an important development indicator correlated with the acquisition of language (Petroff, 1999), symbolic communication (Thelin & Fussner, 2005), adaptive behavior scores (Salem-Hartshorne & Jacob, 2004), and executive function behaviors (Hartshorne et al., 2007).
Early identification of CHARGE syndrome is therefore important to provide interventions to decrease the risk of developmental delays because natural opportunities to learn, move, and communicate can be severely limited (NCDB, 2017). Of particular importance is the child’s ability to walk independently. Independent walking provides a means for children to explore and interact with new objects, people, and environments. This is especially important for children with CHARGE syndrome because being deafblind, much of their world is accessed through the sense of touch.
Children with CHARGE syndrome do not typically walk until approximately 36 to 60 months (Hartshorne et al., 2011). This age range exceeds the average for children without disabilities (8.2–17.6 months; World Health Organization Multicentre Growth Reference Study Group, 2006). Abadie et al. (2000) identified unusual patterns of motor development in children with CHARGE syndrome. For instance, walking indoors was typically not obtained until 18 to 52 months and walking outdoors was not obtained until 2.5 to 5 years. However, there is limited research on the direct causes delaying independent walking in children with CHARGE syndrome, particularly given the complexity of the disability.
Variability in motor development patterns has been explored using the Dynamic Systems Theory (DST; Bernstein, 1967; Stergiou & Decker, 2011; Thelen, 1992). Although primarily applied to children without disabilities, DST can also be used as a framework to explore how and why children experience delayed walking and could be used to inform the design of more effective interventions. DST draws attention to the interaction among an individual, the environment, and the task which formulates different movements (Kugler et al., 1982; Thelen & Ulrich, 1991). In so doing, this perspective contrasts sharply with the medical model of disability, which requires an individualized medical solution to remediate the effects of disability such as CHARGE syndrome (Areheart, 2008).
DST identifies individual, environmental, and task factors that can either encourage or impede movement (Newell, 1984). This ecological model broadly refers to these factors as “constraints” (Newell, 1984, p. 105). Constraints that encourage development and behavioral motor change are termed “affordances” (Gibson, 1977, p. 67). Increased muscular strength, confidence, flexibility, and practice opportunities in variable real-world environments have been identified as affordances in relation to independent walking (Adolph et al., 2018). Alternatively, constraints that impede or delay development are termed “rate limiters” (Thelen, 1998, p. 271). For example, poor lighting or uneven surfaces may operate as rate limiters for independent walking.
Examining affordances and rate limiters can provide valuable information on motor development interventions and adaptations that need to be made to facilitate success. Currently, no affordances have been identified by the literature pertaining to children with CHARGE syndrome. Conversely, research has identified several potential rate limiters relevant to walking, including vision loss, hearing loss, and ear abnormalities (e.g., missing semicircular canals; National Organization for Rare Disorders, 2015). Travis and Thelin (2007) opined the cause of walking delay could be vestibular abnormalities, visual deficits, or muscular hypotonicities. Infants born with CHARGE syndrome also have significant complications, such as surgeries and hospitalization, within the first 3 years of life to manage acute medical and health problems that likely result in developmental delays (Salem-Hartshorne & Jacob, 2004).
Given the relative paucity of data about the affordances and rate limiters of independent walking in children with CHARGE syndrome, a logical starting point would be to gather data from the children themselves. However, the young age and varied communication abilities of this population of interest prevented this line of inquiry. Parents of children with CHARGE syndrome can provide a rich insight into their child’s lived experiences because “the family is the center of the universe for the child with deaf blindness” (Holte et al., 2006, p. 323). Parents often assume a myriad of roles in the lives of their children and are considered experts on their child’s developmental needs (Correa-Torres & Bowen, 2016; Division for Early Childhood, 2014). They observe their child attempting a host of different tasks and in a range of environmental contexts. Moreover, early intervention services usually occur in the child’s natural home environment and are centered on the family. Understanding parental perceptions of affordances and rate limiters could inform the development of more effective interventions. This information may implicate a stronger relationship to how parents’ perceptions can positively influence provider supports and child outcomes.
Thus, the purpose of this research was to examine parent perceptions of individual, environment, and task constraints which encouraged or impeded their child’s obtainment of independent walking. The following research question guided this study: “What affordances and rate limiters of independent walking do parents identify?”
Method
This article reports the qualitative component of a larger mixed-methods study examining affordances and rate limiters of independent walking in children with CHARGE syndrome. The DST framework served as the foundation for the research design, data analysis, interpretation, and coding schemas (Evans et al., 2011; Miles et al., 2014; Sandelowski, 2010).
Participants
Due to this low incidence disability and the unique demands of the research question, purposeful sampling was used to recruit participants. The primary investigator partnered with the CHARGE Syndrome Foundation, a nonprofit organization whose mission includes increasing the knowledge base surrounding CHARGE syndrome, promoting awareness of the disability, and supporting leading-edge research. The Foundation was an effective gate keeper to our population of interest and facilitated access to parents of children with CHARGE syndrome. To be included in this study, individuals had to meet the following inclusion criteria: (a) parent of a child identified with CHARGE syndrome, (b) their child with CHARGE syndrome had independently walked (i.e., five consecutive steps without any form of support) within the past 5 years, and (c) fluent in English. The reason for the 5-year range was to ensure parents remembered their child’s development of walking.
Participants were recruited via three methods: (a) information flyers distributed at the 2015 International CHARGE Syndrome Conference, (b) direct face-to-face recruitment at the same conference, and (c) email to CHARGE Syndrome Foundation members. In total, 51 individuals responded to the recruitment calls, 86% (N = 44) of whom met the inclusion criteria. All eligible participants were invited to participate in the qualitative phase of the study with 55% (N = 24) completing the interview process.
Of the 24 participants, 17% (n = 4) were fathers and 83% (n = 20) were mothers. The parents’ age ranged from 27 to 64 years (M = 38 years). Three geographical regions were represented: North America (n = 21), the Middle East (n = 2), and Australia (n = 1). No race, ethnicity, or social economic status indicators were recorded at the time of the interview. In total, 23 children were represented within this sample group, with one interview containing both the mother and the father. Overall, 43% (n = 10) of the children were females and 57% (n = 13) were males. The children were aged between 2 years 9 months and 10 years (M = 5 years). They obtained independent walking between 18 and 60 months (M = 36 months). The children represented the full range of vision and hearing loss associated with CHARGE syndrome. Additional demographic information of the sample is provided in Table 1.
Descriptive Information of Participants and Their Child with CHARGE Syndrome.
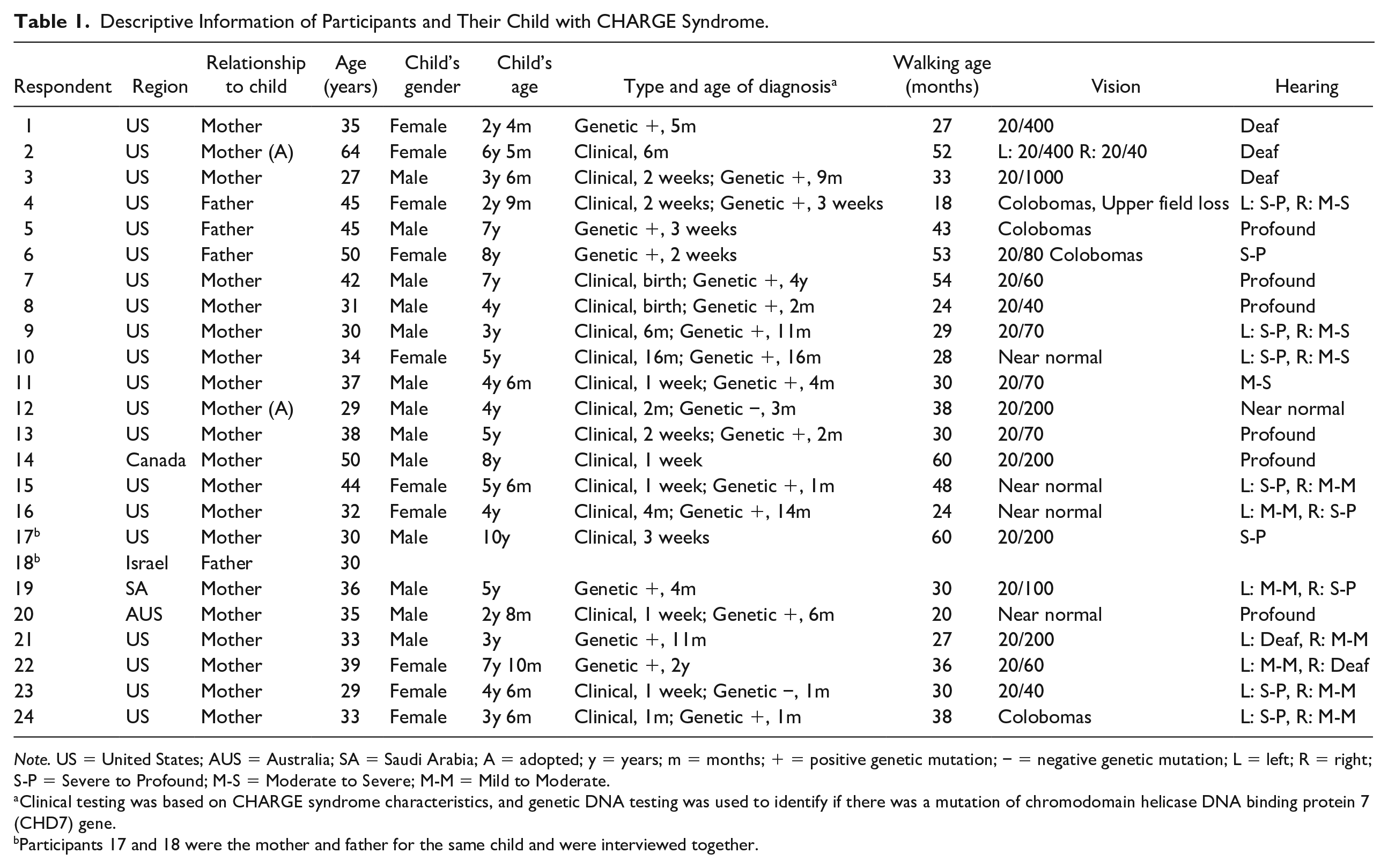
Note. US = United States; AUS = Australia; SA = Saudi Arabia; A = adopted; y = years; m = months; + = positive genetic mutation; − = negative genetic mutation; L = left; R = right; S-P = Severe to Profound; M-S = Moderate to Severe; M-M = Mild to Moderate.
Clinical testing was based on CHARGE syndrome characteristics, and genetic DNA testing was used to identify if there was a mutation of chromodomain helicase DNA binding protein 7 (CHD7) gene.
Participants 17 and 18 were the mother and father for the same child and were interviewed together.
Instrument
Semi-structured interviews were used to elicit the parents’ perceptions of affordances and rate limiters impacting their child’s capacity to walk independently. This form of data collection was chosen for three primary reasons. First, semi-structured interviews “yield rich insights into people’s biographies, experiences, opinions, values, aspirations, attitudes and feelings” in ways that quantitative surveys cannot replicate (May, 2001, p. 120). The interviewer was able to ask probing, follow-up questions where needed (Roulston, 2010). Second, semi-structured interviews allowed the participants to discuss their perceptions in their own frame of reference, rather than using terminology predetermined by the researcher. This is important in situations where terminology may vary between groups. For instance, in the motor behavior, field creeping (i.e., on hands and knees) and crawling (i.e., stomach on the floor, using forearms to pull) are different motor behaviors. Yet, for most of the general public “crawling” is used to refer to movement on hands and knees. The use of semi-structured interviews enabled the interviewer to gain clarification of the terms used and increase the validity of the data gathered. Finally, semi-structured interviews offer a space in which greater trust and rapport can be developed between participant and researcher. This interpersonal connection may assist in the communication of complex and potentially sensitive information about the child’s development that may not be accessible via quantitative methods (Correa-Torres & Bowen, 2016; Holt, 2010).
The interview guide was informed by the basic principles of DST and acted as a flexible, thematic guide to prompt discussion (see Table 2). Question one enabled participants to set the parameters of the discussion and was designed to create an open, nonthreatening entry into their experiences and observations. Drawing on their responses to question one, the follow-up questions on the guide were asked to all participants. These questions examined developmental milestone progressions, potential constraints, and the three dimensions identified by DST (individual, environmental, and task). Follow-up questions were provided to increase clarity of responses.
Semi-Structured Interview Question Protocol.
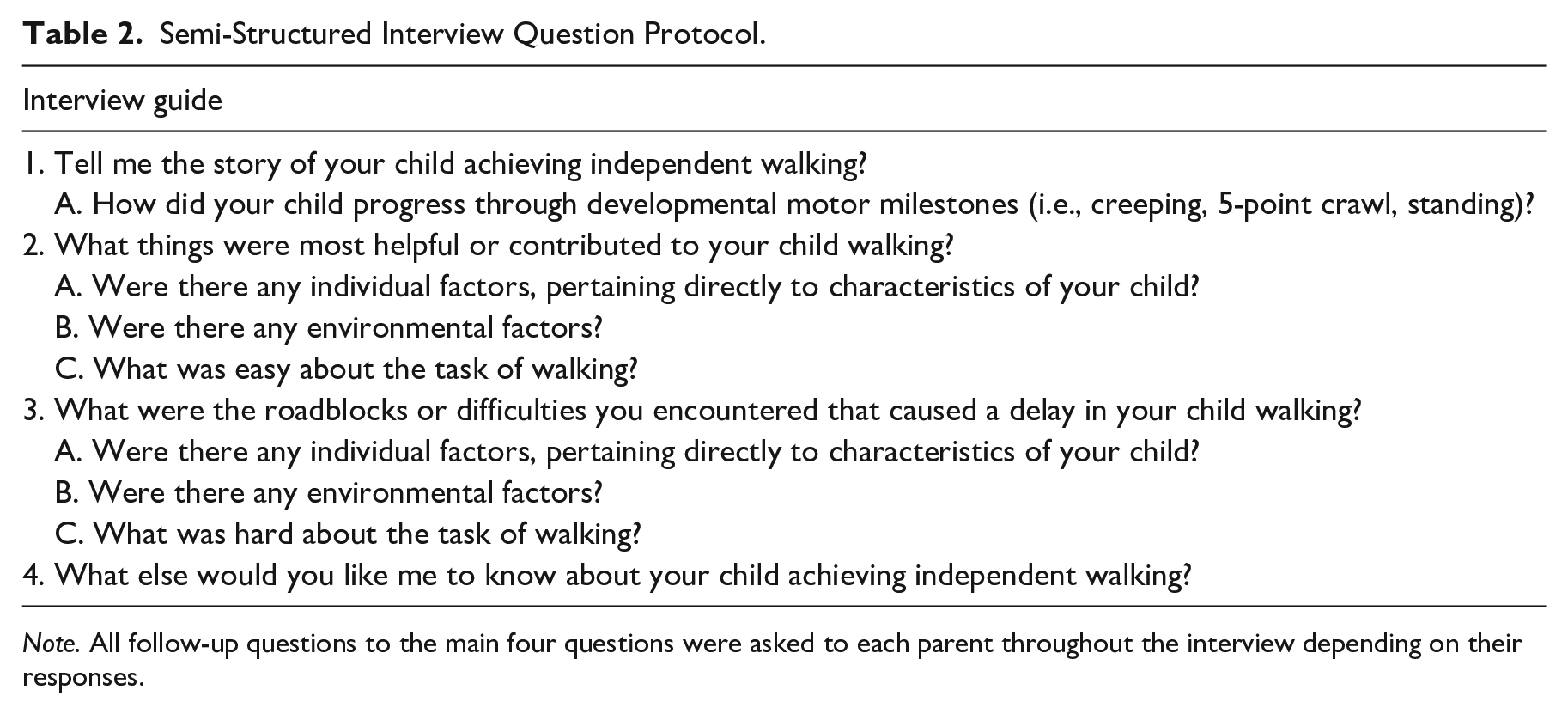
Note. All follow-up questions to the main four questions were asked to each parent throughout the interview depending on their responses.
The interview protocol questions were initially developed by the primary investigator, an expert in the field of adapted physical education. Input was sought from an external professional with expertise in qualitative research and deafblindness. Both reviewed the interview questions until an agreement was reached on whether items could comprehensively reflect the parents’ perceptions and meet the research purpose (Brod et al., 2009). Two pilot telephone interviews were conducted to further refine the interview design. The pilot participants provided feedback on the interview questions and protocol, and adjustments were made. For example, the pilot participants indicated that a visual aid of typical motor milestones would be helpful in identifying how their child may deviate from these expected patterns of development. This was subsequently included in the final protocol.
Procedure
Approval was obtained from the Institutional Review Board prior to conducting research, and all required procedures were followed. Informed consent was obtained via signed documentation. Due to the regional disparity of the participants and ease of use for the parents, telephone interviews were conducted at a time and date set by the participants (Hanna, 2012; Holt, 2010). The interview length ranged between 10 and 27 min (M = 18 min) due to parent time limitations. Each interview was audio recorded, transcribed verbatim by the primary researcher, and pseudonyms were assigned to maintain confidentiality. Field notes were also taken and analyzed in conjunction with the transcripts (Brantlinger et al., 2005).
Following recommendations from the pilot, participants received an informational packet 2 weeks prior to the scheduled interview. This packet contained the interview guide, demographic questions related to their child (e.g., age of independent walking, visual acuity, decibel loss), and the visual aid of typical developmental motor milestones. Due to the varied professional, educational, and personal histories of the participants, our pilot parents recommended that this information be provided prior to the interview. In so doing, parents could gather any relevant medical records related to visual acuity and decibel loss. Providing the interview guide in advance was also recommended as a strategy to reduce participant anxiety, build trust, and help allay any fears or concerns the parents may have in discussing sensitive material about their child.
Data Analysis
Once interviews were transcribed, and the complete transcriptions were emailed back to participants for a member check. Three participants responded to provide changes to their transcripts. Two provided additional information about their child’s development of walking and one corrected a demographic response to their child’s visual acuity. The DST framework informed the data analysis process (Evans et al., 2011; Miles et al., 2014; Sandelowski, 2010). First, the transcriptions were read several times to ensure familiarization of their content by the primary investigator. The raw data were analyzed with directed content analysis (Colorafi & Evans, 2016). The initial codes mirrored the three constraint areas identified by DST, individual, environment, and task. Prior to the second level of coding, another researcher reviewed the transcripts and conducted the same directed content analysis. Once complete, both researchers met and discussed their coding of the transcripts until an agreement was made regarding key perspectives that pertained to the individual, environment, and the task of walking.
Second, domain analysis occurred, in which conceptually similar contexts among transcripts were grouped. This second level coding process began with collating all the individual, environmental, and task codes across the interviews. Each were then examined for affordances (i.e., parental perceptions of constraints that encouraged walking) and rate limiters (i.e., constraints that impeded walking). Groups of similar codes were further examined through comparisons across parental perspectives to detect patterns both within and across participants.
The interrelationships of the categories and codes led to the development of higher-level analytic meanings, with the use of data displays through an iterative process (Miles et al., 2014). This final stage of coding resulted in examining the individual themes as being either structural or functional constraints, the environment being either physical or psychosocial, and the task being goals, rules of performance, equipment, or support. This process began with a lot of discussion between the two researchers and revisiting the theory that framed the study, which led to a deeper understanding of the information.
Findings
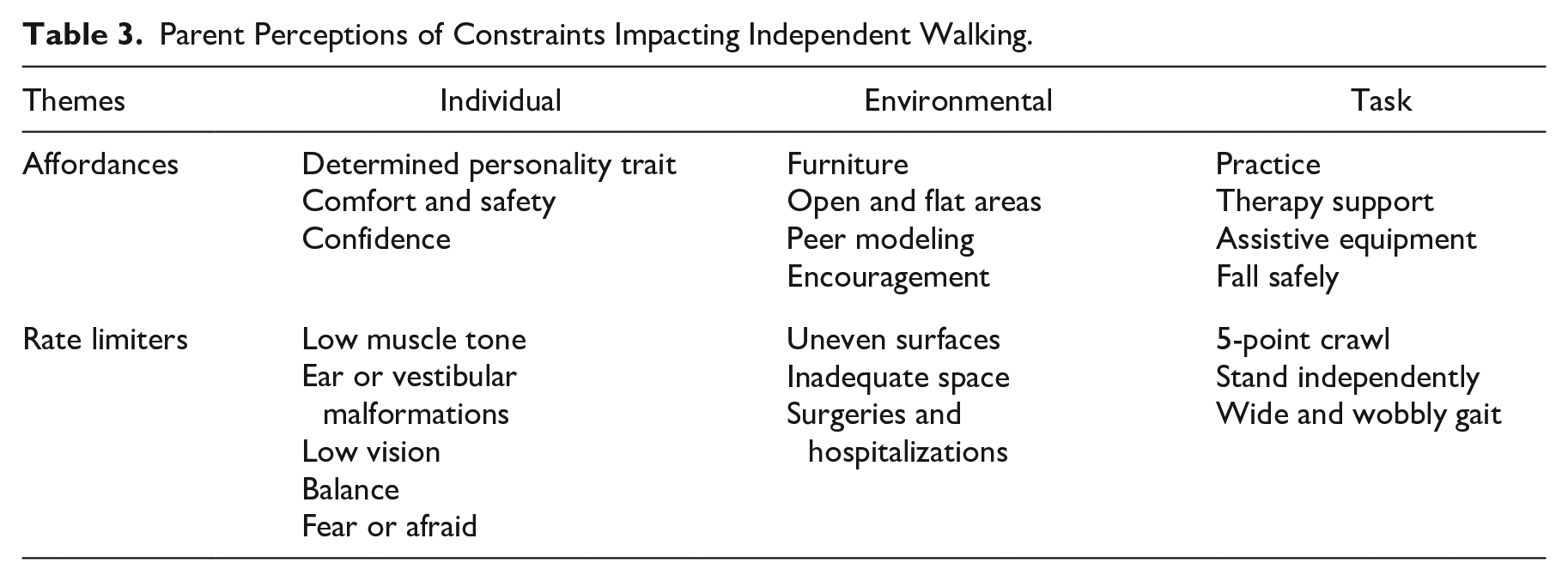
Parents provided information related to affordances and rate limiters of their child’s development of independent walking. These constraints, as situated within the DST framework are summarized in Table 3.
Parent Perceptions of Constraints Impacting Independent Walking.
Affordances
Parents of children with CHARGE syndrome identified affordances based on all three DST areas. Each will be discussed in turn.
Individual
These constraints relate to the specific child and can be further separated into two categories: structural (i.e., body structures) and functional (i.e., individual characteristics). No structural affordances were mentioned by the parents. Any mention of structural constraints appeared as rate limiters.
Parents strongly perceived functional affordances as an influential impact on the acquisition of walking independently. They reported specific personality traits which they believed assisted in their child’s attainment of walking independently and articulated their child’s determination and confidence as affordances. Several parents described their children as “fighters.” As one mother explained, “She is very determined, she practiced a ton, just very determined, she was going to walk herself so I think that was a big factor in all of the progress.” Another mother stated how her son’s determination helped him learn to walk: I think for himself, personally, he has been described this way by a number of therapist that he has a very strong agenda. If he wants to do something, he will do it. When that sort of mechanism clicked in his head, that yes, I want to get moving [independent walking], that’s really what has helped him learn so quickly. That has been quite a big thing for him.
Parents also expressed the perception that when their child felt safe and comfortable, he or she would attempt the task of walking. An increase in feelings of comfort and safety positively impacted the child’s attainment in independent walking. As one parent described, “Just until he got comfortable with that [cruising furniture] and started feeling safer, he would start walking a little bit . . . I feel like he started walking when he was comfortable and felt safe to walk.” One mother shared, “I think just working on it [walking] in her comfort zone really helped.”
Parents perceived a state of readiness or confidence that was important to the attainment of walking. One mother stated, “I think he walked when he was ready, when his balance system was ready.” Another mother stated that her child needed support until she had the confidence to walk independently, “She could pretty much walk holding onto our pinky fingers by the time she was 22 months. She didn’t have the confidence to let go.” Another mother had a similar experience that she shared as follows: He just needed that confidence with something to hold. That’s why that summer when he finally let go and walked, he was just, I can remember his face, he was just so excited that he finally made it without falling. So, I think a lot of it was the confidence.
Environmental
Parents further explained how the environment encouraged the attainment of walking. The parents described the use of furniture to assist in the development of walking. Because cruising is usually seen as a precursor to independent walking, many parents rearranged their houses to encourage movement. For example, one mother described how “he would slowly take a couple of steps after a week, when he was comfortable with that, we would move furniture a little bit more away.” Parents also reported the use of furniture to increase their child’s confidence and feeling of comfort, which increased opportunities to practice walking. One mother stated, We have a lot of furniture, which was helpful for him to be able to hold onto the furniture and take steps without being independently walking. So, he could go from couch to couch and chair and walking around the full living room without letting go of anything.
In addition to the parents manipulating the furniture within their household to encourage independent walking, parents also stated that they would travel to new flat and open areas within their community which motivated their child with CHARGE syndrome to move. Many parents responded that exploration and curiosity of the new environments stimulated movement as an affordance. As one mother described, . . . we would take her to the stores where it was bigger space and “kinda” let her run [with the assistance of a walker] around. [In] our house, we have limited space for her to run and kind of work on her [pause] endurance.
A father further explained as follows: We lived in a city so we would walk to different places holding hands with him. So, I mean, he was in an environment which walking is a basic mode of transportation . . . and if we take him to a playground, he will motivate himself to walk anywhere.
Another mother explained how they, “would take him to the mall and he would walk around with it [walker]” to gain confidence and build endurance for walking independently.
Also, peer modeling prompted the child to try to walk independently. There was a consensus among the parents that observations of another child walking had a positive impact (i.e., affordance) on their child’s motor development. Parents were particularly aware of role models who walked and ran in their child’s surrounding environment. As one mother explained, “He had brothers and he just wanted to do everything that they do. So, he is being pushed because of them; he just wants to keep up with them.” Another mother shared her perception: “What motivated her was seeing other kids, I think even to this day she wants to be like everyone else, so being around other friends and seeing them walk was motivating for her.”
Based on functional affordances, parents stated that encouragement was needed by their child. An encouraging environment increased opportunities to practice and execute independent walking. As one mother described, “It is just constant encouragement to just take one step and then two steps. Rather than it taking six weeks, it takes a year but we got there!” Another mother shared her perception: I think what helped him the most was that we just kept encouraging him and working with a physical therapist and an occupational therapist. We pushed him. It was my goal, even on all his IEPs [individualized education programs], everything is walking.
Furthermore, the encouraging environment came from family support of the therapist and each other. For example, one mother explained, “With the help, with the different strategies and support, he started walking. I can’t say really one thing, just a good team effort. We have a great team. I have the dream team.” A different father shared, “we had a good strong support system.”
Task
Throughout the interviews, parents explained the use of practice as an affordance. Practice provided children with CHARGE syndrome multiple opportunities to engage in movement, learn about their body, and strengthen their muscles. When asked about how her daughter achieved independent walking, this mother responded with, “. . . she practiced a ton!” A different mother explained, “We have seen this in so many things in her life, it’s really practice makes perfect. It is just practice takes a long time.”
Many parents described the benefits of therapy on developing independent walking. Parents reported movement gains from various therapy supports, which included physical therapy, occupational therapy, and hippotherapy (i.e., therapeutic horseback riding). One mother shared her perception as follows: I would say, first of all early intervention. The earlier the better, even though we didn’t see a lot of improvement for the first seven months that he was doing that but it was one of the main things, getting that training into him.
Another mother had a similar experience, “I think the physical therapy obviously played a ‘humongous’ role, I don’t think we could have done it without that.” Another mother shared her perspective on hippotherapy, “he started therapeutic riding, we truly believe working on that core and sitting up on the horse really helped his balance because he wasn’t walking when we started riding and then after he started riding, he started walking.”
Parents also provided their perceptions on the impact of various pieces of assistive or supportive equipment that was used to encourage walking. For instance, one mother described the benefit of her son using a walker, “I honestly feel like the walker he was in, actually got him walking sooner.” Many parents mentioned that the use of assistive equipment (e.g., walkers, gait trainers, push toys) contributed to the development of independent walking in their child with CHARGE syndrome.
However, one mother described her child’s struggle with the use of a walker. “He wouldn’t take a walker or any other type of aid that we were trying to give him to help him.” She then stated that her son with CHARGE syndrome, “. . . had a normal toy walker you see at ‘Target,’ he liked to walk with that. His physical therapist got him a medical walker but he would not use that at all.” It is important to note that the parents had to make adjustments to the assistive equipment to fit their child’s needs to provide increased opportunities to walk.
Ultimately, level of safety was a concern for many parents. Some parents explained how they taught their son or daughter with CHARGE syndrome to fall safely to the ground to increase their sense of comfort and safety. This coincided with an increase in confidence and a decrease in the fear of walking. One father discussed this process: I think as far as the independent walking, one of the good things we did was to teach her [daughter with CHARGE syndrome] how to catch herself when she fell. Because by the time she was doing assisted walking she was old enough to build up a pretty healthy fear of falling and getting hurt which was holding her up from walking independently. So, we worked on teaching her how to catch herself with her hands when she fell so she wouldn’t be quite as scared.
Rate Limiters
Parents of children with CHARGE syndrome identified rate limiters based on all three DST areas and each will be discussed in turn.
Individual
Similar to affordances, individual rate limiters were split into structural and functional. One functional rate limiter described by parents was low muscle tone. As one father described, “She has really poor muscle tone, especially core muscle tone. I think that was probably the biggest setback.” Another mother discussed her daughter’s experiences: “She is getting better every day and stronger but she still has low muscle tone.” Another mother described “. . . her low muscle tone could be a factor . . . she has low muscle tone, even now, though it has improved over time.”
Another structural rate limiter was vision loss. As one mother described, “She doesn’t see. She is usually looking up or down and it is hard to get her to notice things on the ground when she is looking forward so the vision is one of the big factors.” Another mother explained, For vision perception he has to touch the ground to know where he is, he has to put his hands down. . . . he doesn’t have terrible vision, but he can’t see a lot and I think we take for granted that some of the things he does is actually a vision issue.
Vestibular malformations were another commonly identified structural rate limiter. Parents described how their son or daughter was challenged by the loss of information obtained through the vestibular system. As one parent stated, “He doesn’t have any semi-circular canals; they are completely absent so he has no vestibular input I suppose. In his ability to walk, he had to rely on vision and proprioceptive alone.” Another father described his son had “. . . serious malformations with his cochlea and vestibular function. So he, I think, so his result [is] he has terrible sense of balance. That’s the primary thing here.”
All three of the individual structural rate limiters impacted the functional rate limiter of balance. A mother described this effect: Definitely, the balance issues, when you don’t have the equipment [semicircular canals] to have balance, I think it was a cause for delay [of walking] . . . the fact that he has [absent] semi-circular canals and balance issues, the fact that he is walking is quite a miracle.
A second mother explained the interaction of low vision and balance that impacted her daughter’s ability to walk independently, “She tracts slowly with her vision so if something was coming at her or moving to her, it throws her off balance.” One mother shared her perception that “severe balance issues made it really hard for her to achieve that milestone.” The mother further stated that her daughter “knew she was unsteady and I think that delayed her unease with her balance, maybe kind of kept her from walking sooner.” A different mother had a similar perception: “I think balance was his number one challenge.” Many parents shared that even after their child obtained independent walking, balance was still a factor. One mother stated that her child starting walking at two but “balance is a huge issue, [pause] even for him now at age four. So just trying to stand independently, fighting the whole balance issue was a challenge. That was pretty much the main only one factor.”
Parents’ perception of their child’s characteristics or functional rate limiters delayed their development of attaining walking independently. Some parents explained that their children felt fearful or afraid to walk independently: “His confidence came gradually and so that is why I think it took so long for him to actually walk. He wanted to but he was just scared.” A different mother explained how fear impacted her daughter’s development of independent walking: Mainly her fear, because at first, she was very afraid. I think she was afraid because of her vestibular system. Because things weren’t really stable for her. We knew at a certain stage that her muscles were strong enough to let her walk but she was afraid to come toward us without holding on. The reason I think it may have been because her vestibular systems weren’t well developed and she was always afraid to fall.
Another parent described how fear acted as a rate limiter: “I feel like he could have started walking well before 29 months but I just don’t think he felt safe doing it. I think he was afraid of getting hurt.”
Finally, a rate limiter not identified by the DST emerged. Tactile aversion to specific textures and not wanting to be touched was mentioned by several parents. This limited level of comfort with touch posed a restriction on how parents and service providers were able to interact and instruct the child with CHARGE syndrome. As one mother stated that her daughter “. . . did not like having anyone touch her hands, making it more difficult to help her in her journey . . .” This can be seen as a functional rate limiter very specific to children with CHARGE syndrome.
Environmental
Children with CHARGE syndrome had increased difficulties walking on uneven or non-level surfaces. As one mother stated, “Outside, uneven grass and ground even after she started walking. That was always a challenge to get her to walk outside and anywhere that wasn’t completely flat.” Another mother stated her child “doesn’t do well on any uneven ground” which impacted her ability to practice walking in various environments.
Furthermore, inadequate space was a rate limiter to the development of walking by the restriction it caused on the child’s incentive to move and the ability to explore. One mother explained the impact of their house: “The main room was very small and so for her, it was like 10 steps across the floor, it is all she could get so there was room limitations.” A different mother shared this perception: She needed space to walk around in. She didn’t have a whole lot of area that was a flat surface for her to get around so she was just stuck to one little spot. Outside, it was very difficult for her to get up by herself so she didn’t attempt it unless someone was holding her hand.
In addition, parents reported a restricted environment, such as being in a hospital for extended periods, further delayed their child’s development of walking. One mother stated, “I think one of the biggest things was that he was in the hospital for the first seven months of his life. There wasn’t a lot we could do.” Some parents identified specific medical equipment as a rate limiter, due to restricting free movement. One father explained his child’s experience: “He was in the hospital for a while just lying down so he didn’t have a chance to move around like other children. He was hospitalized so he wasn’t moving and he was connected to many machines.”
Also, surgeries that the children with CHARGE syndrome went through in their early developmental years were seen as rate limiters by parents. One mother shared their medical journey: “From birth to the time she walked alone, she had 19 surgeries, including three open heart surgeries . . .” Another mother described the following rate limiters: I just think health concerns for the first year of life for all kids with CHARGE really pushes them behind. She was born in the NICU [Neonatal Intensive Care Unit] for six months for four major surgeries, heart surgery, she has a trach [tracheostomy], feeding tube, [and] swallowing difficulties. So, when she came home at six months, she was basically a newborn and the doctors had kind of said when we do any evaluations to subtract six months off of her life because she came home as a newborn, she was going to be delayed.
Task
Parents described the 5-point crawl, difficulty standing independently, and a wide, wobbly gait as task rate limiters delaying the development of walking. A 5-point crawl is when a child’s hands, knees, and head is in contact with the ground. This form of movement is very specific to children with deafblindness and was a preferred mode of movement, portrayed by the parents in this study. One mother stated, “He turned to bulldozing, like the 5-point crawl, and head down crawling that way everywhere. We knew he would be delayed walking since he was a ‘bulldozer’ with his head down.” Another mother shared how her son was sort of stuck in development due to his 5-point preferred position: He would be in the 5-point crawl position but he didn’t move in that position. He liked to be in that position, he liked to get that feedback on his head, deep pressure on his head, looking like he was about to do a tumble. He liked to do that a lot.
For children with CHARGE syndrome, parents shared that many children learned to stand independently after they learned to walk independently, as one mother shared, “He learned to stand still after he learned to walk.” Another mother shared her perception of standing: “Another big thing that we had to work on, when he first learned how to walk, he would walk but he couldn’t stop and stand still. I didn’t realize that stopping and standing still was actually really hard work.” A mother explained how her child “has to grab onto something or he is going to fall” when he would stop walking because he could not stand still without support which is atypical to the sequence of motor milestones.
Parents also reported that their child’s gait pattern was wide and often times unstable. One mother reported that her child had a “very wide stance at first and [was] wobbling from side to side” which caused delay in developing the skill of independent walking. Another father concurred stating his child “walks with a wide stance and pretty wobbly, kind of a drunken sailor walk a little bit,” impacting his ability to continuous walk independently.
Discussion
This study posed the question, what affordances and rate limiters of independent walking do parents of children with CHARGE syndrome identify? The findings provide insight into affordances and rate limiters within the individual, task, and environment based on the DST. The individual rate limiters which impeded or delayed development of independent walking were the child’s fear, low muscle tone, ear or vestibular malformations, low vision, and difficulty with balance. Uneven surfaces, inadequate space, and hospitalization or surgeries were environmental rate limiters. Task rate limiters were using a 5-point crawl, difficulty standing independently, or a wide and wobbly gait. The individual affordances which encouraged development of independent walking were the child’s determined personality trait, confidence, and feeling safe and comfortable. Furniture, peer modeling, encouragement, and open flat areas were environmental affordances whereas practice, therapy support, assistive equipment, and falling safely were task affordances.
Historically, research investigating infant motor development has primarily focused on individual characteristics, particularly rate limiters (Areheart, 2008). This study offers an incremental contribution to the literature by broadening the scope of investigation to examine possible affordances. Investigating constraints related to independent walking using the DST conceptual framework also provided information about the relationships among the child, the environment, and constraints related to this task.
The children’s rate limiters, as perceived by parents, support the existing literature on rate limiters. The structural rate limiters, which were vision loss and vestibular malformations, reiterate previous research indicators identified as causing a motor delay and balance difficulties in children with CHARGE syndrome (Abadie et al., 2000; Travis & Thelin, 2007). Although ear and vestibular malformations were identified as structural rate limiters, the child’s actual hearing loss was not a prominent factor or theme that parents described as negatively impacting the attainment of walking. Although only reported by a few parents in this study, the researchers think it is important to note that parents perceived tactile aversion as a rate limiter impacting the development of walking and success of therapies. Tactile aversion or tactile hypersensitivity or defensiveness is very specific to individuals with CHARGE syndrome and is currently not discussed at great length in motor development literature.
Functional individual rate limiters such as fear, low muscle tone, and difficulty with balance seemed to stem from the impact of the structural rate limiters caused by CHARGE syndrome. Fear of falling and a sense of being afraid was described as a rate limiter by parents. Although commonly identified as a rate limiter in the context of elderly patients (Mortazavi et al., 2018), fewer studies have connected these fears to children with deafblindness. Such a fear appears prevalent for children with CHARGE syndrome who seem to not exhibit reflexes necessary to “catch” their fall. Parents described having to teach their child how to fall safely to decrease their fear.
In addition, within the environment, parents reported uneven surfaces and inadequate space as additional environmental rate limiters. Similar to falling, the impact of uneven surfaces has been reported to impact walking in adults with Parkinson’s disease (Xu et al., 2018) and older adults (Brookfield et al., 2017). Furthermore, due to the acute health complications with CHARGE syndrome, the effect of hospitalizations or surgeries was reported by parents to cause a delay on the development of walking due to the restrictive environment. A similar finding was also reported by Hartshorne et al. (2011).
A task rate limiter unique to CHARGE syndrome was the 5-point crawl. Parents shared that this preferred mode of mobility may have delayed their child’s ability to shift their movement pattern to being upright and walking. Abadie et al. (2000) and Coker (2013) describe how movement patterns prefer to be in a state of stability rather than instability and children at times may become “stuck” in development due to their comfort in a specific movement pattern. Task and environmental rate limiters extend our understanding of factors inhibiting children with CHARGE syndrome from meeting developmental expectations such independent walking.
We also investigated individual, task, and environmental affordances that facilitate independent walking. Parents reported that their child’s determination and confidence were affordances which assisted in their development of independent walking. Personality traits have been argued as key factors which contribute to an individual’s physical activity level (Sutin et al., 2016; Wilson & Dishman, 2015); however, these traits have not been examined in relation to motor development. Parents also reported that their child’s level of comfort and safety greatly impacted their attainment of independent walking. This can be linked to the environment, both psychosocial and physical, which can be arranged to facilitate assistance and success (Thelen & Ulrich, 1991). Parents reported the importance of peer modeling in the acquisition of independent walking which supports findings about typically developing children (Magill & Anderson, 2013). The encouraging psychosocial environment was also considered highly important by parents for positively influencing their child’s development of walking. Research has supported encouragement in motor skill development in children with and without disabilities (Valentini et al., 2017). Parents further indicated using furniture and open, flat surfaces within the physical environment promoted walking.
Within the task of walking, various therapies were reported to assist with the development of walking such as physical therapy and hippotherapy. Hippotherapy is an evidenced-based practice and therapy used to increase functional performance of the sensory, motor, and cognitive systems (American Hippotherapy Association, 2020). Furthermore, parents reported assistive devices helped in the development of walking; however, success was dependent on the child’s interests. Often these types of assistive devices were used in a trial and error approach to achieve independent walking. Therefore, providing appropriate assistive equipment that is based on the child’s preferences can be beneficial.
The parents revealed an overlap and influence of the individual, environmental, and task constraints. The complex interplay between the three constraints was apparent in the responses provided by the parents and are relative to the DST (Newell, 1984). The complex nature of these interrelated constraints made it difficult for parents to report only one main constraint having a primary impact on their child’s motor development. Although this sample of parents does not represent all families of children with CHARGE syndrome, the perceptions shared in this study provide new insights into the complexity of motor development and constraints which may impact the attainment of walking.
Limitations
Three notable limitations of this study were identified. First, the recruitment methods may have limited the participant pool to parents who are engaged in the foundation or attended the conference. There may be a difference in the experiences of parents who were not able to access those opportunities or information through being a member of the Foundation. Furthermore, the findings only represent the perceptions of the parents and not findings from other sources or stakeholders. Second, the majority of parental perceptions were from mothers predominantly located within the United States, which restricts our ability to consider factors related to cultural differences that may be important to understand based on family units. In addition, no race, ethnicity, or social economic status indicators were recorded at the time of interview. Third, the use of telephone interviews potentially limited the depth of information and nonverbal cues that are provided in face-to-face interviews. Furthermore, the telephone interviews were short in length which may have limited the amount of information obtained.
Implications for Research and Practice
Given the limited research available on the development of walking in children with CHARGE syndrome, future research should explore the impact of a more diverse sample by examining if different family structures (i.e., single parent, same-sex parents, adopted), social economic status, race, and gender impact perceptions related to walking in children with CHARGE syndrome. Parent perceptions may differ between family structures, further informing professional practice in the home setting. Because therapies are prevalent within this population, future research should expand the scope to include interviews with therapy providers to gain information about further constraints impacting the attainment of walking. An interesting second step would be to compare data between parents and service providers to determine if differences exist. As the acquisition of walking in children with CHARGE syndrome can occur during different age ranges, it would be beneficial to compare the impact of the age and gender of children with CHARGE syndrome on walking independently because experience and gender roles impact motor development.
The parents’ perceptions shared in this study inform future directions for improving services for children with CHARGE syndrome. Based on the uniqueness of each child’s constraints, educators and parents should examine and manipulate the environment and task to promote motor development because individual constraints cannot be immediately manipulated (Coker, 2013; Thelen & Ulrich, 1991). Manipulating the environment by moving furniture and toys can increase movement success and opportunities to practice (Foster et al., 2019; Foster & French, 2018). Adaptations based on the child’s preferences for an assistive device or support may increase the child’s willingness to utilize the support. Establishing a comfortable and encouraging environment which is flat and open to facilitate movement should be addressed when implementing services or practicing movement at home. Due to the instability and balance issues children with CHARGE syndrome face, proper techniques of falling safely may need to be included within services. Parents and therapists can provide opportunities to practice falling in a safe environment and assist children in the movement of their arms and body to support their fall. Also, tilting a child to the front, back, and side to side can aid in balance readjustments which may prevent falls in the future. Furthermore, services and interactions may need to be tailored to address tactile aversion by providing different textures of equipment and providing a hands-off approach.
Environmental and task adaptations can support children with CHARGE syndrome to reach their full potential of motor development and attainment of independent walking. Given that children with CHARGE syndrome often have chronic health needs that may require substantial effort, parents and professionals must work together to help improve the child’s motor development. Furthermore, we urge service providers to communicate and listen to the family and parents because they have the most influential impact on the development of their children.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Editor-in-Charge: Stacy K. Dymond