
Abstract
Children with Coloboma, Heart defects, Atresia choanae, Restricted growth, Genital hypoplasia, and Ear abnormalities (CHARGE) syndrome have many sensory impairments that can cause delays in motor development impacting physical activity, health, and quality of life. However, only one limited study has investigated motor competence in children with CHARGE syndrome. The purpose of this study was to examine differences in motor competence between children with and without CHARGE syndrome and the relationship between motor competence and age at independent walking, an important motor milestone. Thirty-three children with CHARGE syndrome and 38 typically developing peers were assessed on 13 motor skills using the Test of Gross Motor Development–Third Edition. Parents completed a demographic questionnaire about their child’s age, sex, and motor milestones. Results indicated that the children with CHARGE syndrome were significantly behind their typically developing peers for all motor skills (p < .001). Age at independent walking in children with CHARGE syndrome was significantly later than their typically developing peers (p < .001) and had significant negative correlations with all motor skills (p < .01). The results of the study demonstrate a clear need for interventions focused on improving motor competence in children with CHARGE syndrome. Intervention planning should include a multidisciplinary team of relevant service providers to ensure the individualized needs of the child are met.
Children with Coloboma, Heart defects, Atresia choanae, Restricted growth, Genital hypoplasia, and Ear abnormalities (CHARGE) syndrome are diagnosed through several identifiable genetic patterns of conditions at birth and are recognized as children with some of the most complex, multisensory impairments in the current educational environment (Pagon et al., 1981; Tegay & Yedowitz, 2009). Although quite rare, ranging between one per 10,000 and one per 15,000 live births (Deuce et al., 2012), it is the leading genetic cause of deafblindness (National Center on Deaf-Blindness, 2018). The characteristics present in each child with CHARGE syndrome can vary, and there is wide variability in the severity of each characteristic. Typically, most individuals with CHARGE syndrome are deaf and/or have varying degrees of hearing loss, and colobomas are present in at least 70% to 90% of individuals with CHARGE syndrome (National Organization for Rare Disorders, 2009). The primary etiology for most children with CHARGE syndrome involves a sensorineural hearing loss that causes damage to the eighth cranial nerve, the inner sensory mechanism, the vestibule, and/or the cochlea/semicircular canals. Sensorineural hearing loss often causes the largest impact to balance and the kinesthetic control of one’s body in space (Butterfield & Ersing, 1988). Additional findings suggest that damaged or missing vestibular organs that work in conjunction with vision exacerbate movement patterns and balance (Möller, 2011).
Medical information about individuals with CHARGE syndrome is available and abundant, yet research applicable to other professionals that work with these individuals in an education or therapeutic setting is limited (CHARGE Syndrome Foundation, 2016). The CHARGE Syndrome Foundation states that foundational physical characteristics influencing gross motor performance in individuals with CHARGE syndrome commonly include low muscle tone, visual impairments, skeletal anomalies, and vestibular dysfunction. Children with CHARGE syndrome, similar to other children with multiple disabilities, often experience teachers who lack the needed professional preparation and teaching experience to modify the physical and learning environment (Lieberman et al., 2012; Perkins et al., 2013). In addition, children with CHARGE syndrome face environmental challenges, such as prolonged hospitalizations (Hartshorne et al., 2011) and decreased opportunities for physical activity, physical education, and recreation in comparison with their peers without disabilities (Imel et al., 2020; Lane et al., 2020; Lieberman et al., 2012). Based on these research findings, it is apparent that children with CHARGE syndrome face many challenges that may limit their ability to develop fundamental motor skills needed to participate in physical activities.
Motor competence has been operationalized as an individual’s ability to consistently execute different motor acts (Henderson & Sugden, 1992), which includes fine motor skills (e.g., writing, typing, sewing) and gross motor skills (e.g., kicking, running, throwing). Research has shown that individuals with disabilities demonstrate lower levels of motor competence than their peers without disabilities (Emck et al., 2009; Hartman et al., 2011; Wagner et al., 2013). However, very little is known about motor competence in children with CHARGE syndrome (Haibach-Beach et al., 2019). Early development in infants and children with CHARGE syndrome has revealed that they walk approximately 25 months later than children without disabilities (Dammeyer, 2012). Age of walking is an important milestone in motor development as it has been negatively associated with motor competence measures such as balance, throwing, running, sliding, and kicking (Perreault et al., 2020), and it is also associated with other important developmental outcomes, such as executive function (Hartshorne et al., 2007), adaptive behaviors (Salem-Hartshorne & Jacob, 2005), and language delays (Dammeyer, 2012).
Balance is a common challenge for individuals with CHARGE syndrome (Haibach & Lieberman, 2013; Haibach-Beach et al., 2020) likely due to their sensory deficits in both vision and the vestibular system (Möller, 2011). Reduced sensory input in multiple sensory systems greatly reduces their compensatory strategies causing the maintenance of balance to be quite challenging (Assländer & Peterka, 2014). Children with CHARGE syndrome have scored significantly lower in balance measures than their peers without disabilities and these scores have been associated with their balance self-efficacy scores (Haibach & Lieberman, 2013).
Motor milestones and balance are building blocks to fundamental motor skills, such as running, sliding, and kicking, that lead to motor competence in later childhood through adulthood (Clark & Metcalfe, 2002). These fundamental motor skills are necessary to develop sport specific skills and are rudimentary in engaging in physical activity (Clark & Metcalfe, 2002). Children with low proficiency in motor competence tend to opt for a less physically active lifestyle in an attempt to avoid movement challenges (Wrotniak et al., 2006). When motor competence is low, the likelihood of physical inactivity and associated health problems (i.e., obesity) are high (Stodden et al., 2008). Physical inactivity in childhood tends to lead to physical inactivity in adolescence through adulthood (Telama, 2009). For these reasons, early experiences promoting motor skill development and, therefore, a physically activity lifestyle are critical to ensure children reach their potential for full engagement at school and in the community.
Health-related indices are particularly important now as the prevalence of overweight and obese children is rising (Hales et al., 2017) and this prevalence is even higher in children with disabilities (Augestad & Jiang, 2015; Bandini et al., 2015; Haegele & Porretta, 2015). This global epidemic is in part due to lack of adequate physical activity levels, causing increasing morbidity in youth and skyrocketing worldwide burdens (Booth et al., 2017). Children with disabilities tend to be less physically active, increasing their likelihood of poorer health indices (Augestad & Jiang, 2015; Bandini et al., 2015; Haegele & Porretta, 2015). A major underlying factor to physical activity is motor competence (Ennis, 2011). Motor competence and health and fitness indices are correlates of physical activity in children (Barnett et al., 2009; Stodden et al., 2008).
Currently, there is only one known study on motor competence in children with CHARGE syndrome, and the assessment was limited to five motor skills from the Test of Gross Motor Development–Second Edition (Ulrich, 2000): throwing, jumping, sliding, running, and kicking (Haibach-Beach et al., 2019). Participants were provided modifications as needed for sensory support including a sound source and bright-colored markers and balls. Results revealed that the children with CHARGE syndrome were behind their peers without disabilities in all skills and particularly struggled in using appropriate foot placement and adequate knee flexion during the run. Many participants also did not exhibit any of the required coordination components for the throw. The purpose of this study was to expand upon these findings by comparing motor competence between children with and without CHARGE syndrome on a full assessment of 13 fundamental motor skills using the entire Test for Gross Motor Development–Third Edition, which has been found to be valid and reliable in youth without disabilities (Webster & Ulrich, 2017) and youth with visual impairments (Brian et al., 2017). A secondary purpose was to examine the association of age of walking with each of the skills. These findings will help practitioners understand specific needs related to gross motor development for children with CHARGE syndrome and assist in the development of individualized programs to promote gross motor competence and physical activity. Promoting efficient gross motor skill development will assist children with CHARGE syndrome in engaging in typical sports, recreation, and physical activity in school and the community.
Method
Participants
To be included in the study, participants in the experimental group had to meet the following criteria: (a) diagnosed with CHARGE syndrome, (b) between the ages of 3 and 13 years old, and (c) ambulate independently (a requirement to complete the motor competence assessment). Thirty-three children with CHARGE syndrome who attended the 2019 International CHARGE syndrome Conference in Dallas, TX, met these criteria and participated in the study. Eleven of the participants were male and 22 were female. Their mean age was 6.75 years (SD = 2.57). Based upon parental report, 26 of the participants had severe to profound hearing loss and the other seven participants had mild to moderate hearing loss in one or both ears. Fifteen participants were missing their semicircular canals, 10 had partially formed semicircular canals, three had fully formed semicircular canals, and five did not report. It was also reported that 28 participants had a heart defect, 17 had choanal atresia, and 21 had restricted growth.
The control group consisted of 38 typically developing children of similar age (M = 6.97 years, SD = 2.27) and gender distribution (19 males, 19 females). A t test and chi-square analysis confirmed that the two groups did not differ significantly based on age, t(68) = −.387, p = .70, or gender, χ2(1, N = 71) = 2.01, p = .16.
Measure
Motor skills were assessed by trained researchers using the Test of Gross Motor Development–Third Edition (TGMD-3; Ulrich, 2019). The TGMD-3 has been shown to be reliable and valid in children aged 3 to 10 years, 11 months who are typically developing (Webster & Ulrich, 2017) and children up to age 18 years who are visually impaired (Brian et al., 2017). The TGMD-3 consists of 13 skills divided into two subtests: (a) locomotor skills and (b) ball skills. Locomotor skills are those that require transporting the body from one location to another (i.e., run, gallop, hop, skip, slide, jump), whereas ball skills require manipulation of an object via propulsion (i.e., overhand throw, kick, underhand roll, two-hand strike), interception (i.e., catch), or both (i.e., dribble, one-hand strike). Each skill is assessed twice based on an established list of criteria. For each attempt the observer indicates whether each criterion is met (1) or not met (0). The resulting raw score for each skill ranges from 6 to 10 points based on the number of criteria. Higher scores indicate a higher level of motor competence for the skill. Skill scores within each subtest can be combined to produce a maximum raw score of 46 points for locomotor skills and 54 points for ball skills. When the subtests are combined, a maximum gross motor score of 100 points is possible.
Procedure
The Institutional Review Board at the lead researcher’s institution approved all procedures. Assent was obtained from all participants and informed consent was obtained from each participant’s legal guardian. The children with CHARGE syndrome were assessed on site at the conference. The assessments took place in a large private room with no distractions or outside noise. Children in the control group were assessed at the lead investigator’s institution following the assessment of the children with CHARGE syndrome. The assessments took place in a large open gym on a weekend day to limit distractions and outside noise.
Prior to the TGMD-3 assessment, legal guardians completed a demographics questionnaire about their child’s age, sex, CHARGE syndrome characteristics, and motor milestones (e.g., age at independent walking). Following the questionnaire, each child was filmed on a digital recording device by a trained research assistant performing all 13 motor skills from the TGMD-3 according to the established protocol. Filming was necessary to ensure accurate and reliable scoring. Appropriate equipment modifications and communication support were provided when needed. Modifications included a beeping ball for kicking and batting, a bell ball for catching, bright cones and a sound source for the locomotor skills, and extensive demonstrations prior to each skill assessment. At times, the researcher would move alongside the participant during locomotor skills to provide aid in case the participant lost balance, to assist with communication, or to help with motivation. Communication with the participants with CHARGE syndrome ranged from using voice and demonstrations to signed English with demonstrations to American Sign Language (ASL) with interpreters when necessary. Some participants needed the signs in close proximity. Two of the researchers are fluent in ASL and could accommodate the various communication needs of the participants.
Data Analyses
Each participant’s performance on the TGMD-3 was scored independently by two members of the research team while watching the digital video recordings. Adequate interrater reliability was obtained κ = 0.88, p < .001 (Landis & Koch, 1977). Percentiles based on normative data for each subtest score were obtained using Appendix C of the TGMD-3 manual (Ulrich, 2019). Mann–Whitney U tests for skill scores, individual skill component scores, and subtest scores were conducted to examine differences in motor skill competence between the children with and without CHARGE syndrome. Independent samples t tests were used to examine differences in percentiles for locomotor and ball skill subtests between children with and without CHARGE syndrome. In addition, Spearman rank-order correlation coefficients were performed to determine the relationship between each motor skill and age at independent walking.
Results
Motor Skill Competence
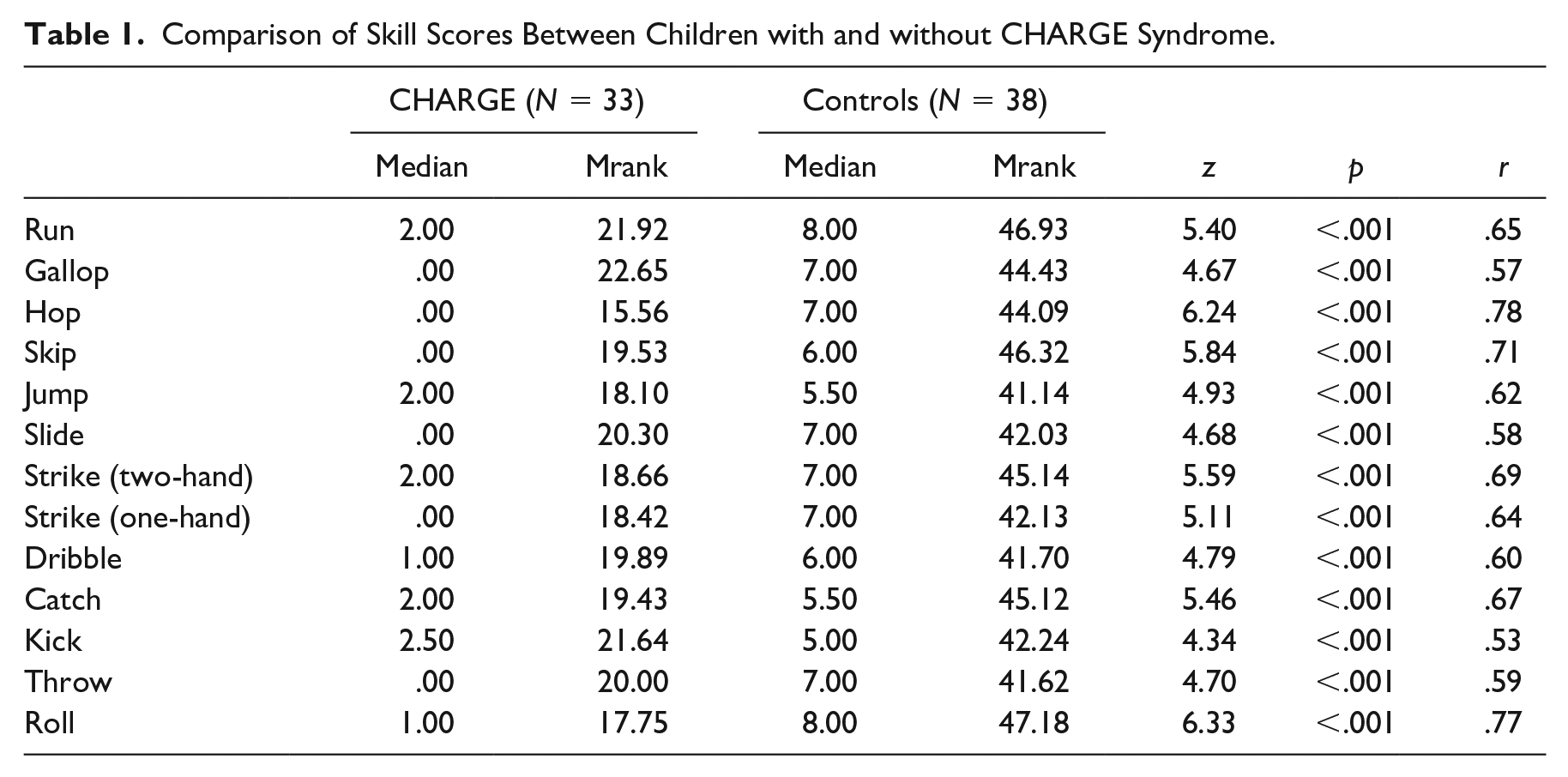
The analysis revealed that the children with CHARGE syndrome were significantly behind their typically developing peers for all 13 motor skills, p < .001 (see Table 1). The largest effect occurred for the hop (U = 53.50, p < .001, r = .78), underhand roll (U = 67.50, p < .001, r = .77), and skip (U = 121.00, p < .001, r = .71). The component analysis for each skill revealed a similar trend (p < .001). Likewise, the subtest score analysis indicated that the children with CHARGE syndrome performed significantly lower overall on locomotor (U = 60.5, p < .001, r = .78) and ball skills (U = 95.0, p < .001, r = .73) than their typically developing peers. Finally, the percentile analysis revealed that the children with CHARGE syndrome were at a significantly lower percentile for both locomotor, t(42.63) = 12.87, p < .001, and ball skills, t(62.87) = 11.55, p < .001, than their typically developing peers. The children with CHARGE syndrome had mean percentiles of 2.16 (SD = 6.81) and 8.50 (SD = 16.08) for locomotor and ball skills, respectively, whereas their typically developing peers’ mean percentiles were 60.03 (SD = 26.71) for locomotor skills and 67.13 (SD = 25.93) for ball skills. There were no gender differences in motor competence for either group across all measures.
Comparison of Skill Scores Between Children with and without CHARGE Syndrome.
Age at Independent Walking
The analysis revealed that the children with CHARGE syndrome walked significantly later (Mage = 36.71 months, SD = 17.48) than their typically developing peers (Mage = 12.52 months, SD = 1.96), t(28.7) = 7.41, p < .001. Age at independent walking had a significant negative correlation with all motor skills (r = −.47 to −.73, p < .01). The motor skills with the strongest negative correlations with age at independent walking were the underhand roll (r = −.73), hop (r = −.68), one-hand strike (r = −.68), two-hand strike (r = −.67), run (r = −.63), and skip (r = −.62).
Discussion
This study analyzed gross motor skills and age at independent walking in 33 children with CHARGE syndrome compared with 38 typically developing peers to examine differences in their motor competence. It was found that the children with CHARGE syndrome were significantly behind their typically developing peers on all 13 motor skills and began walking independently an average of 2 years later. More specifically, three motor skills with the most significant differences were the hop, underhand roll, and the skip. The locomotor skills of the hop and skip are two of the most difficult gross motor skills and require the need for sufficient balance to produce these motor movements. Haibach and Lieberman (2013) and Haibach-Beach et al. (2020) have found that children with CHARGE syndrome have limited balance ability, which can directly affect performance on locomotor skills. Furthermore, balance was reported by parents of children with CHARGE syndrome as a rate limiter impeding their child’s ability to develop independent walking (Foster et al., 2020). Thus, it is not surprising that the current study found significant negative correlations between age at independent walking and locomotor performance for the children with CHARGE syndrome.
Children with CHARGE syndrome have additional barriers, such as a variety of medical complications, that often require frequent hospitalizations, multiple surgeries, and long recoveries, which can slow and even impede with natural motor development and educational programming (Hartshorne et al., 2011; Salem-Hartshorne & Jacob, 2005). Foster et al. (2020) reported that parents of children with CHARGE syndrome perceived restricted environments, such as hospitals, and even medical equipment, as a cause for motor developmental delay in walking. Even when these children return from their medical leave, they are often excused from physical education for extended periods of time (Hilgenbrinck et al., 2020). These long absences from physical education and movement opportunities, which would typically improve their gross motor skill performance, may add to existing challenges with balance (Butterfield & Ersing, 1988; Haibach and Lieberman, 2013; Haibach-Beach et al., 2020; Perreault et al., 2020) and vestibular function (Möller, 2011) if they are not provided adapted and individualized services. These balance and vestibular challenges exacerbate the impact of the multiple surgeries and prolonged hospital stays. These barriers must be addressed to promote a strong foundation of gross motor development.
In addition to these obstacles, research has shown that physical education teachers typically do not know how to teach children with CHARGE syndrome, and therefore, children with CHARGE syndrome do not receive adequate physical education programming (Lane et al., 2020). Moreover, many children with CHARGE syndrome do not have physical education as part of their Individualized Education Program (IEP; Sorrell & Stratton, 2019) even though it has been shown that children with CHARGE syndrome benefit from appropriate placement in physical education (Lieberman et al., 2012). However, appropriate placement is often difficult to determine without a knowledgeable and collaborative interdisciplinary team (Hilgenbrinck et al., 2020). Thus, it is important that all stakeholders involved in physical education placement and programming are properly educated to ensure that children with CHARGE syndrome are provided with the best opportunities for improving their motor competence.
The results of this study illuminate the urgent need for early intervention for children with CHARGE syndrome. Early intervention on gross motor skills can promote the development of proprioception, balance, and stability (Brambring, 2006). Providing early intervention will also ensure that the child has an Individual Family Service Plan (IFSP) in place that includes gross motor skills (Houston-Wilson, 2017). This programming will help emphasize the importance of the child with CHARGE syndrome working on motor skills at home and in his or her preschool program. When goals related to motor skill development are included on the IFSP, there is a greater likelihood that they will also be included on their IEP when the child enters school (Houston-Wilson, 2017). Moreover, the interdisciplinary team will also see the goals and objectives on the IFSP and see them as valuable in the child’s overall development.
Thus, future research is needed to determine effective individualized gross motor instructional plans for early intervention as well as the feasibility of their implementation in various contexts, such as school or home. Aiding children with CHARGE syndrome in the foundational skills necessary to be active in their school and home communities will enable them to have choices in their sport and physical activity engagement.
Limitations
The current study includes some limitations. Given the low incidence and geographical distribution of CHARGE syndrome in the general population, a random sample was not a viable option. Thus, the children with CHARGE syndrome were recruited from a biannual international conference on CHARGE syndrome—a convenience sample. The conference brings in a large number of professionals and families from across the United States and other countries. Thus, the sample may not be representative of the entire CHARGE syndrome population and possibly subject to sampling error. In addition, we only included children with CHARGE syndrome who can ambulate independently in the study; thus, the findings cannot be generalized to children with CHARGE syndrome who do not meet these criteria.
Implications for Future Research
Given the limited research in this area and the convenience sample used for this study, future studies should continue to assess motor skills in children with CHARGE syndrome to have a more complete understanding of motor competence in this population. This includes recruiting participants beyond a conference setting to have a more accurate representation of this population and conducting longitudinal studies to examine changes in motor competence across time to better understand the changing needs of children with CHARGE syndrome throughout childhood and adolescence. As preliminary evidence suggests children with CHARGE syndrome are behind their typically developing peers in motor competence, it is also important to examine the feasibility and impact of interventions designed to improve motor competence in various contexts. This includes the development and piloting of interventions in homes and physical activity settings that could then be implemented on a larger scale with pre- and post-assessments to determine effectiveness in improving motor competence.
Implications for Practice
The results of this study revealed delays in all gross motor skills indicating the need for interventions that include an interdisciplinary IEP team of physical educators, adapted physical educators, special educators, and physical therapists to address the balance and movement needs of children with CHARGE syndrome to increase their level of motor competence. This study also illuminates the need to train the early childhood interdisciplinary team to promote motor skills in children with CHARGE syndrome. Research has shown that physical education teachers of children with CHARGE syndrome do not know what to do related to promoting the acquisition of motor skills of children with CHARGE syndrome (Lane et al., 2020). This itself can be a major barrier to acquiring motor skills at an early age and for the child to build on those foundational skills.
The IEP may need to include additional time from related service providers if the child with CHARGE syndrome has experienced surgeries and prolonged hospital stays. Service providers (including special educators and therapists) can manipulate the task and environment to encourage a child with CHARGE syndrome to perform optimal movement patterns based on their individual characteristics and provide ample opportunities to practice balance and movement skills to increase their motor competence (Foster et al., 2019). For example, equipment modifications, such as a mini-trampoline, can help a child with CHARGE syndrome understand the movement pattern of hopping, the motor skill with the largest effect, while improving their balance. Moreover, the rhythmic element of skipping can be aided by providing physical cadence through coactive skipping with a peer or practitioner.
Conclusion
Children with CHARGE syndrome have many sensory deficits and environmental constraints that may impact their ability to develop motor competence at a rate similar to their typically developing peers. The current study confirmed this assertion by revealing that a sample of children with CHARGE syndrome were significantly behind a sample of peers without disabilities in 13 different fundamental motor skills. This is concerning in that fundamental motor skills serve as building blocks for context specific motor skills used in many sports and recreation activities. Without these skills, it is less likely that these individuals will participate in physical activity, which may lead to additional health problems. Thus, it is important these children receive early interventions and that gross motor skills are included in the child’s IEP.
Footnotes
Editor in Charge: Fred Spooner
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.