
Abstract
Background:
Associations between different forms of emotional distress (depression, anxiety, posttraumatic stress) and lower urinary tract symptoms (LUTS) among general populations of women are well established.
Objective:
To contribute to culturally informed clinical practice, this study examines the association between emotional distress and LUTS among Somali migrant women who have experienced female genital cutting (FGC).
Methods:
Data was analyzed from the Our body, Our health study of Somali women (n = 300; mean age, 36 years). Data were collected via audio computer-assisted self-survey between September 2021 and April 2023. The Refugee Health Screener was used to assess emotional distress (symptoms of depression, anxiety, and posttraumatic stress). LUTS items were adapted from the International Consultation on Incontinence Questionnaire-Female Lower Urinary Tract Symptoms.
Results:
In logistic regression analyses adjusting for covariates (age, education, vaginal childbirth, episiotomy, FGC type), total emotional distress was associated with greater odds of experiencing all assessed LUTS (urgency, frequency, nocturia, urgency and stress urinary incontinence, straining, bladder pain). For example, for each 1-unit increment in total emotional distress, participants’ odds of urgency increased by 10% (OR = 1.10, 95% CI = 1.05, 1.16), urgency urinary incontinence by 9% (OR = 1.09, 95% CI = 1.04, 1.14), and stress urinary incontinence by 12% (OR = 1.12, 95% CI = 1.07, 1.18).
Conclusions:
In this cross-sectional study of Somali migrant women who had experienced FGC, consistent associations were observed between emotional distress in the past month and an array of LUTS. Women who present with LUTS should be screened for emotional distress and referred for mental health services as indicated.
Keywords
Introduction
Lower urinary tract symptoms (LUTS) include urgent and/or frequent urination, urinary incontinence (UI), difficulty urinating, and bladder or urethral pain before, during, or after urination. 1 LUTS are common among women. For example, prevalence of overactive bladder (OAB), characterized by urgent and often frequent urination, with or without incontinence, 1 ranges between 15% and 33% in samples of adult women in the United States and Europe. 2 LUTS are related to reduced quality of life and more symptoms of depression and anxiety, particularly among those who experience bother or functional loss due to LUTS (e.g., avoiding activities).3–6
Some cultural practices among migrants may influence the likelihood that women experience LUTS. For example, female genital cutting (FGC) refers to any procedure involving the partial or total removal of external genitalia. 7 Type 3 FGC, infibulation, is defined as the “narrowing of the vaginal orifice with the creation of a covering seal” over the vagina. Infibulation is achieved “by cutting and appositioning the labia minora and/or the labia majora, with or without excision of the clitoris.”7,8 Long-term physical health complications of Type 3 FGC include UI, urinary tract infections (UTIs), and painful urination.9,10 In one study of women presenting with symptoms of a UTI at gynecology clinics in Khartoum, Sudan, women with FGC were more likely to be diagnosed with a UTI than women without FGC. 11 In addition, antimicrobial-resistant bacteria were more prevalent among women with than without FGC.
Of importance with respect to etiology, mental health symptoms are also prospectively linked with LUTS. Among adults, self-reported depressive symptoms are prospectively associated with self-reported incident UI,4,12–14 LUTS more broadly, 15 and persistence or progression of existing OAB, 16 UI, 17 and LUTS. 18 Similarly, anxiety symptoms are prospectively associated with self-reported incident OAB, 16 UI,19,20 and LUTS more broadly. 15 Among women, cross-sectional studies have linked posttraumatic stress to OAB, UI, nocturia, and bladder pain.16,21–25 Potential inter-related mechanisms linking mental health symptoms to LUTS include central nervous system dysregulation, particularly with respect to neurotransmitter activity,26–28 inflammation,29,30 autonomic nervous system activity, 31 hypothalamic–pituitary–adrenal axis activity, 30 and constraints on health behaviors that lead to or maintain obesity. 32
Given associations of depression, anxiety, and posttraumatic stress with LUTS, migrants from regions that have experienced strife are an important population to consider with respect to LUTS prevention and treatment. Using the Refugee Health Screener, estimates of emotional distress of any severity (mild, moderate, severe) have ranged between 11% and 77% in samples of refugees.33–37 Migrants can experience stressors in their destination country that impact mental health. Among participants in the 2014 European Social Survey, immigrants had more depressive symptoms in comparison to native-born Europeans, an association that was mediated (explained) largely by economic stressors (e.g., financial and housing difficulties), and to a lesser degree, by social and cultural stressors (e.g., low trust in others and institutions, low sense of belonging). 38 In the Somali Youth Longitudinal Study, which sampled from four cities in the United States and Canada, increases in reported experiences of discrimination over a 6-year period were associated with increases in symptoms of depression, anxiety, and posttraumatic stress. 39
Associations between FGC and mental health symptoms (e.g., anxiety, depression, and posttraumatic stress disorder) have also been observed. 40 Thus, FGC could conceivably influence the likelihood of experiencing LUTS not only through changes to women’s anatomy but also through changes to mental health. Other cultural practices of refugees and migrants may enhance the negative impact of LUTS once symptoms have developed. In one qualitative study of Moroccan and Turkish Muslim women who had migrated to the Netherlands and sought care for UI, the need to maintain a state of religious cleanliness by washing after each episode of UI was a challenge. 41
A literature review yielded no studies that have examined associations between emotional distress and LUTS among Muslim populations, including Somali migrants. In addition, no studies were identified that have examined associations between emotional distress and LUTS among women who have experienced FGC. The present study is a secondary analysis of data from the Our Body, Our Health study among Somali women living in Minnesota who have experienced FGC. Findings may inform culturally informed clinical practice, including screening and treatment for emotional distress among migrants and women who have experienced FGC.
Materials and Methods
Procedure
Three hundred Somali women were recruited to participate in a study about female circumcision, reproductive health, and sexual health. Inclusion criteria were as follows: identifying as a Somali woman (including Arab, Bantu, Oromo, and Ethiopian co-identity); being aged 18–45 years; experiencing “circumcision,” the term broadly preferred by Minnesota Somali women who have experienced FGC; ever being married; and being sexually active in the last year. Due to the inclusion criterion of experiencing FGC, all women were born outside of the United States, where FGC is illegal. Data were collected in Minneapolis, St. Paul, and seven surrounding Minnesota counties between September 2021 and April 2023. Recruitment was monitored to prevent concentration of participants from any one region or neighborhood within the region. Women were approached by Somali bilingual community recruiters in two University-affiliated family medicine clinics with large Somali patient populations, as well as community settings (e.g., apartment buildings, Somali shopping malls, community centers, resettlement agencies). Initial participants could refer up to one other individual; 47% of the study sample was recruited by participant referral. Data were collected in person via audio computer-assisted self-interviewing at a location of the participant’s choosing. Surveys could be taken in Somali or English. Participants were reimbursed $75 for participation and given an additional $30 for childcare, as needed.
IRB approval was obtained from the University of Minnesota. An 11-member community advisory board composed of Somali health professionals and community leaders met regularly to provide guidance. A cross-cultural equivalence process was utilized to translate, adapt, and develop measures.42,43
Measures
Emotional distress and appraisal of coping
Participants completed the Refugee Health Screener 15 (RHS-15).36,44 For emotional distress items, participants were asked to “indicate the degree to which the symptom has been bothersome to you over the past month.” Response options were “not at all” (coded 0), “a little bit” (coded 1), “moderately” (coded 2), “quite a bit” (coded 3), and “extremely” (coded 4). To address potential cultural differences in understanding of numerical scales, symbols of jars of beans were shown over each response, with increasing amounts of beans across responses. Consistent with past literature, a total emotional distress composite variable was created by summing across items assessing depressive, anxiety, and posttraumatic stress symptoms (α = 0.90). The 13-item total emotional distress composite is a valid screening instrument for detecting common emotional disorders.33,36 It has been validated against the Patient Health Questionnaire (PHQ-9), Generalized Anxiety Disorder (GAD-7), and Primary Care Posttraumatic Stress Disorder (PC-PTSD-4) instruments. 33 A score of 11 has been recommended as a cutoff for mild symptoms, 18 for clinically significant or moderate symptoms, and 25 for identifying individuals in need of acute or advanced care. 33 Coping appraisal (item 14) assessed beliefs about one’s general ability to cope with stress over one’s life; responses ranged from 0 (able to handle or cope with anything that comes your way) to 4 (unable to cope with anything). Responses were reverse-scored so that higher scores indicated more favorable coping appraisals.
LUTS and bother
Seven items assessing individual LUTS were adapted from the ICIQ-FLUTS. 45 Nocturia was assessed with the question, “In the last month, on average, how many times did you get up during the night to urinate?”; response options were “never” (coded 0), “1 time” (coded 1), “2 times” (coded 2), “3 times” (coded 3), and “4 or more times” (coded 4). Remaining LUTS were assessed on a sliding scale ranging from “never” (coded 0) to “always” (coded 4); each item began with the words, “in the last month, on average.” Participants were instructed to pick a number on the line, with anchors of “never” and “always.” Items assessed urgency (how often did you have a sudden need to rush to the toilet to urinate?), frequency (did you need to urinate more than every two hours during the day?), urgency incontinence (how often did you leak urine because you cannot make it to the bathroom in time?), stress incontinence (how often did you leak urine with physical activity including coughing, lifting, jumping or straining?), straining (how often did you have difficulty with starting or pushing to pee?), and bladder pain (how often did you have pain in your bladder?).
A total, continuous LUTS composite score was created by summing across items (α = 0.82; possible range 0–28). Dichotomous variables were created for each of the individual LUTS items. For nocturia, getting up “1 time” or “never” was coded as 0 (no), and all other responses were coded as 1 (yes), consistent with definitions of clinically meaningful nocturia in the broader literature. 46 For all other LUTS items, “never” was coded as 0 (no), and all other responses were coded as 1 (yes).
Bother was assessed across all items: “In the last month, how bothered were you by your urinary problems?” Response options were “not at all” (coded 1), “a little bit” (coded 2), “moderately” (coded 3), “quite a bit” (coded 4), and “extremely” (coded 5). A dichotomous variable was created by coding “not at all” as 0 (no) and all other responses as 1 (yes).
Willingness to seek treatment
Participants were asked the following questions: (1) Would you consider seeing a doctor for treatment to improve your peeing or urinary problems? (2) Would you consider surgery to improve your peeing or urinary problems? Response options for both items were “no” (coded 1) and “yes” (coded 2).
Covariates
Covariates included age, education (high school or more versus less than high school), and history of vaginal childbirth (1 or more versus 0), episiotomy (i.e., being cut downward or sideways; yes versus no), and Type 3 FGC (never; infibulated but subsequently deinfibulated; infibulated and never deinfibulated).
Analytic plan
Distributions of sample characteristics and study variables were examined. To examine associations between RHS variables (emotional distress, coping appraisal) and different outcomes, multiple logistic regression models were conducted for dichotomous outcomes (each of the seven individual LUTS items, each of the two willingness to seek treatment variables) and multiple linear regression models were conducted for outcomes treated as continuous (total LUTS composite score, bother). Emotional distress and coping appraisal were examined as predictors of LUTS, bother, and willingness to seek treatment variables in separate regression models, as coping is a separate construct from distress. Bother and willingness to seek treatment were examined as outcomes only among those who experienced any LUTS symptoms (i.e., LUTS composite score ≥1). All regression models adjusted for covariates. The willingness to seek treatment models were additionally adjusted for the total LUTS composite score and LUTS bother. For regressions of LUTS symptoms on RHS variables, analytic sample sizes ranged from 278 to 295. For regressions of LUTS bother and willingness to seek treatment on RHS variables, analytic sample sizes ranged from 188 to 214.
Results
Table 1 shows distributions of sample characteristics. Participants were aged 20–45 years (M = 36.6, SD = 5.4). Over 60% reported less than a high school education. Over 75% had experienced vaginal childbirth at least once, and 15% reported experiencing an episiotomy. While experience of some type of FGC was an inclusion criterion, nearly 36% of participants reported not experiencing Type 3 FGC, infibulation. In contrast, nearly 48% had been deinfibulated after Type 3 FGC, and nearly 17% had never been deinfibulated after Type 3 FGC. Other descriptive data showed that nearly 98% of participants had health insurance, over 63% had a household income of less than $30,000, and over 90% were married. Over half had lived in a refugee camp before coming to the United States, and over two-thirds chose to complete their survey in Somali. All participants identified their religion as Islam (not shown in table).
Distributions of Sample Characteristics and Study Variables
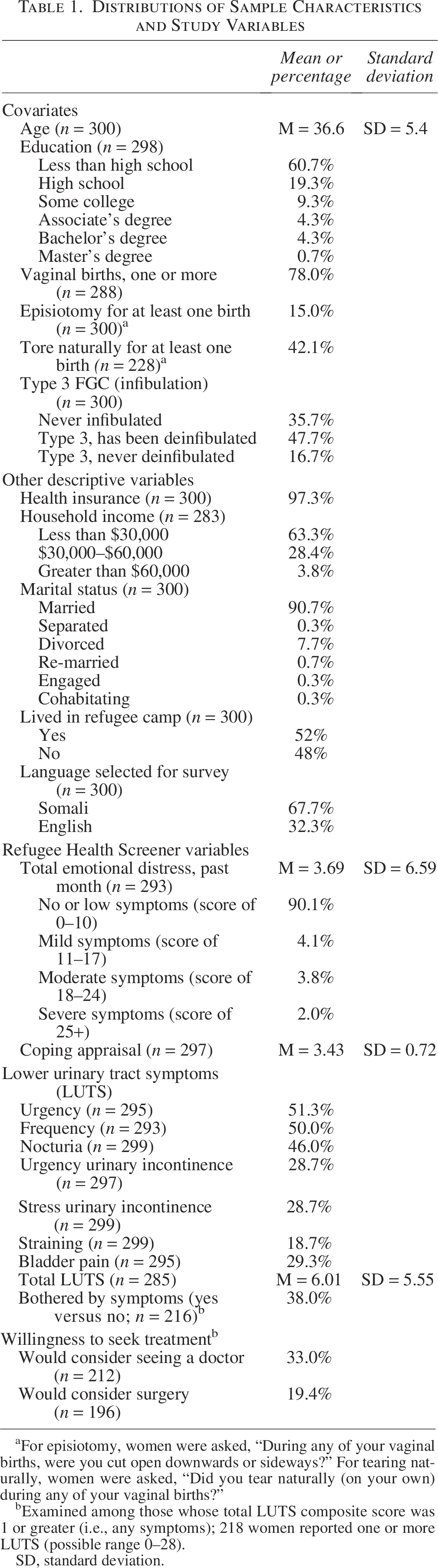
For episiotomy, women were asked, “During any of your vaginal births, were you cut open downwards or sideways?” For tearing naturally, women were asked, “Did you tear naturally (on your own) during any of your vaginal births?”
bExamined among those whose total LUTS composite score was 1 or greater (i.e., any symptoms); 218 women reported one or more LUTS (possible range 0–28).
SD, standard deviation.
Table 1 also shows that the average total emotional distress score was 3.69 (SD = 6.59; possible range, 0–52), with 90% of this community-based sample reporting scores consistent with no emotional distress symptoms or low symptoms. In contrast, roughly 4% reported mild and moderate symptoms, and 2% reported severe symptoms. Most participants reported being able to handle or cope with anything that came their way (M = 3.73, SD = 0.72; possible range, 0–4). With respect to LUTS, roughly half of the sample reported symptoms of any urgency or frequency, 46% reported nocturia, roughly 29% reported urgency UI, stress UI, or bladder pain, and nearly 19% reported straining while urinating. The average total LUTS score was 6.01 (SD = 5.55, possible range 0–28). Of the 218 participants who reported any LUTS, 38% reported any bother, 33% would consider seeing a doctor, and approximately 19% would consider surgery.
Table 2 shows regressions of individual LUTS variables on covariates and RHS variables. For the most part, covariates were not associated with individual LUTS. In comparison to participants who had never experienced Type 3 FGC, women who had experienced Type 3 FGC (infibulation) and subsequently been deinfibulated had nearly double the odds of experiencing bladder pain (OR = 1.92; 95% CI = 1.05, 3.52), and more than double the odds of experiencing urgency UI (OR = 2.47; 95% CI = 1.32, 4.60) or stress UI (OR = 2.35; 95% CI = 1.27, 4.35). Adjusting for covariates, a greater score on the continuous total emotional distress variable was associated with greater likelihood of experiencing all assessed LUTS. For example, for each 1-unit increment in total emotional distress, the odds of reporting urgency increased by 10% (OR = 1.10; 95% CI = 1.05, 1.16), urgency UI by 9% (OR = 1.09; 95% CI = 1.04, 1.14), and stress UI by 12% (OR = 1.12; 95% CI = 1.07, 1.18). Adjusting for covariates, appraisal of coping was not associated with individual LUTS variables.
Regressions of Individual Lower Urinary Tract Symptom Variables on Covariates and Refugee Health Screener Variables a
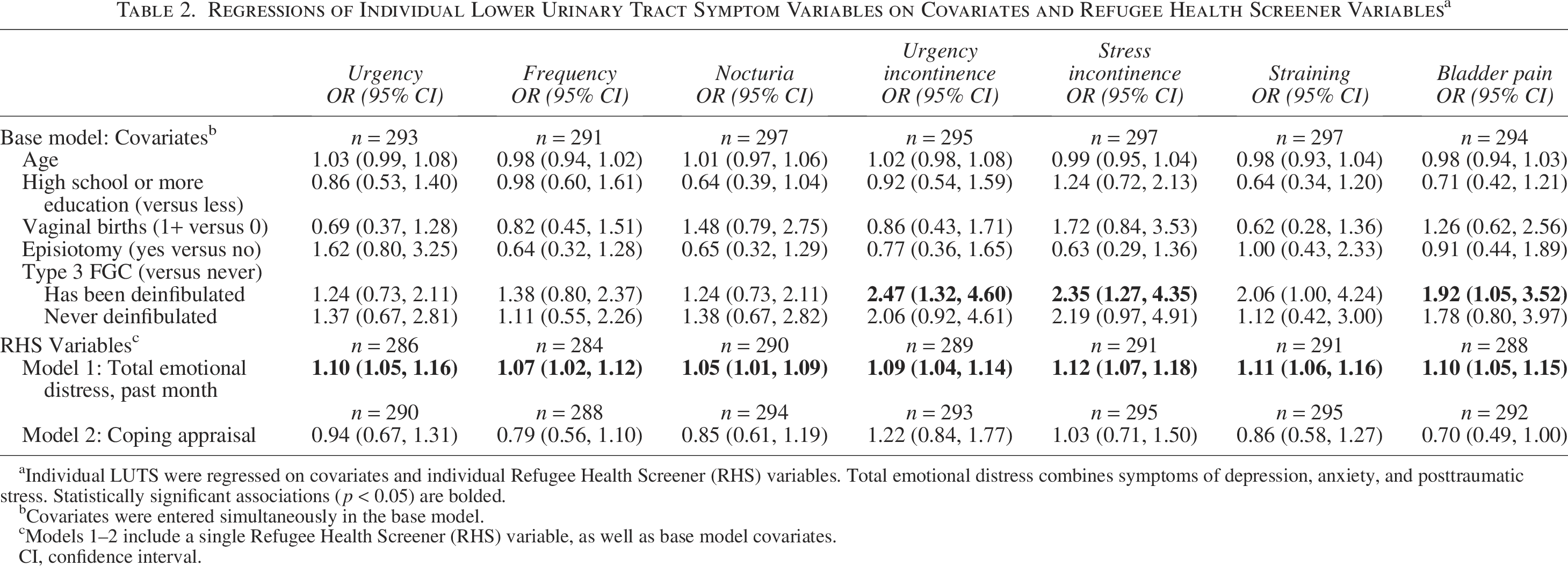
Individual LUTS were regressed on covariates and individual Refugee Health Screener (RHS) variables. Total emotional distress combines symptoms of depression, anxiety, and posttraumatic stress. Statistically significant associations (p < 0.05) are bolded.
Covariates were entered simultaneously in the base model.
Models 1–2 include a single Refugee Health Screener (RHS) variable, as well as base model covariates.
CI, confidence interval.
Table 3 shows regressions of total LUTS, bother, and willingness to seek treatment variables on covariates and RHS variables. In comparison to participants who had never experienced Type 3 FGC (never been infibulated), women who had experienced Type 3 FGC and subsequently been deinfibulated had a 2.2 times higher score on the total LUTS composite (b = 2.23, 95% CI = 0.75, 3.72). While effect sizes were in the same direction for women who had experienced infibulation and never been deinfibulated, effects were not statistically significant. Adjusting for covariates, each 1-unit increment in total emotional distress was associated with a 0.35 higher score on the total LUTS composite (b = 0.35, 95% CI = 0.26, 0.44). Among those participants with any LUTS, each 1-unit increment in total emotional distress was associated with 8% greater odds of any LUTS bother (OR = 1.08, 95% CI = 1.03, 1.13). Among those participants with any LUTS, the total LUTS score (OR = 1.11, 95% CI = 1.03, 1.21), a continuous variable, and any LUTS bother (OR = 6.92, 95% CI = 3.09,15.48), a dichotomous variable, were independently associated with greater odds of being willing to consider seeing a doctor. Similarly, total LUTS score (OR = 1.12, 95% CI = 1.03, 1.22) and any LUTS bother (OR = 5.18, 95% CI = 1.93, 13.54) were independently associated with greater odds of being willing to consider surgery. After adjustment for covariates, total LUTS, and any bother, total emotional distress was not associated with willingness to seek treatment (consider seeing a doctor or having surgery) among participants with LUTS. Adjusting for covariates, coping appraisal was not associated with total LUTS score or any LUTS bother. Adjusting for covariates, total LUTS, and any bother, each 1-unit increment in perceived ability to cope was associated with 40% lower odds of being willing to see a doctor for LUTS among those participants with LUTS (OR = 0.60; 95% CI = 0.37, 0.98); coping appraisal was not associated with willingness to consider surgery.
Regressions of Total LUTS, Bother, and Willingness to Seek Treatment Variables on Covariates and Refugee Health Screener Variables a
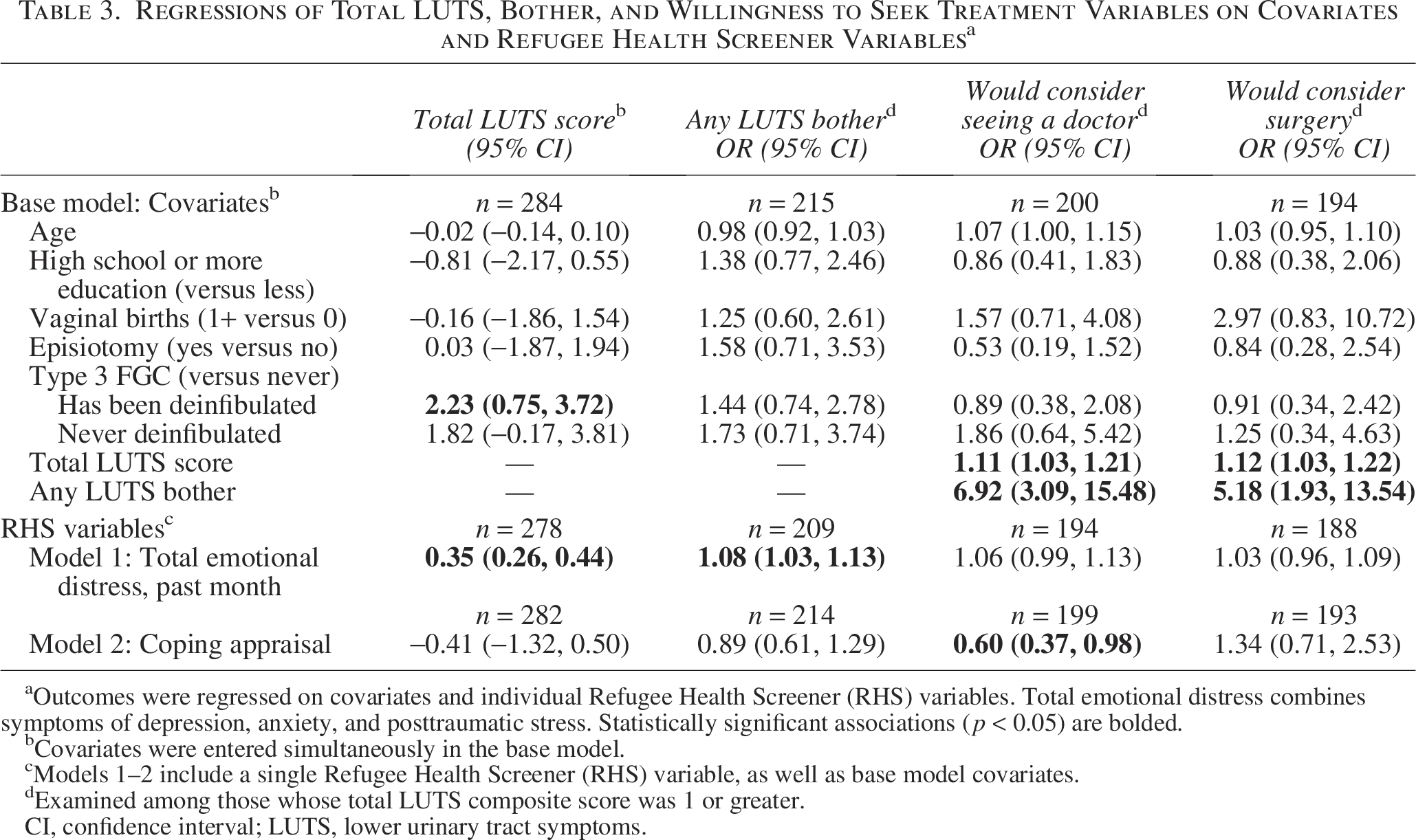
Outcomes were regressed on covariates and individual Refugee Health Screener (RHS) variables. Total emotional distress combines symptoms of depression, anxiety, and posttraumatic stress. Statistically significant associations (p < 0.05) are bolded.
Covariates were entered simultaneously in the base model.
Models 1–2 include a single Refugee Health Screener (RHS) variable, as well as base model covariates.
Examined among those whose total LUTS composite score was 1 or greater.
CI, confidence interval; LUTS, lower urinary tract symptoms.
Discussion
In this cross-sectional study of Somali migrant women in Minnesota who had experienced FGC, greater emotional distress (symptoms of depression, anxiety, and posttraumatic stress) in the past month was associated with greater odds of reporting any urgency, frequency, nocturia, urgency UI, stress UI, straining while voiding, and bladder pain in the past month, as well as report of greater frequency of overall LUTS. After adjustment for total LUTS, any LUTS bother, and other covariates, total emotional distress was not associated with willingness to seek treatment. More positive coping appraisals (i.e., evaluation of one’s ability to cope with anything that comes one’s way) were associated with lower likelihood of willingness to consider seeing a doctor for LUTS among those women with any LUTS.
Findings are consistent with studies of general populations of women showing that symptoms of depression and anxiety are associated with incident LUTS.4,12–16,19,20 However, it is possible that some symptoms of distress are a result of LUTS. 4 Indeed, the broader literature suggests that associations between affective symptoms and LUTS are bidirectional. 15 One possible mechanism that could explain associations is central nervous system dysregulation, particularly with respect to neurotransmitter activity,26–28 inflammation,29,30 autonomic nervous system activity, 31 and hypothalamic–pituitary–adrenal axis activity. 30 Central nervous system dysregulation could conceivably mediate associations of emotional distress with LUTS, or influence the development of both emotional distress and LUTS (i.e., act as a confounder). Longitudinal research with repeated assessments of emotional distress, LUTS, and biomarkers of central nervous system dysregulation is needed.
In comparison with women who had never experienced Type 3 FGC, women who had experienced Type 3 FGC (infibulation) and who had subsequently been deinfibulated had roughly twice the odds of reporting urgency UI, stress UI, and bladder pain in the past month; they also reported greater frequency of overall LUTS. Effects were not significant for women who had experienced infibulation and never been deinfibulated, potentially due to the smaller number of women in this group. Findings are consistent with the greater risk for LUTS among women who have experienced Type 3 FGC that has been observed in the broader literature.9,10
Clinical implications
Findings are consistent with studies of the association between affective symptoms and LUTS within non-Muslim populations and women who have not experienced FGC.4,12–20 To foster culturally-informed clinical practice, health practitioners should be aware of the unique ways in which LUTS may be experienced and managed among Muslim women and women who have experienced FGC. For example, the need to wash prior to Muslim ritual prayer, which occurs five times per day, may make management of UI a particular challenge. In one sample of Muslim women, washing each time that UI nullified the status of ritual cleanliness was perceived as burdensome. 41 Although Type 3 FGC is a risk factor for LUTS, there are currently no randomized controlled trials or observational studies examining whether deinfibulation improves urologic complications. 47 Health practitioners could potentially highlight other potential benefits of deinfibulation, including making it easier to cleanse one’s body and potentially prevent the growth of bacteria that may contribute to UTIs.
Screening for emotional distress is warranted among women who present with LUTS or FGC, including Somali migrants. Screening should not only take place in specialty clinics, but also in primary care clinics. Mental health services may be framed as part of maintaining overall health and well-being, as seeking mental health services may be stigmatized in some Somali migrant communities.48–50 Given the importance of religion and strong social network ties in Muslim communities,48,50 inquiring about attitudes towards seeking mental health services among religious leaders, family members, and close friends may yield useful information. When others’ attitudes are positive, practitioners could frame seeking mental health treatment as consistent with a patient’s religious teachings and culture. When others’ attitudes are not positive, practitioners could emphasize confidentiality of mental health services.
Study limitations and strengths
Study limitations include its cross-sectional design, which prevents causal inference. Adaptive behaviors to accommodate LUTS (e.g., fluid restriction, voiding without urge to avoid symptoms, use of absorbent products to manage leakage) were not assessed; such behaviors may affect perceived bother and willingness to seek treatment. In addition, this study did not assess prior or current treatment for LUTS. Study strengths include its community-based sample of Somali migrants who had experienced FGC.
Conclusions
In this cross-sectional study of Somali migrant women who had experienced FGC, strong, consistent associations were observed between emotional distress (symptoms of depression, anxiety, and posttraumatic stress) in the past month and an array of LUTS (urgency, frequency, nocturia, urgency UI, stress UI, straining while voiding, bladder pain), as well as more frequent LUTS in the past month. Women who present with LUTS should be screened for emotional distress and referred for mental health services as indicated.
Authors’ Contributions
S.S.B.: Conceptualization, visualization, writing-original draft, and writing—review and editing. R.R.-K.: Conceptualization, formal analysis, methodology, software, validation, visualization, and writing—review and editing. B.B.E.R.: Conceptualization, funding acquisition, project administration, and writing—review and editing. N.N.: Conceptualization and writing—review and editing. J.J.C.: Conceptualization, funding acquisition, project administration, data curation, validation, and writing—review and editing.
Footnotes
Acknowledgments
The authors are grateful to members of our Community Advisory Board (Salma Hussein, Salado Hassan, Safi Khalif, Nimo Said, Nimo Abdi, Sadiya Hassan, Hiba Sharif, Mahmud Kanyare, Fardoza Yusuf, Hibak Roble, Sulekha Ibrahim, Zahra Bashir, and Miski Abdulle), translators (Lucky Omaar and Abdirahman Furre), co-investigators (Cawo Abdi, Nicole Chaisson, Bernie Harlow, Crista Johnson Agbakwu, Shannon Pergament, and Michael Miner), consultants (Nicole E. Warren, Gillian Einstein), research staff (Kalthum Abdikeir, Fathi Ahmed, Muzi Chen, Yiting Li, Munira Salad, and Zahra Sheik), and our research project coordinator (Amy Ash). The authors are also grateful to the participants.
Author Disclosure Statement
The authors report no conflicts of interest.
Funding Information
Research and writing of this article were funded by the Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD) (R01 HD091685). NICHD had no role in study design; collection, analysis, and interpretation of data; writing of this article; and the decision to submit the article for publication. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Additional administrative support was provided by the Department of Family Medicine and Community Health and the Eli Coleman Institute for Sexual and Gender Health, University of Minnesota Medical School.