
Abstract
Objective:
To describe and compare current attitudes, practices, and needs in the provision of menopause care across multiple specialties.
Materials and Methods:
An anonymous survey was emailed to providers in primary care, endocrinology, and obstetrics and gynecology (OB/GYN) at Duke University and the University of Utah between January 4 and February 14, 2024.
Results:
The response rate was 18% (238/1326). Data analysis was performed on the 201 fully licensed providers who completed the survey. Most primary care physicians (PCPs) (92%, 94/102) and OB/GYNs (95%, 54/57) reported providing care for symptomatic menopause, whereas only 38% (16/42) of endocrinologists reported the same. The respondents indicated the following specialties as being responsible for the provision of menopause care at the following frequencies: 83% (166/201) primary care, 96% (193/201) OB/GYN, and 40% (81/201) endocrinology. OB/GYN providers endorsed the highest rates of confidence and understanding with menopausal hormone therapy, whereas endocrinologists endorsed the lowest rates. Most frequently reported barrier to provision of menopause care was lack of training (62%, 124/201). Most frequently reported way to improve provision of menopause care was training for providers (92%, 184/201). For primary ovarian insufficiency, only 45% (46/102) of PCPs always found it appropriate to treat with hormone therapy as compared with 82% (47/57) of OB/GYNs and 86% (36/42) of endocrinologists.
Conclusions:
Our pilot study highlights the need for enhanced provider education and the existing variations in menopause care across specialties. However, due to the study’s limited generalizability, a nationally representative study is necessary to better understand the provider-related factors influencing menopause care delivery.
Keywords
Introduction
Up to 80% of women experience symptomatic menopause, which is defined as menopause accompanied by consequent symptoms of ovarian estrogen withdrawal (e.g., vasomotor symptoms and genitourinary symptoms), often with undesirable effects on their quality of life.1–4 Furthermore, the economic impact of symptomatic menopause on a societal level is substantial, with an estimated annual loss of 1.8 billion dollars in the United States due to missed work days. 5 Despite the existence of effective treatments for symptomatic menopause, including menopausal hormone therapy (MHT) and nonhormonal prescription therapy (non-HT), these remain vastly underutilized in the clinical setting.6–8 Provider factors (e.g., specialty and education) are likely contributing to this gap between available and utilized therapies for symptomatic menopause. Health care providers’ perspectives on the current state of menopause care remain poorly understood.
Provider practices changed dramatically following publication of the landmark Women’s Health Initiative (WHI) study in 2002, which reported an increased risk for cardiovascular disease and breast cancer in women using conjugated equine estrogen and medroxyprogesterone acetate.6–10 Prescriptions for MHT subsequently declined dramatically, falling by 25–72%. 6 However, follow-up age-stratified data analyses from WHI, and other studies, have since demonstrated favorable risk-benefit profiles when MHT is used for symptom management in women under 60 years of age and within 10 years of menopause.10–13 Multiple societies have updated their guidelines to reflect these data and to inform providers that MHT remains the most effective and appropriate treatment for women experiencing symptomatic menopause with moderate-to-severe vasomotor symptoms, who lack contraindications for use.14–17 Guidelines also include non-HT treatment options as alternatives to MHT when contraindications exist, such as selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), gabapentin, fezolinetant, or oxybutynin. 18
Despite updates in clinical guidelines and understanding of menopause symptomatology, there has not been significant improvement in screening, evaluation, or treatment of symptomatic menopause. Prevalence of MHT use remains around 4.7% with low rates of MHT initiation and continuation.7,8 A national survey of 2,000 women aged 40–64 reported that 69% of women initially mistook their menopause symptoms for something else. 19 When they sought care from providers, 27% were not offered management options and 25% felt that their symptoms were dismissed. 19 Survey studies to date have explored the perspectives of providers to better understand this gap in care; however, these studies have largely focused on primary care and obstetrics and gynecology (OB/GYN) providers who already engage in menopause care on a regular basis (i.e., have at least three menopause care visits per week).20,21 To gain a comprehensive understanding of why menopause treatments are rarely prescribed in practice, it is essential to explore the perspectives of providers, regardless of whether they routinely provide menopause care.
The objective of this pilot survey study was to describe and compare current attitudes, practices, and needs in the provision of menopause care across the specialties commonly consulted by symptomatic menopausal women, including primary care (family medicine or internal medicine), endocrinology, and OB/GYN. We also aimed to identify barriers to care and potential areas for future intervention to improve the quality of care provided to women with symptomatic menopause.
Methods
The survey was designed in collaboration with a multidisciplinary provider team of five, representing two primary care physicians (PCPs), two endocrinologists, and one OB/GYN provider. The questions were created with the objective of understanding current attitudes, practices, barriers, and needs in the provision of menopause care. The questions were intentionally designed not to test knowledge, rather to assess providers’ perceptions of their own knowledge and comfort with this topic area. The provider team assessed the survey items for appropriateness of addressing the study objective and evaluated the overall length to ensure feasibility of completion. Once consensus was reached on survey content, a survey methodologist at Duke Social Science Research Institute was consulted to assist with refinement. The provider team collectively incorporated feedback on syntax and wording into a second iteration of the survey, ensuring that the original objective remained intact. The revised version was reviewed again by the survey methodologist, and subsequent revisions were incorporated into the final version of the survey. This study was approved by the institutional review boards at both Duke University (protocol 00114426) and the University of Utah (protocol 00172371).
A copy of the survey can be found in the supplementary appendix. The survey was developed on Qualtrics software, and it was emailed to providers across Duke University (n = 846) and the University of Utah (n = 480) between January 4, 2024, and February 14, 2024: 782 PCPs (n = 561 at Duke, n = 221 at Utah), 440 OB/GYN providers (n = 216 at Duke, n = 224 at Utah), and 104 endocrinologists (n = 69 at Duke, n = 35 at Utah). PCPs were defined as those practicing family medicine or internal medicine. Survey responses were collected anonymously. All respondents had the option to be redirected to another site after completion of the survey to enter a raffle ($100 at each institution).
All providers were included, regardless of whether menopause care was a regular part of their practice, as the intent of this survey was to capture the perceptions of any provider who may be encountering symptomatic menopause in clinical practice. We excluded in-training providers from data analysis (n = 23), as this is a distinct provider population that was not the target of this survey study.
Descriptive statistics were used to summarize survey data. Data from Duke University and the University of Utah were pooled to simplify the interpretation of results. Only data from completed surveys were used for analysis. The incomplete surveys (n = 14) contained primarily demographic data without substantial completion of perceptions data; thus, these surveys were excluded to prevent inappropriate representation of survey responses.
Results
The survey response rate was 20% (n = 165/846) at Duke University and 15% (n = 73/480) at the University of Utah, for a combined response rate of 18% (n = 238/1326). Out of the total 238 respondents, data analysis was performed on 201 fully licensed providers who completed the entire survey.
Approximately half of the survey respondents were PCPs (51%, n = 102/201), whereas fewer were OB/GYNs (28%, n = 57/201) and endocrinologists (21%, n = 42/201) (Table 1). Most providers were physicians by training (71%, n = 142/201), self-identified as women (78%, n = 156/201), and were in their first 10 years of independent practice (52%, n = 104/201). Among PCPs and endocrinologists, approximately a fifth of the respondents (21%, n = 30/144) reported receiving prior training focused on women’s health; however, the majority of these were PCPs, with only four endocrinologists reporting such training.
Demographic Characteristics of Survey Respondents
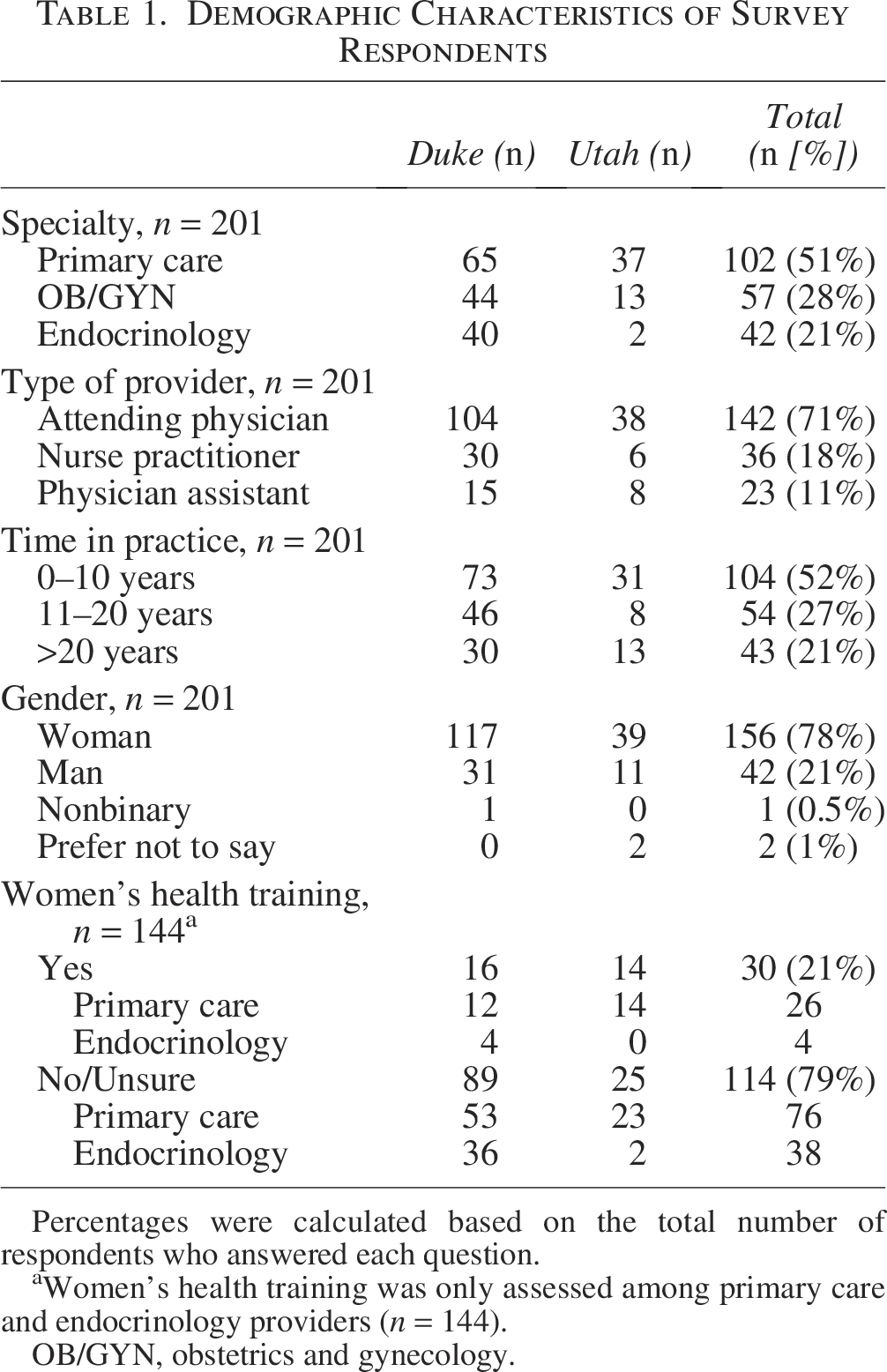
Percentages were calculated based on the total number of respondents who answered each question.
Women’s health training was only assessed among primary care and endocrinology providers (n = 144).
OB/GYN, obstetrics and gynecology.
Provision and ownership of menopause care
Provision of care
Eighty-two percent (n = 164/201) of respondents indicated that they provide care to address symptoms related to menopause, although this varied widely by provider specialty; 95% (n = 54/57) of OB/GYN, 92% (n = 94/102) of primary care, and only 38% (n = 16/42) of endocrinology providers endorsed provision of symptomatic menopause care (Table 2). Of those that endorsed providing menopause care, 85% (n = 139/164) reported prescribing MHT and 88% (n = 145/164) reported providing non-HT. As displayed in Figure 1, there were specialty differences in types of menopause care provided. Nonprescription therapy (e.g., complementary alternative medicine, cognitive behavioral therapy, and lifestyle) had lower uptake overall.
Menopause-Related Provision of Care, Symptom Screening, and Referrals
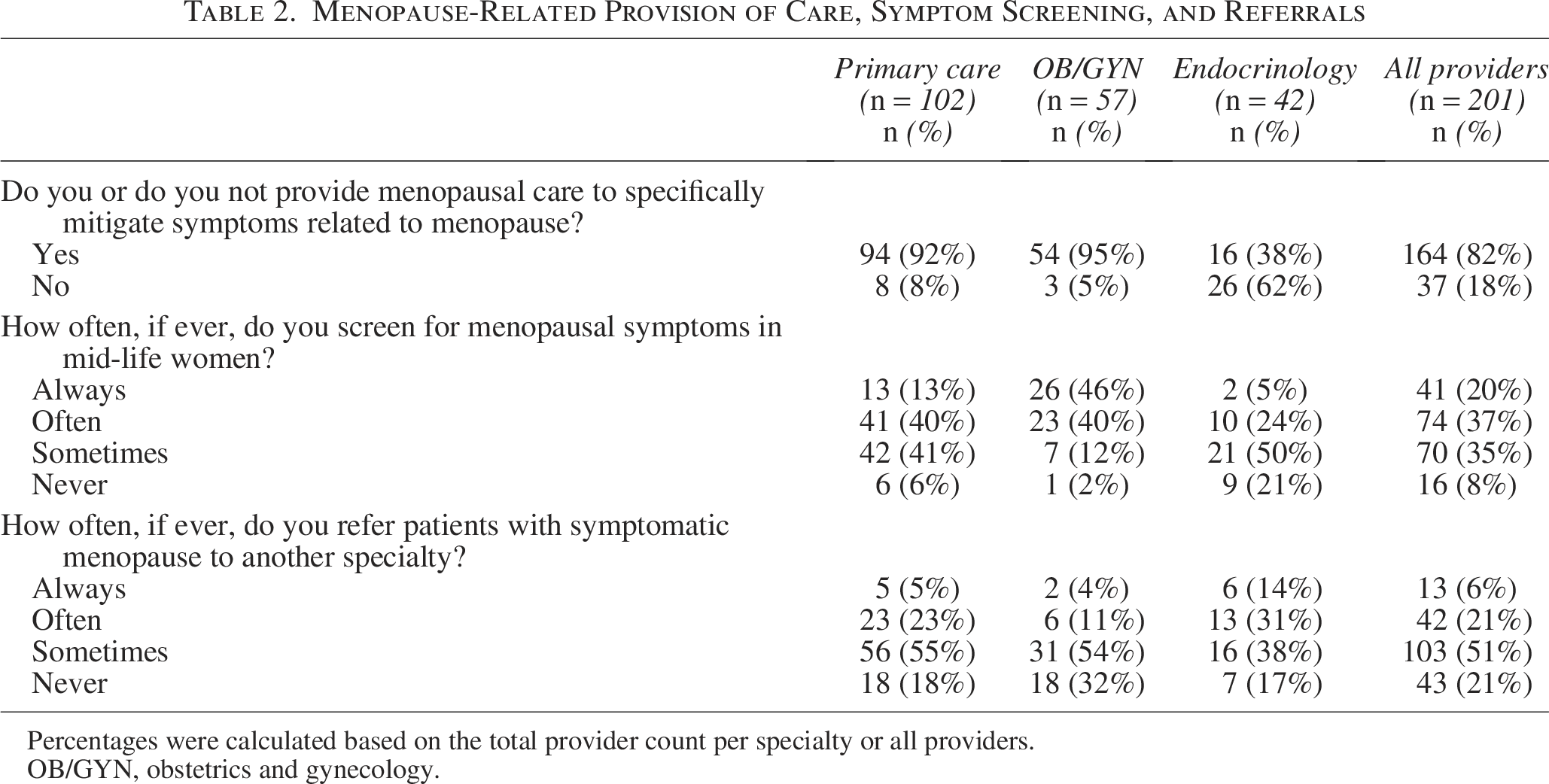
Percentages were calculated based on the total provider count per specialty or all providers.
OB/GYN, obstetrics and gynecology.
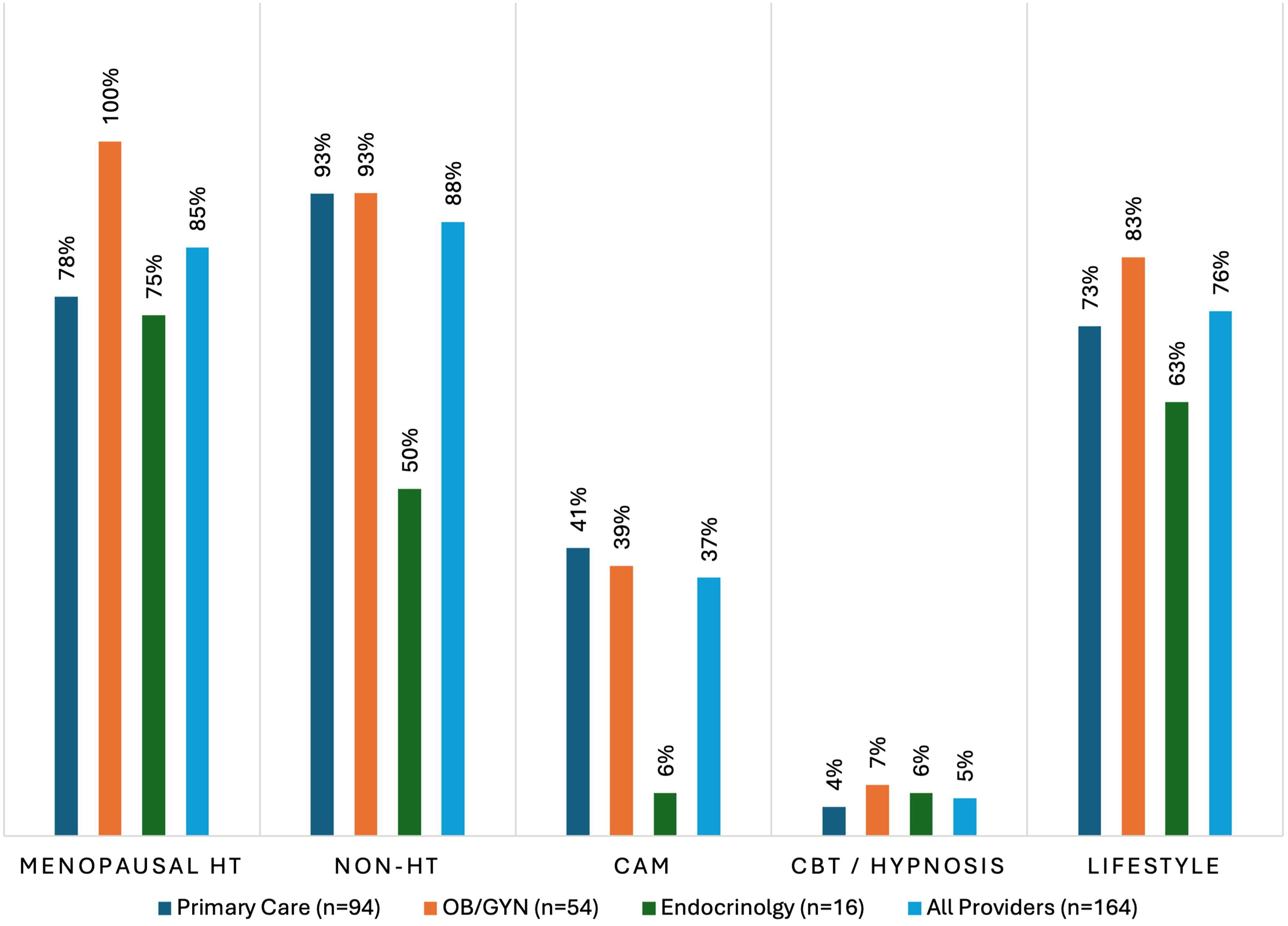
Types of symptomatic menopause care provision by specialty. Survey question: Which of the following types of care, if any, do you provide for symptomatic menopausal women? Select all that apply. This survey question was only administered to those that indicated providing menopausal care. The frequencies indicate the percent of total provider count per specialty or all providers. CAM, complementary alternative medicine; CBT, cognitive behavioral therapy; HT, hormone therapy; non-HT, non-hormonal prescription therapy; OB/GYN, obstetrics and gynecology.
Screening
When asked how often providers screen for menopausal symptoms in mid-life women, 57% (n = 115/201) of the respondents indicated always or often doing so, whereas 43% (n = 86/201) endorsed sometimes or never doing so (Table 2). Notably, there were specialty differences with 86% (n = 49/57) of OB/GYN noting that they always or often screen, whereas 53% (n = 54/102) of PCPs and 29% (n = 12/42) of endocrinologists endorsed doing the same.
Referrals for menopause
Approximately half of the respondents (51%, n = 103/201) reported that they would sometimes refer to another provider for symptomatic menopause care (Table 2). Notably, there were specialty differences with higher frequency of reported referrals from endocrinologists, followed by PCPs and the least in OB/GYN. For those who endorsed referring for symptomatic menopause, a large majority (85%, n = 135/158) reported referring to OB/GYN with far fewer providers referring to primary care (3%, n = 5/158) and endocrinology (2%, n = 3/158).
Ownership of menopause care
To determine perceived ownership of symptomatic menopause care in the provider population, they were asked to indicate which specialties were seen as being primarily responsible for providing care for symptomatic menopause. The majority of the providers indicated OB/GYN at 96% (n = 193/201) and primary care at 83% (n = 166/201) as being the primarily response; however, interestingly 40% (n = 81/201) indicated endocrinology as being a co-owner of this niche of care (Supplementary Fig. S1). Specialty stratified answers are available in the supplemental appendix (Supplementary Table S1).
Confidence and understanding of HT versus non-HT
Hormone therapy
When providers were asked to rate their confidence in prescribing or counseling for MHT, there was variable confidence as noted by Figure 2A, with almost half the providers indicating that they are very confident (24%, n = 49/201) or moderately confident (25%, n = 50/201). OB/GYNs had the largest proportion of providers indicating that they are extremely confident at 26% (n = 15/57), whereas endocrinology had the largest proportion of providers indicating that they are not at all confident at 31% (n = 13/42).
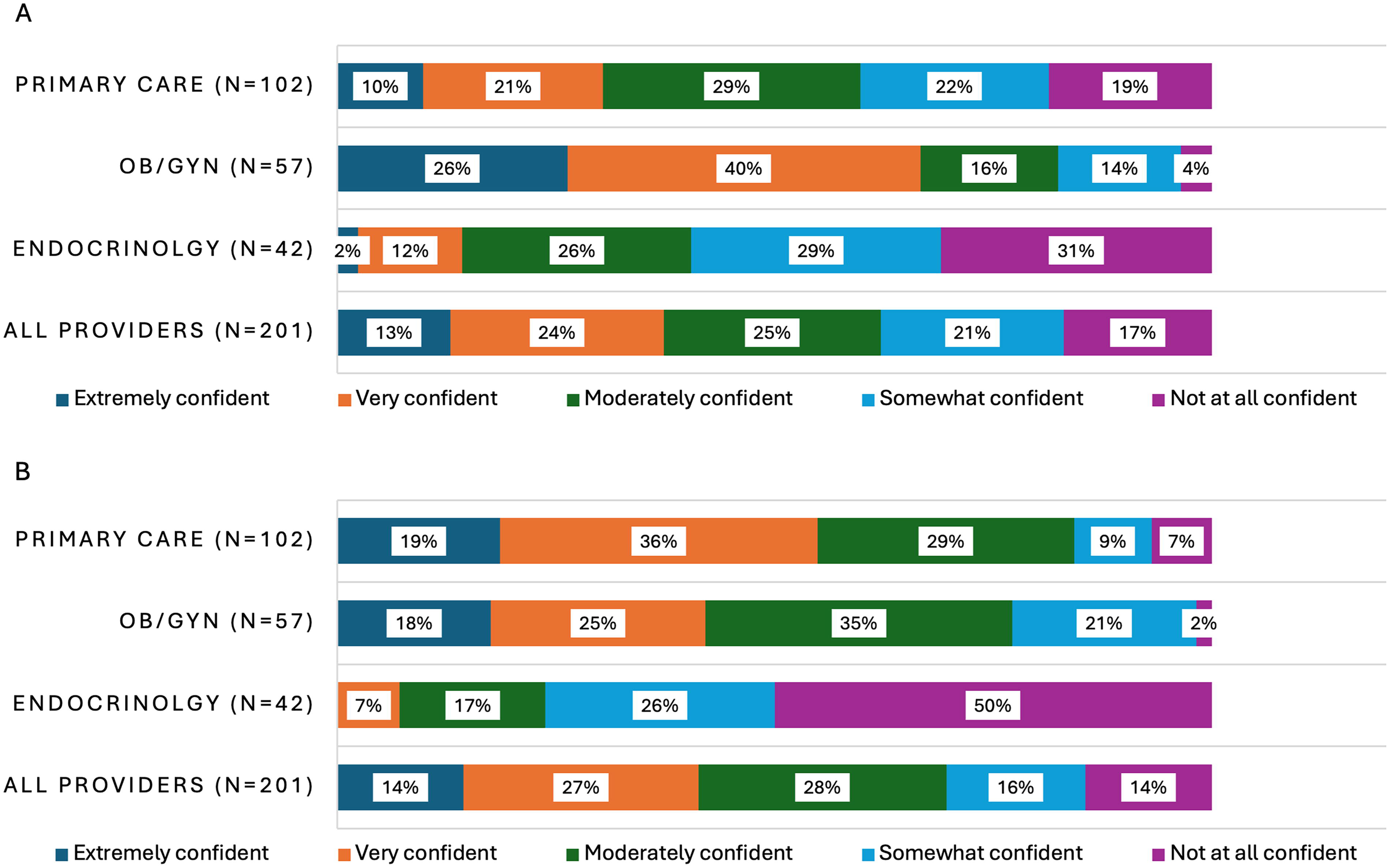
Confidence in MHT and non-HT prescribing and counseling.
When asked to rate their own understanding of risks versus benefit profile of MHT, responses varied widely, with the majority of providers indicating good (39%, n = 79/201) or average (32%, n = 65/201) understanding (Fig. 3A). Providers were also asked to rate their understanding of routes and formulations of MHT, with the majority of providers reporting good (37%, n = 74/201) or average (30%, n = 61/201) understanding (Fig. 3B). OB/GYN providers indicated the highest understanding of risks versus benefit and differing routes and formulations with 42% (n = 24/57) and 30% (n = 17/57) endorsing excellent understanding, respectively.
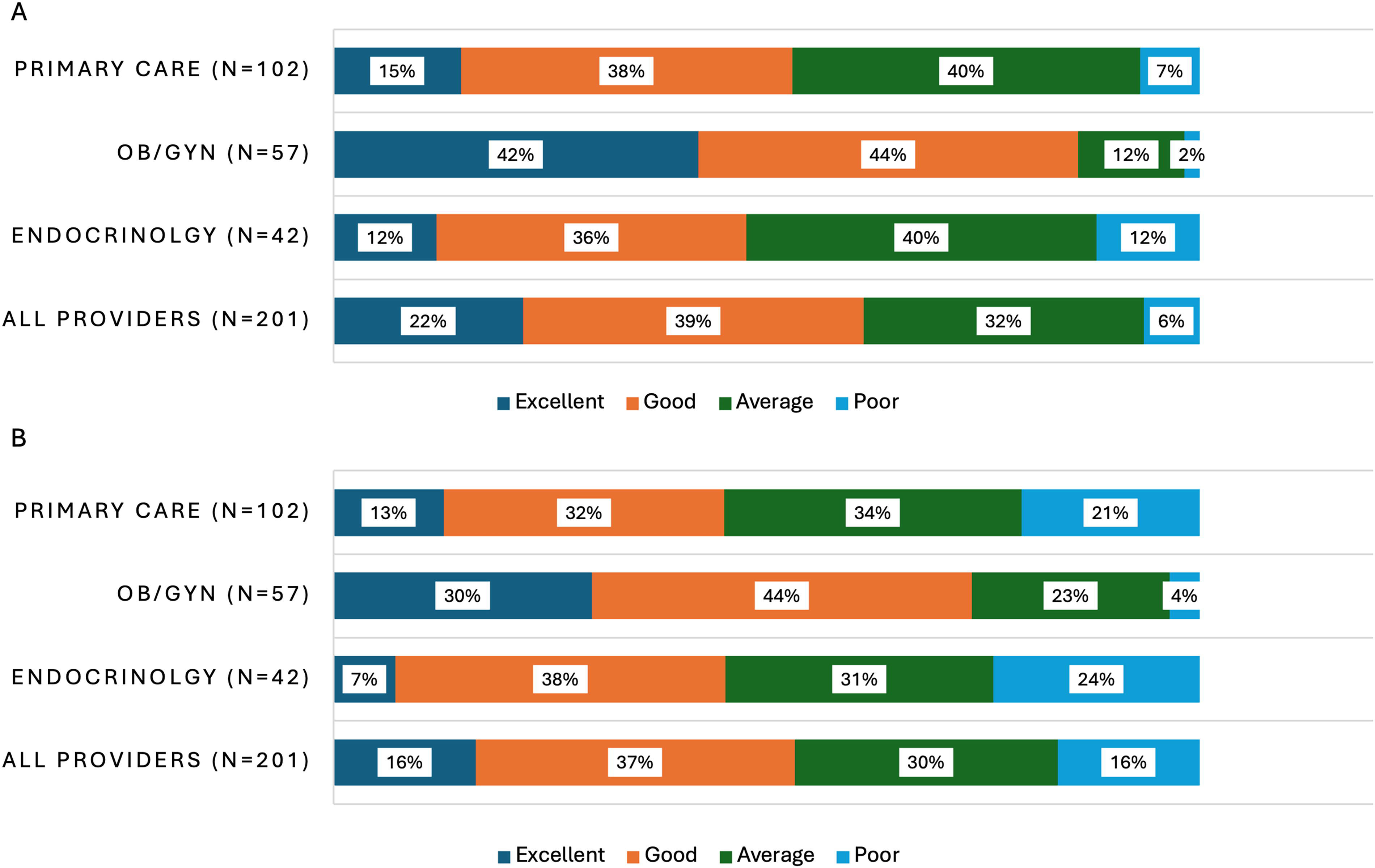
Understanding of MHT.
Confidence in MHT prescribing and counseling, understanding of risks versus benefit profile, and understanding of differing MHT routes and formulations also varied by time in clinical practice, with higher confidence and understanding observed with longer time in practice (Supplementary Figs. S2A, S3A, S3B).
Nonhormonal therapy
When providers were asked to indicate their degree of confidence in prescribing or counseling for non-HT (e.g., SSRI, SNRI, gabapentin, clonidine, oxybutynin, and fezolinetant), about half indicated that they were very (27%, n = 54/201) or moderately confident (28%, n = 57/201) (Fig. 2B). The highest confidence with non-HT was noted in primary care and the lowest confidence in endocrinology. Higher confidence was observed in those with longer time in practice (Supplemental Fig. S2B).
Barriers to and improvements in provision of menopause care
Providers were asked to indicate the barriers that they encountered in providing menopause care to women. Most frequently indicated barriers to provision of menopause care were lack of training (62%, n = 124/201), lack of time for in depth risk–benefit analysis (57%, n = 115/201), lack of clinical toolkit (e.g., algorithm and calculator) to streamline discussion (52%, n = 105/201), and patients’ safety concerns about available treatment options (52%, n = 104/201; Fig. 4A).
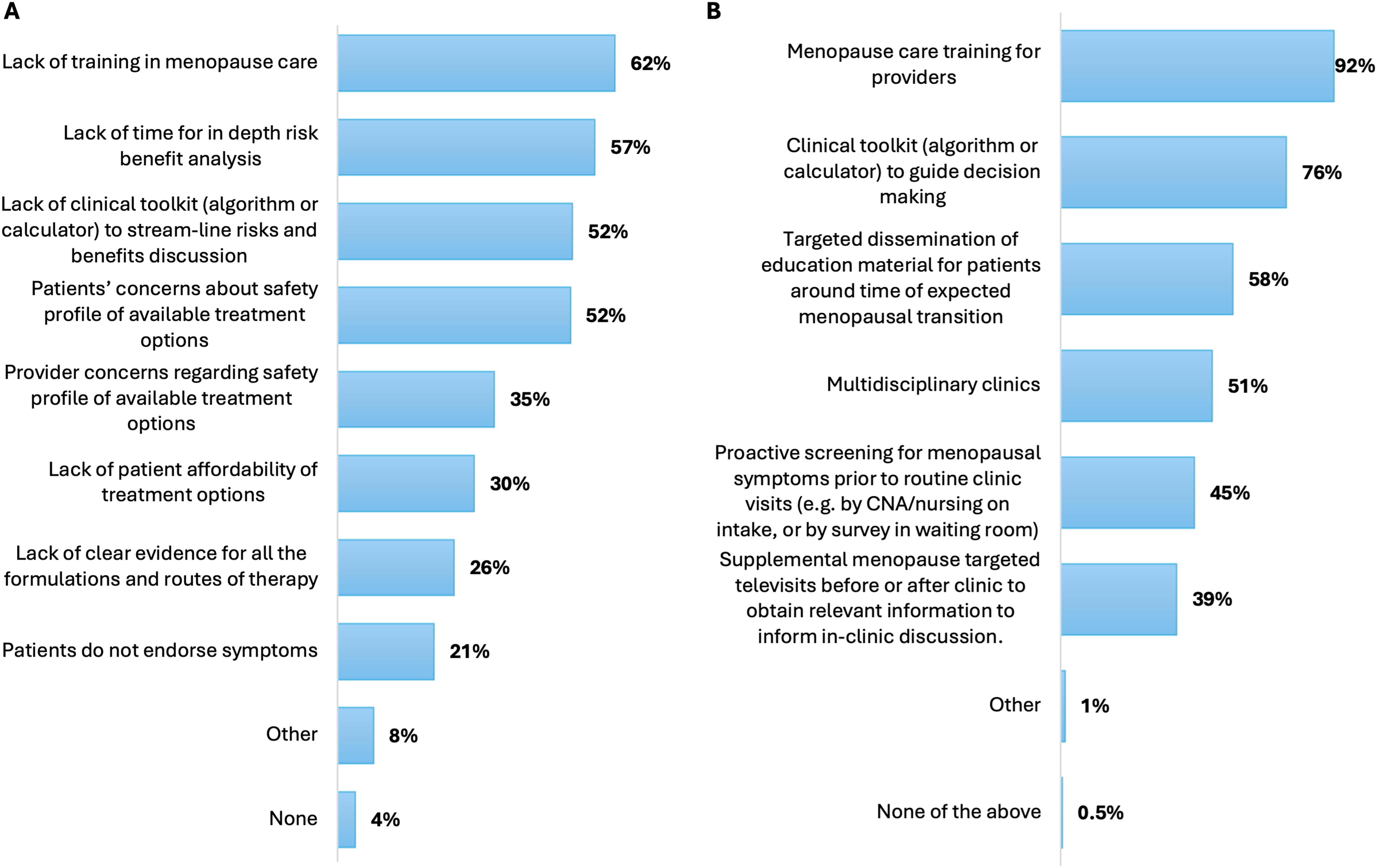
Barriers and strategies to improve menopause care.
When asked to indicate ways to effectively improve provision of menopause care to women, a large majority of the providers (92%, n = 184/201) chose menopause care training for providers. Other frequently indicated choices were clinical toolkit (e.g., algorithm and calculator) to guide decision-making (76%, n = 152/201), targeted dissemination of education material for patients around time of menopause transition (58%, n = 116/201), and multidisciplinary clinics (51%, n = 102/201; Fig. 4B).
Appropriateness of menopause care
Symptomatic menopause
Providers were asked which scenarios were appropriate to treat with MHT for symptomatic spontaneous menopause in women <60 years of age and within 10 years of menopause without any excess cardiovascular or breast cancer risk. Majority of the respondents (72%, n = 144/201) indicated that it was always appropriate or appropriate if patients have any distressing symptoms associated with menopause (Fig. 5). Notably, there were specialty-based differences in these answers with the highest proportion of providers in OB/GYN endorsing that it is always appropriate or if there are any distressing symptoms. Almost a third of PCPs (36%, n = 37/102) endorsed that it was appropriate to treat symptomatic menopause “only if symptoms are severe and interfere with quality of life.”
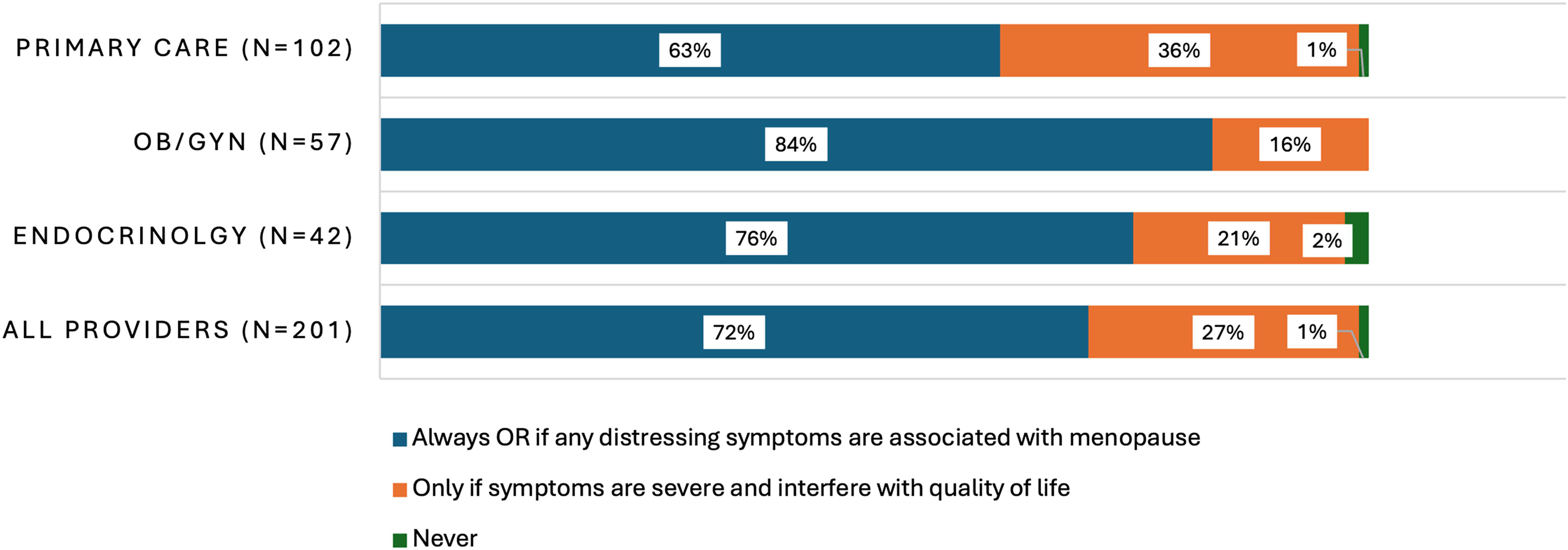
Appropriateness of symptomatic menopause treatment with hormone therapy. Survey question: Under which of the following scenarios, if any, would it be appropriate to provider would it be appropriate to provide menopausal hormone therapy for symptomatic natural menopause in women who are <60 years of age or who are <10 years past menopause and who do not have excess cardiovascular or breast cancer risk? The frequencies indicate the percent of total provider count per specialty or all providers. OB/GYN, obstetrics and gynecology.
Personal use of MHT
When asked which scenarios would lead providers to consider use of MHT for themselves (if applicable) or to recommend its use to family/friends for symptomatic menopause in a hypothetical scenario without excess cardiovascular and breast cancer risk, the majority of participants (69%, n = 138/201) indicated that it is always appropriate or appropriate if there are any distressing symptoms associated with menopause (Supplementary Fig. S4). Twenty-nine percent (n = 59/201) indicated that it is appropriate only if symptoms are severe and interfere with quality of life. Notably, there were specialty differences in responses to MHT uptake for personal use with the highest rate of uptake for personal use in OB/GYN.
Primary ovarian insufficiency
Providers were also asked in which scenarios they thought it was appropriate to use hormone therapy for primary ovarian insufficiency (POI) as a distinct entity from spontaneous menopause. There were stark specialty differences in answers to this question with endocrinology and OB/GYN indicating it is always appropriate to use hormone therapy for POI at 86% (n = 36/42) and 82% (n = 47/57), respectively, whereas only 45% (n = 46/102) of primary care indicated that it is always appropriate (Supplementary Fig. S5).
Discussion
In our pilot study of primary care, endocrinology, and OB/GYN providers conducted at two academic medical centers, we found a wide range of attitudes, practices, barriers, and needs as it relates to the provision of menopause care. Strikingly, the most frequently chosen barrier to, and means to improve, provision of menopause care was training for providers. There were clear differences in attitudes and practices related to menopause across specialties. Notably, OB/GYN providers endorsed the greatest confidence and understanding of MHT (e.g., of risks, benefits, routes, and formulations), whereas endocrinologists indicated the least. In terms of perceived ownership of menopause care, most providers indicated OB/GYN and primary care as owners of this care. Although endocrinology providers reported low frequency of menopause care provision and low comfort with MHT, over one-third of surveyed providers still considered endocrinology to share responsibility for menopause care.
Barriers and opportunities for improvement in menopause care
We found that lack of provider training was perceived to be the greatest barrier to the provision of menopause care, as well as the most important gap to address the uptake and quality of menopause care. This differs from prior provider survey studies that note patient concerns to be the most frequently identified barrier to menopause care.20,21 Differences in provider populations surveyed may be accounting for some of this discrepancy across studies. For instance, clinicians who provide menopause care on a consistent basis may be less likely to report “lack of training” as a barrier. Also, earlier surveys may not have even listed provider training as a possible barrier. A trainee survey by Kling et al. 22 noted that the majority of respondents (from 20 primary care and OB/GYN residency programs) endorsed feeling inadequate in menopause management, with comparable findings noted in two other studies.23,24 Furthermore, providers in practice for over 20 years reported greater comfort and understanding of MHT compared with those earlier in their careers. This may be reflective of routine clinical practice and training that predated the publication of the WHI findings. Collectively, these findings signal limitations in provider training related to menopause care, especially among providers who started practice in the post-WHI era.
While training was perceived to be the most effective means of improving menopause care in this study, passive training alone is unlikely to lead to lasting changes in provider behavior and clinical practices.25–27 Provider behavior is influenced by numerous factors, including individual characteristics, patient factors, and the broader community and workplace culture, among others. 27 Effective and sustainable change in provider behavior is likely to require implementation of targeted multifaceted approaches, including the use of local opinion leaders, audit and feedback, educational outreach, reminders, clinical guidelines, and economic incentives.26,28 In order for future education and training-based interventions to have the greatest impact on provider behavior, they should be interactive, contextually relevant, administered in individualized or small group settings, and followed up with posttraining engagement. 28
We also found that lack of a clinical toolkit was a frequently perceived barrier and access to such a toolkit as a commonly perceived strategy to improve menopause care. While clinical guidelines are available from multiple societies, there is no widely adopted clinical decision support tool (e.g., clinical calculator, electronic health-record integrated algorithm, and mobile app) to streamline treatment decisions for symptomatic menopause. The MenoPro app, formerly offered by the Menopause Society for providers and patients, is no longer available. 29 A provider toolkit, featuring menopause-related care algorithms in print, is endorsed by the International, British, and Australian Menopause Societies; however, there are no data on its clinical uptake. 30 To address the persistent global gap between available and utilized therapies for symptomatic menopause, a new assessment tool has been developed by Stute and colleagues to evaluate the risk-benefit ratio of MHT, although it is not yet available outside of research settings. 31 Our survey findings highlight the potential utility of decision aids in improving the provision of menopause care. However, evidence indicates that specific features are essential for these tools to be effective: integration into the clinical workflow, availability at the time and location of care, provision of actionable recommendations, and use of computer-based platforms. 32
Variation in practice across specialties
In this study, we observed substantial variation across specialties in screening frequency, comfort, and understanding of MHT. Prior studies have noted comparable specialty-dependent differences in the treatment of symptomatic menopause. For example, patients seen by OB/GYN are more likely to use MHT than those evaluated by other specialties.33,34 Primary care reported the lowest uptake of MHT for symptomatic menopause in women without clear contraindications, despite MHT being the most effective treatment for vasomotor symptoms. This is also reflected by other studies noting lower HT prescriptions and lower understanding of HT risk profile in primary care as compared with OB/GYN, despite primary care being the most frequented specialty by midlife women.33–36
In our study, there was a notable deficit in HT uptake for POI among primary care providers. The early loss of reproductive hormones in POI has deleterious cardiovascular, bone, and neurological consequences.37,38 Guidelines of the Menopause Society, the American College of Obstetricians and Gynecologists, and the Endocrine Society reflect these findings and recommend hormone replacement therapy in this population, in the absence of clear contraindications, until the average age of spontaneous menopause.14,16,39 The lack of HT prescriptions by PCPs for POI shows a clear deficit in guideline-based practice for primary care. Similar findings were noted by Kling et al., 22 with only 38.7% of the 183 surveyed trainees indicating that they would provide HT until the average age of spontaneous menopause.
This is the first survey to include endocrinologists’ perceptions of menopause care. Notably, the lowest level of comfort and understanding of MHT was endorsed by endocrinologists, which may reflect the current paucity of training, practice culture, and lack of ownership of menopause in most endocrinology settings. Although endocrinologists make up a very small proportion of the provider population, they have expertise in hormone-related disease and routinely manage conditions relevant to menopause in midlife women (e.g., osteoporosis, metabolic disease). Thus, endocrinologists are faced with multiple, likely missed, opportunities to initiate menopause care in women who are already experiencing diseases related to estrogen deficiency. Strikingly, 40% (n = 81/201) of provider respondents identified endocrinologists as co-owners of menopause care. Historically, the perspectives of endocrinologists have not been well represented in the menopause literature, and these notable findings reflect the need for change in endocrinology practice and culture.
Providers in this survey indicated OB/GYN and primary care as owners of menopause care at the highest frequencies (96% and 83%, respectively). However, as discussed above, these specialties’ attitudes and practices varied widely. OB/GYN specialty alone cannot sufficiently provide care and counseling for the majority of midlife women experiencing symptomatic menopause. Per American Medical Association physician data, one PCP is estimated to see 2,700 patients, whereas OB/GYNs have a ratio of 1:7,685 patients. 40 Given the staggering number of around 6,000 women entering menopause daily, with up to 80% experiencing symptoms related to this transition, all providers and specialties surveyed in this study should be well equipped to provide care to these women.41,42
Limitations
This pilot survey study has several limitations. Its findings may have limited external validity given its inclusion of only two academic medical centers, with no representation of community health settings. For simplicity of interpretation, the survey results were combined and analyzed together despite the potential institutional and geographical differences in provider populations. Given the voluntary nature of this study, there exist nonresponse and volunteer biases. Those who chose to respond to the survey may be uniquely different with vested interest in menopause care versus those who chose not to complete it. This may also explain the predominance of women respondents (78%), suggesting the potential for gender-based differences in perceptions.
There are several factors that may have influenced the observed survey responses from endocrinologists in this pilot survey. There was a disproportionate representation of surveyed endocrinologists (40%, n = 42/104) as compared with PCPs (13%, n = 102/782) and OB/GYN (13%, n = 57/440). In addition, academic medical centers often have endocrinologists with subspecialty expertise (e.g., bone and pituitary) who may have limited involvement in general endocrinology care. It will be important to corroborate these findings with data from broader representation of endocrinologists, particularly those practicing in community settings. Despite these limitations, this pilot study has notable strengths in capturing the perspectives of three specialties across two geographically distinct institutions. It highlights potential specialty-based variations in menopause care practices and a broader need for provider education in this area.
Conclusions
Despite new evidence, guidelines, and treatment options since WHI in 2002, we found that a large proportion of surveyed providers from two U.S. academic medical centers are not adequately equipped to deliver menopause care, with notable variations across specialties. Providers identified menopause training as the largest barrier and means to improve this niche of care. This calls for a larger representative survey of U.S. providers’ perceptions to assess current provider factors that impact the provision of menopause care. This will provide essential insights to revamp clinical training programs, practice culture, ownership of menopause care, and the creation of decision support tools that can assist providers in the provision of holistic care to midlife women experiencing symptomatic menopause.
Authors’ Contributions
A.J.: Conceptualization (equal), methodology (equal), formal analysis (lead), writing—original draft (lead), and review and editing (equal). A.-S.A.: Conceptualization (equal), methodology (equal), and writing—review and editing (equal). K.M.G.: Conceptualization (equal), methodology (equal), and writing—review and editing (equal). A.C.M.: Conceptualization (equal), methodology (equal), and writing—review and editing (equal).
Footnotes
Author Disclosure Statement
The authors declare they have no conflicts of interest.
Funding Information
This research received no specific grant from any funding agency. The corresponding author’s postdoctoral fellowship was supported by NIH T32 DK007012. A.S.A. was supported by the Duke Clinical and Translational Science Institute (award number KL2TR002554).
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.