
Abstract
Background:
Women with physical disabilities (WWPDs) have lower screening rates for cervical cancer than the general population globally. This scoping review aims to define the type of studies and content of studies currently available to promote cervical cancer screening among WWPDs. It seeks to clarify the type of disabilities WWPDs have that lead to the poorest participation in cervical cancer screening and highlight how health care systems can address the disclosed gaps.
Methods:
We developed our scoping review in compliance with the Preferred Reporting Items for Systematic Review and Meta-Analysis extension for Scoping Review. We reviewed Ovid Medline, Scopus, and REHABDATA sources with librarian-created search strategies between August 2, 2021, and September 2023.
Results:
We identified 891 articles from OVID Medline, 1,237 from Scopus, and 27 from REHABDATA for 2,155 articles. After removing duplicates and articles with exclusion criteria, 17 articles remained for full review. Their study designs were limited to cohort and cross-sectional studies. The definition of disability was either self-described or a medical diagnosis. Eighty-two percent of the studies used secondary data sources, and nearly all came from high-income countries. Cervical cancer documentation was self-reported for some and medically linked for others, but all occurred in the physician’s office. No study described the cervical cancer screening technique. The severity of disability and the increasing age of the WWPDs led to less screening.
Conclusions:
The gaps identified included the need for studies to address self-sampling for primary HPV testing for WWPDs for future increases in cervical cancer screening.
Background
People with a cervix who also have a physical disability have fewer experiences with preventive health care than with problem-oriented health care.1,2 One area of preventive care is cervical cancer prevention by human papillomavirus (HPV) vaccination and screening. HPV causes cervical cancer by infection through skin-to-skin contact of the genitals. HPV vaccination could prevent up to 7 of the 14 types that cause cervical cancer if a single dose is given in early adolescence. 3 However, there is little information on the HPV vaccination programs for people with physical disabilities.4,5
Likewise, cervical cancer screening is not globally available to all women. 6 Primary HPV testing, the most efficient screening test, is used in 25% of low-income countries, 16% of lower-middle-income countries, 35% of upper-middle-income countries, and 45% of high-income countries. Women have had a single or no screening in about 20% of the high-income countries, about 50% of upper-middle-income countries, about 90% in lower-middle-income countries, and about 97% in low-income countries. 6
One group for whom little has been done to address cervical cancer screening lapses is women with physical disabilities (WWPDs). WWPDs are sexually active before and after their disability, sometimes in non-consenting situations,7–9 putting them at the same risk as the general population for cervical cancer. In addition, physicians often lack training in how to offer accommodations for cervical cancer screening to WWPD. 9 Little known is why physicians/health care systems do not promote screening and why WWPDs do not seek screening. Our first aim is to define the type of evidence in place to inform future questions about increasing the participation rate of WWPDs for cervical cancer screening.
A challenge of this work is defining what a physical disability is. The International Classification of Functioning, Disability, and Health (ICF) 10 attempts to classify disabilities by the capacity and level of performance required to complete a task. The studies of WWPDs examining the uptake of cervical cancer screening use a wide variety of skill set rankings or self-definitions that are not easy to aggregate into homogenous categories. Our second aim is to clarify the types of physical disabilities that WWPDs have who do not participate in screening.
Lastly, the cervical cancer screening technique, age at initiation and cessation, and screening frequency differ by country and professional organizations. Our third aim is to identify the research gaps that, if addressed, may increase WWPD participation in cervical cancer screening.
Methods
We organized our scoping review in compliance with the Preferred Reporting Items for Systematic Review and Meta-Analysis extension for Scoping Review (PRISMA-ScR) (Fig. 1). 11 We initiated a scoping review process focused on interventions designed to improve cervical cancer screening rates in persons with disabilities. We developed our protocol after several iterations of review, which showed no evidence that cervical cancer incidence among WWPDs existed.

Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Diagram.
We developed the eligibility criteria using a Population, Intervention, Control, Outcomes, Study design, and Time frame (PICOST) framework. 12 We aimed to find, assess, and synthesize all articles focusing on MeSH terms, including women aged 18–65 years, with a cervix, with a physical disability, and any factors facilitating screening. If cervical cancer screening occurred in any sort, including but not limited to urine, vaginal sampling, or speculum exams/visual inspection, then we included the articles. We excluded studies if cervical cancer screening did not occur. This scoping review was necessary because studies to increase cervical cancer screening among WWPDs will depend on current practices and understanding existing influencers.
Table 1 describes the inclusion/exclusion criteria. We included all study designs that used original research with primary source data, either human or survey. We included all studies of females (including anyone with a cervix) who were aged 18–65 years, with a cervix, and with a physical disability (including but not limited to cerebral palsy [CP], spina bifida [SB], spinal cord injury [SCI], multiple sclerosis [MS], rheumatoid arthritis [RA], hemiplegia, paraplegia, quadriplegia, loss or deformity of limbs, stroke, osteogenesis imperfecta, and muscular dystrophy) were eligible for this review. We required studies to include patients with at least a 15-year lifespan. We included cervical cancer screening techniques that used urine, vagina, or cervical self-sampling; techniques with speculum exams or by visual inspection.
Inclusion/Exclusion Criteria
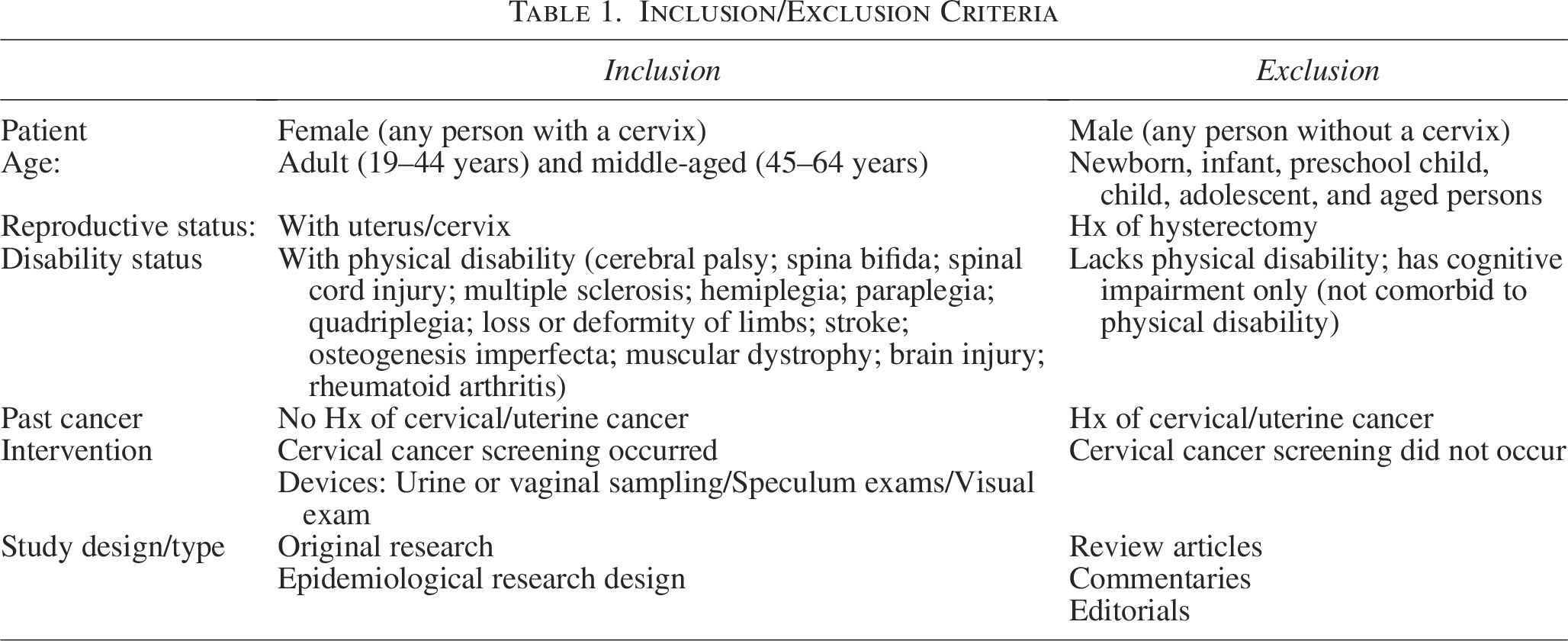
We excluded review studies. We excluded anyone with a history of cervical or uterine cancer. We excluded males (including persons assigned the gender male at birth that have never had a cervix and/or a cervix was not created), persons aged birth to 17 years, persons aged 66-end, persons with a history of hysterectomy, persons who lack a physical disability, or persons who have cognitive or learning impairments.
This scoping review did not require IRB approval because it does not collect new data from human subjects. Moreover, we only included published studies that met ethical standards and had appropriate IRB oversight.
Search strategy
The search strategy (Supplementary Appendix A1) was constructed and tested by librarians PFA and LNJ. We included the following components in the design of the search strategies: MeSH and other index terms, synonyms and concept descriptors as free text and keywords, and search filters. The primary concept groups were (1) physical disabilities and (2) cervical cancer screening, with complex concepts such as cervical cancer screening divided into multiple discovery strategies, such as cancer screening for cancer of female reproductive anatomy, HPV variants of clinical interest, various specific technologies for reproductive cancer screening, and similar reworkings of the core concept. We included gender as a population search limit, but framed it inclusively and not limited to the gender limit feature offered in PubMed. We included other inclusion criteria during screening. The following formula depicts the concepts and relationships as searched.
Physical Disabilities AND [(“Cervical cancer” OR (Neoplasms AND Cervix)) AND ((Screening OR Diagnosis) OR (Cervical cancer screening))]/Women*
Preparation of this search filter included examination of search strategies and search recommendations from prior work.13–18 The preceding work helped shape strategic decision making and discovery of appropriate keywords, structured vocabulary, databases, concept clustering concepts, structures, and related methodological considerations.
The databases searched included Ovid Medline, Scopus, and REHABDATA. All were searched from inception through the date available at the time of the search completion. We searched Ovid Medline on August 2, 2021, for content through the 4th week of July 2021. (Supplementary Appendix A1). We searched Scopus on December 20, 2021. We searched REHABDATA on September 7, 2023. We applied no publication type or language restrictions during the initial search. In collaboration with a translator, we assessed the non-English language articles retrieved. Deduplication for the Scopus search was performed within the search strategy (Supplementary Appendix A2). We performed the deduplication for REHABDATA manually.
The research team identified several sentinel articles for validation purposes.19–26 We developed the following screening methodology. We exploded the epidemiological study characteristics, crossed them against the screened and selected studies, added the limits of search-only exclusion criteria, applied the specific inclusion/exclusion criteria for the study and its population, then expanded the terms for disability concepts and updated the search.
To determine eligibility, four reviewers independently reviewed titles and abstracts in pairs. We resolved discrepancies through consensus with a third reviewer. Studies meeting inclusion criteria moved on to full-text review for eligibility and, if eligible, data extraction.
Data extraction
Working in pairs, four reviewers independently extracted data from the eligible studies, beginning with confirmation of study eligibility. We extracted the following information from each eligible study: sponsorship source; study country (including World Health Organization world regions and the World Bank income classification); year published; study design; study purpose; sample size and number of WWPDs included in sample; source of sample; whether screening was performed; whether abnormal results were reported (and if so, proportions reported for women with and without disability); and other study outcomes. We resolved discrepancies in the data extractions through the consensus of the paired reviewers.
Critical appraisal
While scoping reviews do not always include a critical appraisal of bias, nor are they required by the PRISMA-ScR guidelines, we chose to evaluate the quality of included studies. To do this, we developed a customized critical appraisal guide to assess study designs eligible for this review. Reviewers selected the tool that best fit the study’s design and completed the items for that tool; the reviewer pairs reviewed this, and we reconciled any discrepancies (including the selection of the tool). We used appraisal tools for quantitative studies only. The Scottish Intercollegiate Guidelines Network 27 was used for cohort, case-control, and randomized controlled designs, the Appraisal Tool for Cross-Sectional Studies 28 for cross-sectional designs, and the Institute of Health Economics 29 for case series designs. Scoring for each tool was standardized to a common metric. Each eligible article was independently evaluated by reviewers using a rating system that aligned with its study design. Discrepancies were discussed and reconciled.
Data analysis and charting
We summarized the study and participant characteristics through descriptive analyses using the world regions from the study’s population and that country’s income classification. We included the study’s risk for bias and the component of the studied population who were disabled, as well as the method of defining the disability with descriptive analyses. We included the data sources for cervical cancer screening and the screening technique (cytology, HPV testing, liquid-based, conventional) in the descriptive analyses.
Results
Overview of studies
Using our search strategy, we identified 891 articles from OVID Medline, 1,237 from Scopus, and 27 from REHABDATA for 2,155 articles. After removing duplicate articles, there were 1,166 remaining articles for human screening, of which we excluded 1,062, leaving 104 articles to be assessed for eligibility using the seven criteria listed in Figure 1, resulting in 17 articles for full review (Table 2). The total population of the included studies was 8,709,161 adult women, of whom 427,410 (5%) had a physical disability by either self-report (50%) or medical verification (50%).
A Summary of the Studies Included in the Scoping Review
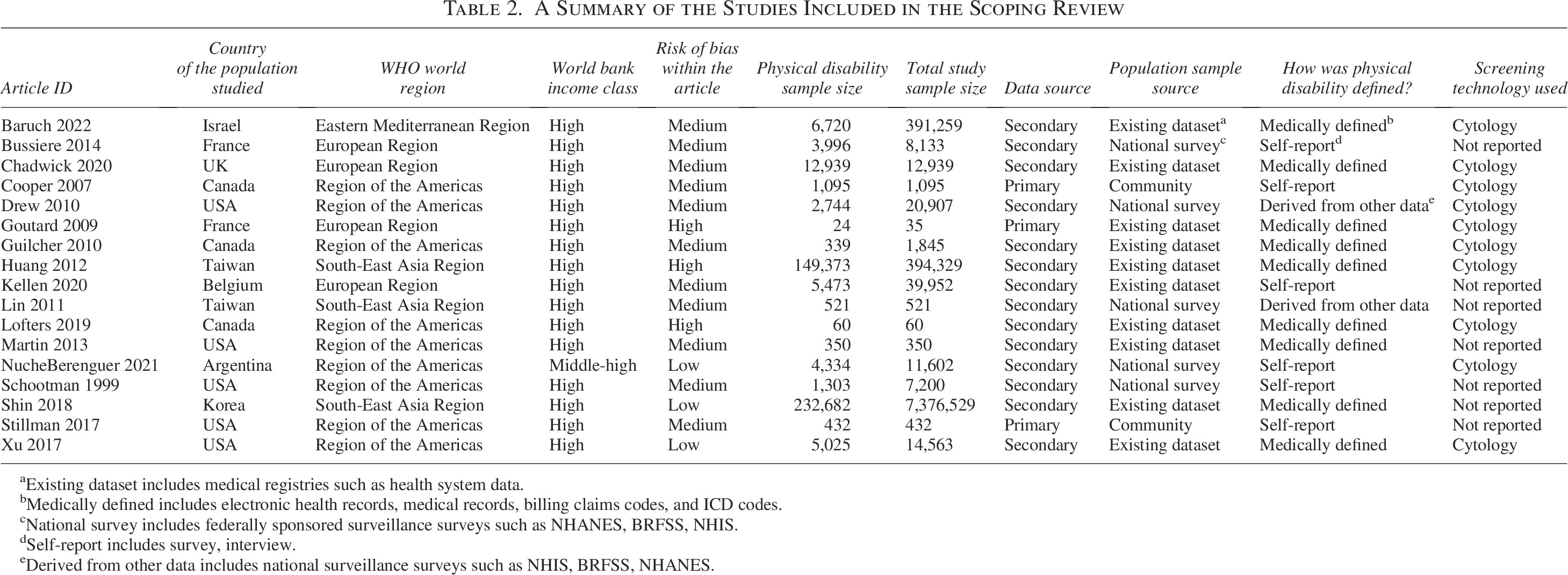
aExisting dataset includes medical registries such as health system data.
bMedically defined includes electronic health records, medical records, billing claims codes, and ICD codes.
cNational survey includes federally sponsored surveillance surveys such as NHANES, BRFSS, NHIS.
dSelf-report includes survey, interview.
eDerived from other data includes national surveillance surveys such as NHIS, BRFSS, NHANES.
Table 3 displays the summary of the characteristics of the reviewed study.
Characteristics of the Studies, Population, and Cervical Cancer Screening Data

aTwo studies reported more than one interval screening.
All studies used an observational design: 4 (24%) were cohort30–33 and 13 (76%) were cross-sectional.20,34–45 In addition, 3 (18%) collected primary data32,37,43 and the remaining 14 (82%) used secondary data sources.
The majority of the articles studied women in the Region of the Americas (53%), where five studies (29%) described a US-based population,20,33,41,43 three described Canadian population,31,37,45 and one Argentia’s population, 40 followed by the European Region (23%)30,36,39 two from the Southeast Asia Region (12%),32,38 and one from the Eastern Mediterranean Region (6%). 34 Nearly all (94%) studies were conducted in high-income countries.
We ranked most of the studies to have a medium bias (65%)20,31–37,39,41,43 with the remaining studies split evenly between low40,42,44 and high30,38,45 risk of bias (18%). Only one article was published before 2000. 41 Four (24%) were published between 2000 and 2010,20,30,31,37 ten (59%) were published between 2011 and 2020,32,33,35,36,38,39,42–45 and two (12%) were published after 2020.34,40
Six (35%) of the studies included only WWPDs,32,33,36,37,43,45 whereas two (12%) had less than a 5% disabled population, five (29%) included between 10% and 20% of the study population as disabled, and four (24%) reported 20–70% of the study population with disabilities. The studies defined the woman’s physical disability in three ways: women self-declared a physical disability (5, 29%), she/they described the disability from a set of self-report activity scales (3, 18%), and those defined by a medical diagnostic code (9, 53%). Three specific medical diagnoses (SCI, RA, and neuromuscular myopathies) were associated with four studies; one included only women in wheelchairs and 12 (71%) studies defined disability by a scaled response to reported or performed activity limitations.
Eight (47%) studies recorded self-reported cervical cancer screening.20,32,35,37,39–41,43 Nine (53%) studies reported that clinicians performed all the screens. However, only 59% of the studies reported the technique of cervical cancer screening occurring (Table 3). All screenings were speculum-based cytology and clinician-directed without conventional versus liquid-based cytology specification.
Cervical cancer screening
Cervical cancer screening is region-dependent. Eleven studies used the every 3-year screen to indicate screening occurred, whereas four studies used screening within the last year, one used screening within the past 2 years, two used every 5 years according to the woman’s age, and three used ever screened.
Women with disabilities
Eight studies included only women with disabilities (not a general population).30–33,37,38,43,45 Of these studies, three reported screening participation rates around 50%: among those with SCI, 50% (95% CI: 25–74%), 45 and among those using wheelchairs, 48% (27–68%) 30 and 64% (59–70%). 43
Others provided adjusted analyses. One showed that women with cerebral palsy were the least likely to screen among women with disabilities (aOR = 0.17 [0.05–0.64]). 37 One study showed that treatment for the disability did not change the uptake of cervical cancer screening within the past 5 years. 36 Adjusting for age showed that women with SCI who were younger than 45 years (63%) were more likely to screen than older women (52%) (aOR = 1.7 [1.1–2.5]). 31
When we adjusted for the severity of physical disability, two studies showed that among women with any physical disability, screening rates nearly halved as the disability increased in severity. Lin et al. showed that compared with mild physical disabilities, those with severe disabilities were less likely to screen (aOR = 0.48 [0.23–0.95]). 32 Using the number of activities of daily living (ADLs) requiring assistance, Martin et al. showed that as the number of ADLs requiring assistance increased, the likelihood of screening was diminished (aOR = 0.80 [0.68–0.94]). 33 Likewise, when investigating disability severity, the chances of not being screened were nearly four times higher for women with severe disabilities than those having no disabilities (aOR = 3.93 [3.85–4.01]). 40
When we compared women with disabilities to the general population, we found that 11 studies compared a population of WWPDs to a general population or a population without disabilities in their cervical cancer screening adherence.20,31,32,34–36,38–40,42,44 One study documented that women with severe physical disabilities were more than twice as likely to never screen for cervical cancer than their general population/no disabilities counterpart (aOR = 2.22 [2.17–2.27]). 40
When we aggregated the studies reporting on WWPDs who were screened at guideline intervals, we found five studies that reported cervical cancer screening within the past 1, 2, or 3 years (depending on their national standards) for those with disabilities to be about half that of those without disabilities.20,32,35,39,44 Among women with SCI, 44% screened within the past 3 years compared to 58% among the general population (OR = 0.53 [0.49–0.56]). 44 Women who had more severe physical disabilities had lower adherence to cervical cancer screening within the past 3 years (65%) than those women without a disability (78%) (OR = 0.91 [0.89–0.93]). 35
For a 2-year interval, 58% of women with no disabilities had screened within the past 2 years compared with 44% of women with moderate physical disabilities (OR = 0.87 [0.87–0.88]). 40 For a 1-year interval, 58% of women with mobility disabilities screened within the past year compared with 75% among those without disabilities (OR = 0.52 [0.51–0.53]). 20 Likewise, in Belgium, among WWPDs, 47% screened within the past year compared with 61% of the general population (OR = 0.77 [0.75–0.80]). 39
Age and socioeconomic covariates become important. Among women with SCI, older women were about half as likely to screen within the past 3 years as younger women (OR = 0.59 [0.40–0.91]), but this trend was also seen in older women without SCI. Whereas women with SCI and higher socioeconomic status (SES) were much more likely to have been screened within the past 3 years than women of low SES (OR = 3.6 [1.7–7.5]), but women without SCI did not vary their screening uptake by SES. 31 Similarly, screening within 3 years occurred less often for both women with and without a physical disability as the area of residence was more rural. Still, women with a disability had even worse screening uptake. 41
Four studies adjusted for socioeconomic and comorbidity covariates. One study defined screening within the past 5 years, one within the past 3 years, and two within the past year, adjusted the screening rates for specific comorbidities and socioeconomic covariates (Table 4).34,35,38,42 Overall, WWPDs screened less than women without disabilities, regardless of the screening guidelines in place. As the severity of the disability decreased, the chances of screening decreased by half. Older women with disabilities were much less likely to be screened than those in the youngest screening age group, and the lower the income/education/SES, the lower the screening among disabled women.
Adjusted Odds Ratios for Cervical Cancer Screening among Women with Physical Disabilities Compared to the General Population/no Disabilities

SES, socioeconomic status.
Two studies investigated the screening behavior of WWPDs and other chronic diseases, showing that screening was significantly lower than their peers. However, women with disabilities who had prior noncervical cancers had a 10–20% increased chance of screening for cervical cancer.34,38
Discussion
The results of this scoping review provide compelling evidence that WWPDs screen for cervical cancer less often than their able-bodied counterparts. This disparity was identified across world regions despite laws that have been enacted to protect the rights of people with disabilities. While the definitions of accomplishing a cervical cancer screen differ by region of the world, country income, and local medical guidelines, regardless of whether the definition is once in a lifetime ever screened versus yearly screened, WWPDs screened were significantly less than women without disabilities. No study has advanced the uptake of cervical cancer screening among WWPDs.
We found that the definition of disability is self-reported or a recorded medical diagnosis. Of the medical diagnoses, SCI, RA, and neuromuscular myopathies are the most commonly cited. This mixed definition is a struggle in much disability research, 10 but is less important in this context than the definition of cervical cancer screening. If a woman needs a wheelchair for mobility, the reason for her wheelchair is not as crucial to the cervical cancer screening process as the fact that she is in a wheelchair. From this review, we cannot parse elements of disability types and cervical cancer screening to address our second aim.
We report the documentation of cervical cancer screening to be half self-reported and half medical diagnostic coding in some health records. In other studies, self-reported cervical cancer screening is not accurate, as women have little understanding of the difference between a cervical cancer screen and an exam for irregular bleeding.46,47 We have no data to show that WWPD accurately reports whether they have been screened for cervical cancer, one of the many pieces of information not currently documented in the literature. Medical diagnostics does offer a solid level of confirmation that the screen occurred.
Our search also shows that there is no intersectionality work to understand any compounding effects of race, rurality, income, and education to understand any barriers to cervical cancer screening for WWPDs. The factors associated with decreased cervical cancer screening among the general population (age, rural residence, socioeconomic status, marital and employment status, and other chronic diseases) likewise may worsen the already diminished screening participation by WWPDs. Our evidence shows that WWPDs have not changed their participation in cervical cancer screening over the past 20 years and that screening occurs less often than in women without disabilities, regardless of other intersecting inequities.
One gap identified from this scoping review is the question of whether cervical cancer screening reduces cervical cancer incidence among WWPDs. Currently, no data describe the cervical cancer incidence or mortality of WWPDs. However, WWPDs have the same risk for cervical cancer as the general population. WWPDs are sexually active and are at risk for HPV infections,48,49 thus meeting the USPSTF definition of average-risk, asymptomatic women who require repeated cervical cancer screening. 50
In addition, the cervical cancer screening test is the most salient factor, divided into two halves. The first is the place where screening occurs. While our scoping review did not include studies with qualitative responses to cervical cancer screening from WWPDs, others have published work indicating the access issues (transportation, appointment time, hallways large enough for wheelchairs, and table height accessible) and attitudes of the medical staff (unsure how to hold legs, muscle spasms during the exam, fear of not performing the exam correctly, and the discomfort of the provider with women with disabilities) which prevent screening.51,52 To date, no studies to increase screening in WWPDs have defined alternative options to the office table with stirrups for cervical cancer screening.
The second is the type of cervical cancer screening offered to women, which none of our review articles reported. We do not know if conventional cytology was the test performed, whether liquid-based cytology was available, or whether HPV triage or primary testing was available. These screening details have yet to be reported, yet they reflect the quality of health care that WWPDs may have access to.
Primary HPV screening is now the preferred method of screening average-risk asymptomatic women by the US federal health agencies.50,53 It is a process that more accurately identifies women with cervical intraepithelial neoplasia grade 2/3 (CIN2+) with the fewest colposcopies by avoiding false positive cytology results. Colposcopy, the triage test after screening to determine if a CIN2+ lesion is present and needs treatment, is even more demanding regarding physical flexibility for extended periods on the exam table. The medical profession must actively advocate for increasing screening in WWPDs with tools that decrease false positives without reducing the CIN2+ detected, for example, primary HPV testing. Secondarily, the primary HPV test for cervical cancer screening is now FDA-approved 54 to be self-collected.
Self-screening with urine or a vaginal swab is an option proven to be noninferior to the speculum-based exam in the general population.55,56 Implementation trials to understand the barriers and facilitators of self-screening among women with disabilities are high priority. In addition, each woman’s physical disability may inform her choice of a self-sampling device. Research is needed to increase the development of specific tools for WWPDs to use for self-screening for primary HPV cervical cancer screening. Primary HPV testing will have the greatest possible effect on cervical cancer screening and prevention among WWPDs of any program to date. Funding agencies must fund research to test this in WWPDs.
Strengths/limitations of the study
The strength of this study is the librarian-led search strategies, which allow a vast reach of publications to be evaluated for inclusion. This fundamental step in our methodology allows for one of the most informative reviews of cervical cancer screening among WWPDs to be published.
A limitation of this scoping review is that it is limited to only those with a single disability (physical), and the definition of physical disability is not standardized. In real life, physical disability may also accompany other sensory or intellectual disabilities. Overall, WWPDs encompass many levels of activity limitation. Using medical diagnostic definitions does not include the self-defined and self-assessed physical limitations of other medical diagnoses. The speculum-based exam is not the appropriate screening technique for most women with disabilities, but the best technique has yet to be determined. The results of this scoping review show that health care systems have not shifted to the more effective primary HPV testing that is best for all average-risk asymptomatic women. Our future work will document the adoption of primary HPV screening for the general population and its expansion to WWPDs.
Conclusion
WWPDs do not participate in cervical cancer screening as often as their able-bodied counterparts. Age, SES, and country of residence affect the screening rate. Primary HPV screening offers the best screening test, especially as a self-directed test.
Implications for Practice
The USPSTF draft 2024 guidelines for cervical cancer screening indicate that self-sampling using primary HPV testing is a Grade A recommendation for all women. 57 We anticipate that family medicine, general internal medicine, and gynecology will rapidly adopt primary HPV testing, with the option of speculum versus self-sampling.
Authors’ Contributions
Conceptualization: D.M.H., S.E., and A.M.; Methodology: P.F.A., L.N.J., and C.Z.K.; Software: M.A. and C.Z.K.; Validation: A.M., D.M.H., S.E., and C.Z.K.; Formal analysis: D.M.H.; Data curation: M.A. and C.Z.K.; Writing—Original Draft: D.M.H., P.F.A., L.N.J., and C.Z.K.; Writing—Review and Editing: S.E., A.M., M.A., C.Z.K., D.M.H., P.F.A., and L.N.J.; Project administration: M.A.; Funding acquisition: D.M.H. and C.Z.K.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Institutes of Health through the Michigan Institute for Clinical and Health Research UL1TR002240 and NCI through the University of Michigan Rogel Cancer Center P30CA046592 grants.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.