
Abstract
Objective:
Perinatal health disparities are an important public health concern. Women from racial/ethnic minority groups have elevated rates of maternal and infant morbidities and mortality. In the general population, the social determinants of health (SDoH) are known to worsen overall health outcomes. We did not find a review of studies on SDoH during the perinatal period in different racial/ethnic groups. This narrative review focused on studies comparing Black and/or Hispanic women with non-Hispanic (NH) White women.
Methods:
Articles were identified using PubMed, PsycINFO, and EMBASE databases based on specified criteria. Six systematic reviews, one scoping review, and one integrative review met the inclusion criteria.
Results:
The rates of maternal comorbidities, including hypertension, diabetes, and obesity, as well as preterm birth, low birth weight, still births, and maternal and infant mortality, were higher in Black and Hispanic women than in NH White women. Adverse SDoHs that were more common in minority populations included socioeconomically disadvantaged neighborhoods, food insecurity, low education, poverty, segregation, and air pollution. While adverse SDoHs were associated with worse maternal and infant health, some studies unexpectedly reported more severe effects of these SDoHs in White women than in minority women. Several studies have had methodological limitations.
Conclusions:
This underexplored area of research highlights the urgent need for well-designed research on SDoHs related to maternal–infant health in different racial/ethnic groups, such as the development and testing of pragmatic interventions. Public health professionals, researchers, and policymakers should address health care disparities to improve perinatal outcomes.
Introduction
Perinatal health encompasses pregnancy through the first year postpartum and is a critical determinant of maternal and infant well-being. 1 The interplay among psychological, social, and biological factors during this period profoundly influences the long-term health outcomes of the mother–infant dyad.1–3 Among these factors, social determinants of health (SDoH), defined by the World Health Organization as nonmedical factors, including conditions in which people are born, grow, live, work, and age, and a wider set of forces and systems that shape the conditions of everyday life, play a pivotal role in influencing perinatal health outcomes. 4 Adverse social determinants (socioeconomic deprivation, racial discrimination, inadequate health care access, and housing instability) increase the risk of health complications, particularly perinatal complications,5–7 and have been linked to poor maternal mental health outcomes.5,8 Additionally, women who experience various adverse determinants incur compounding adversity, which increases the risk of poor perinatal health outcomes.7,9 However, many studies do not test the direct associations between SDoHs and specific perinatal or fetal health outcomes and do not include SDoH assessments, which represents a critical gap in the literature. Compounding the dearth of information is the notable absence of narrative reviews examining the connection between SDoH and perinatal outcomes among Black and Hispanic women.
We summarized, synthesized, and analyzed the existing review research on SDoH and perinatal health to provide an overview of the current knowledge, including identifying key themes, gaps in research, and potential areas for future investigation.10,11 A recent Agency for Healthcare Research and Quality 12 reviewed MEDLINE®, CINAHL®, and the Social Sciences Citation Index databases through November 2022 to assess observational studies examining exposure to SDoH and at least one health or health care-related outcome for pregnant and birthing women. The outcome domains included maternal mortality, severe maternal morbidity (SMM), hypertensive disorders, gestational diabetes, cardio/metabolic disorders, weathering (the physiological effect of premature aging caused by chronic stressful experiences), depression, other mental health or substance use disorders, and cost/health care use outcomes. Unfortunately, the risk of bias was high, and no studies had a moderate or low risk of bias; therefore, the authors did not evaluate the overall strength of evidence for any outcome.
This narrative review aimed to advance the understanding of the relationship between SDoH and perinatal health, with a particular focus on maternal and infant health outcomes. We synthesized evidence from existing systematic, scoping, and integrative reviews on the influence of SDoH on perinatal outcomes. The goal was to highlight a blueprint for interventions that mitigate these effects. The findings and recommendations of this review can inform policy decisions and guide the development of interventions to reduce perinatal health disparities.
Methods
Literature search, inclusion criteria, and data extraction
The list of SDoH was developed based on a search strategy and consensus among authors with expertise in SDoH.13,14 Examples of SDoH include education, poverty, discrimination, food insecurity (FI), economic stability, and socioeconomic status (SES). These SDoHs align with those highlighted by the World Health Organization and U.S. Department of Health and Human Services. 15 Examples of perinatal health outcomes include preterm birth (PTB), weight gain, gestational age, low birth weight (LBW), infant mortality (IM), pregnancy-related hypertension and diabetes, and SMM. 12 Three authors (E.G., M.D., and J.S.) independently screened titles and abstracts and assessed full texts for eligibility, with disagreements resolved by discussion. We compiled a list of systematic, scoping, and integrative reviews that presented findings on the association between SDoH and perinatal health outcomes. Figure 1 lists the search terms and databases (PubMed, PsycINFO, and EMBASE). This list, developed through a consensus among the coauthors, serves to underscore the underexplored research gap and the adverse associations of SDoH with perinatal (maternal and infant) outcomes in Black and/or Hispanic women. Racial/ethnic comparison groups varied among the studies. We specifically selected studies that offered evidence-based findings on perinatal outcomes and sought to link them to SDoH. The results were limited to English-language, peer-reviewed, and full-text publications.

PRISMA flowchart of the search process, inclusion/exclusion criteria, and included studies. PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
A total of 5,036 articles were identified during the initial search of PubMed, PsycINFO, and EMBASE. Following the removal of 258 duplicates, the exclusion of other unrelated types of studies/materials (e.g., empirical studies, books, lectures, discussions, nonfemale [3,602]), other articles based on title and abstract screening (537), and a total of 639 full-text articles were assessed for eligibility. Of these, eight articles met the inclusion criteria for review (Fig. 1).
The article must be a review study (e.g., systematic, meta-analysis, scoping, narrative, or integrative review).16,17 Perinatal health outcomes (maternal and/or infant health) specific to Black and/or Hispanic women must be addressed.
12
At least one measure within the article must assess an SDoH.12,15 Studies must include a racial/ethnic group and a White comparison group (e.g., samples of only race/ethnic groups were not included for review). Studies must compare the findings between Black and/or Hispanic and White women. Note: Some studies use different racial and ethnic categories (e.g., Black versus African American; Hispanic versus Mexican; White versus Caucasian versus non-Hispanic [NH] White). For consistency purposes, and per the U.S. Census Bureau racial categorization, this review will utilize the term Black/African American interchangeably, Hispanic/Mexican interchangeably, and White/NH White/European American interchangeably, as reported in the studies.
18
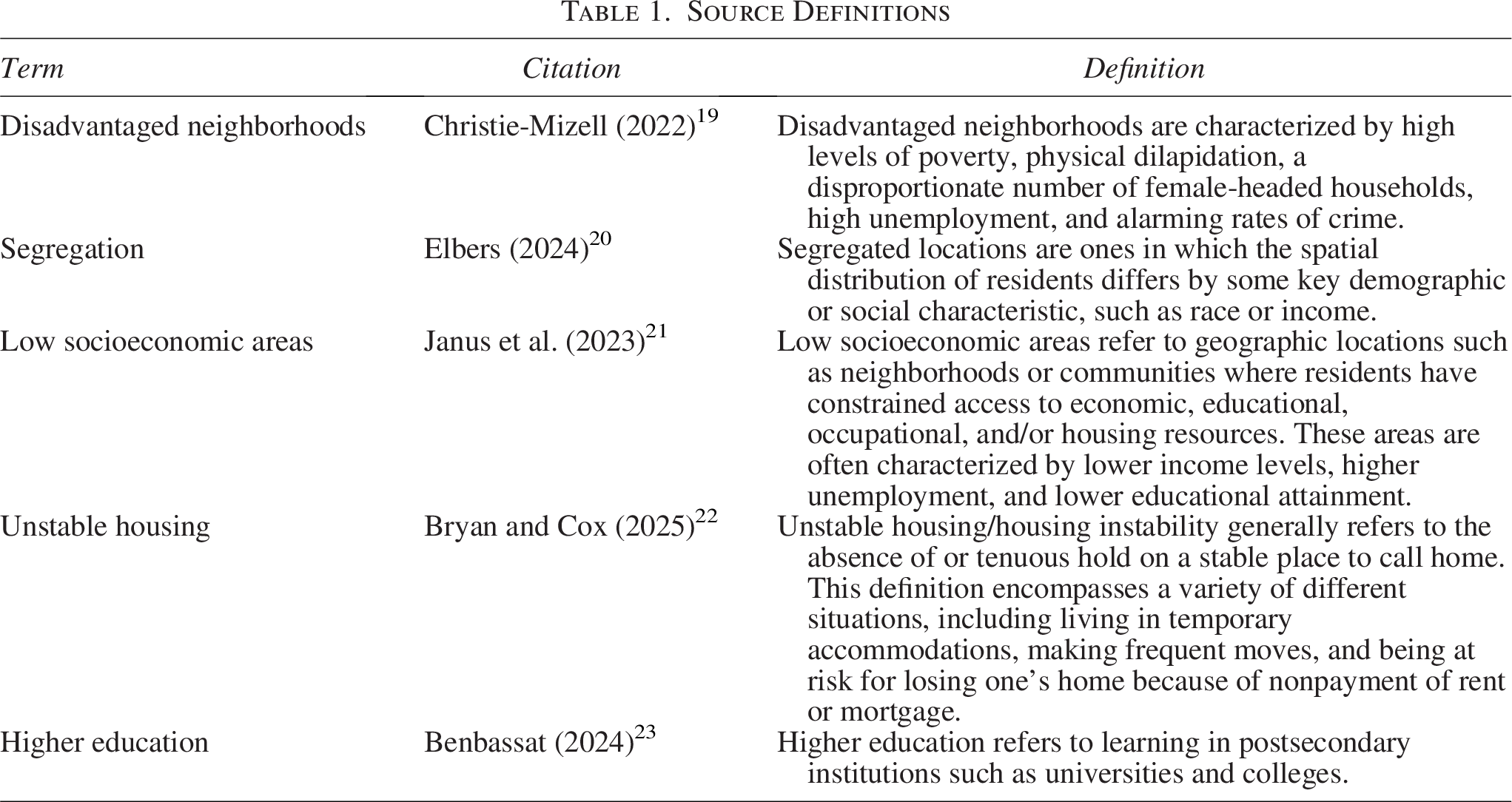
Table 1 summarizes the characteristics of main SDoH.19–23 The data extracted from the eligible articles are summarized in Table 2. They included (1) author and year (range = 2018–2025), (2) study type, (3) number of included studies (6–124), (4) sample size, (5) demographic breakdown by race/ethnicity, (6) SDoH measures, (7) listed covariates, (8) perinatal health outcomes, and (9) findings. Please note that the individual studies did not describe the definitions of SDoH as listed in Table 1. When available, statistical data such as p values, 95% confidence intervals (CIs), and odds ratios (ORs) were extracted. A summary of the findings relevant to this study is presented in table. The countries included in the studies across reviews are as follows: Australia, Spain, Nigeria, Colombia, Trinidad, Brazil, Israel, Malaysia, Mexico, the United Kingdom, the United States, and Senegal.
Source Definitions
Systematic, Scoping, and Integrative Reviews

aOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; IM, infant mortality; OR, odds ratio; pOR, prevalence odds ratio; RD, risk difference; SES, socioeconomic status; PPH, Post Partum Hemorrhage; SGA, Small Gestational Age; VBAC, Vaginal Birth After Cesarean.
Results
We summarized the results of eight systematic/meta-analysis/scoping/integrative reviews that met the inclusion criteria, focusing on statistically significant findings. Table 2 provides a brief summary of the findings reported by each author.
Amjad et al. 24 performed a systematic review of racial disparities in birth outcomes among adolescent mothers. African American mothers had significantly higher odds of PTB and LBW than their Caucasian counterparts. Specifically, African Americans had greater odds of PTB (prevalence OR [pOR] = 1.67, 95% CI: 1.59, 1.75) and delivering LBW infants (pOR = 1.53, 95% CI: 1.45, 1.62).
Elsmore et al. 25 published a systematic review and meta-analysis on the effects of race, ethnicity, and socioeconomic deprivation/housing on postpartum hemorrhage. Black and Hispanic women experienced higher risks of postpartum hemorrhage than White women (OR = 1.16, 95% CI: 1.09, 1.23) and (OR = 1.20, 95% CI: 1.12, 1.29). Additionally, one study found that Black women were more likely to be exposed to unstable housing than White women (29.8% versus 11.5%).
A systematic review by Ncube et al. 26 demonstrated that individuals residing in the most socioeconomically disadvantaged neighborhoods faced significantly higher risks of adverse birth outcomes. Specifically, those living in these areas had an increased risk of PTB compared with individuals in the least disadvantaged neighborhoods. When analyzed by race and ethnicity, NH White (NHW) women in the most disadvantaged neighborhoods had a 48% higher risk of PTB (OR = 1.48; 95% CI: 1.25, 1.75), whereas NH Black (NHB) women had a 15% higher risk (OR = 1.15; 95% CI: 1.09, 1.21).
Demetrio et al. 27 conducted a systematic review of 26 studies on maternal health outcomes associated with FI. FI in pregnant women was associated with being Black (prevalence ratio [PR] = 1.83, 95% CI: 1.08, 3.10), participation in social protection programs (PR = 1.43, 95% CI: 1.02, 2.01), and low education levels (PR = 2.73, 95% CI: 1.68, 4.43). FI increased the chances of being overweight (PR = 1.57, 95% CI: 1.29, 1.91) and obese (PR = 1.47, 95% CI: 1.15, 1.87), as well as excessive weight gain (PR = 1.42, 95% CI: 1.10, 1.82) and inadequate weight gain (PR = 1.47, 95% CI: 1.09, 1.97) during pregnancy. FI in the pregestational phase was associated with obesity (PR = 1.47, 95% CI: 1.15, 1.87) and overweight (PR = 1.57, 95% CI: 1.29, 1.91).
A systematic review by Hailu et al. 28 explored various maternal health outcomes related to race and segregation. This review has synthesized the findings of several studies. One study examined the effects of segregation and found that Black women in high versus low segregation areas had an adjusted OR (aOR) of 1.10 (95% CI: 0.82, 1.46), and in medium versus low segregation areas, the aOR was 1.09 (95% CI: 0.77, 1.54). These aORs were too small to be considered clinically meaningful. Another study reported that Black women had slightly higher odds of pregnancy-related hypertension (aOR = 1.10, 95% CI: 1.01, 1.20) and pregnancy-related diabetes than White women, although the estimates for White women were not statistically significant.
Dzekem et al. 31 examined racial disparities in PTB and other birth outcomes, focusing mainly on the differences between NHB and NHW mothers. A higher prevalence of PTB among NHB mothers was found, with a predicted difference in the probability of PTB of 0.056 (95% CI: 0.054, 0.058), demonstrating the advantage of White compared with Black infants. Individual- and neighborhood-level factors explained 37.8% of the Black–White disparity in PTB, with individual variables (such as age and education) accounting for 17.5% and neighborhood variables (such as socioeconomic environment) accounting for 16.1%. Air pollution was less influential, accounting for 5.7% of this disparity.
In a scoping review, Reno et al. 34 examined the effects of education and poverty on IM rates and disparities across racial and sex groups. Higher levels of education significantly reduced the IM rates across all groups. For European American female births, the IM rate decreased by 2.3-fold (95% CI: −2.5, −2.1), and for male births, the decrease was 3.3-fold (95% CI: −3.6, −3.0). Similarly, the IM rate for African American female births decreased by 1.7 (95% CI: −2.3, −1.0), and for male births, it decreased by 2.4 (95% CI: −3.0, −1.6). The data also highlighted the substantial impact of poverty on IM, with NHB infants having an aOR of 2.34 (95% CI: 1.47, 3.74) and NHW infants with an aOR of 2.17 (95% CI: 1.53, 3.08).
Spurlock et al. 35 conducted an integrative review evaluating the association between race, ethnicity, birth origin, SES, acculturation, and cesarean birth. Generally, a higher SES is linked to higher rates of primary cesarean births. The comparison of high cesarean rates between NHW and Mexican American women was 20.6% and 13.9%, respectively. Additionally, Mexican American women with U.S. immigration and naturalization service documentation were more likely to have cesarean births (33.7%) than those without documentation (17.4%).
Discussion
This narrative review highlights studies on the association between SDoH and perinatal or infant health outcomes. Below, we discuss our findings in detail, followed by the specific needs for the suggested research priorities and limitations. To our knowledge, this is the first narrative review of SDoH associated with perinatal health outcomes that focused on Black and/or Hispanic versus White women. The published studies show an association between worse maternal and infant health outcomes in women from racial/ethnic minorities who experienced greater exposure to adverse SDoH, such as racial and ethnic discrimination, worse SES, and lower level of education.
Of the eight studies included, five24–26,31 examined Black or Hispanic women and identified significant associations between neighborhood or environmental SDoH and outcomes, such as PTB, LBW, preeclampsia, gestational diabetes, and SMM. Two additional studies24,27 that focused on SDoH factors (FI, poverty, income inequality, and SES) also reported significant links to adverse outcomes, including inadequate weight gain, infant death, perinatal mortality, preeclampsia, and gestational diabetes. Additionally, out of the eight reviews, all eight included White women, seven24–28,31,34 included Black/African American women, and four25,28,31,35 included Hispanic/Latina/Mexican Americans. The SDoHs with the strongest associations with maternal and infant health outcomes included infant death, cesarean section, PTB, LBW, early gestational age, and stillbirth. Based on these findings, our narrative review demonstrates the need for critical attention to be paid to the complex interplay between SDoH and perinatal health outcomes. Few studies have shown significant associations between social factors and poorer perinatal health outcomes. It is essential to note that SDoH should not be considered a cause of perinatal complications; instead, it should be viewed as determinants that contribute to or exacerbate perinatal health conditions. Specific social factors in groups of people or places they live in are consistently associated with (on average) worse conditions and opportunities and, therefore, poorer health and higher mortality; however, SDoH cannot be translated into individual predictors. 40
This review provides evidence that adverse SDoH is a risk factor for poor perinatal outcomes, which exacerbate outcomes such as PTB, gestational diabetes, and SMM.
Suggested research priorities
To streamline and enhance future research, prioritizing the use of well-validated and standardized rating scales is essential for achieving accurate and reliable assessments of SDoH and its impact on maternal and fetal health. Future studies should also use clear definitions of SDoH. The recent Committee on Clinical Consensus 40 provides recommendations, including the need for a comprehensive pregnancy assessment inclusive of social and structural factors. A variety of unmet needs exist in pregnant women, and these must be addressed using a holistic team and systems-based approach to provide women with the best opportunity for a healthy pregnancy. This narrative review supports these recommendations. It will be beneficial to identify additional SDoH (e.g., faith/religion/access to quality health care) and other types of perinatal health outcomes (e.g., emotional, behavioral, social, and cognitive problems for children) and prioritize them in national and global public health policy efforts. Such studies with appropriate and advanced statistical analyses hold promise for identifying the mechanisms of causal relationships in the perinatal period and beyond, paving the way for significant advancements in maternal and fetal health. Longitudinal designs also enable the exploration of causal relationships and identification of critical periods during pregnancy, where targeted interventions could have the most significant impact. These investigations may demonstrate the strong interrelations between factors and may help strengthen longitudinal studies with large and diverse samples. Identifying the SDoH most associated with perinatal and fetal health (e.g., SES and PTB versus discrimination and SMM versus FI and gestational diabetes) is essential.
From a clinical perspective, integrating the routine assessment of SDoH and social constructs that are strongly associated with perinatal health outcomes into daily clinical assessment and practice would help improve care.41,42 For example, efforts to develop and validate suitable assessment measures will be critical in screening and monitoring racial/ethnic populations deemed high risk. Integrating comprehensive SDoH data into electronic health records is important for clinical care. Another potential opportunity to enhance clinical assessments is to provide regular training on trauma-informed care, cultural humility, and the impact of systemic inequities on perinatal outcomes. 7 Interdisciplinary team-based care (e.g., collaboration with social workers, individuals, and community health workers) provides a method for follow-up on needs identified through screening as well as personalized support. Finally, future research must expand its focus to include a broader range of overlooked SDoHs and their association with maternal and fetal health at the individual, community, and population levels. While traditional SDoHs such as income, education, and access to health care are well-documented, other determinants such as incarceration, social fragmentation, homelessness, and heat insecurity warrant investigation.41,42 For instance, incarceration disrupts family stability, exacerbating stress and trauma, all of which can negatively impact maternal and fetal health. Furthermore, while interventions to address SDoH at the individual level are vital for clinical settings, addressing SDoH at the community and population levels would help shift and change public policies and legislation.
Limitations
Narrative reviews have inherent limitations. 43 First, their primary objective is to broadly map the existing literature rather than conduct a critical appraisal of individual study quality or provide an in-depth analysis of the findings. As a result, they are limited in their ability to draw definitive conclusions or evaluate the strength of evidence. Second, many of the included studies relied on cross-sectional designs, which could not establish causal relationships. Additionally, the variability in sample types and sizes across studies highlights the need for greater standardization of research methodologies to ensure more reliable and generalizable results. Last, there were inconsistencies across studies in assessment of SDoH, reporting of perinatal health outcomes, and standardization of racial and ethnic categories.
Conclusion
This narrative review provides comparisons between Black and Hispanic women and White women with adverse perinatal health outcomes related to SDoH. This underexplored area of research highlights the urgent need for studies focused on perinatal health and pragmatic interventions in different racial/ethnic groups. Public health professionals, researchers, and policymakers must address these disparities and develop a more equitable future with improved perinatal outcomes in all populations.
Authors’ Contributions
E.G.: Conceptualization, methodology, data curation, visualization, validation, and writing—original draft preparation. M.D.: Methodology, validation, and writing—reviewing and editing. R.J.: Supervision and writing—reviewing and editing. J.S.: Methodology, validation, and writing—reviewing and editing. K.L.W.: Conceptualization and writing—reviewing and editing. D.V.J.: Conceptualization, methodology, supervision, and writing—original draft preparation.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This study was not funded by any organization.
Ethics Statement
This study did not involve human participants.