
Abstract
Objectives:
This study aimed to better estimate the risk of progression of vaginal intraepithelial neoplasia (VaIN) into vaginal cancer.
Method:
A systematic review was conducted to identify eligible studies that (1) reported at least one event of progression from VaIN to vaginal cancer, (2) provided the VaIN grade, (3) had a follow-up period of at least 6 months, and (4) specified the proportion of treated and untreated patients. The effect size was the risk of progression from VaIN to invasive cancer, calculated as the number of events of progression out of all the observed cases at enrolment.
Results:
Five thousand seven hundred and sixty-eight references were screened; 30 case series were deemed eligible for qualitative analysis. Twenty case series of treated women, and four case series of untreated women were quantitatively analyzed. Both subgroups included cases of high-grade VaINs (no progressions to vaginal cancer found in low-risk VaINs). A sensitivity analysis on the subgroup of untreated women resulted in the exclusion of a study with excessive influence, with the final data synthesis based on three poor-quality case series. The risk of progression of high-grade VaIN to vaginal cancer in treated women was 7.09% (95% confidence interval [CI]: 6.83–7.36%). The risk of progression of high-grade VaIN to vaginal cancer in untreated women was 29.88% (95% CI: 11.22–58.96%). Progression events primarily occurred within 5 years of follow-up.
Conclusion:
The risk of progression of high-grade VaIN to vaginal cancer is higher than previously reported and more serious for untreated women (CRD42024618227).
Introduction
The risk of progression of vaginal intraepithelial neoplasia (VaIN) to vaginal cancer is reported to be 5%. 1 This estimate is based on outdated studies. 2 More recently, a study of pooled data from Italy 3 and a recent meta-analysis 4 on the VaINs rate of no-regression (events of persistence, relapse, invasion summed altogether) reported both risks of invasion of around 5% in both treated 3 and untreated 4 high-grade VaINs.
However, the above estimates 2 –4 may be subject to historical bias, 2 bias due to pooled data, 3 and to simulated data. 4 In the latter case, 4 specifically, the authors applied a probabilistic calculation based on literature to extract the hypothetical chance of progression to cancer from the no-regression rate estimates of VaINs. Moreover, it is still difficult to provide any outcome data on untreated VaIN cases, because they typically undergo treatment. To overcome these issues, the present descriptive systematic review aimed to provide an up-to-date and comprehensive estimate of the risk of VaIN progression to vaginal cancer based on the existing literature.
Methods
This is a descriptive meta-analysis. It focuses on the risk of progression of VaIN to vaginal cancer, expressed as a crude rate based on the existing literature (events of progression out of the whole observed cases).
Eligible studies were screened using the search terms “vaginal intraepithelial neoplasia, vaginal cancer risk” and “vaginal intraepithelial neoplasia, vaginal cancer progression” in the databases PubMed, SciELO, Scopus, and Web of Science. Each term was entered into the general search box of each database. No specific time frame or language limits were set, with the aim of identifying all relevant published studies to maximize the number of untreated cases of VaIN. Additionally, references deemed eligible in a previous meta-analysis 4 were included, and the internal databases published in Indraccolo et al. 4 were reassessed. Both authors of this study screened and selected eligible studies, resolving any disagreements through discussion.
Following the consensus statement on VaIN (all treatments suggested according to one’s own experience, without specifying what the better treatment is), 5 it was assumed that all treatments for VaIN are effective in reducing VaIN progression and therefore treated patients were not distinguished based on the type of treatment. VaINs were grouped according to their grade (low-grade and high-grade VaIN) and treatment status (treated and untreated patients). The effect size was based on the overall rate of vaginal cancer observed in patients treated and untreated for VaIN of each grade, calculated as the number of events of progression to invasive cancer out of the total number of observed subjects at enrolment. The samples were not subgrouped according to risk factors conditioning the outcome of VaIN (lesions in the vaginal cuff after hysterectomy, multifocal lesions, human papillomavirus [HPV] status, immunodeficiency status, etc.), with the aim of providing a better real-world estimate of the rate of vaginal cancer. This approach is consistent with the approach employed in the previous meta-analysis referenced at Indraccolo et al. 4 It is acknowledged that the present meta-analysis, thus, includes heterogeneous samples at the qualitative level.
Eligible studies had to report: (1) The number of VaIN cases according to their grade. (2) A follow-up period of at least 6 months on average/median. (3) A clear definition of treated and untreated women. (4) At least one case of progression to cancer. The latter inclusion criterion was chosen because cancer events are rare; therefore, it was expected that some case series may have identified 0 events. Depending on the size and of the proportion of case series with 0 events in the database of pooled series, inclusion of these studies could lead to a wrong evaluation of the cancer risk, which would affect the final results.
A minimum of three patients in a case series was required for assessment in this study, because it was expected that there would be few eligible series, especially of untreated patients, and the available studies would include small numbers of subjects.
A qualitative analysis was conducted by both authors of the current study. In instances of disagreement, discussions were held to reach a consensus. As this is a descriptive meta-analysis, a customized Grading of Recommendations Assessment, Development, and Evaluation (GRADE)-like scoring system was utilized to assign a definitive quality score. This GRADE-like score is similar to the one used to assess quality in the previous meta-analysis referenced at Indraccolo et al. 4 Specifically, the following criteria were considered: (1) enrolment: randomized study +3, prospective study +2, retrospective study +1, less than 15 cases 0 (small series, higher risk of bias) and (2) highest follow-up time: more than 24 months: +1; 12–24 months: 0, 12 or less months: −1. (3) Description of sample (average/median age and hormonal status both described: +1; only one parameter described +0.5, both parameters not described 0). Studies with a score of 2 or higher were deemed to be of good quality. To test whether the quality score affected the variability of the analysis, an exploratory meta-regression was planned between the quality score and the standard error of the series. If the meta-regression was not significant, lower quality score series would not be excluded from the analysis.
The data extraction was independently conducted by the two authors of this systematic review. In the case of disagreement, discussions were held to resolve any discrepancies and ensure consistent data assessment. Events were collected as crude numbers or rates from the text, tables, or images of each included study. To extract data from images, Digitizelt.de 2.6 software was used.
At a quantitative level, Cochrane’s Q test was used to test heterogeneity. A random model was used to calculate the overall effect size if heterogeneity (at the quantitative level) was found, and a fixed model was used if heterogeneity was not found. Additionally, the fractal tool described in Indraccolo et al. 6 was applied by default to address nonrandom biases, as the authors chose a priori to include heterogeneous samples at the qualitative level. Sensitivity analyses were also conducted to test if any studies had an excessive influence on the final result. To address publication bias, Egger’s tests were performed.
Time to progression from VaIN to invasive cancer is presented in a descriptive manner, as it was determined that detailed data such as time-to-event curves would not be available based on available literature collected.
KyPlot 5.0 software was used for the meta-regression and for Egger’s tests. LibreOffice 7.0.3.1 software was used for all other calculations.
This systematic review was registered on the PROSPERO database (CRD42024618227). However, at the time of registration of the protocol, we were not aware of what the literature on VaIN evolution to cancer would be able to offer and had expected different findings. As a result, many changes were made to the registered protocol during the process of completing the review. Here, we have chosen to report on the final version of the study according to the new protocol, which we needed to adopt when assessing the available literature. The protocol registered in PROSPERO was not updated during the meta-analysis phases.
Results
The literature search was conducted on July 6, 2025, with 5,768 references retrieved. After removing duplicates and screening the remaining 3,379 references (Fig. 1), 114 were assessed for eligibility, leading to a final selection of 30 case series for qualitative analysis, obtained from 27 published studies. 3,4,7 –32 Among these 30 series, 4 involved untreated women, whereas 26 involved treated women. Table 1 provides a list of the series assessed, 3,4,7 –32 and Table 2 presents the quality scores assigned to them. 3,4,7 –32 The majority of series found in the literature were retrospective, and some were outdated. No studies reported cancer progression from low-grade VaIN, so only high-grade VaINs were included in the pooled analysis (Tables 1 and 2). 3,4,7 –32 Meta-regression analysis revealed that the quality score influenced the variability of the data only in the subgroup of treated women (p = 0.0002). Therefore, 20 high-quality series (quality scores ≥2) of treated women and 4 predominantly low-quality series of untreated women were included in the quantitative analysis.
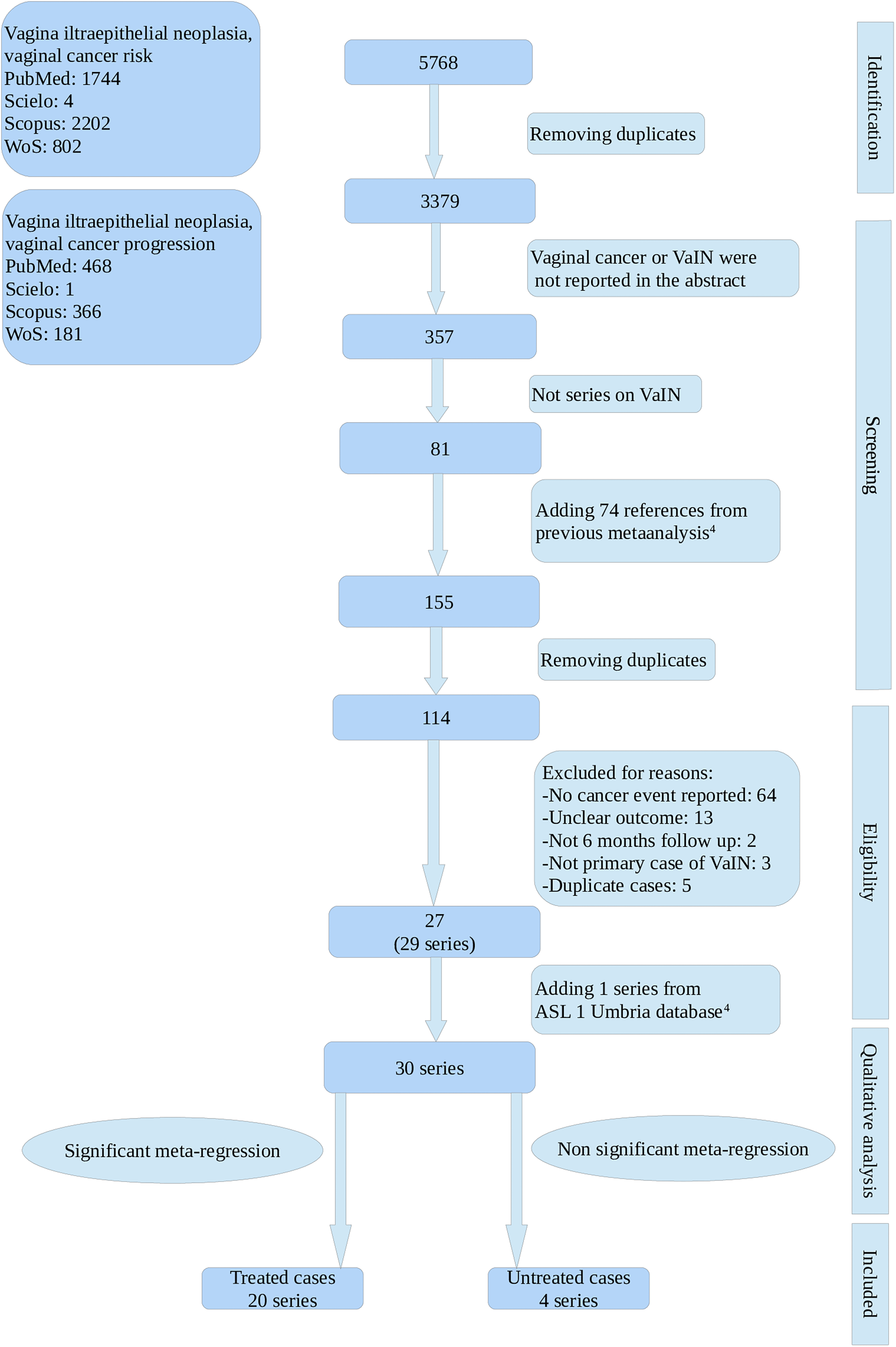
PRISMA flowchart. PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Alphabetical List of Studies from Which Eligible Series Have Been Extracted
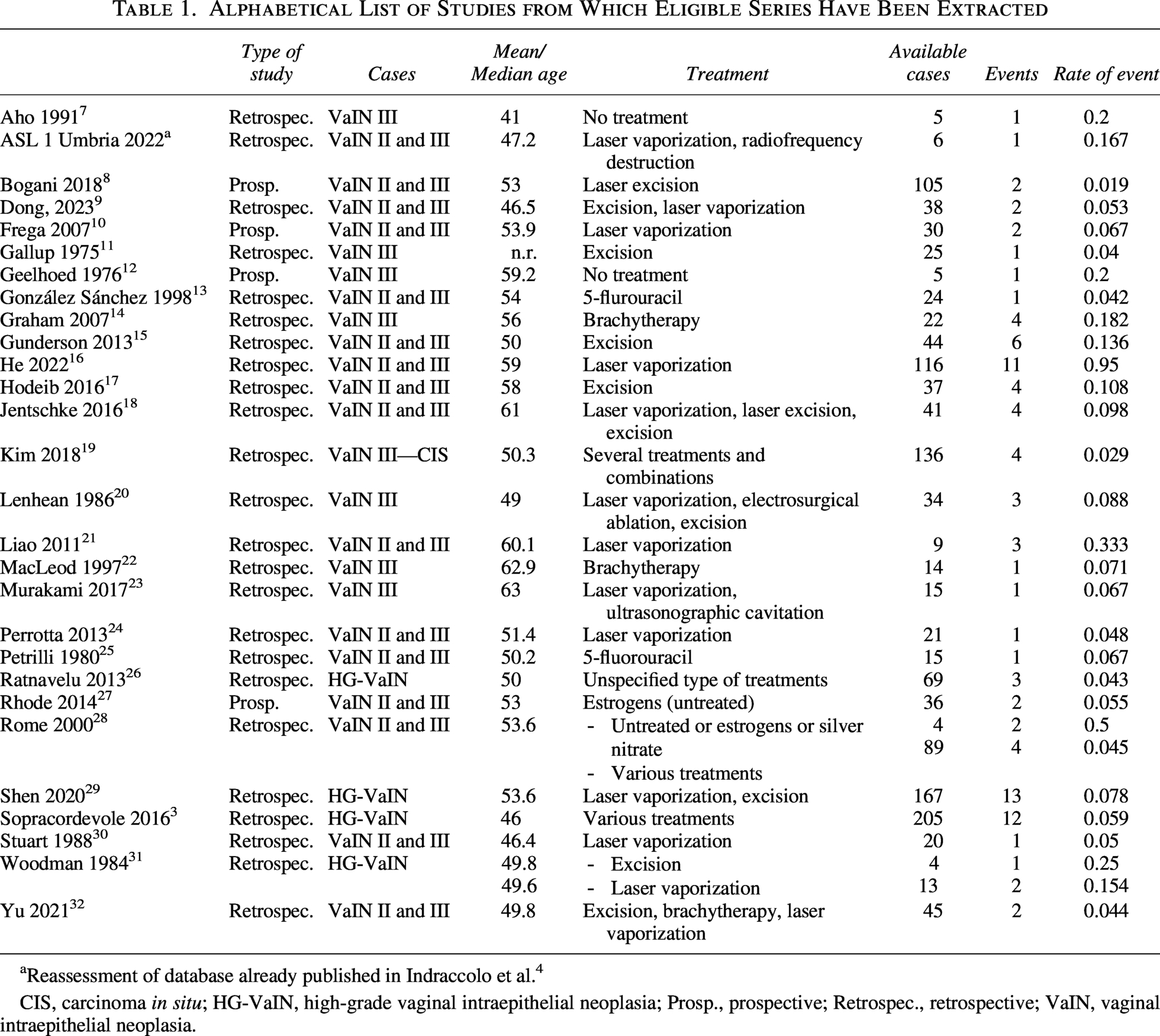
Reassessment of database already published in Indraccolo et al. 4
CIS, carcinoma in situ; HG-VaIN, high-grade vaginal intraepithelial neoplasia; Prosp., prospective; Retrospec., retrospective; VaIN, vaginal intraepithelial neoplasia.
Quality Score Attributed to Each Series
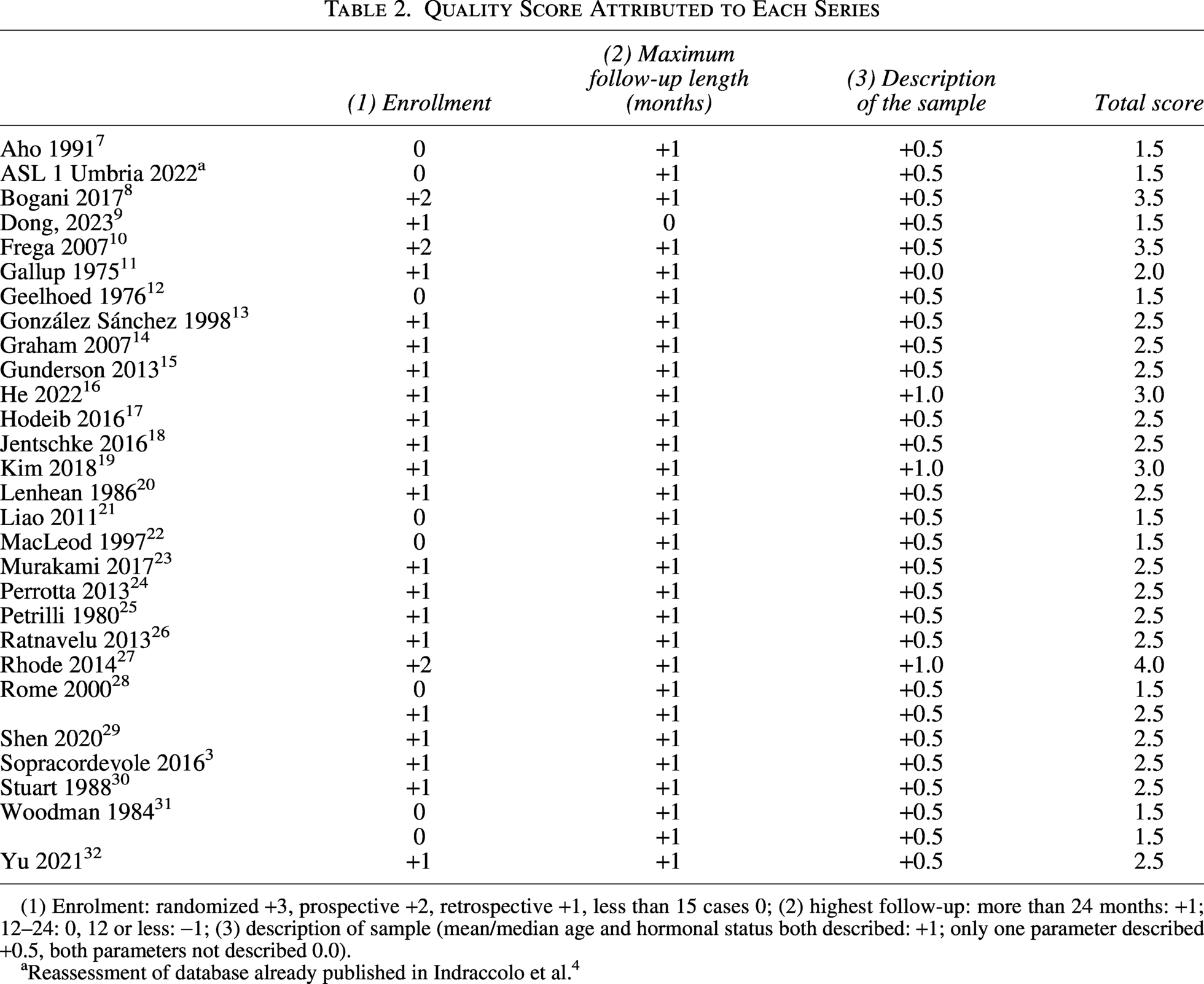
(1) Enrolment: randomized +3, prospective +2, retrospective +1, less than 15 cases 0; (2) highest follow-up: more than 24 months: +1; 12–24: 0, 12 or less: −1; (3) description of sample (mean/median age and hormonal status both described: +1; only one parameter described +0.5, both parameters not described 0.0).
Reassessment of database already published in Indraccolo et al. 4
The quantitative analysis for treated patients is reported in Figure 2. The risk of progression to vaginal cancer in treated women was 7.09% (95% confidence interval [CI]: 6.83–7.36%, Q = 19.521, I 2 = 2.7%), and this was substantially unchanged after fractal check. 6 Egger’s test was not statistically significant: p = 0.104. Then, a sensitivity analysis was conducted to test if studies with a higher number of observed patients would have an excess of influence on the overall effect size. The Q was partitioned into two groups: series with the number of observed patients over the mean (mean observed patients was 63) and series with the number of observed patients under the mean. The Q value between the groups was 1.456 and was not statistically significant for 1 degree of freedom. Therefore, larger series weights did not affect the final estimate.
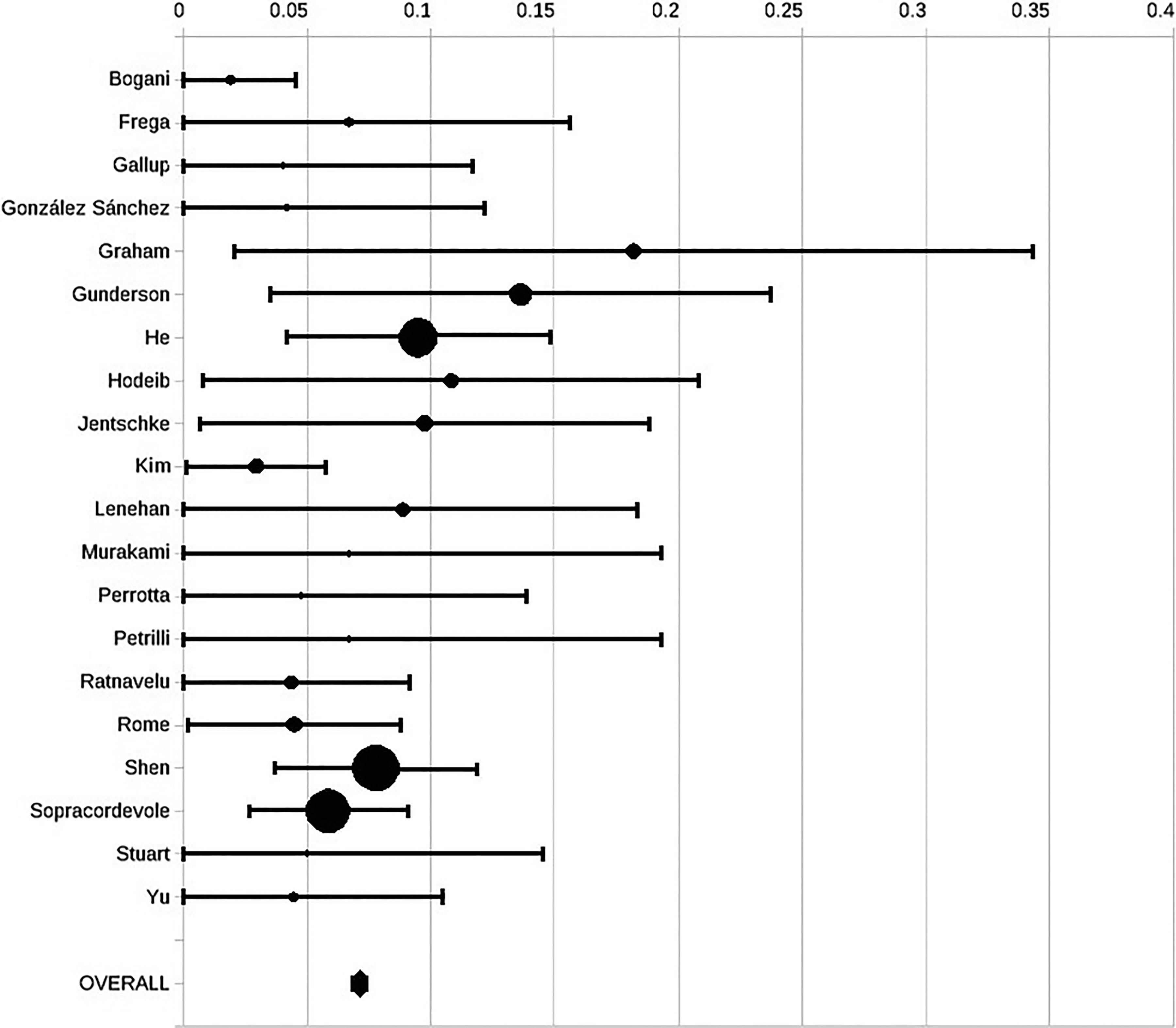
Forest plot on risk of progression to cancer in treated women.
Figure 3 presents the forest plot of the data summary for untreated women, without the inclusion of the study by Rhodes et al. 27 The high-quality study by Rhodes et al. 27 was an outlier and had an excess influence on the overall effect size, as observed by examining the overall effect size after its removal from the analysis (sensitivity analysis). After a broad discussion, it was decided to exclude the study by Rhodes et al. 27 from the final analysis to provide a more robust estimate of the risk of progression in the limited number of cases of untreated women available in the literature. The risk of progression of VaIN to vaginal cancer in untreated women was 37.87% (95% CI: 32.64–43.41%, Q = 1.183, I 2 = 0%), and after fractal check, 6 it was 29.88% (95% CI: 11.22–58.96%), as illustrated in Figure 3. Egger’s test was significant: p < 0.001. When including the study by Rhodes et al. 27 in the data synthesis, the estimate was 17.83% (95% CI: 16.75–18.96%, Q = 5.472, I 2 = 45.2%), corrected to 17.83% (95% CI: 5.69–43.81%) after fractal check. 6 Egger’s test was not significant.
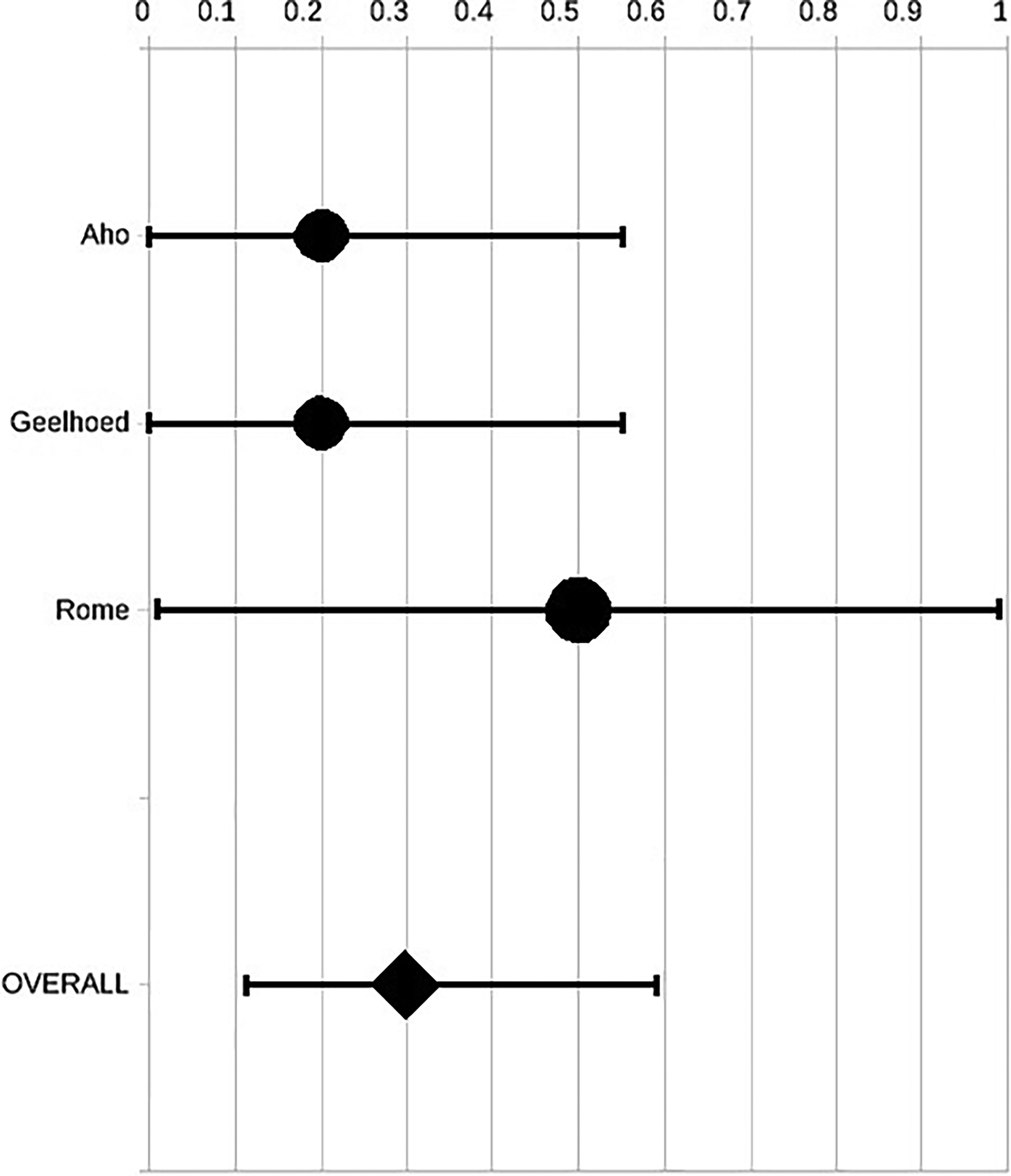
Forest plot on risk of progression to cancer in untreated women.
For both treated and untreated high-grade VaIN, the majority of cases that progressed to invasive vaginal cancer did so within 5 years of the primary diagnosis of high-grade VaIN (Table 3).
Descriptive Table on Time of Cancer Occurrence During Follow-Up
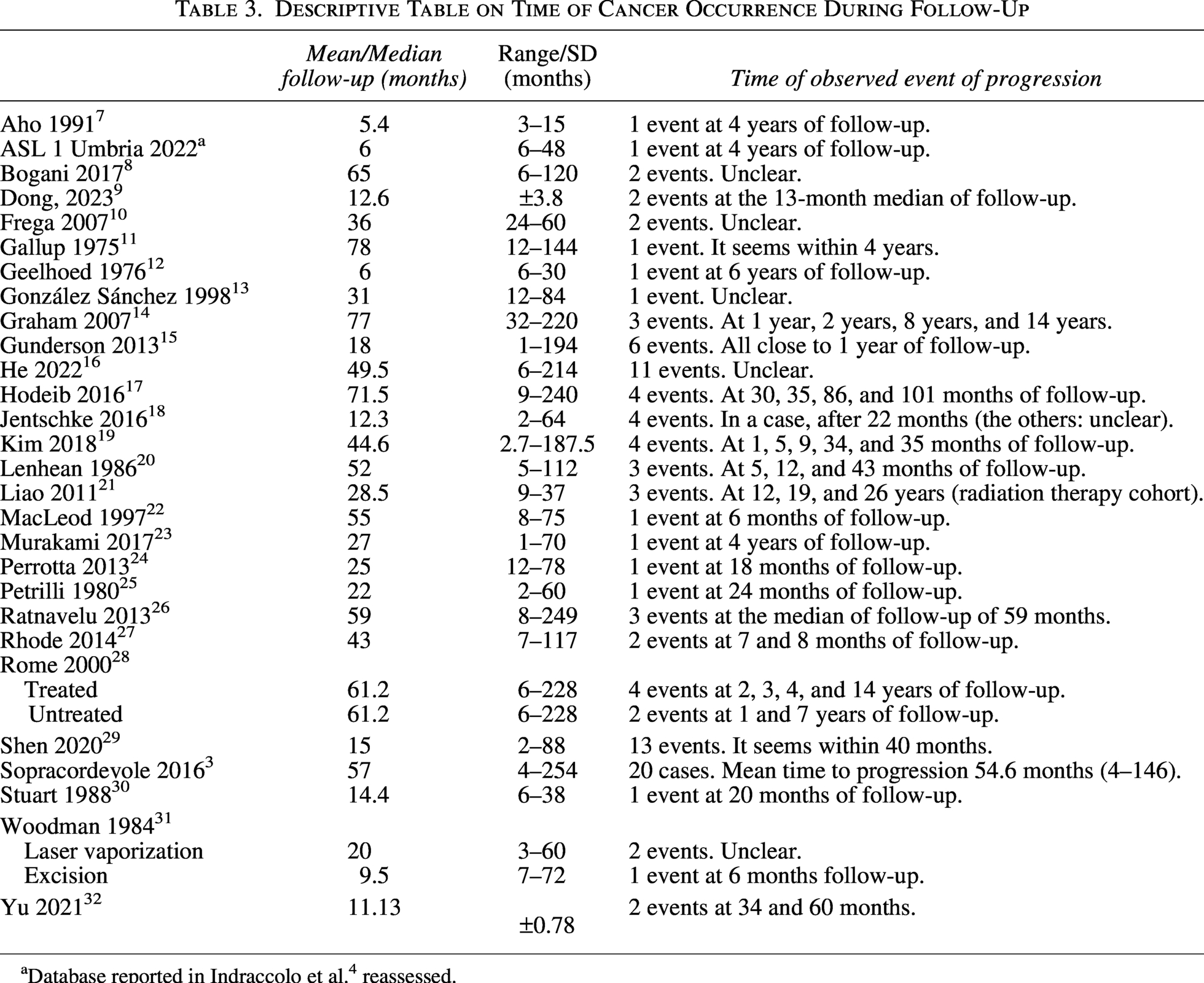
Database reported in Indraccolo et al. 4 reassessed.
Discussion
This systematic meta-analysis provides new insights into the risk of progression from VaIN to vaginal cancer. However, there are several limitations of this study that should be acknowledged.
First, despite the low quality of the evidence provided by current literature, a meta-analysis was performed. A meta-analysis is able to summarize the evidence in the pooled studies, thereby reducing the level of uncertainty and strengthening the degree of evidence. The quality of the result of a meta-analysis, however, depends strictly on the quality of the studies assessed. The current meta-analysis provides a description of the risk of progression of VaIN to cancer based on studies with low-quality evidence, without any outcome measures. Thus, we cannot make strong inferences from the findings reported in the current study, given the descriptive nature and the low quality of evidence in the current literature (no randomized trials, mainly retrospective series, usually no control groups). This finding, however, is what the literature can offer.
While the available literature on VaIN is of poor quality and heterogeneous, this study does provide real-world descriptive data on the rate of progression to vaginal cancer in both treated and untreated patients. Nonetheless, there was only a small number of untreated patients that were obtained from series judged as being low-quality based on our customized GRADE-like assessment. It would be very difficult to assess a higher number of untreated VaIN patients in future studies because leaving VaIN patients untreated in order to observe their outcomes is obviously not ethical. Regarding treated patients, readers may question the choice to consider all VaIN treatments equally effective. We have applied the approach used in a previous consensus statement, 5 which suggests treating all patients with VaIN without disclosing the better treatment approach, and we included all treated patients in a single group. It is likely that this issue needs much more scientific attention, because treatments may not be equivalent. The previous meta-analysis by Indraccolo et al. 4 did not obtain conclusive evidence on the treatment effectiveness of various VaINs treatments (although the findings suggested that laser vaporization and brachytherapy are promising). In contrast, the recent large study by Gallio et al., 33 published after the time of the current review, reported that excisional treatments and hysterectomy status increase the risk of VaIN recurrence, thereby suggesting that treatments are not equivalent for all types of VaINs.
Another weakness of this study is that the included series were not stratified for risk factors or types of treatments. As discussed above, we chose to include all types of VaINs (after hysterectomy, multifocal, in immunosuppressed patients, in HPV-positive patients, etc.) to provide a better, real-world estimate of the evolution of VaINs. This choice is consistent with the approach adopted in our previous meta-analysis. 4 It should be noted that, at present, it is impossible to subgroup VaINs according to risk factors for poorer outcomes. Analogously, it is hard to subgroup data for any treatment reported for VaIN, as the authors of a previous meta-analysis attempted, 4 without being able to draw a conclusion.
There are no reported data on the progression to vaginal cancer from low-grade VaIN. The only study that raised suspicion of such progression was the study by Aho et al., 7 which reported a case of progression in the “VaIN I and II” subgroup. In the Aho et al. study, 7 it is unclear whether this case of progression originated from low-grade VaIN or high-grade VaIN. On the contrary, high-grade VaINs in treated women appear to have a risk of progression higher than the 5% commonly acknowledged in the literature, 1 –4 estimated to be around 7.1%. Furthermore, treatments should be effective in reducing the progression of high-grade VaIN, for which the risk of regression is about four times higher (29.9/7.1) when untreated.
Some patients in the untreated group underwent local estrogen administration. 27,28 Rome et al. 28 reported that this therapy is not a treatment. We therefore deemed that estrogen therapy would not be a treatment according to Rome et al. 28 and considered women who had undergone estrogen therapy as untreated. However, it remains unclear if estrogen therapy is truly effective, as contrary findings were reported by Rhodes et al. 27 However, the Rhodes et al. 27 study was not included in the final data synthesis because the study was an outlier after the sensitivity analysis. If this study 27 was included in the pooled results, the final findings would be a lower risk of progression to cancer (17.8% versus 29.9%). Nonetheless, this risk was still higher than the risk of progression for treated patients.
For a gross comparison, in the case of untreated cervical intraepithelial neoplasia (CIN), the risk of progression to invasive cancer is 31.8%. 34 This value is close to what was reported in this study for high-grade VaIN (29.9%, without Rohdes et al. 27 ), leading to the suspicion that many high-grade VaINs, presumably HPV related, share a similar risk of progression as high-grade CINs if no treatment is carried out. On the contrary, in treated high-grade CIN, the risk of invasive cancer seems to be around 2%, 35 which is far from the 7.1% reported for high-grade VaIN. Therefore, it could be that treatments for high-grade VaINs are less efficacious than treatments for high-grade CIN and that some clinical conditions of VaIN would play a role in its outcome. Consistently, authors have reported that it is difficult to treat high-grade VaIN in the vaginal vault 33,36,37 and that multifocal VaINs can have a worse outcome 38 due to the difficulty in treating them. Therefore, prospective studies that stratify patients according to HPV status, VaIN type, immunologic status, and, hopefully, VaIN treatment are needed to improve care and patient outcomes.
Time-to-event curves would be ideal for assessing the outcome of an event by time. These curves are lacking in the literature on VaIN. Therefore, the present study was unable to predict the precise timing of progression from high-grade VaIN to invasive cancer. Nonetheless, the findings indicate that progression to cancer primarily occurred within 5 years of follow-up (Table 3). This highlights the importance of timely management of any persistent high-grade VaINs.
In conclusion, the risk of progression to invasive cancer in high-grade VaIN is higher than expected in treated patients and very high in untreated patients. The current evidence was primarily derived from retrospective studies and, for untreated high-grade VaINs, also from studies of poor quality. Further prospective studies, with stratification of risk factors for VaINs and for type treatment, are urgently needed.
Authors’ Contributions
U.I. performed the systematic review, assessed the studies, extracted data, assigned quality scores, made statistical analyses, and wrote the article. A.F. assessed the studies, extracted data, assigned quality scores, and provided full scientific editing of the draft. Both authors collaborated to resolve any disagreements through discussion. Both authors agreed with the results interpretation given in the latest version of the article.
Footnotes
Author Disclosure Statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This work did not receive any external funding.