
Abstract
Importance:
Recognition awards from medical societies are a key marker of professional achievement and play a crucial role in physician career advancement. At many academic institutions, national honors—such as society-based recognition awards—are integral to the criteria for promotion to the rank of full professor.
Objective:
To systematically review and conduct a meta-analysis of studies assessing the gender distribution of recognition awards conferred by United States (U.S.)-based medical societies.
Materials and Methods:
A systematic search of Ovid MEDLINE, Embase, Web of Science, Cochrane CENTRAL, and ClinicalTrials.gov was conducted in November 2023. Studies evaluating the gender composition of recipients of recognition awards from U.S. physician-focused medical societies were included. Studies without explicit methodology for selecting recognition awards were excluded. Data were independently extracted by two reviewers following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Study quality was assessed using the Newcastle-Ottawa Scale. A random-effects meta-analysis was performed to estimate the pooled proportion of women award recipients. The primary outcome was the proportion of women among recognition award recipients from U.S. medical societies.
Results:
A total of 35 studies comprising 16,994 award recipients were included. Across 25 medical specialties, the pooled proportion of women award recipients was 19% (95% CI: 15–23%). A similar pattern was observed among women physician recipients at 17% (95% CI: 13–23%). Substantial heterogeneity was observed (I2 = 95.5%), reflecting variations across specialties and award categories. Funnel plot analysis suggested minimal publication bias. Notably, representation of women overall varied widely across disciplines, with pediatric emergency medicine and pathology showing the highest proportion of women recipients, whereas neurosurgery and orthopedics were among the lowest.
Conclusions and Relevance:
Overall, women are underrepresented among recipients of recognition awards from U.S. medical societies. Addressing this gap will require intentional, systemic efforts by both medical societies and academic institutions to promote equitable recognition and advancement for all physicians.
Keywords
Introduction
Recognition awards granted by medical societies serve as important markers of professional achievement and play a critical role in the career advancement of their recipients. 1 These honors acknowledge meaningful accomplishments and contributions to a field through research, education, mentorship, leadership, service, and other scholarly and professional activities. Accordingly, such awards confer prestige, enhance the visibility of the recipient, foster new networking and career opportunities, and may positively influence rank promotion and academic advancement. 1
In the United States (U.S.), concerns have emerged regarding the equitable distribution of these awards. A 2017 analysis revealed that recognition awards conferred by medical societies were disproportionately awarded to men physicians, with women physicians often underrepresented or entirely absent from awardee rosters. 1 Subsequent studies across multiple specialties have largely corroborated these disparities.2–5 Disparate distribution of recognition awards may undermine the broader goals of academic medicine, including equitable mentorship, innovation, and patient care.6,7
This systematic review and meta-analysis aimed to synthesize the current evidence regarding the representation of women among recipients of recognition awards from U.S. medical societies, focusing primarily on awards intended for physicians. We sought to assess overall gender representation and identify trends across medical specialties.
Materials and Methods
Search methods
This systematic review and meta-analysis were performed in accordance with the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses reporting guidelines. 8 The study protocol was first submitted to the International Prospective Register of Systematic Reviews (PROSPERO) on 11 December 2023 and registered on 22 December 2023 (CRD42023488791). Electronic searches for published literature were conducted by a medical librarian [M.L.] using Ovid MEDLINE, Embase.com, Web of Science Core Collection, Cochrane Central Register of Controlled Trials (Ovid), and ClinicalTrials.gov. The searches were run in November 2023. The search strategy incorporated controlled vocabulary and free-text synonyms for the concepts of women and awards. The full database search strategies are documented in Supplemental Data (S.1. Search strategy and Supplementary Table S2). All identified studies were combined and de-duplicated using EndNote (EndNote, 2013) and EPPI-Reviewer (EPPI-Reviewer, 2010) then uploaded into Covidence systematic review software (Covidence, 2023) (Fig. 1).
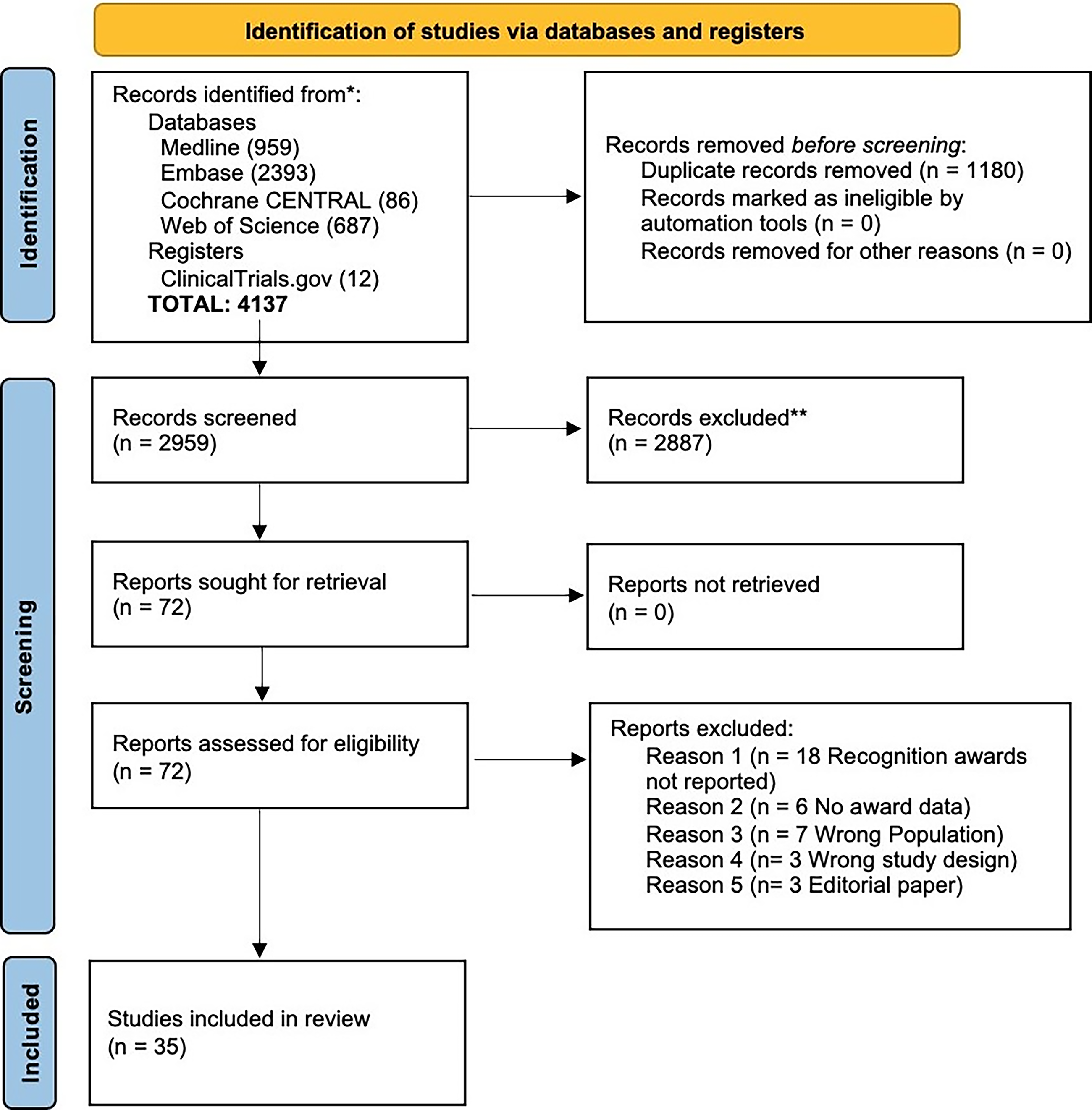
A PRISMA-style flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Eligibility and inclusion criteria
We included English-language studies that evaluated the gender and/or sex of recognition award recipients from U.S.-based physician-focused medical specialty or subspecialty societies. Eligible studies examined awards from one or more societies, rather than single award groups. We excluded studies focused on U.S. state medical societies or organizations not primarily focused on physicians. Also excluded were conference abstracts without full text, books, book chapters, Delphi reports, position or consensus statements, and other publications not originating from U.S.-based medical specialty societies.
Data extraction
Two authors [I.T. and A.M.] screened the titles and abstracts of all identified articles for eligibility. Full-text articles were screened from eligible studies using the Covidence online program. Disagreements were adjudicated by a third author [J.K.S.]. Data were extracted using an Excel spreadsheet-based form, which was reviewed and piloted by all authors. The following information was extracted by two authors [I.T. and A.M.] independently: Study ID (year published, first author), medical society’s specialty or subspecialty, name of medical society, time period of the study, types of awards (recognition awards), and total number of recognition award recipients (overall awardees, men awardees, women awardees, overall physicians awardees, men physicians awardees, women physicians awardees). While not all studies reported the occupations of nonphysician recipients, those that did included individuals with a PhD or JD degree, as well as medical laboratory professionals and administrators who have contributed significantly to the field. Some reports only included percentages, preventing data extraction; as such, those reports were excluded. Duplicate data from the same society award and timeframe were also excluded. In addition, we did not have access to individual-level data (i.e., the identity/gender of individual award recipients), and therefore the meta-analysis occurred at the study level, not the individual award recipient level. For multinational studies, only data corresponding to U.S.-based medical societies were extracted and included.
Study quality assessment
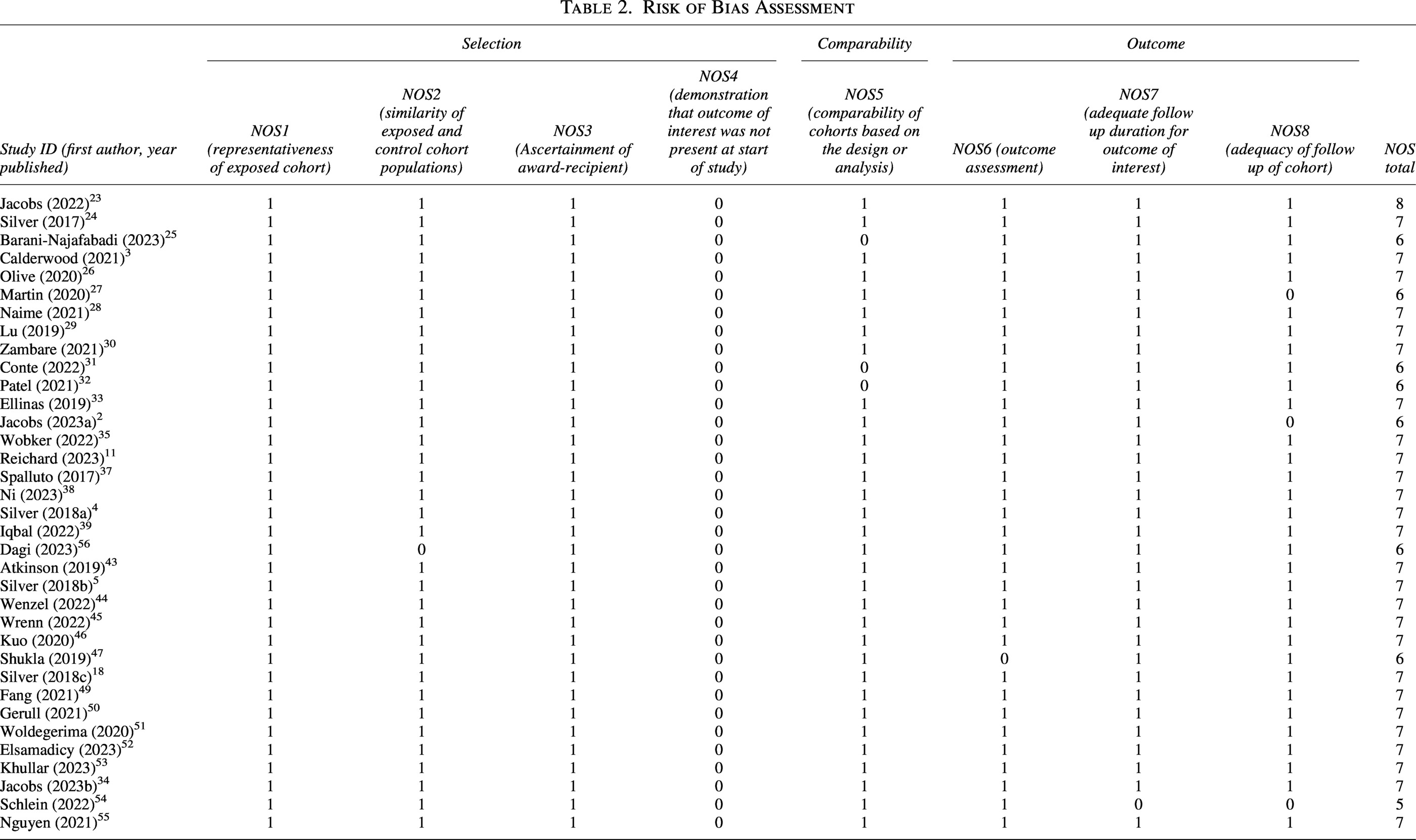
Two reviewers [I.T. and A.M.] independently assessed the quality of the studies included. The Newcastle-Ottawa Scale (NOS) was used for the quality assessment of the studies. 9 Based on the NOS criteria, we assigned a maximum of four stars for selection, three stars for exposure and outcome assessment, and two stars for comparability (maximum of nine stars). Studies with fewer than five stars were considered low quality; five to six stars, moderate quality; and seven or more stars, high quality.
Statistical analysis
We conducted a descriptive analysis to characterize the included studies, followed by two random-effects meta-analyses evaluating the proportion of (1) all women awardees and (2) women physicians awardees among recipients of recognition awards from U.S. medical societies. Statistical heterogeneity was assessed using the I2 statistic and Cochran’s Q test; an I2 > 50% or significant Q statistic supported the use of a random-effects model to account for both within- and between-study variance. Proportions and corresponding 95% confidence intervals were calculated to quantify representation and associated statistical uncertainty. Egger’s test was used to evaluate the risk of publication bias, and a funnel plot was created to assess the variability of the included studies. Bar graphs were constructed to examine trends in women’s representation by medical specialty. All statistical analyses were performed using Stata/SE 18.0 and R version 4.0.2 with a restricted maximum-likelihood estimator. Gender parity (i.e., 50:50 balanced gender representation) was our predefined threshold for equal representation; studies reporting < 50% women were considered to reflect underrepresentation.
Sex and gender consideration
We recognize the important distinction between sex (biological characteristics) and gender (social and cultural identity). However, the included studies used inconsistent terminology, with some reporting “sex” and others “gender.” For the purposes of this analysis, we treated these terms as equivalent when studies appeared to use male/female and man/woman interchangeably to describe the same populations, whereas acknowledging that this represents a limitation in precision. 10
Results
Study characteristics
After deduplication and application of the prespecified inclusion criteria, 35 of the 2,959 screened records satisfied eligibility requirements and were incorporated into the systematic review and meta-analysis (Fig. 1). These 35 studies encompassed a total of 16,994 award recipients spanning 25 medical specialties and 121 professional societies. Key study characteristics, including specialty type, society affiliation, and gender composition of awardees, are summarized in Table 1. All studies were published between 2017 and 2023 and included awards granted from the years 1911 to 2022.
Characteristics of Included Studies
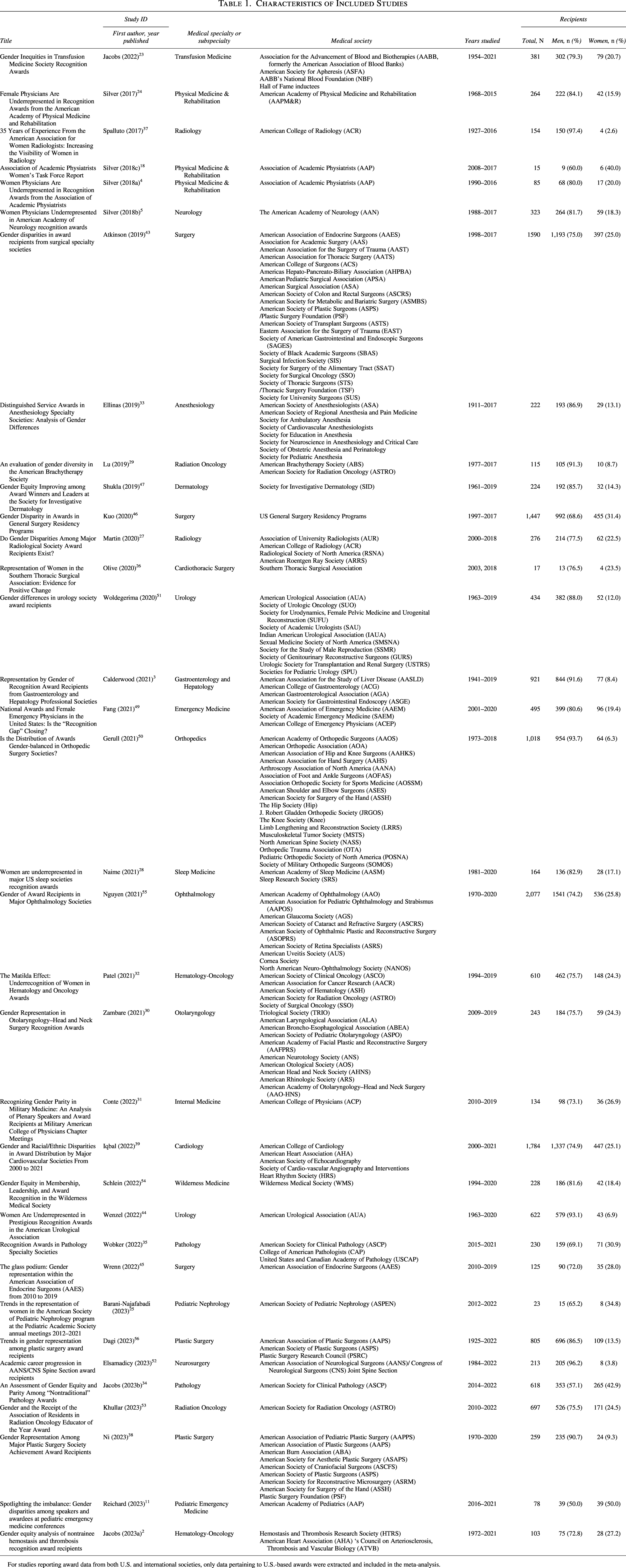
For studies reporting award data from both U.S. and international societies, only data pertaining to U.S.-based awards were extracted and included in the meta-analysis.
Overall, gender representation
The proportion of women recipients of medical society recognition awards varied widely across studies, ranging from 50% (95% CI: 38–62%) 11 in pediatric emergency medicine to just 3% (95% CI: 1–5%) 1 in multispecialty awards. The pooled proportion of women recipients across all 35 studies was 19% (95% CI: 15–23%), representing 3,582 women out of 16,994 total award recipients (Fig. 2). Men received 78.9% of the awards (13,412 recipients). Substantial heterogeneity was observed (I2 = 95.5%, τ2 = 0.5003, p < 0.0001), indicating considerable variability across specialties and time periods (Fig. 2).
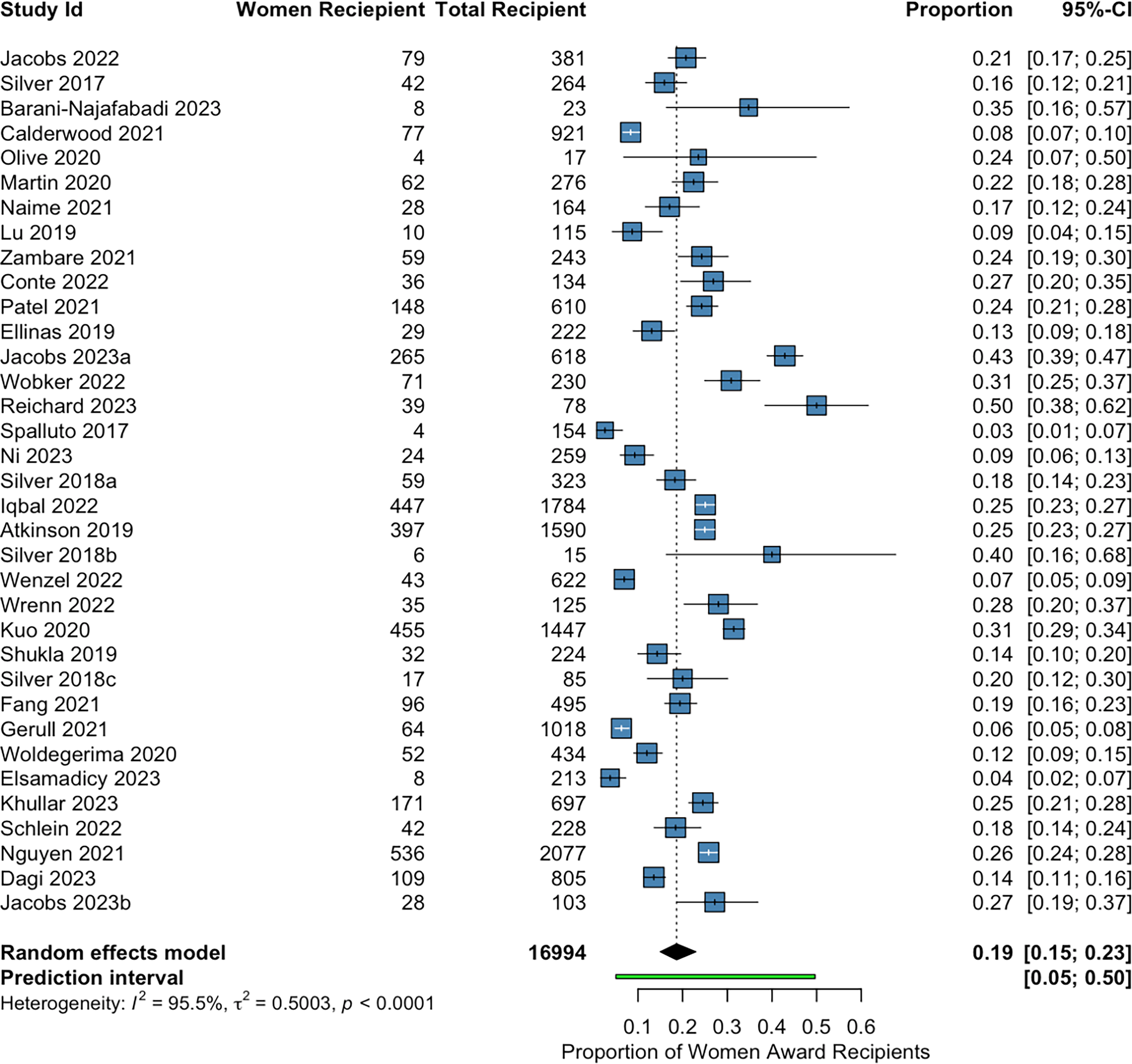
Meta-analysis of included studies. The 95% prediction interval depicts the expected range of the underlying true proportion of women among recognition award recipients across medical societies, accounting for between-society heterogeneity beyond the uncertainty captured by the pooled estimate and its 95% confidence interval.
Medical specialty-specific disparities
Analysis of gender representation by medical specialty revealed substantial variability in the proportion of women award recipients across different fields of medicine (Fig. 3). Pediatric emergency medicine demonstrated the highest proportion of women recipients (50%), followed by pathology (39.6%) and pediatric nephrology (34.8%). Other specialties such as internal medicine (26.9%) showed moderate representation. Among internal medicine subspecialties, cardiology (25.1%) and hematology–oncology (24.7%) also demonstrated moderate representation of women award recipients.
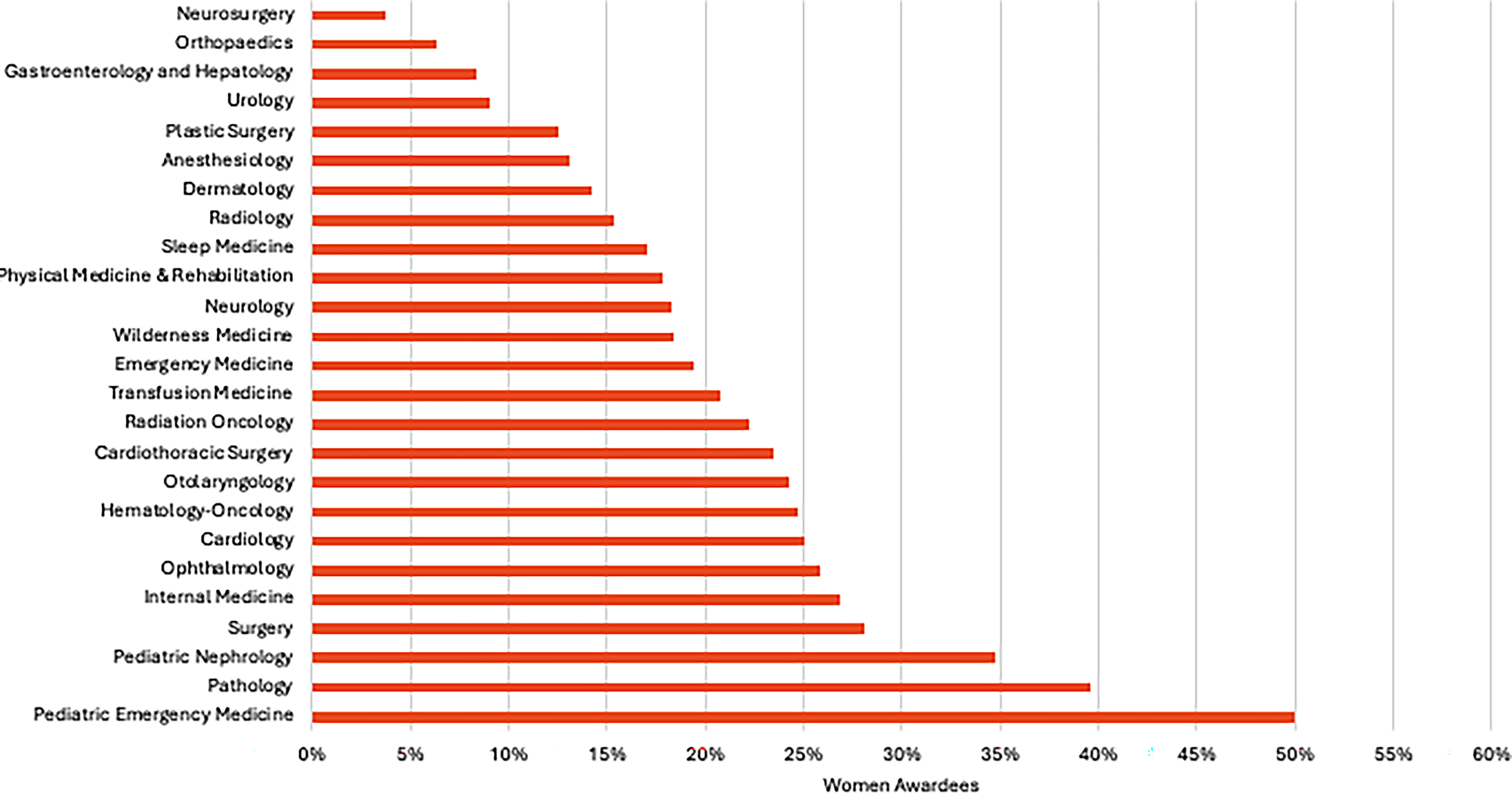
Trend in percentage of women recognition award recipients by specialty. Internal medicine also includes physicians serving in the military.
Conversely, surgical and technical specialties showed markedly lower representation of women awardees. Neurosurgery reported the lowest percentage (3.8%), followed by orthopedics (6.3%) and urology (9.0%). Other specialties such as gastroenterology and hepatology (8.4%) and anesthesiology (13.1%) also ranked at the lower end of the distribution.
Subgroup analysis: Women physician recipients only
The focused analysis of 22 studies (Fig. 4) specifically examining women physician recipients revealed similar patterns. These studies were published from 2017 to 2023 and included awards from 17 medical specialties conferred from 1925 to 2022. The overall pooled proportion, estimated using a random-effects model, was 17% (95% CI: 13–23%), representing 1,838 women physicians out of 9,609 total physician award recipients (Fig. 4). This analysis also demonstrated substantial heterogeneity (I2 = 96.3%, τ2 = 0.5899, p < 0.0001), reflecting considerable differences across specialties and time periods.
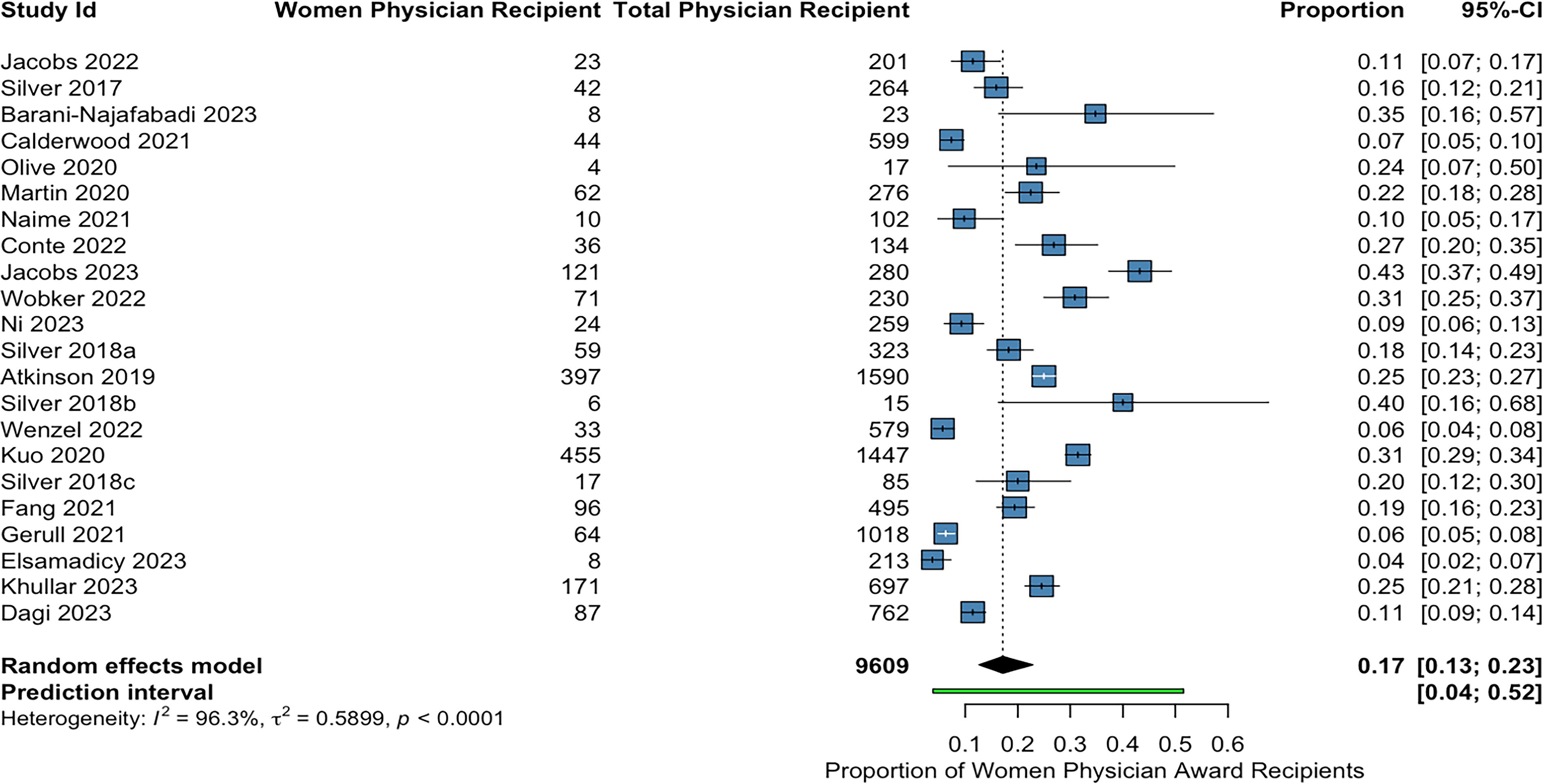
Meta-analysis of included studies of women physician recognition award recipients. The 95% prediction interval depicts the expected range of the underlying true proportion of women among recognition award recipients across medical societies, accounting for between-society heterogeneity beyond the uncertainty captured by the pooled estimate and its 95% confidence interval.
Figure 5 illustrates the percentage of women physicians who received recognition awards by specialty. There was notable variation across fields. Pathology showed the highest representation of women physicians (37.6%), followed by pediatric nephrology (34.8%), surgery (28.1%), and internal medicine (26.9%). In contrast, surgical subspecialties such as orthopedics (6.3%), urology (5.7%), and neurosurgery (3.8%) were among the lowest representation of women physicians.
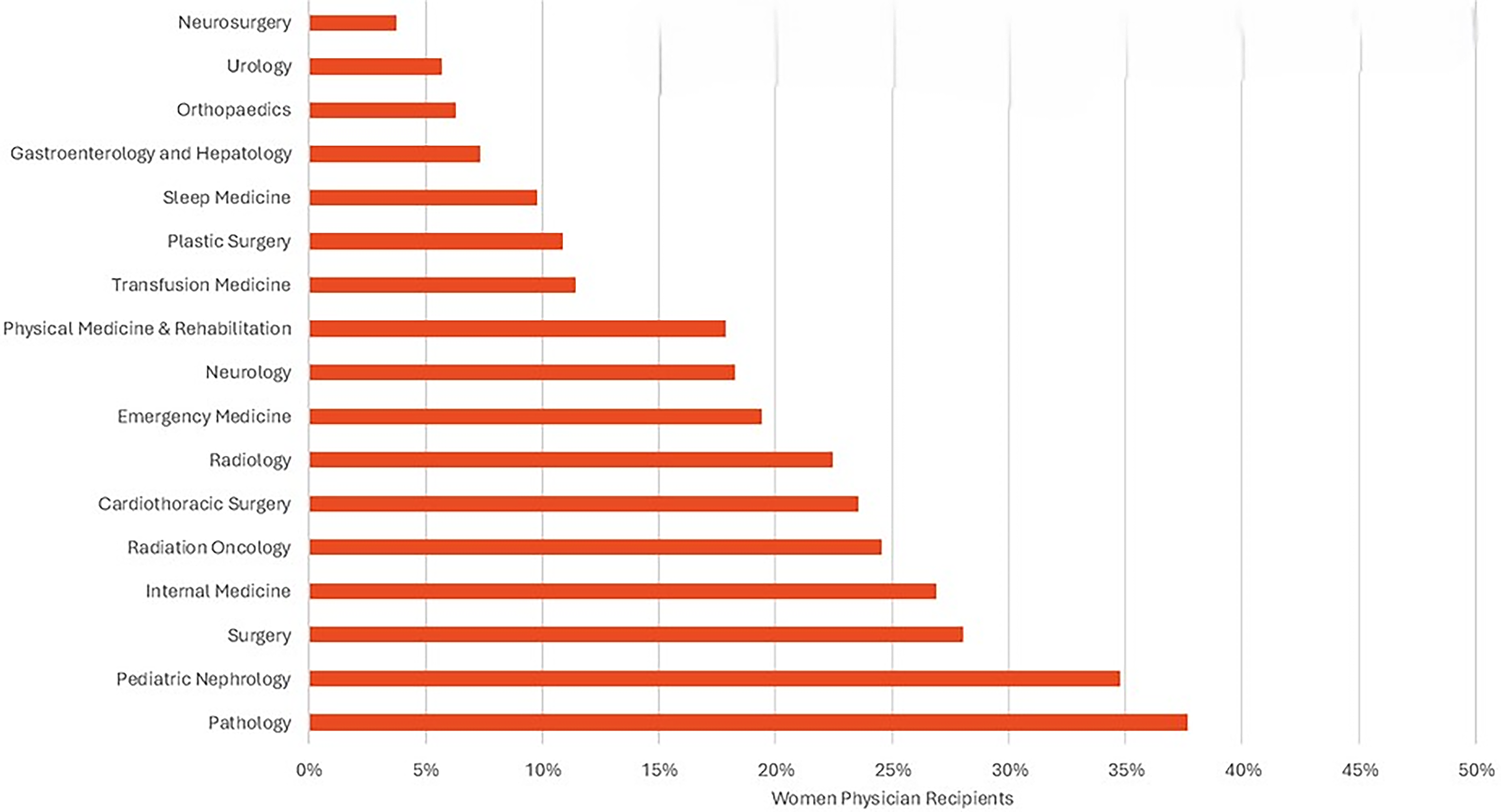
Trend in percentage of women physician recognition award recipients by specialty.
The 95% prediction interval for the pooled proportions of women recipients overall and women physician recipients was wide, extending from approximately 0.05 to 0.50 (all women) and 0.04 to 0.52 (women physicians), indicating that whereas some societies may approach parity, others may have virtually no women or women physicians among their awardees.
Discordance between overall women vs women physician representation
Figure 6 displays side-by-side comparisons of the proportion of women physician award recipients and all women recipients across medical specialties. The chart reveals several notable patterns and discordances. For example, in several specialties, the proportion of all women recipients exceeded that of women physicians, suggesting that nonphysician awardees contributed to higher overall women representation. For example, pathology showed 39.6% of all recipients were women compared with 37.6% among physicians. Similar patterns were seen in transfusion medicine (20.7% versus 11.4%), sleep medicine (17.1% versus 9.8%), gastroenterology and hepatology (8.4% versus 7.3%), and urology (9.0% versus 5.7%).
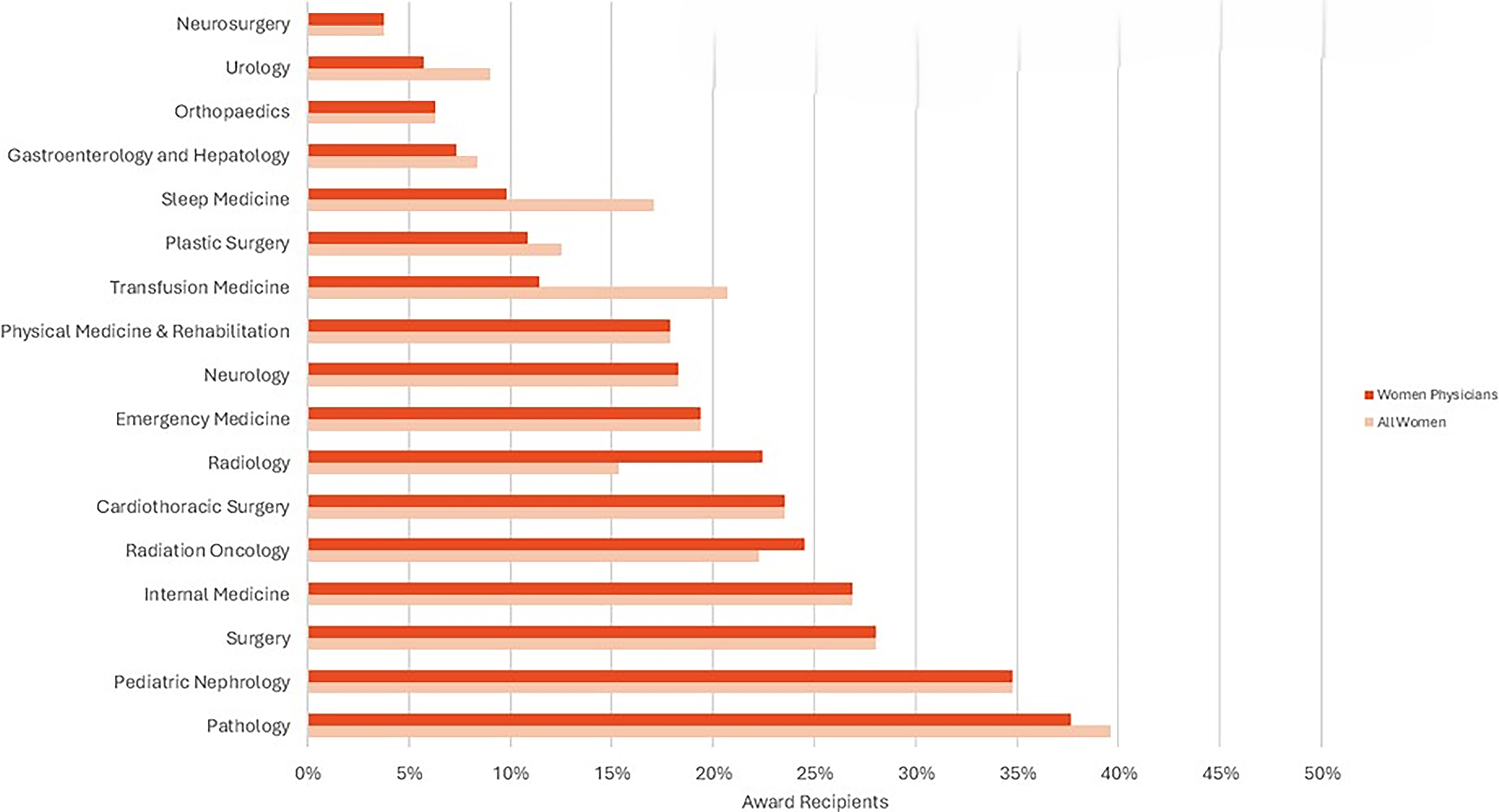
Comparison of women award recipients by medical specialty.
Conversely, in a few specialties, women physicians constituted a larger share of award recipients than women overall. In radiology, for example, women physicians represented 22.5% of physician recipients compared with 15.3% when considering all awardees. Radiation oncology was nearly equivalent, with women physicians accounting for 24.5% of physician recipients versus 22.3% overall.
Study quality and risk of bias
Among the 35 studies reviewed, no studies were rated as low quality (NOS score < 5), 8 were rated as moderate quality (score of 5–6), and 27 studies were rated as high quality (score ≥ 7). This distribution reflects an overall moderate to high methodological quality across the included studies (Table 2).
Risk of Bias Assessment
The funnel plot analysis (Fig. 7) suggested minimal publication bias, appearing somewhat symmetrical. However, some outliers were visible, potentially contributing to the observed heterogeneity. The concentration of points around the center indicates that most studies have proportions close to the overall effect estimate.
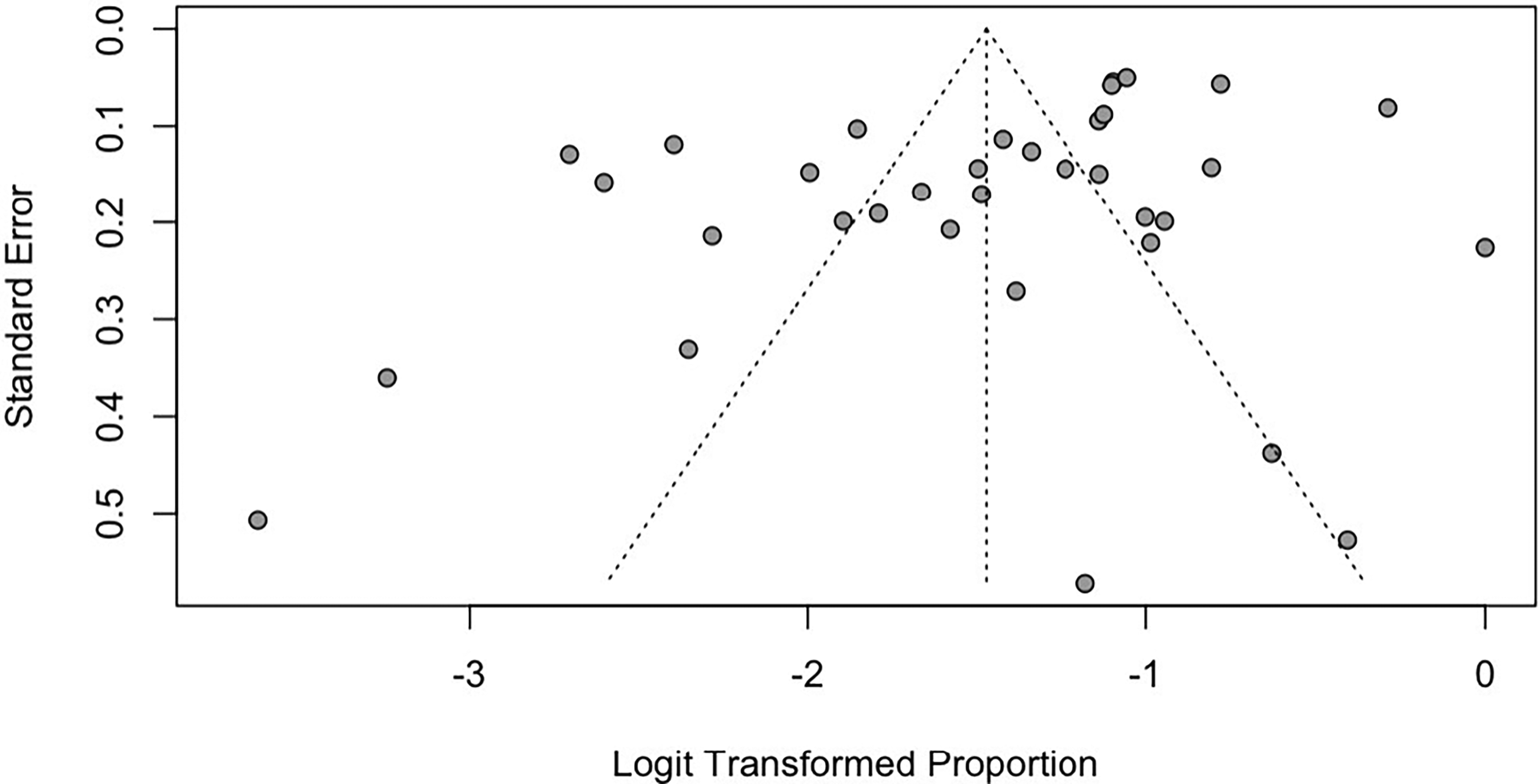
Funnel plot of included studies.
Discussion
In this systematic review of 35 studies encompassing 16,994 award recipients from physician-focused U.S. medical specialty societies, both women overall and women physicians were consistently underrepresented compared with men. This disparity was evident across nearly all medical specialties analyzed in this systematic review and meta-analysis, underscoring a persistent gender imbalance in professional recognition despite the growing representation of women in the physician workforce.12,13
Our findings align with prior reports documenting the paucity of women awardees across numerous medical specialty societies. 14 Specialty-specific analyses in our review revealed that certain procedural and surgical fields continue to demonstrate particularly stark disparities. Neurosurgery, urology, and orthopedics had the lowest representation of women physician award recipients (3.8%, 5.7%, and 6.3%, respectively). These patterns reflect entrenched gender imbalances in professional recognition within specialties traditionally dominated by men. 42
In multiple specialties, the proportion of women among all award recipients exceeded the proportion of women physicians among physician awardees, suggesting a notable presence of nonphysician honorees. This pattern was particularly evident in physical medicine and rehabilitation, ophthalmology, and transfusion medicine.36,48 While nuanced, this finding suggests that women physicians may experience greater disparities than would be apparent from analyses limited to the overall awardee population. Our findings suggest that gender gaps in recognition remain deeply embedded and may reflect structural and cultural barriers within certain specialties.
Overall, this analysis highlights persistent underrepresentation of women overall and women physicians in professional recognition across U.S.-based medical societies. Efforts to improve transparency, implement equitable nomination practices, and monitor gender representation in awards are needed to advance recognition equity in medicine.
Understanding these findings requires careful consideration of each specialty’s underlying gender composition. While women represented a small fraction of award recipients in orthopedic-related fields, this proportion may actually exceed their overall representation within these specialties. 40 In contrast, pediatric subspecialties—which historically attract higher proportions of women physicians—showed the greatest representation of women among award recipients at 50%. However, from 1992, when pediatric emergency medicine became a board-certifiable specialty, through the year 2023, when the report was published, there were 58.9% female board-certified pediatric emergency medicine physicians overall, suggesting a decreased representation of women award recipients in this specialty. 15 These patterns underscore the crucial need for future studies to benchmark awardee demographics against specialty-specific workforce data. Only through such comparative analysis can we meaningfully assess gender parity and equity in professional recognition.
This study also invokes a fundamental question about whether gender parity (i.e., 50:50 representation of women and men) or gender equity (i.e., balanced representation of men and women as compared with their respective composition in the particular specialty) is a more appropriate goal. This distinction between parity and equity has important implications for how researchers and policy stakeholders evaluate and address disparities in professional recognition across medical specialties.
Regardless of the ideal benchmark, gaps in formal recognition merit close attention, as they may shape career trajectories and access to advancement opportunities. Recognition awards confer not only individual prestige but also tangible benefits, including enhanced eligibility for research funding, leadership roles, and academic promotion. 41 The persistent underrepresentation of women among recognition award recipients may perpetuate gender disparities in senior faculty ranks, executive leadership within medical institutions, and compensation gaps across the profession.16,17
The findings of this review likely reflect a constellation of contributing factors. For example, one medical society reported a lack of nominations for mid- and late-career women physicians. 18 The same report noted that while early-career women physicians were nominated, none were ultimately selected by the awards committee. These patterns underscore that no single intervention is likely to achieve gender parity or equity in recognition. In response, the society implemented multiple strategies, including targeted encouragement of nominations for mid- and late-career women and the provision of implicit (unconscious) bias training for awards selection committee members. A subsequent evaluation suggested that the interventions had a positive impact. 18
Academic productivity may also influence award candidacy, as several studies have noted that early-career women often lag in traditional metrics of scholarship. These gaps often stem from systemic factors, such as the disproportionate caregiving responsibilities borne by women physicians. One recent report on this topic suggested institutional policy reforms to better support women in medicine, including extending family leave beyond childbirth (or catastrophic events), increasing flexibility in work hours, and providing subsidized eldercare services.19,20
Recommendations
Previous reports have suggested various processes to ensure disparities are addressed. For example, one report outlined a continuous quality improvement cycle with the following steps: examine the data and share results with stakeholders; investigate causality; implement strategic interventions; track outcomes and adjust strategies; and disseminate results.
21
More specifically, addressing gender disparities in recognition awards requires a multifaceted approach that includes, but is not limited to:1,22
Updated, Transparent, and Inclusive Award Criteria: Medical societies should update award descriptions and criteria. They should make the award nomination processes transparent by clearly stating award criteria on their websites and during nominations and actively encourage nominations of women and individuals from underrepresented groups. Diversity in Selection Committees: Increasing the diversity of award committees may help mitigate biases and foster equitable evaluation of candidates. Mentorship and Sponsorship Programs: Institutions should implement structured mentorship programs to support women in seeking recognition and leadership roles. Tracking and Reporting Gender Disparities: Medical societies should systematically report gender distribution in award recipients to monitor progress and guide future interventions.
Limitations
This analysis has some limitations. Importantly, this was a study-level meta-analysis. Therefore, we did not have individual-level data from all the studies to compare the data with the gender composition of the various types of awards, medical societies, and medical specialties over time. In addition, the studies varied in methodological quality, time frames, and award categories, contributing to heterogeneity. Although the included studies focused on physician-oriented U.S. medical societies, not all studies assessed physician awardees independently of nonphysician award recipients. The studies also used heterogenous methods to assign gender to individual awardees (e.g., reviewing biographical information, reviewing names/headshots, and utilizing tools such as genderize.io or gender-api.com). While these methods may be mostly correct and provide a broader picture of gender equity, 57 some inaccuracies may exist compared with self-identification. Our meta-analysis centered on gender disparities and could not evaluate other potentially influential factors such as race, ethnicity, academic rank, or institutional affiliation. In relying on published literature, we excluded studies lacking methodological transparency or demographic data on awardees. Furthermore, not all medical specialties were represented, particularly specialties that have women in significant proportions, such as obstetrics and gynecology, family medicine, internal medicine, endocrinology, rheumatology, and others. Therefore, whereas the observed trends were generally consistent across included specialties, these findings may not generalize universally. Finally, differences in specialty workforce composition and the absence of denominator data may limit direct comparisons of representation among awardees. Some reports only included percentages, and we could not extract the data.
Conclusions
This systematic review found that women remain largely underrepresented among recipients of awards conferred by physician-focused U.S. medical societies. These disparities have implications for academic visibility, career advancement, and the broader goals of equity in medicine. Addressing them will require systemic efforts to improve transparency, representation, and accountability at every stage of the award selection process, as well as improvements to the environment in medicine and academia.
Footnotes
Author Disclosure Statement
None of the authors have disclosures related to this article. Unrelated, J.K.S. discloses that she is a venture partner at Third Culture Capital and an advisor to Simplifed; J.W.J. has received compensation for non-consulting services and honoraria from Werfen and research funding from Bayer. G.S.B. discloses that he has received compensation for consultative services and honoraria from Grifols, which is unrelated to this article.
Funding Information
No funding was received to complete this work.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.