
Abstract
Background:
Despite increasing interest in the medical use of substances such as cannabis and psychedelics, little is known about their use to manage premenstrual symptoms. This study assessed self-reported use of substances to manage premenstrual mood and physical symptoms, including among those with premenstrual dysphoric disorder (PMDD) and in perimenopause.
Methods:
Inclusion criteria were age 18 and older with a menstrual cycle within the past year. Participants responded to an online survey querying the use of substances (alcohol, nicotine, cannabis, psychedelics, cocaine, stimulants, opiates, benzodiazepines) to manage premenstrual or perimenopausal symptoms, including frequency in the follicular and luteal phases of the menstrual cycle. Premenstrual symptoms were assessed via the Premenstrual Symptoms Screening Tool (PSST). Participants were categorized as PMDD if diagnosed by a health care provider via daily symptom tracking for two menstrual cycles.
Results:
Seven hundred and three individuals responded; 634 reported a menstrual cycle in the past year (n = 167 PMDD). To manage premenstrual mood symptoms, participants most commonly used cannabis (30.0%), alcohol (16.1%), and psychedelics (5.9%), with higher percentages within the PMDD group (51.5% cannabis, 16.2% psychedelics). PSST score positively correlated with luteal frequency of cannabis and nicotine use (ps < 0.01). Cannabis (p < 0.01) and psychedelics (p < 0.005) were used more frequently in the luteal phase than the follicular. Among n = 45 who reported perimenopausal symptoms, cannabis was most frequently used to manage symptoms.
Conclusions:
This study was the first to assess psychedelic use across the menstrual cycle. These data underscore the need for research to assess the efficacy of these substances for premenstrual and perimenopausal symptoms.
Introduction
Interest in cannabis and psychedelics for managing mood symptoms has been increasing in the United States,1,2 alongside changing legislation. 3 Data from a nationally representative prospective study of people who completed high school in the United States with statistics dating back to 1986 suggests the prevalence of cannabis and hallucinogen/psychedelic use continues to have an upward trend in the United States among adults aged 19–50 years old. 4 According to the Global Psychedelic Survey, over 40% of people who use psychedelics reported using for medical or therapeutic purposes. 5 Highlighting interest in these substances to manage mood symptoms, there are numerous trials investigating psychedelic-assisted psychotherapy for treatment of major depressive disorder,6–10 and assessing medicinal cannabis to manage affective symptoms.11–13 With a large population already using these substances, sometimes with the explicit goal of managing mood or physical symptoms, 2 and often outside of a medical provider’s supervision, it is important to understand use patterns and goals of those who use substances.
Mood and physical symptoms are common in the premenstruum; a nationwide, cross-sectional, internet-based survey among 42,879 women with menstrual cycles in the Netherlands found premenstrual symptoms to affect 80% of respondents. 14 In a recent international study of 238,114 people who menstruate and use a specific menstrual cycle tracking mobile application (app), 64.18% reported premenstrual mood swings or anxiety. 15 Significant mood and physical symptoms occur in the luteal (premenstrual) phase of the menstrual cycle in conditions such as premenstrual syndrome (PMS), 16 premenstrual dysphoric disorder (PMDD), 17 and premenstrual exacerbation of a psychiatric disorder.18–20 Premenstrual symptoms can be challenging to manage,21,22 and some individuals may explore nonprescription substances to manage symptoms.23,24 However, few research studies have examined cannabis or psychedelic use across the menstrual cycle, nor use to manage premenstrual symptoms specifically. Two studies found more frequent cannabis use in the premenstrual phase compared with follicular and/or ovulatory phases,25,26 and use correlated with self-reported premenstrual stress levels. 26 Among individuals with prospectively diagnosed PMDD, cannabis use was more frequent during the menstrual phase. 24 To the best of our knowledge, there have been no studies examining the use patterns of psychedelics across the menstrual cycle, particularly to manage premenstrual symptoms.
Similar to the premenstruum, perimenopause is a time in which many women experience mood or physical symptoms.27,28 Eighty percent of perimenopausal individuals reported symptoms including sleep difficulties, vasomotor symptoms, and mood changes. 29 Some women use cannabis to address perimenopause symptoms, 30 with 78.7% using cannabis specifically for perimenopause-related symptoms in an online survey based in the United States, 31 and 74% reporting that cannabis was helpful for symptoms in an online survey based in Canada. 32 There is relatively little research on the use of cannabis to manage perimenopause symptoms, and to the best of our knowledge, no studies investigating the use of psychedelics in perimenopause.
Given the increased use and interest in substances including cannabis and psychedelics, the study aims were to assess use of substances across the menstrual cycle, whether participants reported using substances to manage premenstrual or perimenopausal symptoms, how use correlated with premenstrual symptom severity, and whether use varied by PMDD diagnosis or perimenopausal status. We hypothesized that substances would be used more frequently in the luteal phase compared with the follicular phase, that participants would report using substances to manage premenstrual and/or perimenopause symptoms, that more severe premenstrual symptoms would be correlated with more frequent substance use, and that substance use would be greater among those with a PMDD diagnosis than those without.
Methods
Participants
Participants were recruited via fliers, websites (IAPMD.org, The Johns Hopkins University [JHU] Reproductive Mental Health Center [RMHC] website), JHU Sona Psychology Research Portal, and emails to previous research participants in the RMHC who had consented to further contact. Participants were directed to a secure Qualtrics website managed by the JHU Center for Psychedelics and Consciousness Research that described the survey study. They were informed that no personal identifiers were collected, and that their identity and data would be kept completely confidential. They provided consent by reading a statement that “I have read the explanation provided to me, and I voluntarily agree to participate in this survey study” and responded “Agree to participate” or “Do not agree to participate” to indicate their consent.
Inclusion criteria were age 18 years and older and having experienced a menstrual cycle within the past year.
No compensation was provided to participants, although students who participated via the Sona portal could earn extra credit in an undergraduate psychology course. This study was approved by the JHU School of Medicine IRB (Protocol 00298239).
Survey
The survey was posted from May 12, 2023, to July 10, 2024. The survey included sections on demographics, menstrual cycle characteristics, premenstrual mood symptoms, premenstrual physical symptoms, PMDD diagnosis, hormonal medication use, psychiatric medication use, use of medications or supplements to manage premenstrual symptoms, and substance use.
In the substance use section, participants were asked about their use of alcohol, nicotine, cannabis, hallucinogens or psychedelics, cocaine, stimulants, opiates, and benzodiazepines. They were asked “During the premenstrual phase, which starts before your period and stops within a few days of bleeding, which substances do you use to cope with your premenstrual MOOD symptoms, i.e., irritability, sadness, or anxiety?,” and “During the premenstrual phase, which starts before your period and stops within a few days of bleeding, which substances do you use to cope with your premenstrual PHYSICAL symptoms, i.e., cramping, headaches, bloating, breast tenderness etc.?” If the participant indicated that they used a substance to manage symptoms, they were asked the type or method of consumption, and how frequently they used (number of times per week) in the follicular and luteal phases of the menstrual cycle, in a typical cycle. For alcohol, participants reported the number of standard units consumed per week with the definition as “a standard unit of alcohol is equivalent to 12 oz of regular beer, 5 oz of wine, 1.5 oz of distilled spirits/hard liquor.” They were provided with the following definitions: “Follicular phase is from the start of the period (first day of bleeding) until ovulation or roughly mid-cycle. Luteal phase is the premenstrual phase, from ovulation until the start of the next period. This is when premenstrual symptoms would occur.” Participants were also asked how each substance impacted their premenstrual mood and physical symptoms using a 5-point Likert scale, rating if the substance use made their symptoms worse, a little worse, no impact, a little better, or better.
PMDD status, premenstrual symptom severity
Participants were categorized as having PMDD if they responded “Yes” to all of the following items: “Do you notice changes in your mood or physical symptoms, which start before your period and stop within a few days of bleeding?,” “Have you been formally diagnosed by a health care provider with premenstrual dysphoric disorder (PMDD)?,” and “If yes, did you complete daily symptom tracking for two months (for example, the Daily Record of Severity of Problems or Penn Daily Symptom Report)?” All other participants were categorized as non-PMDD.
To assess premenstrual symptom severity, participants completed the Premenstrual Symptoms Screening Tool (PSST). 33 The PSST is a 19-item questionnaire that queries premenstrual symptom severity on a Likert scale of 0 (Not at all) to 3 (Severe), with total scores ranging from 0 to 57.
Statistical analyses
Demographic characteristics and dependent variables were tested for normality using Kolmogorov–Smirnov tests and normal probability plots and summarized by standard descriptive measures. Graphical displays were used to assess relationships between variables and distributional assumptions. To address extreme outliers, data were Winsorized to the 95th percentile.
A Welch’s two sample t-test compared continuous demographic and health characteristics between the Non-PMDD and PMDD groups, and Chi-square tests compared categorical demographic and health variables between the two groups. To assess the relationship between premenstrual symptom severity and frequency of substance use during the luteal phase, a Spearman’s correlation was run for each substance. Mixed effects models assessed differences in frequency of substance use by menstrual cycle phase (follicular, luteal) and group (Non-PMDD, PMDD). As racial makeup differed significantly between groups, race was adjusted for as a covariate in mixed effects models. To explore the potential impact of prescription medication use for managing premenstrual symptoms in addition to substances, medication use was added to models in the same way. Analyses were performed in RStudio. 34
Results
Sample characteristics, demographics
Data were collected from 703 survey responders. Of those, 665 (94.6%) reported having a menstrual cycle in the past year. Among those participants, the mean age was 28.7 (9.1) years; 658 (99.0%) reported being assigned female at birth, and reported gender identities included female (n = 633, 95.2%) and nonbinary (n = 22, 3.3%) (remainder indicated “other” or “prefer not to answer”). Participants who only filled out the demographics section of the survey but did not complete any other questions were excluded from further analysis, leaving 634 participants (Table 1). The racial makeup of these participants were White or Caucasian (n = 358, 56.5%), Asian, Native Hawaiian, or Pacific Islander (n = 105, 16.6%), Hispanic or Latino/a/x (n = 54, 8.5%), Black or African American (n = 48, 7.56%), Biracial/Multiracial (n = 40, 6.3%), other (n = 15, 2.3%), American Indian or Alaska Native (n = 3, 0.5%), and the remainder indicated “Prefer Not to Answer” or left the question blank (n = 11, 1.7%).
Demographics
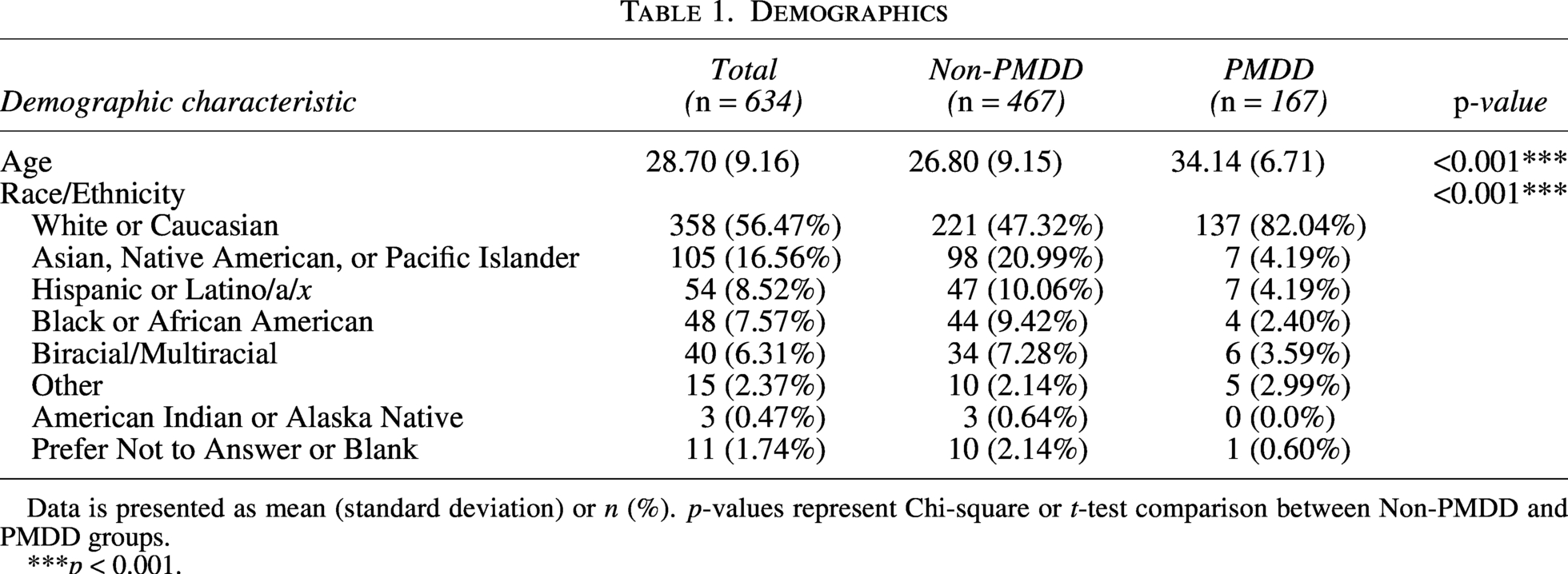
Data is presented as mean (standard deviation) or n (%). p-values represent Chi-square or t-test comparison between Non-PMDD and PMDD groups.
***p < 0.001.
Among these 634 participants, 280 (44.2%) reported being diagnosed with PMDD by a health care provider. Of those, 180 (64.3%) reported performing two menstrual cycles of daily symptom rating in the diagnosis process. Based on health care provider diagnosis using two menstrual cycles of daily symptom rating, participants were grouped as PMDD (n = 167) or non-PMDD (n = 467). Non-PMDD participants, with a mean age of 26.8 (SD 9.2) years, were significantly younger than PMDD participants whose mean age was 34.1 (SD 6.7) years, (t[610] = −9.2, p < 0.001). There was a significant difference in the racial makeup between the non-PMDD and PMDD groups, (X2 [8, 665] = 66.09, p < 0.001): White or Caucasian respondents comprised 47.3% of the non-PMDD group, and 82.0% of the PMDD group.
Premenstrual mood and physical symptoms
Premenstrual symptoms screening tool
Regarding premenstrual symptom severity, the mean PSST score was significantly higher in the PMDD group (M = 46.4 [7.1])than the non-PMDD group (M = 32.0 [15.4]), (t[632] = −11.6, p < 0.001), indicating more severe symptoms in the PMDD group.
Symptoms endorsed on the PSST at the moderate or severe level were fatigue/lack of energy (n = 522, 82.3%), tearful/increased sensitivity to rejection (n = 489, 77.1%), anxiety/tension (n = 472, 74.4%), anger/irritability (n = 466, 73.5%), physical symptoms such as breast tenderness, headaches, joint/muscle pain, bloating (n = 464, 73.2%), depressed mood/hopelessness (n = 462, 72.9%), feeling overwhelmed or out of control (n = 452, 71.3%), decreased interest in social activities (n = 438, 69.1%), overeating/food cravings (n = 435, 68.6%), decreased interest in work activities (n = 431, 68.0%), difficulty concentrating (n = 421, 66.4%), decreased interest in home activities (n = 397, 62.6%), hypersomnia (n = 365, 57.6%), and insomnia (n = 258, 40.7%).
Among all participants, n = 503 (79.3%) reported that premenstrual symptoms, at the moderate or severe level, interfered with their functioning, including work efficiency or productivity (n = 455, 71.8%), social activities (n = 413, 65.1%), home responsibilities (n = 375, 59.1%), relationships with family (n = 362, 57.1%), and relationships with peers (n = 344, 54.3%). Out of the 167 PMDD participants, interference was reported in work efficiency or productivity (n = 134, 80.2%), social activities (n = 119, 71.3%), home responsibilities (n = 112, 67.1%), relationships with peers (99, 59.3%) and relationships with family (n = 97, 58.1%).
Medications and supplements
Many participants reported being prescribed medication specifically for their premenstrual mood symptoms (n = 207 [32.7%]) (Table 2). Within the PMDD group, n = 104 (62.3%) reported using medication prescribed to manage premenstrual mood symptoms, and in the non-PMDD group n = 103 (22.1%). The most common medications prescribed for premenstrual mood symptoms among the full sample included antidepressants (n = 136, 21.5%), hormonal contraceptives (n = 65, 10.3%) including oral contraceptives (n = 39, 6.2%) and hormonal IUD (n = 26, 4.1%), and benzodiazepines (n = 30, 4.7%). Mean PSST severity was significantly higher in participants who were prescribed medication specifically for premenstrual symptoms (p < 0.005).
Medication and Supplement Use to Manage Premenstrual Symptoms

Data is presented as n (%). p-values represent Chi-square comparison between non-PMDD and PMDD groups.
***p < 0.001.
Many participants reported using over-the-counter supplements to manage their premenstrual symptoms, the most common being magnesium (n = 156), vitamin D (n = 146), and B vitamins (n = 128).
Recreational substance use
Participants were asked to indicate which substances they used recreationally and/or without a prescription from a health care provider. Participants reported using alcohol (n = 304, 48.0%) cannabis (n = 208, 32.8%), tobacco/nicotine (n = 89, 14.0%), psychedelics or hallucinogens (n = 67, 10.6%), stimulants (n = 14, 2.2%), cocaine (n = 5, 0.8%), and benzodiazepines (n = 4, 0.6%).
Substance use to manage premenstrual symptoms
When asked which substances they use to manage premenstrual mood symptoms, such as irritability, sadness, or anxiety, participants reported using cannabis (n = 190, 30.0%), alcohol (n = 102, 16.1%), tobacco/nicotine (n = 55, 8.7%), psychedelics or hallucinogens (n = 39, 6.2%), benzodiazepines (n = 29, 4.6%), stimulants (n = 20, 3.2%), and cocaine (n = 1, 0.2%). Within solely the PMDD group, participants reported using cannabis (n = 86, 51.5%), alcohol (n = 34, 20.4%), tobacco/nicotine (n = 27, 16.2%), psychedelics or hallucinogens (n = 21, 12.6%), benzodiazepines (n = 10, 6.0%), and stimulants (n = 11, 6.6%) to manage their premenstrual mood symptoms. Among those who used each substance, the proportion using it to manage premenstrual mood symptoms was 91.4% for cannabis, 61.8% for nicotine, 58.2% for psychedelics, and 33.6% for alcohol.
To manage physical symptoms, participants reported using cannabis (n = 146, 23.0%), alcohol (n = 39, 6.2%), tobacco/nicotine (n = 19, 3.0%), stimulants (n = 12, 1.9%), benzodiazepines (n = 6, 1.0%), and cocaine (n = 1, 0.2%). Within the PMDD group, participants reported using cannabis (n = 67, 40.1%), tobacco/nicotine (n = 11, 6.6%), alcohol (n = 9, 5.4%), stimulants (n = 7, 4.2%), and benzodiazepines (n = 2, 1.2%) to manage physical symptoms. Among those who used each substance, the proportion using to manage premenstrual physical symptoms was 70.2% for cannabis, 21.3% for nicotine, 12.8% for alcohol, and none for psychedelics.
Substance use frequency correlation with symptom severity
Participants reported the frequency of substance use per week in the follicular phase and the luteal phase (Table 3). There was a significant positive correlation between PSST score and cannabis use during the luteal phase (p < 0.005) (Fig. 1) as well as a positive correlation between PSST score and nicotine use (p < 0.005 (Fig. 2). No significant correlation was found between symptom severity and alcohol or psychedelic use. Within participants with PMDD, there was a significant positive correlation between PSST score and cannabis use during the luteal phase (p < 0.001). No significant correlation was found for alcohol, nicotine, or psychedelic use within the PMDD group.
Mean Substance Use Frequency per Week by Group and Menstrual Cycle Phase
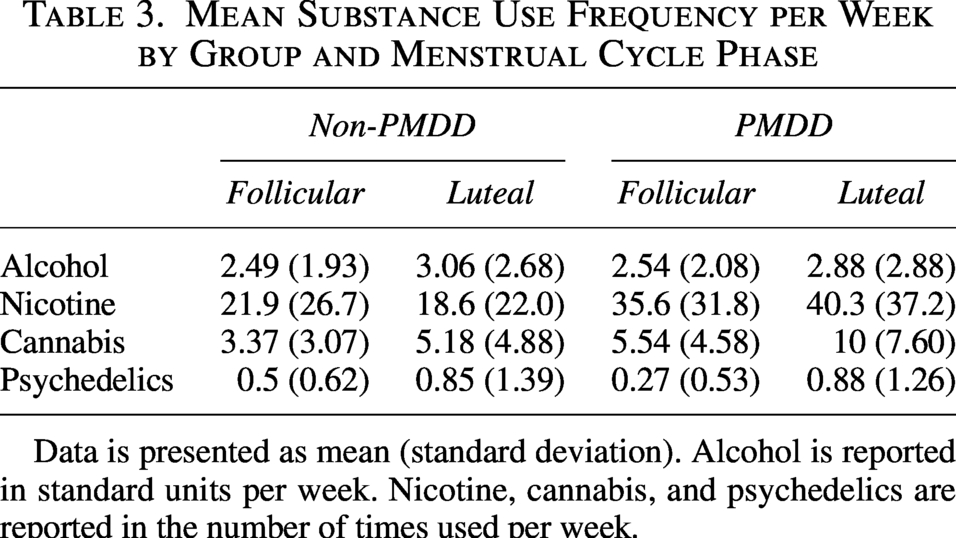
Data is presented as mean (standard deviation). Alcohol is reported in standard units per week. Nicotine, cannabis, and psychedelics are reported in the number of times used per week.
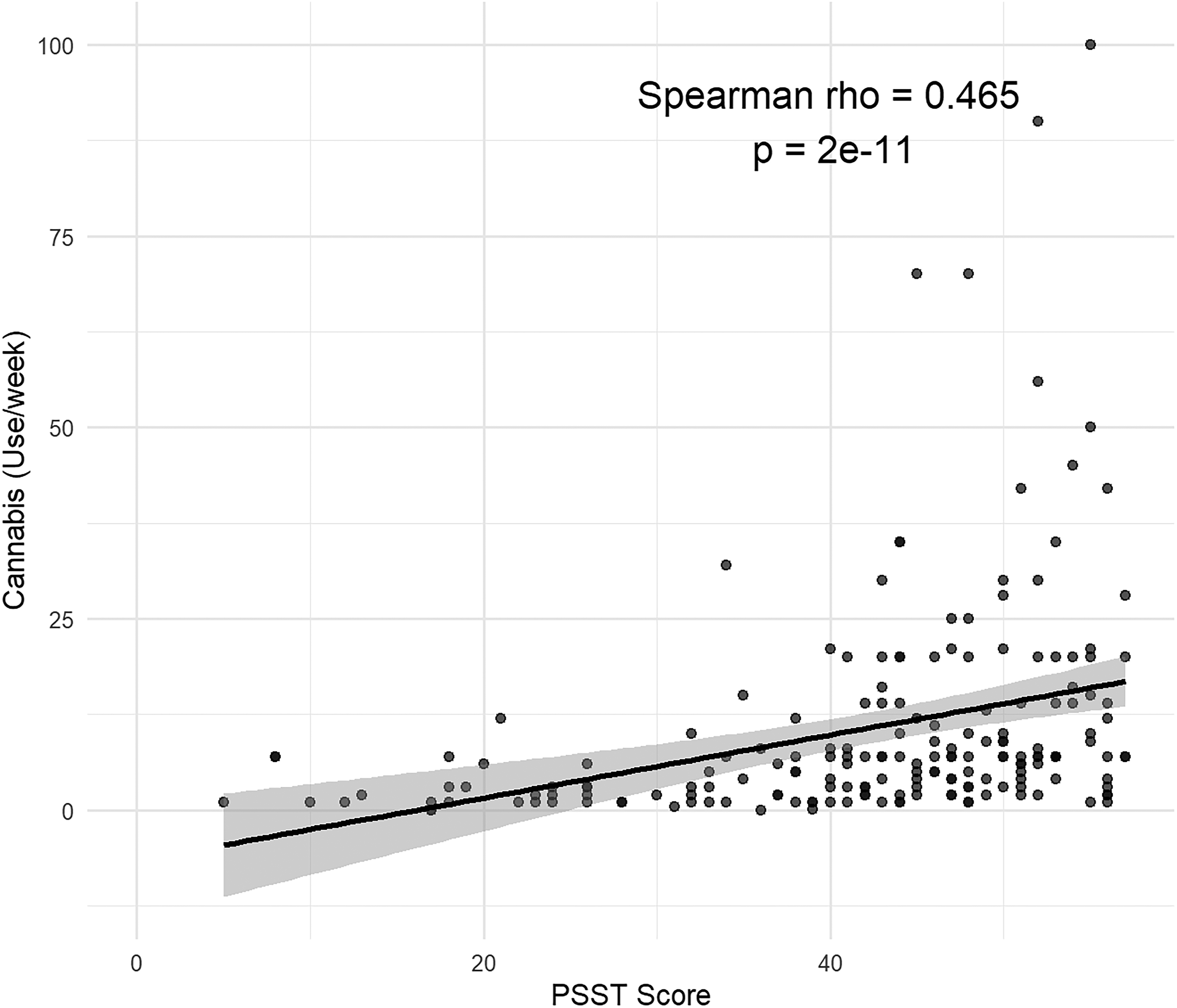
A significant correlation was found between Premenstrual Symptoms Screening Tool (PSST) score and cannabis use during the luteal phase.
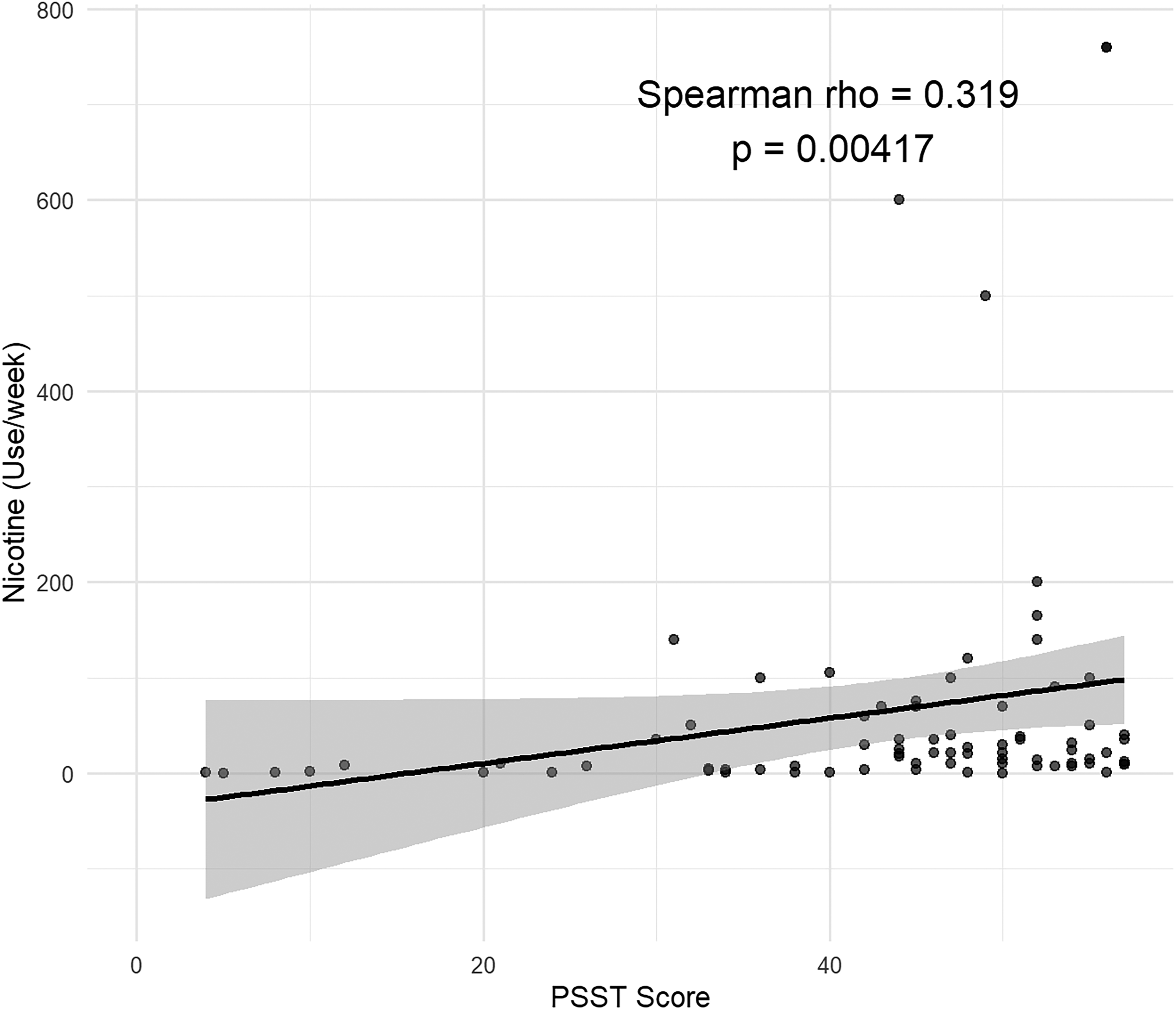
A significant correlation was found between PSST score and nicotine use during the luteal phase.
Alcohol
Participants reported consuming 3.4 (SD 3.6) alcoholic drinks per week in the follicular phase, and 4.4 (SD 6.0) alcoholic drinks per week in the luteal phase.
A mixed effects model indicated a significant main effect for phase (F[1, 275.4] = 12.3, p < 0.001), indicating that alcohol use was greater in the luteal phase than the follicular phase in both non-PMDD and PMDD groups. There was no significant main effect of group (F[1, 276.6] = 1.4, p = 0.2) and no interaction between group and phase (F[1, 275.4] = 0.3, p = 0.6).
When models were adjusted for race and medication use, race was a significant covariate (p = 0.02), but prescription medication use had no effect (p = 0.3). Still, there was no significant main effect of group (F[1, 274.6] = 1.0, p = 0.3) and no interaction between group and phase (F[1, 275.4] = 0.3, p = 0.6).
Among participants who reported that alcohol affected their symptoms, some reported that alcohol made their premenstrual mood symptoms better (n = 5, 5.4%), a little better (n = 40, 43.5%), or had no impact (n = 16, 17.4%). Others reported it made mood symptoms a little worse (n = 17, 18.5%) or worse (n = 14, 15.2%). Of participants who reported alcohol impact on premenstrual physical symptoms, participants reported alcohol made their symptoms better (n = 2, 5.6%), a little better (n = 13, 36.1%), had no impact (n = 10, 27.8%), a little worse (n = 7, 19.4%), or worse (n = 4, 11.1%).
Within the PMDD group, there was not a significant difference in alcohol use during the luteal phase between participants who take prescribed medications to manage their premenstrual mood symptoms compared with those who do not (t[47.1] = 1.0, p = 0.3).
Nicotine
Based on IQR, 95%, two values were Winsorized in these analyses. In the follicular phase, participants reported consuming nicotine/tobacco M = 56.9 (129.3) times per week, and in the luteal phase, consuming M = 66.0 (145.3) times per week.
A mixed effects model indicated a significant interaction between group and phase (F[1, 77] = 5.2, p = 0.03), such that PMDD participants reported more nicotine use than non-PMDD participants in the luteal phase. When models were adjusted for race and medication use, neither race (p = 0.1) nor medication use (p = 0.3) was significant. The significant interaction between group and phase remained (F[1, 77] = 5.2, p = 0.03).
While some participants reported that nicotine made their premenstrual mood symptoms better (n = 3, 5.8%) or a little better (n = 19, 36.5%), others reported that it had no impact (n = 25, 48.1%) on their symptoms, made mood symptoms a little worse (n = 4, 7.7%), or worse (n = 1, 1.9%). For premenstrual physical symptoms, some participants reported nicotine made their symptoms a little better (n = 4, 22.2%), while most reported no impact (n = 14, 77.8%).
Within the PMDD group, there was no significant difference in nicotine use during the luteal phase between participants who take prescribed medications to manage their premenstrual mood symptoms compared with those who do not (t[15.5] = 1.14, p = 0.3).
Cannabis
A variety of formulations were used by participants who reported cannabis use (n = 208): edibles (n = 132, 63.5%); joints, blunts, pipes or bongs (n = 129, 62.0%); vaping (n = 76, 36.5%); tinctures (n = 23, 11.1%); topical oils or lotions (n = 17, 8.2%); beverages (n = 16, 7.7%); synthetic cannabinoids such as delta-8 THC (n = 14, 6.7%); THC resin (n = 13, 6.3%); capsules (n = 5, 2.4%); sprays (n = 2, 1.0%); transdermal patches (n = 2, 1.0), or other (n = 3, 1.4%).
A mixed effects model found a main effect for cycle phase, such that cannabis use was more frequent in the luteal phase (M = 10.7 [14.8]) than the follicular (M = 7.4 [9.7]), (F[1, 185] = 29.6, p =< 0.001). There was also a significant main effect for group, suggesting that PMDD individuals used cannabis more often than those without PMDD in both phases (F[1, 185] = 6.9, p = 0.01); those in the PMDD group reported using cannabis in follicular phase M = 9.5 (11.2) times per week and in the luteal phase M = 14.1 (16.1) times per week, while those in the non-PMDD group used M = 6.02 (8.3) times per week in the follicular and M = 8.5 (13.5) in the luteal. There was a trend toward a significant interaction between group and phase (F[1, 185] = 2.7, p = 0.1). When models were adjusted for race and medication use, race was a significant covariate (p = 0.01), but medication use (p = 0.6) was not significant. Still, there was a main effect of cycle phase (F[1, 185] = 29.6, p =< 0.001) and group (F[1, 183] = 4.6, p = 0.03), as well as a trend toward a significant interaction between group and phase (F[1, 185] = 2.7, p = 0.1).
Most participants reported that cannabis made their premenstrual mood symptoms better (n = 67, 38.1%) or a little better (n = 99, 56.3%), and others reported it had no impact (n = 4, 2.3%) or made mood symptoms a little worse (n = 6, 3.4%). For premenstrual physical symptoms, participants reported cannabis made their symptoms better (n = 39, 28.7%), a little better (n = 83, 61.0%), while some others reported no impact (n = 13, 9.6%) or making symptoms a little worse (n = 1, 0.7%).
Within the PMDD group, there was no significant difference in cannabis use during the luteal phase between participants who take prescribed medications to manage their premenstrual mood symptoms compared with those who do not (t[27.9] = 1.3, p = 0.2).
Psychedelics, hallucinogens
Participants who said yes to psychedelic and hallucinogen use reported using psilocybin or mushrooms/truffles (n = 51, 76.1%), LSD (n = 14, 18.4%), MDMA (n = 11, 16.4%), ketamine (n = 7, 10.5%), DMT (n = 3, 4.5%), ayahuasca (n = 2, 3.0%), or other (n = 2, 3.0%).
A mixed effects model indicated a significant main effect for phase (F[1, 33] = 8.0, p = 0.01), with more frequent use of psychedelics during the luteal phase compared with the follicular phase in both groups. In the luteal phase, participants reported using psychedelics a mean of M = 2.14 (2.5) times per week, and in the follicular phase using M = 1.2 (2.0) times per week. There was no significant main effect of group (F[1, 33] = 1.9, p = 0.2), and no significant interaction between group and phase (F[1, 33] = 1.2, p = 0.3). When models were adjusted for race and medication use, neither race (p = 0.3) nor medication use (p = 0.2) were significant. Still, there was a significant main effect for phase (F[1, 33] = 8.0, p = 0.01), and no significant main effect of group (F[1, 33] = 0.04, p = 0.5), and no significant interaction between group and phase (F[1, 33] = 1.2, p = 0.3).
Most participants reported that psychedelics made their premenstrual mood symptoms better (n = 15, 44.1%) or a little better (n = 16, 47.1%), and others reported it had no impact (n = 2, 5.9%) or made mood symptoms worse (n = 1, 2.9%). For premenstrual physical symptoms, participants reported psychedelics made their symptoms better (n = 4, 57.1%) or a little better (n = 3, 42.9%).
Within the PMDD group, there was no significant difference in psychedelic use during the luteal phase between participants who take prescribed medications to manage their premenstrual mood symptoms compared with those who do not (t[9.5] = 0.41, p = 0.7).
Cocaine, stimulants, opioids, benzodiazepines
Eleven participants endorsed using stimulants recreationally, n = 5 cocaine, n = 4 benzodiazepines, and n = 3 opioids recreationally. Given the low number of responses, this data was not analyzed.
Substance use to manage perimenopausal symptoms
Among participants experiencing menstrual periods, n = 89 (14.0%) reported being age 40 years or older. Of those, n = 45 (50.6%) reported experiencing perimenopausal symptoms.
Among participants aged 40 and older who reported perimenopausal symptoms, when asked which substances they use to manage perimenopausal mood symptoms, participants reported using cannabis (n = 8, 17.8%), tobacco/nicotine (n = 5, 11.1%) alcohol (n = 3, 6.7%), and opiates (n = 1, 2.2%). To manage perimenopausal physical symptoms such as hot flashes, participants reported using cannabis (n = 4, 8.9%), tobacco/nicotine (n = 2, 4.4%), alcohol (n = 1, 2.2%), psychedelics or hallucinogens (n = 1, 2.2%), and opiates (n = 1, 2.2%).
Given the low number of responses on how these substances impacted perimenopausal symptoms, this data was not analyzed.
Discussion
This is the first study, to our knowledge, to assess the use of psychedelics across the menstrual cycle, including frequency and symptom management. These data, drawn from over 600 participants, found that nearly 30% reported using cannabis and about 6% reported using psychedelics to manage premenstrual mood symptoms. Within the PMDD group, over 50% reported using cannabis and 12.6% using psychedelics to manage premenstrual mood symptoms.
Many of those with PMDD reported using cannabis to manage premenstrual mood symptoms or physical symptoms. This echoes a prior survey study, in which 88.5% of participants reported using cannabis to manage premenstrual headaches, nausea, diarrhea, anger, sadness and weakness, and 89.4% reported that it had improved symptoms. 35 Notably, our data showed an association between premenstrual symptom severity and frequency of cannabis use during the luteal phase, suggesting that individuals with more severe premenstrual symptoms may use cannabis more often in order to cope with symptoms. Participants perceived that cannabis improved their premenstrual symptoms; approximately 94% stated that cannabis made their mood symptoms better or a little better, and approximately 90% reported that cannabis made their physical symptoms better or a little better.
Psychedelics were used by 12.6% in the PMDD group to manage premenstrual mood symptoms, although none reported using them to manage physical premenstrual symptoms. There was no association between frequency of psychedelic use and premenstrual symptom severity in the luteal phase, unlike cannabis. Participants perceived psychedelics as useful in managing their premenstrual mood symptoms, with approximately 91% reporting that they made mood symptoms better or a little better.
Several substances—psychedelics, cannabis, and alcohol—were used more frequently in the luteal phase than the follicular, regardless of PMDD status. This is consistent with previous research for cannabis,25,26 and alcohol.36,37 For cannabis, there was also a main effect of group, such that PMDD individuals used cannabis more often than those without PMDD regardless of menstrual cycle phase. For nicotine, PMDD participants reported significantly more nicotine use than non-PMDD participants in the luteal phase only, consistent with a systematic review that found that nicotine use increased premenstrually, which was more pronounced in women with PMS or PMDD. 24 As described, there was an association between premenstrual symptom severity and frequency of cannabis and nicotine use during the luteal phase, which could suggest self-medication with these substances. Indeed, women with greater coping motives combined with more severe premenstrual depressive symptoms reported more frequent cannabis use during the luteal phase, 25 and in women with PMDD, depressed mood predicted increased self-reported cannabis use in the first days of menses. 24
Some participants used these substances in addition to prescribed medications such as antidepressants. Within the PMDD group, 62.3% reported using medication prescribed by a healthcare provider to manage premenstrual mood symptoms, and 60.5% of participants reporting using both prescribed medication and substances to manage premenstrual mood symptoms. However, there was no difference in frequency of use of any of the substances during the luteal phase when comparing participants who did versus did not take prescribed medications to manage their premenstrual mood symptoms.
Further research, particularly controlled trials, are needed regarding use of substances such as cannabis and psychedelics to manage premenstrual symptoms. Clinical trials have shown some positive effects of cannabis products, mainly focused on premenstrual physical symptoms. A CBD suppository reduced premenstrual pain and physical symptoms compared with treatment as usual. 38 In an open-label trial, CBD oral softgels decreased self-reported premenstrual anxiety, stress, and irritability. 39 In women who self-reported having PMS or PMDD, participants reported positive expectancies that cannabis would help manage premenstrual irritability, mood swings, depressed mood, anxiety, and sleep. 40 Placebo-controlled trials of psilocybin have shown it can be effective in treating mood disorders such as major depression,6,7,9,41 but there are no trials to date of psychedelic treatment for PMDD.
The survey also explored how people use substances to manage perimenopausal symptoms. Among those who reported perimenopause symptoms, they most often used cannabis to manage mood symptoms. Previous studies have found that cannabis is often used to manage perimenopausal symptoms including sleep, muscle/joint pain, and depressive or anxiety symptoms.31,32 Regarding psychedelics, one participant reported using to manage physical symptoms. There are no other studies to our knowledge that investigate psychedelic use to manage symptoms in perimenopause.
This survey study had several strengths and limitations. Strengths included a large sample representing a range of ages and demographics, although as a self-selecting sample, the generalizability is unknown. This is the first study to assess use of psychedelics across the menstrual cycle, including individuals with PMDD, an understudied population. 42 A key limitation was reliance on self-report data, including self-reporting if and how they were diagnosed with PMDD, and reliably reporting on substance use. Regarding self-reported PMDD diagnosis, we used a strict definition: changes in symptoms that start before menses and stop within a few days of bleeding, formal diagnosis of PMDD by a health care provider, using daily symptom tracking for two menstrual cycles. As two cycles of prospective tracking is required by the DSM for PMDD diagnosis, this was meant to capture people who likely met strict DSM criteria for PMDD. Our categorization is based on a similar anonymous survey study that asked participants “Has a medical professional ever examined daily symptom ratings across two cycles to determine a diagnosis of PMDD?;” those who participants responded affirmatively were included in the PMDD group. 43 However, we acknowledge that classifying all other participants as non-PMDD likely risks misclassification, as this non-PMDD group could include participants with probable PMDD who did not complete prospective tracking. Regarding substance use frequency, retrospective self-report data can be affected by recall bias, and asking respondents to recall substance use frequency in two discrete menstrual cycle phases may have introduced inaccuracies. There may have been variations between the definitions of menstrual cycle phases that we provided, versus what an individual participant’s specific phases were given menstrual cycle length and ovulation timing. Dichotomizing of follicular and luteal phases may have led respondents to expect there to be a difference between these two phases, possibly prompting them to misrepresent differences in usage patterns in these phases. Methods that assess substance use and menstrual cycle phase prospectively, such as daily diaries, timeline follow-back calendars, or menstrual cycle tracking calendars, are less subject to recall bias.
Another limitation was recruiting from a limited population; responders were drawn from IAPMD.org (an organization that serves individuals with premenstrual disorders worldwide), the JHU RMHC website (visible to anyone worldwide with internet access), the JHU Sona Psychology Research Portal (available only to JHU students), and emails to previous research participants in the RMHC (a sample of individuals with prospectively diagnosed PMDD who previously participated in clinical research in our center), and are therefore not necessarily representative of all individuals who experience menstrual cycles or use substances, again, limiting generalizability. Relatedly, White or Caucasian respondents comprised 47% of the non-PMDD group and 82% of the PMDD group; race was adjusted for in models to reduce the possibility that results are confounded by race. Questions about differences in PMDD in minoritized groups are not well-studied. 44 Studies assessing PMDD prevalence by race have generally not used prospective symptom ratings. 17 One such study found that Black women were less likely than White women to experience PMDD, 45 and another found that PMDD prevalence rates are higher in the African continent than in Europe or North America. 17 The inclusion of more minoritized participants in future studies would make the results more generalizable. Finally, we did not account for polysubstance use, asking about use of each substance in isolation, which may also limit generalizability. It is possible that a participant who was using multiple substances for instance, attributed premenstrual symptom improvement to one substance, when it could have been due to another or to a combination.
Future research should include clinical trials to assess efficacy and safety of substances such as cannabis and psychedelics to manage premenstrual symptoms, especially given that these substances are, according to this survey, commonly used for premenstrual symptoms, despite a lack of research data on safety or efficacy. Further, given the powerful effects of neuroactive steroid hormones on neurotransmitter systems that are targeted by drugs such as psilocybin and cannabis,46,47 work is needed on how ovarian hormones may influence psychedelic effects in females. 48
Authors’ Contributions
Conceptualization: L.H. and M.E.Y. Data curation: M.N. Formal analysis: M.N. and V.P. Investigation: L.H. and M.E.Y. Methodology: L.H. and M.E.Y. Project administration: M.N. Supervision: L.H. and M.E.Y. Visualization: M.N. and V.P. Writing—original draft: A.G., L.H., M.N., V.P., and M.E.Y. Writing—review and editing: A.G., L.H., M.N., V.P., and M.E.Y.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
M.E.Y, received support from philanthropic contributions from the Heffter Research Institute, Steven and Alexandra Cohen Foundation, Tim Ferriss, Matt Mullenweg, Craig Nerenberg, and Blake Mycoskie. M.N. received support from an Undergraduate Summer Fellowship from the Women, Gender, and Sexuality Department at Johns Hopkins University.